
Abstract
Social anxiety is highly prevalent among nursing students and is associated with poor mental health. However, the underlying mechanism in such an association remains unclear. This study aimed to examine the potential mediating role of social intelligence in the association between social anxiety and mental health using the Stress-Coping Model (SCM) as the theoretical framework. A cross-sectional study was conducted among 748 nursing students recruited from a Chinese University from December 2022 to March 2023. Students completed an online questionnaire to assess their social anxiety, social intelligence, and mental health. The PROCESS SPSS Macro (model 4) was used to test the mediation effect of social intelligence on the association between social anxiety and mental health. The results showed that nursing students had moderate levels of social anxiety, social intelligence, and mental health, which varied according to their profile characteristics. Social anxiety was negatively associated with mental health, and the association was partially mediated by social intelligence. Our study offers fresh insights into the impact of social anxiety on mental health and sheds light on the intricate mediating role of social intelligence. These findings offer valuable insights for research and clinical endeavors aimed at formulating psychosocial interventions to enhance the mental health of nursing students.
Similar content being viewed by others
Introduction
Social anxiety is a common mental disorder characterized by an intense fear during and avoidance of many social situations, with impaired social functioning as its hallmark symptom1,2. Worldwide, social anxiety is highly prevalent, with a reported lifetime prevalence across nations ranging from 0.2% in Nigeria to 12.1% in the USA3. Epidemiological studies show that social anxiety disproportionately affects the young population, occurring in more than 1 in 3 (36%) young people4. Additionally, social anxiety is more prevalent in females than males3. People with social anxiety often struggle with social situations and have difficulty initiating and maintaining human interactions, manifested as extreme and persistent fear of embarrassment and humiliation4.
The impact of social anxiety is widespread, and numerous studies have demonstrated a significant association between social anxiety and mental health5,6,7. According to the World Health Organization (WHO), mental health is “a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community”8. Mental health problems have become a major global health concern, with an increasing trend in their diagnoses and treatment in various populations and across countries, as evidenced by several recent literature reviews [9 10,11.
Nursing is a challenging and stressful profession characterized by excessive workload, leadership/management styles, professional conflict, and the emotional cost of caring12,13. As the world’s largest direct care group, nurses undertake the major communication responsibilities to interact with the patients and families, and they also have to deal with relationships with other healthcare providers, which all put nurses at a high risk of emotional distress12,13. In addition, nursing students in nursing education programs need to receive high-intensity training and advance their interpersonal communication skills to better prepare them for their future professional nursing roles, which may produce high levels of stress and anxiety12,13. A study showed that 27.4% of nursing students had moderate social anxiety, and 76.8% had average professional adjustment14. Nursing students with social anxiety are at an increased risk of developing mental health problems such as depression, anxiety, and even suicide ideation15.
While the significant association between social anxiety and mental health is well-established among nursing students, few studies have explored the underlying mechanism of such an association. One potential factor that may play a crucial role in linking social anxiety and mental health is social intelligence. The concept of social intelligence was first coined by Thorndike in 192016, who described it as the ability to understand and manage others and react appropriately in framing adaptive social relationships. Although various definitions have been proposed regarding social intelligence, they all share two key elements: the awareness of others and the response and adaptation to others17. Social intelligence is a broad term that involves multiple components, including personal attitude, social performance skills, empathetic ability, emotional expressiveness, and emotional confidence18. Socially intelligent people are creative and friendly people who can solve problems and tackle various tasks in social life, thus developing healthy co-existence with other people17. Social intelligence is culture-dependent, and different aims and objectives of the behaviors may be assumed as socially intelligent by various cultures19.
The essential role of social intelligence in maintaining a healthy social life has received increasing research attention. A plethora of studies have consistently shown a positive association between social intelligence and a wide range of health outcomes, such as self-esteem, resilience, and general mental health in clinical and non-clinical populations20,21,22. In addition, social intelligence is also closely associated with social anxiety since both can be understood as the interpersonal signals of one person affecting the behaviors of another23. People with social anxiety may lack the ability to correctly understand others’ emotions in social interactions, thus reinforcing their fear of misbehaving and leading to poor social intelligence24. On the other hand, people with poor social intelligence are more likely to develop psychological distress due to their inappropriate interactions with other people, leading to poor mental health20. However, the potential role of social intelligence linking social anxiety to mental health among nursing students has not been fully understood. Knowledge of the underlying mechanism underlying the correlation between social anxiety and mental health may be helpful in developing effective and targeted intervention programs to reduce the negative impacts of social anxiety and improve nursing students’ mental health.
To better comprehend the association between social anxiety, social intelligence, and mental health, we leveraged the Stress-Coping Model (SCM) developed by Lazarus and Folkman25,26 as our theoretical framework and asserted that social anxiety may affect mental health indirectly through social intelligence. The SCM posits that coping, including cognitive and behavioral responses, determines individuals’ different adaptations to the same stressful situation. According to Lazarus and Folkman25,26, stress results from an imbalance between perceived external or internal demands and the perceived personal and social resources to deal with them, which involves two steps: primary appraisal and secondary appraisal. Primary appraisal is the initial evaluation of whether the situation is irrelevant or stressful to one’s well-being, while secondary appraisal is the assessment of whether one’s resources can be used to adapt to the situation. Using this theoretical framework, when nursing students encounter social anxiety, they may appraise it as a stressful event and may also evaluate how much social anxiety may affect their mental health (primary appraisal). Next, the nursing students appraise what types of coping resources they have and how they can use their coping resources, such as social intelligence, to reduce the negative effects of the stressor (secondary appraisal). Lastly, their social intelligence may cope with stressors and limitations, leading to improved mental health. That is, social intelligence may function as a coping resource, reducing the effects of social anxiety on mental health in nursing students. In this situation, social intelligence functions as a mediating factor.
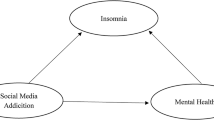
Based on the SCM25,26, we conducted the current study to examine the mediating effect of social intelligence on the association between social anxiety and mental health among Chinese nursing students. Figure 1 shows the hypothesized conceptual mediation model of the study. Specifically, we proposed the following two hypotheses:
-
1.
Social anxiety was negatively associated with mental health among Chinese nursing students.
-
2.
Social intelligence mediated the association between social anxiety and mental health.

The conceptual mediation model.
Methods
Study population and procedure
A cross-sectional study was conducted at a University in Henan Province, China, from December 2022 to March 2023. A convenient sampling method was utilized to recruit nursing students who satisfied the following inclusion criteria: (1) age ≥ 18, (2) nursing students enrolled in accredited nursing programs, (3) with normal cognitive and mental ability to comprehend and respond to the questionnaire, and (4) voluntary participation in the study. We excluded nursing students who had completed less than one semester of their nursing programs and those who were unable to complete the questionnaire due to severe physical and mental illness. The sample size was calculated according to the formula provided by Israel27: n = N * [Z2 * p * (1-p) /e2] / [N – 1 + (Z2 * p * (1-p) /e2], we set z = 2.58 (corresponding to a confidence interval of 99%), p = 0.5, N = 3,000 (population size, the total number of nursing students), and e = 0.05, which required a minimal sample size of 545. Considering a rejection rate of 25%, we further expanded our sample size to 727.
The research proposal was approved by the Ethics Review Committee of Philippine Women’s University (ERB PROTOCOL NUMBER: ERB2022_0105). The study was conducted in strict accordance with the relevant guidelines and regulations governing research involving human participants. Students were recruited by a nursing instructor in a course who provided detailed information about the study’s purpose, procedure, benefits, and potential risks. The students were informed that participation was voluntary, and refusal or dropping out of the study would not affect their study and credits in the course. The research team developed the online questionnaire using Sojump, which is China’s largest online survey platform for questionnaire design and distribution28. The anonymous function was activated to disable IP address tracking and ensure student privacy and anonymity. Students interested in participation could scan a QR code and access the online questionnaire after providing electronic informed consent. The online questionnaire included a request for demographic information (e.g., age and gender) and measures for social anxiety, social intelligence, and mental health, which took about 20–30 min to complete. We distributed 800 questionnaires and received 748 valid ones after eliminating invalid ones, such as those with too short completion time, with a 93.5% response rate.
Instruments
Demographic information
A researcher-designed information sheet was used to collect students’ demographic information, including gender, family ranking, place of origin, personality, student leadership position, and family parenting style.
Results
Sample characteristics
The sample characteristics are shown in Table 1. Among the 748 students, most were females (81.8%), from rural areas (71.8%), not holding student positions (78.7%), and had introverted personalities (65.9%). Only children accounted for only 9.4% of the total sample. Regarding family parenting styles, the largest proportion of students reported democratic parenting style (46.5%), followed by dominant (29.9%) and uninvolved (17.4%) parenting styles. The mean scores of social anxiety, social intelligence, and mental health were 9.16 ± 3.83, 94.76 ± 12.99, and 16.20 ± 4.54, respectively.
Comparison of social intelligence by sample characteristics showed significantly higher scores in those with student positions (P < 0.001), extrovert personalities (P < 0.001), and democratic parenting styles (P = 0.016). Comparison of social anxiety by sample characteristics showed significantly higher scores in females (P = 0.002), those without student positions (P < 0.001), and those with introverted personalities (P < 0.001). Comparison of mental health by sample characteristics showed significantly higher scores in those with extrovert personalities (P < 0.001) and democratic parenting styles (P < 0.001).
Correlation analysis
As shown in Table 2, Pearson’s correlation analysis showed significant correlations among the participants’ social anxiety, social intelligence, and mental health. Specifically, social anxiety was negatively correlated with social intelligence (r = − 0.48, P < 0.01) and mental health (r = − 0.40, P < 0.01). In addition, social intelligence was positively correlated with mental health (r = 0.35, P < 0.01).
Mediation analysis
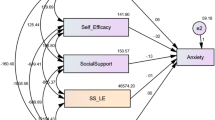
We utilized the SPSS PROCESS v.4.3 macro (Model 4) by Hayes36 for mediation analysis, with social anxiety as the independent variable, mental health as the dependent variable, and social intelligence as the mediator while controlling for all sample characteristics. The results are depicted in Fig. 2; Table 3.
In assessing Hypothesis 1, a significant negative correlation was found between social anxiety and mental health (total effect c = − 0.469, 95% CI = − 0.556 to − 0.383), indicating that higher social anxiety was associated with poorer mental health. However, the correlation coefficient between social anxiety and mental health decreased from − 0.469 to − 0.371 (p < 0.001) after the inclusion of the mediator social intelligence, signifying partial mediation.
Upon testing Hypothesis 2, a notable indirect influence of social anxiety on mental health via social intelligence was identified (ab = − 0.098, 95% CI − 0.144 to − 0.057), indicating that higher social anxiety was associated with lower social intelligence (a = − 1.469, p < 0.001), which in turn, was associated with poorer mental health (b = 0.067, p < 0.001).
The following demographic variables were adjusted: gender, place of origin, holding student positions, personality types, family ranking.

Schematic diagram of the mediation model illustrating the effect of social intelligence in the association between social anxiety and mental health. The following demographic variables were adjusted: gender, place of origin, holding student positions, personality types, family ranking.
Discussion
The levels of social anxiety, social intelligence, and mental health
Our study showed that the nursing students’ social anxiety was moderate, with a mean score of 9.16 ± 3.83 out of a total score of 18. This finding was consistent with previous research indicating the high prevalence of social anxiety among Chinese university students37,38. The cultural emphasis on collectivism and interpersonal harmony in Chinese society, the challenges of adapting to societal changes, and the pressure to succeed may contribute to university students’ social anxiety in social interactions39,40. The average social intelligence score was 94.76 ± 12.99 out of a total score of 144, indicating a moderate level. Our study’s social intelligence level was higher than that reported by Zhou using the same scale (84.21 ± 3.78)41. This difference may be attributed to the participants’ educational background, as the current study included four-year bachelor students who may have received more humanities-related courses, potentially enhancing their social skills.
In addition, our study’s average mental health score was 16.20 ± 4.54 out of a total score of 25, indicating a moderate level. This finding aligned with previous research indicating lower mental health levels among Chinese nursing students compared to their international counterparts42,43. One likely explanation may be related to the COVID-19 pandemic and the stringent isolation policies in China42. The increasing number of confirmed COVID-19 cases and deaths, the strict prevention and control measures, and the long-term social isolation all pose potential mental health risks for college students42. Due to inadequate life experiences and social skills to cope with the adverse impacts of COVID-19, college students are at an increased level of psychological distress, emotional disorders, and even suicidality44. The adverse psychological effects related to COVID-19 and its control measures lasted even after the Chinese government started to loosen its COVID-19 control policies44. In addition, college students in China are under high levels of academic pressure due to the increasingly fierce competition in the job market when graduate unemployment has become a growing concern45. The academic pressure is even more significant in those majoring in medicine and nursing, which demand an extensive investment of time and energy to complete their study tasks, leading to even poorer mental health46. Furthermore, other factors such as routine-oriented activities, limited leisure time, and the impact of excessive digital device use and passive engagement with social media may also contribute to the low levels of mental health in Chinese college students47.
The finding that women showed higher levels of social anxiety than men aligned with previous studies highlighting gender differences in social anxiety, social skills, and emotional recognition abilities. Societal pressures may influence women’s susceptibility to social anxiety, while men’s social skills may be attributed to competitive communication strategies and assertive communication styles48,49,50. Our study showed that students holding leadership positions exhibited significantly higher levels of social intelligence and lower levels of social anxiety than students without leadership roles. These findings aligned with previous research highlighting the positive impact of leadership positions on students’ personal and social development, including the development of essential competencies such as communication, critical thinking, teamwork, and problem-solving skills51,52. Participation in student leadership activities has been associated with higher self-esteem, life satisfaction, lower stress levels, and better mental health51,52.
Furthermore, our study showed that extroverted students exhibited significantly higher levels of social intelligence and mental health and lower levels of social anxiety than introverted students. This finding was congruent with previous studies demonstrating higher social engagement, better social support, and more positive perceptions of social situations among extroverted individuals, leading to better social skills, more happiness, and higher life satisfaction53,54. Additionally, our study indicated that parenting style had a significant influence on social intelligence and mental health, with the highest levels of social intelligence and mental health observed in students with democratic parenting styles. These findings aligned with previous research highlighting the importance of parental warmth, support, and communication in promoting positive social outcomes, while authoritarian and permissive parenting styles may have negative effects55,56.
The mediating effect of social intelligence on the association between social anxiety and mental health
Our study revealed significant relationships between social anxiety, social intelligence, and mental health. Social anxiety was negatively associated with social intelligence and mental health, while social intelligence was positively related to mental health. These findings aligned with previous research highlighting the detrimental impact of social anxiety on mental health and the positive influence of social intelligence on psychological functioning57,58. Prior research indicates that social anxiety hampers social interactions and decreases mental health, while social intelligence enhances social connections and contributes to positive mental health57,58. The study emphasizes the importance of addressing social anxiety and promoting social intelligence to improve mental health among nursing students.
Based on the SCM theory, our study examined the mediating role of social intelligence in the relationship between social anxiety and mental health among Chinese nursing students. The results indicated a significant negative indirect effect of social anxiety on mental health through social intelligence as a mediator. Specifically, higher levels of social anxiety were associated with lower levels of social intelligence, which, in turn, were associated with lower levels of mental health. Our findings added further support to the SCM theoretical framework, in which nursing students encountered social anxiety as a primary stressor and evaluated its negative impact on their mental health (primary appraisal). Then, they utilized social intelligence as a coping resource to alleviate the adverse effects of the primary stressor (secondary appraisal), which ultimately led to improved mental health.
The mediation model underscores the pivotal role of social intelligence in aiding nursing students in navigating social pressures and fostering mental well-being. Social intelligence is a multi-component global capacity encompassing intellectual, personal, communicative, and behavioral traits that are closely related to individual characteristics and interpersonal relationships59. Social intelligence plays a crucial role in medical fields as it shapes the level of empathic tendencies and the type of interpersonal relations with the patients60. For nursing students, it determines the peculiarities of their interactions and communication with patients and their effectiveness in providing appropriate care60. Therefore, nursing students with higher levels of social intelligence have better knowledge, skills, and competency in their future professional careers.
These theoretical insights substantiate our findings and offer implications for the cultivation and improvement of social intelligence among nursing students to improve their mental health. Our results have implications for nursing education, suggesting the integration of interventions to promote social intelligence skills among students and enhance their subjective well-being. Specifically, ongoing training curriculums and educational programs related to social intelligence promotion should be provided to all nursing students to ensure sustained personal development and career improvement. Education and training not only enhance nursing students’ knowledge and skills in social interaction and interpersonal relationships but also promote confidence and competency in their future clinical work, leading to improved mental health. In addition, it is suggested that social intelligence should be included as a critical evaluation indicator for academic performance to evaluate nursing students’ level of preparation and academic readiness to become a nurse in the future. Clinical internships can benefit from addressing social anxiety and fostering social intelligence to enhance students’ well-being in healthcare settings. Integrating social intelligence development into the curriculum and evaluation can further promote nursing students’ mental health and better prepare them for their future professional practice.
The study has several limitations that need to be acknowledged. First, the cross-sectional study design precludes the establishment of causal relationships among variables, which warrants future longitudinal study designs. Second, the nursing students were recruited from one university in Henan province, China, and may not represent nursing students from other universities in other areas. Future mufti-center studies across various parts of China are needed to test our findings in a more diverse population. Third, a convenient sampling method was used to select the study settings and participants, possibly creating a selection bias. Future studies should consider using a random sampling method to get a more representative sample. Finally, the self-reported data may result in inaccurate results due to social desirability bias. Future studies should consider combining both self-reported data and objective indicators to get a more accurate assessment and increase the reliability of research results.
Conclusions
In summary, our study showed that undergraduate nursing students had moderate levels of social anxiety, social intelligence, and mental health, which varied according to their profile characteristics. Social anxiety was significantly associated with mental health both directly and indirectly through social intelligence. It underscores how decreased social anxiety may contribute to improved social intelligence, which may further lead to improved mental health. Our study offers fresh insights into the impact of social anxiety on mental health and sheds light on the intricate mediating role of social intelligence. These findings offer valuable insights for research and clinical endeavors aimed at formulating psychosocial interventions to enhance the mental health of nursing students.
References
American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5®) (Am. Psychiatric Pub, 2013).
Morrison, A. S. et al. Empathy for positive and negative emotions in social anxiety disorder. Behav. Res. Ther. 87, 232–242. https://doi.org/10.1016/j.brat.2016.10.005 (2016).
Stein, D. J. et al. The cross-national epidemiology of social anxiety disorder: Data from the World Mental Health Survey Initiative. BMC Med. 15, 143. https://doi.org/10.1186/s12916-017-0889-2 (2017).
Jefferies, P. & Ungar, M. Social anxiety in young people: A prevalence study in seven countries. PLoS ONE 15, e0239133. https://doi.org/10.1371/journal.pone.0239133 (2020).
Pilkioniene, I., Sirvinskiene, G., Zemaitiene, N. & Jonyniene, J. Social anxiety in 15–19 year adolescents in association with their subjective evaluation of mental and physical health. Child. (Basel). https://doi.org/10.3390/children8090737 (2021).
Ho, J. T. K. & Moscovitch, D. A. The moderating effects of reported pre-pandemic social anxiety, symptom impairment, and current stressors on mental health and affiliative adjustment during the first wave of the COVID-19 pandemic. Anxiety Stress Coping 35, 86–100. https://doi.org/10.1080/10615806.2021.1946518 (2022).
Qazi, N. O., Khizar, U. & Baloch, U. Impact of social anxiety and humor styles on Mental Health. Pak. J. Humanit. Social Sci. 9, 292–297 (2021).
World Health Organization. Promoting Mental Health: Concepts, Emerging Evidence, Practice (Summary Report) (World Health Organization, 2004).
Hossain, M. M. et al. Epidemiology of mental health problems in COVID-19: A review. F1000Res 9, 636. https://doi.org/10.12688/f1000research.24457.1 (2020).
Campbell, F. et al. Factors that influence mental health of university and college students in the UK: A systematic review. BMC Public. Health. 22, 1778. https://doi.org/10.1186/s12889-022-13943-x (2022).
Cheng, C., Ying, W., Ebrahimi, O. V. & Wong, K. F. E. Coping style and mental health amid the first wave of the COVID-19 pandemic: A culture-moderated meta-analysis of 44 nations. Health Psychol. Rev. 18, 141–164. https://doi.org/10.1080/17437199.2023.2175015 (2024).
Cornine, A. Reducing nursing student anxiety in the clinical setting: An integrative review. Nurs. Educ. Perspect. 41, 229–234. https://doi.org/10.1097/01.NEP.0000000000000633 (2020).
Simpson, M. G. & Sawatzky, J. V. Clinical placement anxiety in undergraduate nursing students: A concept analysis. Nurse Educ. Today. 87, 104329. https://doi.org/10.1016/j.nedt.2019.104329 (2020).
Reghuram, R. M. A study on occurrence of social anxiety among nursing students and its correlation with professional adjustment in selected nursing institutions at Mangalore. J. Health Allied Sci. NU. 4, 064–069 (2014).
Choi, S. H. Effect of perceived stress and anxiety, depression on suicide ideation of junior nursing students. J. Convergence Cult. Technol. 8, 15–22 (2022).
Thorndike, E. L. Intelligence and its use. Harper’s Magazine. 140, 227–235 (1920).
Saxena, S. J. Social intelligence of undergraduate students in relation to their gender and subject stream. J. Res. Method Educ. 1, 1–4 (2013).
Marlowe, H. A. Social intelligence: Evidence for multi dimensionality and construct independence. J. Educ. Psychol. 78, 52–58 (1986).
Handa, D. S. Intelligence cultural intelligence and occupational success: A review of literature. IUP J. Soft Skills 12 (2018).
Moeller, R. W., Seehuus, M. & Peisch, V. Emotional intelligence, belongingness, and mental health in college students. Front. Psychol. 11, 93. https://doi.org/10.3389/fpsyg.2020.00093 (2020).
Dehghan, F., Kaboudi, M., Alizadeh, Z. & Heidarisharaf, P. The relationship between emotional intelligence and mental health with social anxiety in blind and deaf children. Cogent Psychol. 7, 1716465 (2020).
Özdemir, N. & Adıgüzel, V. The relationship between social intelligence, self-esteem and resilience in healthcare professionals and the affecting factors. J. Psychiatric Nurs. (2021).
Cejudo, J., Rodrigo-Ruiz, D., Lopez-Delgado, M. L. & Losada, L. Emotional Intelligence and its relationship with levels of social anxiety and stress in adolescents. Int. J. Environ. Res. Public. Health 15 https://doi.org/10.3390/ijerph15061073 (2018).
Pittelkow, M. M., Het Rot, A., Seidel, M., Feyel, L. J., Roest, A. M. & N. & Social anxiety and empathy: A systematic review and Meta-analysis. J. Anxiety Disord. 78, 102357. https://doi.org/10.1016/j.janxdis.2021.102357 (2021).
Lazarus, R. S. & Folkman, S. Transactional theory and research on emotions and coping. Eur. J. Pers. 1, 141–169 (1987).
Lazarus, R. S. & Folkman, S. Stress, Appraisal, and Coping (Springer publishing company, 1984).
Israel, G. D. Determining Sample Size (University of Florida, 1992).
Del Ponte, A., Li, L., Ang, L., Lim, N. & Seow, W. J. Evaluating SoJump. Com as a tool for online behavioral research in China. J. Behav. Exp. Financ. 100905 (2024).
Fenigstein, A., Scheier, M. F. & Buss, A. H. Public and private self-consciousness: Assessment and theory. J. Consult. Clin. Psychol. 43, 522–527 (1975).
Scheier, M. F. & Carver, C. S. Optimism, coping, and health: Assessment and implications of generalized outcome expectancies. Health Psychol. 4, 219–247 (1985).
Hu, B., Wang, Y., Zhou, H. T., Li, M. & Zheng, L. A study on the impact of mental health problems on the academic buoyancy of medical students and the mechanisms. Front. Public. Health 11, 1229343. https://doi.org/10.3389/fpubh.2023.1229343 (2023).
Silvera, D. H., Martinussen, M. & Dahl, T. I. The Tromso Social Intelligence Scale, a self-report measure of social intelligence. Scand. J. Psychol. 42, 313–319. https://doi.org/10.1111/1467-9450.00242 (2001).
Guo, W. Translation and analysis of the Chinese version of the ThromsΦ Social Intelligence Scale and intervention on social intelligence among undergraduate nursing students (Doctoral dissertation, Nanhua University) (2013).
Topp, C. W., Ostergaard, S. D., Sondergaard, S. & Bech, P. The WHO-5 well-being index: A systematic review of the literature. Psychother. Psychosom. 84, 167–176. https://doi.org/10.1159/000376585 (2015).
Fung, S. F. et al. Validity and psychometric evaluation of the Chinese Version of the 5-Item WHO well-being index. Front. Public. Health. 10, 872436. https://doi.org/10.3389/fpubh.2022.872436 (2022).
Hayes, A. F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach (Guilford Publications, 2017).
Dong, Z., Zhou, S., Case, A. S. & Zhou, W. The relationship between perceived parenting style and social anxiety: A meta-analysis of mainland Chinese Students. Child. Psychiatry Hum. Dev. 55, 247–261. https://doi.org/10.1007/s10578-022-01399-4 (2024).
Li, W., Zhao, Z., Chen, D., Peng, Y. & Lu, Z. Prevalence and associated factors of depression and anxiety symptoms among college students: A systematic review and meta-analysis. J. Child. Psychol. Psychiatry. 63, 1222–1230. https://doi.org/10.1111/jcpp.13606 (2022).
Liu, T., Yang, B., Geng, Y. & Du, S. Research on face recognition and privacy in China-based on social cognition and cultural psychology. Front. Psychol. 12, 809736. https://doi.org/10.3389/fpsyg.2021.809736 (2021).
Wu, M. S., Zhou, C., Chen, H., Cai, H. & Sundararajan, L. Cultural value mismatch in urbanizing China: A large-scale analysis of collectivism and happiness based on social media and nationwide survey. Int. J. Psychol. 53 (Suppl 2), 54–63. https://doi.org/10.1002/ijop.12523 (2018).
Zhou, L. R., Guo, W. & Wan, Y. P. Analysis of the current situation and influencing factors of social intelligence in clinical nurses. J. Shanxi Nurs. 4, 1190–1192 (2014).
Li, Y., Wang, A., Wu, Y., Han, N. & Huang, H. Impact of the COVID-19 pandemic on the mental health of college students: A systematic review and meta-analysis. Front. Psychol. 12, 669119. https://doi.org/10.3389/fpsyg.2021.669119 (2021).
Ma, C. & An Empirical Study on the Psychological Health Level of Post. Based on Nearly 20,000 Freshman Students in 2018 (in Chinese). Ideol. Theor. Educ. 480, 97–101 (2019).
Li, Y. et al. Mental health among college students during the COVID-19 pandemic in China: A 2-wave longitudinal survey. J. Affect. Disord. 281, 597–604 (2021).
Ma, Y. & Bennett, D. The relationship between higher education students’ perceived employability, academic engagement and stress among students in China. Educ. Train. 63(5), 744–762 (2021).
Mirza, A. A., Baig, M., Beyari, G. M., Halawani, M. A. & Mirza, A. A. Depression and anxiety among medical students: A brief overview. Adv. Med. Educ. Pract. 202(21), 393–398 .
Cheng, Y., Zhang, X. M., Ye, S. Y., Jin, H. M. & Yang, X. H. Suicide in Chinese graduate students: A review from 2000 to 2019. Front. Psychiatry. 11, 579745. https://doi.org/10.3389/fpsyt.2020.579745 (2020).
Abbruzzese, L., Magnani, N., Robertson, I. H. & Mancuso, M. Age and gender differences in emotion recognition. Front. Psychol. 10, 2371. https://doi.org/10.3389/fpsyg.2019.02371 (2019).
Salavera, C., Usán, P. & Jarie, L. Styles of humor and social skills in students. Gender differences. Curr. Psychol. 39, 571–580 (2020).
Archbell, K. A. & Coplan, R. J. Too anxious to talk: Social anxiety, academic communication, and students’ experiences in higher education. J. Emot. Behav. Disord. 30, 273–286 (2022).
Ye, J. An analysis of the relationship between career decision-making self-efficacy and career selection anxiety of senior students. In Innovative Computing: IC 35–44 (Springer Singapore, 2020).
Kalkbrenner, M. T., Jolley, A. L. & Hays, D. G. Faculty views on college student mental health: Implications for retention and student success. J. Coll. Student Retention: Res. Theory Pract. 23, 636–658 (2021).
Huang, S. et al. Does meaning in life mediate the relationship between proactive personality and well-being? Social Behav. Personality. 48, 1–9 (2020).
Kim, E. K., Furlong, M. J. & Dowdy, E. Adolescents’ personality traits and positive psychological orientations: Relations with emotional distress and life satisfaction mediated by school connectedness. Child Indic. Res. 12, 1951–1969 (2019).
Fan, H. et al. Parents’ personality traits and children’s subjective well-being: A chain mediating model. Curr. Psychol. 1–12 (2020).
Segrin, C. & Flora, J. Fostering social and emotional intelligence: What are the best current strategies in parenting? Soc. Pers. Psychol. Compass. 13, e12439 (2019).
Haslam, C. et al. GROUPS 4 HEALTH reduces loneliness and social anxiety in adults with psychological distress: Findings from a randomized controlled trial. J. Consult. Clin. Psychol. 87, 787 (2019).
Lesani, M. D., Makvandi, B., Naderi, F. & Hafezi, F. Relationship of self-differentiation and social intelligence with happiness by mediating role of difficulty in cognitive emotion regulation among female-headed households. Middle East. J. Rehabili. Health Stud. 7 (2020).
Kunitsyna, V. N., Kazarinova, N. V. & Pogolsha, V. M. Interpersonal Communication: Textbook for Universities (St. Petersburg, 2001).
Melnychuk, T., Onufriieva, L., Chaikovska, O., Kobets, O. & Pavelkiv, R. Social intelligence as a factor of volunteer activities by future medical workers. J. Hist. Cult. Art Res. 1(9), 84–95 (2020).
Author information
Authors and Affiliations
Contributions
Conceptualization, Qiangwei, Bai; Data curation, Jingjing Wang and Zhenti Cui; Investigation, Qiangwei Bai; Methodology, Qiangwei Bai and Jingjing Wang; Resources, Rui Hou; Software, Zhenti Cui; Validation, Jingjing Wang; Writing – original draft, Qiangwei Bai; Writing – review & editing, Qiangwei Bai and Zhenti Cui.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bai, Q., Cui, Z., Hou, R. et al. The mediating effect of social intelligence in the association between social anxiety and mental health among Chinese nursing students. Sci Rep 14, 27208 (2024). https://doi.org/10.1038/s41598-024-78637-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-78637-3
