
Abstract
Ischemic heart disease (IHD) is a leading cause of death in cardiovascular patients. In China, the disease burden of IHD deaths has significantly increased. One of the main influencing factors of IHD is changing climates, and temperature and diurnal temperature range (DTR) are important indicators of climate change. In this study, we aimed to assess the associations of temperature variability on IHD mortality in a fast developing city Hangzhou,China. We obtained daily IHD mortality data and meteorological data from mortality surveillance system from 2014 to 2016. Quasi-Poisson generalized linear regression with a distributed lag non-linear model (DLNM) was applied to estimate the associations between temperature variability and IHD deaths. Potential confounders were controlled in the analysis, including relative humidity, day of the week, public holidays, and long-term trends. A total of 7423 IHD mortality data were included in this study. A J-shaped pattern of DTR and a reversely J-shaped pattern of temperature for IHD mortality were observed. Risk estimates showed that the relative risks (RRs) of IHD mortality with extreme high DTR at lag 0–7 days were 1.309 (95% CI: 0.985, 1.740) while RRs of IHD mortality with extreme low DTR at lag 0–2 days were 1.234 (95% CI: 1.043, 1.460). For extreme hot temperature, the highest RRs at lag 0–2 days were 1.559 (95% CI: 1.250, 1.943); for extremely cold temperatures, the RRs increased from 1.049 (95% CI: 0.930, 1.183) to 2.089 (95% CI: 1.854, 2.352). In Hangzhou city, short-term exposure to extreme temperature was associated with mortality for IHD. These findings have implications for policy decision-making and targeted interventions.
Similar content being viewed by others
Introduction
Cardiovascular disease (CVD) accounts for approximately one-third of global deaths1. CVD encompasses conditions affecting the vascular system supplying the heart, brain, and other vital organs2. Among these, ischemic heart disease (IHD) stands as the most prevalent cardiovascular disease3. IHD results from insufficient oxygen delivery to meet the heart’s demands, often presenting as angina, acute myocardial infarction, and ischemic heart failure4. Merely 2–7% of the general population exhibit no IHD risk factors, while over 70% of high-risk individuals have multiple risk factors5. Despite its global prominence and substantial impact on population health, the correlation between IHD mortality rates and environmental risk factors remains inadequately explored.
In recent years, climate change has emerged as a pressing environmental public health concern, particularly with the escalating incidence of global warming6 and extreme weather events7. Among meteorological factors, temperature has received widespread attention. It’s widely acknowledged that rising temperatures escalate the risk of adverse health outcomes8, ranging from mild subclinical conditions to severe fatal events9. Heat exposure is an important but underappreciated risk factor contributing to cardiovascular disease10, particularly for those already afflicted by cardiovascular diseases. Increased temperatures can elevate blood pressure, augment blood viscosity, and amplify cardiac workload, consequently increasing the incidence of cardiovascular events.
Diurnal temperature range (DTR) denotes the disparity between the maximum and minimum temperatures observed within a specific location over a single day11. Studying DTR is pivotal for comprehending climate patterns and their effects on ecosystems, agriculture, human health12, and various environmental facets13. Alterations in DTR can substantially impact ecological environment, crop cultivation, energy consumption, and the occurrence of weather-related health issues. Increasing epidemiological studies have shown that a rapid temperature change within a day is an independent risk factor for human health14. Nevertheless, in China, scant studies have delved into the effects of temperature variability on IHD mortality.
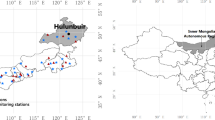
Hangzhou, situated in the southeastern coastal area of China’s Zhejiang Province, serves as the provincial capital and a hub for politics, economics, culture, and transportation within the province. Nestled on the southern bank of the Qiantang River15, adjacent to the East China Sea, Hangzhou lies within the Yangtze River Delta Economic Zone. The city experiences a subtropical monsoon climate characterized by four distinct seasons: sultry and humid summers, mild and pleasant springs and autumns, and chilly and damp winters. The rapid economic expansion and burgeoning population exert profound influence on the trajectories of annual average and extreme temperature indices16. Therefore, studying temperature variability has become an urgent task. Consequently, this research endeavors to scrutinize the correlation between daily mean temperature and Diurnal Temperature Range (DTR) as representative indicators of temperature variation, and mortality from IHD. Using daily meteorological data and mortality statistics from Hangzhou, China to explore this association through time-series analysis.
Methods
Ethics declarations
The Ethics Committee of Zhejiang Provincial Center for Disease Control and Prevention approved the procedures performed in this study in July 22, 2022 with a waiver of informed consent. Informed consent was not required since the data came from anonymous datasets typically used for administrative purpose, and data were analysed at aggregate level without any personal information and not transferable. All methods were carried out in accordance with relevant guidelines and regulations.
Mortality data
Daily data on IHD deaths were retrieved from the mortality surveillance system of Zhejiang Provincial Center for Disease Prevention and Control from 1 January 2014 to 31 December 2016. IHD deaths were classified according to the International Classification of Diseases and Related Health Problems, 10th revision (ICD-10,120–125). Moreover, demographic information (including age and gender) was also collected from the surveillance system.
Meteorological and air pollution data
Daily meteorological data including temperature and relative humidity were obtained from Zhejiang Meteorological Bureau during the study period. Daily mean temperature was the 24-h average temperature. DTR can be calculated in each day from maximum temperature and minimum temperature by means of:
Over the same period, daily air pollution data on particulate matter less than 2.5 μm in aerodynamic diameter (PM2.5), nitrogen dioxide (NO2) and sulfur dioxide (SO2) were obtained from eight environmental monitoring stations in urban areas. The 24-h average concentrations were applied for air pollutants.
Statistical analysis
Frist, a descriptive review of the distribution of IHD deaths, pollutant datasets, and meteorological were presented, then the data were summarized as the mean, standard deviation, and percentile for continuous variables, as well as the absolute and relative frequencies for categorical variables. Next, time series analysis is applied to estimate the relationship between temperature exposure and IHD deaths.
Daily IHD deaths are a small probability event for the general population, with a statistical distribution similar to the Poisson distribution. Thus, this study used a Poisson generalized linear model (GLM) for time series data, which incorporated a distributed lag nonlinear model (DLNM) with natural cubic spline function and a maximum lag of 7 days to account for the relationship between delay and non-linear effects17,18. Specifically, we modeled the cross-basis function for the lag effect on mortality or morbidity for temperature at different day.
The quasi-Akaike information criterion (QAIC) was used for model selection to determine the number of degrees of freedom (df) for temperature and DTR19. The lowest QAIC determined the best model.
Thereafter, 3 df for temperature and lag were adopted, and the df for DTR and lag were set to 3 as they would generate the best model, as well as df for long-term trend was 2 df per year. Besides, the moving average of lag 0–3 and relative humidity were adjusted using a natural cubic spline with 3 degrees of freedom. We also adjusted for the control variables mentioned in previous studies, including the day of the week and public holidays20. In this study, the model used is represented by equation:
where, μt is the daily death number of IHD on specific day t; α and β represents the intercept of the model and the vector of the coefficient for DTR, respectively; γ refers to the vector of the coefficient for temperature. The minimum mortality temperature with the lowest risk was defined as the reference value21, and the 99th percentile of the data distribution were treated as the extreme high temperature and extreme DTR. To evaluate cumulative the time lag and correlation between temperature change and IHD deaths, we calculated relative risks (RRs) and 95% confidence intervals (CIs) of the data, followed by conducting age stratification analysis with the purpose of investigating whether there is a potential differential association between subgroups of exposure22. Seasonal modification for DTR was also examined. Consistent with the previous literature, warm season was defined as April to September, and cold season was defined as October to March23. The 95% CI was used to test the significant difference between subgroups.
Several sensitivity analyses were performed to assess the robustness of our results. On the one hand, we varied the df of calendar time and relative humidity to examine the relative risks of temperatures. On the other hand, We chose to include PM2.524, NO2, and SO225 in the model based on their known associations with cardiovascular disease, including ischemic heart disease. These pollutants are well-documented in the literature as major contributors to air quality-related health risks. Additionally, they are routinely monitored in Hangzhou, ensuring the availability of high-quality data. Other pollutants, such as CO or O3, were not included due to data limitations or lesser relevance to the health outcomes studied.
All the statistical analyses were performed using R software (4.1.0). Statistical significance was considered when a two-sided p value was less than 0.05 (p < 0.05).
Results
Descriptive analysis
Table 1 presents a concise overview of the study population, air pollutants, and meteorological conditions. Over the survey period spanning from January 1, 2014, to December 31, 2016, encompassing 1096 days, a total of 7423 deaths were documented within the study area, averaging 6.79 deaths per day (standard deviation, SD: 3.03). Usually, individuals aged 65 and above, commonly categorized as elderly, comprised a substantial proportion of the deceased, accounting for 92.12% of all recorded deaths. Among the deceased, males constituted 52.46% of the total, slightly outnumbering females at 47.54%.
The daily mean concentrations of PM2.5, NO2, and SO2 stood at 56.83 μg/m3 (ranging from 8.00 to 228.56 μg/m3), 47.9 μg/m3 (ranging from 10.89 to 118.30 μg/m3), and 16.29 μg/m3 (ranging from 4.33 to 81.20 μg/m3), respectively, in Hangzhou, China. Furthermore, the daily mean temperature averaged at 17.77 °C (ranging from − 5.00 to 34.40 °C), with a diurnal temperature range (DTR) of 7.57 °C (ranging from 0.90 to 18.50 °C), and a relative humidity of 74.41% (ranging from 27.00 to 98.00%).
Table 2 illustrates the Spearman correlation coefficients between weather conditions and key pollutants. The criteria for interpreting correlation coefficients were established based on previous research (low for |r|< 0.4; moderate for 0.4 ≤|r|≤ 0.6; high for |r|> 0.6)26. Notably, air pollutants exhibited strong intercorrelations, while demonstrating only slight correlations with IHD deaths. Daily mean temperature displayed negative correlations with both IHD deaths and air pollutants. Conversely, there were low correlations observed between DTR and both air pollutants and temperature. Relative humidity exhibited a slight negative correlation with both IHD deaths and air pollutants, yet demonstrated a notably high negative correlation with DTR.
Time‑lag and cumulative effects
Figure 1 depicts a three-dimensional graph illustrating the RRs for IHD deaths concerning DTR and temperature across various lag days. The results indicate a non-linear exposure–response relationship with increased RRs observed at both high and low temperatures. Moreover, high DTR appears to mitigate adverse effects on IHD deaths, while substantial temperature increases exhibit delayed adverse effects on IHD deaths.

Relative risk of IHD death with DTR and temperature in lags (lag 0 to lag 7 day).
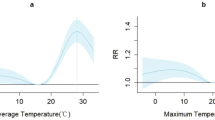
Figure 2 presents exposure–response curves detailing the cumulative effects over 7 days of both DTR and temperature on IHD deaths. The association between DTR and IHD deaths exhibits a J-shaped pattern, while the association with temperature demonstrates a reverse J-shaped pattern, with no clear threshold identified. Using median values as reference points, the minimum mortality temperature for DTR and temperature were found to be 6.5 °C and 22.0 °C, respectively. Subsequently, these values were used as references for further analysis.

Cumulative effects of DTR and temperature at lag 0–7 on IHD death.
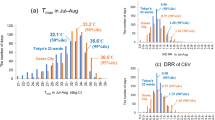
Figure 3 illustrates the cumulative effects of extremely DTR and temperature over a 7-days period. Regarding DTR, a steadily increasing association was observed between extreme high DTR (99th percentile: 16.0 °C) and IHD deaths throughout the lag period, with a significant association noted in lag 0–7 days (RR = 1.309, 95% CI: 0.985, 1.740). Conversely, the greatest RR was observed between extreme low DTR (1st percentile: 1.4 °C) and IHD deaths in lag 0–2 days (RR = 1.234, 95% CI: 1.043, 1.460). Similarly, temperature (1st percentile: 1.86 °C; 99th percentile: 33.0 °C) displayed significant associations with IHD deaths across the entire lag period, with the highest RR observed at lag 0–2 days (RR = 1.559, 95% CI: 1.250, 1.943) for extremely hot temperatures. Conversely, for extremely cold temperatures, the RR increased from 1.049 (95% CI: 0.930, 1.183) to 2.089 (95% CI: 1.854, 2.352).

Cumulative effects of extremely DTR and temperature over 7 days at various lag structures.
Table 3 presents an analysis of the overall cumulative effect among various sub-groups based on gender and age. The subgroup classifications in Table 3 were based on demographic factors that are commonly associated with differential health impacts in relation to temperature and DTR. We included age and gender as these are well-established factors influencing vulnerability to temperature-related health outcomes. Specifically, elderly individuals are at higher risk due to age-related physiological changes, and gender differences may arise from both biological and behavioral factors. These criteria align with similar studies on temperature-related health effects. Notably, females exhibited greater susceptibility than males across different lag days, except for extreme high DTR, although no significant associations were found when comparing both extreme DTR and temperature with IHD deaths. In terms of age, the elderly demonstrated stronger sensitivity compared to the younger population.
Sensitivity analysis
To test the robustness of our results, several sensitivity analyses were conducted and presented in Table 4. Initially, we adjusted the df from 3 to 5 for long-term and seasonal trends, 4–7 for relative humidity. The results indicated minimal changes in the estimation values, suggesting that our findings remained stable. Furthermore, we conducted sensitivity analyses by incorporating additional air pollutants into the model. Overall, when PM2.5 and NO2 were added to the model, the RRs slightly decreased, whereas the inclusion of SO2 led to a moderate increase in RRs. However, these adjustments did not significantly alter the results. Consequently, we have confidence that the model specifications employed in our study accurately reflect the main effects of DTR and temperature on IHD deaths.
Discussions
Hangzhou is located in the southeastern coastal region of China and has a subtropical monsoon climate with distinct seasons. Summers are characterized by high temperatures and humidity, while winters are relatively mild. The study finds that extreme temperatures and humidity can significantly impact cardiovascular health. In particular, high temperatures may increase the burden on the cardiovascular system, leading to a higher incidence of IHD. Additionally, high humidity environments may affect air quality, further exacerbating the risk of cardiovascular diseases. We believe that the combined effects of these geographical and environmental factors provide important contextual information for understanding the variations in IHD incidence in Hangzhou and help explain some of the observed phenomena in the study results.
This study investigated the association between DTR and temperature changes and IHD mortality in Zhejiang, China, from 2014 to 2016. Generally, the correlation between DTR and IHD deaths shows a non-linear (J-shaped) trend, while a reverse J-shaped trend is observed in the effect of temperatures. We then examined the lag effects on IHD deaths. For DTRs, we found that low DTR had almost no influence on RR, while high DTR led to a cumulative effect over the lag period. Regarding temperatures, we found that low temperature also accumulated RR over 7 days, while only a limited cumulative effect was observed for high temperature, which ended on the third lag day. Furthermore, no significant differences were found between gender and age, and the introduction of different pollutants, including PM2.5, NO2, and SO2, did not significantly confound the results.
Currently, extensive attention has been paid to the association of DTR with mortality27,28. However, to our best knowledge, few studies have examined how extreme DTR affects mortality risk from IHD. Our study provides more generalized evidence to support the effects of DTR on IHD. Specifically, we found a non-linear (J-shaped) association between DTR and IHD deaths. Additionally, our study identified the cumulative effect of extremely low DTR, which persisted throughout the lag period, while the effect of high DTR was immediate and limited. This result is consistent with a previous study in Jiuquan, which found that the effect of low DTR was significantly more deleterious than that of high DTR on hospital admissions29. A study in Guangdong also examined the cumulative effects of extreme DTRs, which were greater for extreme high DTRs than those of extreme low DTRs30. Generally, the prior conclusions regarding the association between DTR and daily mortality were not coherent. Some reported a linear relationship between DTR and mortality31, which was different from our results. However, some observed a non-linear (J-shaped) relationship between DTR and cardiovascular-specific mortality32,33,which agrees with our findings. The results of these studies support that extreme DTR is a risk factor for IHD, and the different effects might be explained by the area characteristics and differences in analytic approaches34.
In recent years, the study on the relationship between temperature and disease has received widespread attention from researchers. In general, correlations between daily main temperature and death present non-linear trends, mostly showing "U", “V” or “J” shapes35. A study in Taiwan found a U-shaped relation with temperature for CAD, and cold climates resulted in a reduction of the least temperature range for elderly death36. Another study in Hubei found that low temperature increased the risk of IHD deaths, while no effect of high temperature on IHD death was observed35. Overall, previous studies have suggested that extremely cold and hot temperatures should be considered to affect IHD mortality, but many ignored the lag effects. Consistent with the majority of existing evidence, we detected a non-linear (reversely J-shaped) association between temperature and IHD mortality. Besides, the effects of low temperature could last for more than 7 days, while high temperature only maintained effects for 3 days. This was similar to a study in Guangzhou, which detected a cold effect on IHB that persisted for approximately 12 days, while the hot effect was limited to the first 5 days37. On the one hand, this may be attributed to the hypothesis of acclimatization to local climatic conditions38,39. And Zhejiang Province, as a southern city, its citizens are not sensitive to thermal effects. On the other hand, our findings are biologically plausible. When repeatedly exposed to heat stress, the failure of thermoregulation and the physiological changes in the circulatory system may lead to an increase in mortality40. However, considering the exact mechanism for the temperature-mortality relationship is uncertain to date, further investigation is needed.
Regarding influencing factors, some evidence has found that the magnitude of DTR and temperature effects might vary by gender and age. Several studies reported that males and the elderly showed more vulnerability to the adverse effects of DTR than females and the young for IHD mortality29,33,41, while some agreed that women and the elderly are more susceptible42. Besides, a previous study in Yuxi suggested no evidence for effect modification by gender30. Similarly, despite the slightly increased risk of IHD among females and the elderly, our research identified no significant discrepancies between males and females, as well as between the elderly and youth. The differences in extreme temperature and DTR effects on gender might rely on the research location and population43, and the susceptibility of elderly people may be due to their poor physiological adaptability to changes in ambient temperature. Further study in this field is needed to investigate these potential modifiers.
Many previous studies considered the potential confounding role of air pollutants on the effects of temperature variability on mortalities42,44,45. Accordingly, we introduced the confounding effects of various air pollutants, including PM2.5, NO2, and SO2, to our base models. But no significant changes were found in the results, indicating that air pollutants were not confounders in this study.
There were several strengths in this study. To our best knowledge, limited research simultaneously evaluated the impact of both extreme DTR and temperature on IHD-specific mortality. Additionally, we conducted modification analysis based on gender and age and incorporated humidity and ambient pollutants for subgroup analysis. This indicates that our study of the effects of extreme DTR and temperature on IHD mortality is systematic and comprehensive.
This research, however, is subject to several limitations. Firstly, the design of the current study is ecological study. The lack of individual data might result in factual deviations and insufficient evidence of causality. Besides, other potential confounders such as individual habits or medical history might affect the accuracy of results. Secondly, our data only collect from one single city, which might affect the extrapolation of the results, especially for regions with different geographic situations and climates. Thirdly, insufficient sample size for statistical measurement limited us from performing further subgroup analysis, such as socioeconomic status. Thus, in order to validate the above findings and elucidate their potential mechanisms, it is necessary to further explore diverse groups and more detailed factors, and establish sophisticated models based on more comprehensive data.
Conclusions
In summary, this study unveils a non-linear association between diurnal temperature range (DTR), temperature variability, and mortality from ischemic heart disease (IHD) in Hangzhou, China, with extreme temperature and DTR exhibiting a cumulative effect over the lag period. Gender and age were found not to significantly modify these associations. These findings hold significant implications for the public health department in Hangzhou, suggesting the need to adopt prevention and intervention strategies aimed at reducing exposure to extreme temperature and DTR. Additionally, our study provides insights for research in other Asian cities facing similar climate challenges. In the broader context of global climate change, our findings indicate that by enhancing our understanding of the intricate relationship between temperature variability and health outcomes, we can better equip ourselves to address the multifaceted challenges posed by a changing climate.
Data availability
The data supporting the findings of this study are available from the Mortality Surveillance System of the Zhejiang Provincial Center for Disease Prevention and Control. However, due to restrictions on data availability under license for this study, they are not publicly accessible. Access to the data may be granted upon reasonable request and with permission from the Mortality Surveillance System of the Zhejiang Provincial Center for Disease Prevention and Control. Due to privacy concerns regarding mortality data, it cannot be publicly disclosed at this time. For verification purposes, we can provide software screenshots. For inquiries regarding the data, please contact the corresponding author, Gaofeng Cai, at gfcai@cdc.zj.cn.
References
Mozaffarian, D. et al. Heart disease and stroke statistics-2016 update a report from the American Heart Association. Circulation 133, E38–E360 (2016).
Zhao, D., Liu, J., Wang, M., Zhang, X. & Zhou, M. Epidemiology of cardiovascular disease in China: Current features and implications. Nat. Rev. Cardiol. 16, 203–212 (2019).
Roth, G. et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J. Am. Coll. Cardiol. 70, 1–25 (2017).
Andreenko, E. et al. Ischemic heart disease in subjects of young age: Current state of the problem. Features of etiology, clinical manifestation and prognosis. Kardiologiya 58, 24–34 (2018).
Sampasa-Kanyinga, H. & Lewis, R. Frequent use of social networking sites is associated with poor psychological functioning among children and adolescents. Cyberpsychol. Behav. Soc. Netw. 18, 380–385 (2015).
Kaufman, D. & Broadman, E. Revisiting the Holocene global temperature conundrum. Nature 614, 425–435 (2023).
Weilnhammer, V. et al. Extreme weather events in europe and their health consequences: A systematic review. Int. J. Hyg. Environ. Health 233 (2021).
Ebi, K. et al. Extreme weather and climate change: population health and health system implications. In Annual Review of Public Health, Vol. 42, 2021 (ed. Fielding, J.) 293–315 (2021).
Kim, J. & Lee, J. Synoptic approach to evaluate the effect of temperature on pediatric respiratory disease-related hospitalization in Seoul, Korea. Environ. Res. 178 (2019).
Liu, J., Varghese, B. & Hansen, A. Heat exposure and cardiovascular health outcomes: A systematic review and meta-analysis. LANCET Planet. Health 6, E644–E644 (2022).
Braganza, K., Karoly, D. & Arblaster, J. Diurnal temperature range as an index of global climate change during the twentieth century. Geophys. Res. Lett. 31 (2004).
Davis, R., Hondula, D. & Sharif, H. Examining the diurnal temperature range enigma: Why is human health related to the daily change in temperature?. Int. J. Biometeorol. 64, 397–407 (2020).
Gallou, A. et al. Diurnal temperature range as a key predictor of plants’ elevation ranges globally. Nat. Commun. 14 (2023).
Cheng, J. et al. Impact of diurnal temperature range on human health: A systematic review. Int. J. Biometeorol. 58, 2011–2024 (2014).
Dai, L. et al. Pollution characteristics and source analysis of microplastics in the Qiantang River in southeastern China. Chemosphere 293 (2022).
Gu, C., Hu, L., Zhang, X., Wang, X. & Guo, J. Climate change and urbanization in the Yangtze River Delta. Habitat Int. 35, 544–552 (2011).
Gasparrini, A., Armstrong, B. & Kenward, M. G. Distributed lag non-linear models. Stat. Med. 29, 2224–2234 (2010).
Armstrong, B. Models for the relationship between ambient temperature and daily mortality. Epidemiology 17, 624–631 (2006).
Peng, R., Dominici, F. & Louis, T. Model choice in time series studies of air pollution and mortality. J. R. Stat. Soc. Ser. Stat. Soc. 169, 179–198 (2006).
Alahmad, B., Shakarchi, A., Alseaidan, M. & Fox, M. The effects of temperature on short-term mortality risk in Kuwait: A time-series analysis. Environ. Res. 171, 278–284 (2019).
Gasparrini, A. et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 386, 369–375 (2015).
Schenker, N. & Gentleman, J. On judging the significance of differences by examining the overlap between confidence intervals. Am. Stat. 55, 182–186 (2001).
Guo, H. et al. Short-term exposure to nitrogen dioxide and outpatient visits for cause-specific conjunctivitis: A time-series study in Jinan, China. Atmos. Environ. 247 (2021).
Hayes, R. B. et al. PM2.5 air pollution and cause-specific cardiovascular disease mortality. Int. J. Epidemiol. 49 (2020).
Yang, B.-Y. et al. Association of long-term exposure to ambient air pollutants with risk factors for cardiovascular disease in China. Environ. Health.
Li, D., He, R., Liu, P. & Jiang, H. Di erential e ects of size-specific particulate matter on the number of visits to outpatient fever clinics: A time-series analysis in Zhuhai, China. Front. Public Health.
Zhang, Y., Peng, M., Wang, L. & Yu, C. Association of diurnal temperature range with daily mortality in England and Wales: A nationwide time-series study. Sci. Total Environ. 619, 291–300 (2018).
Kim, J. et al. Comprehensive approach to understand the association between diurnal temperature range and mortality in East Asia. Sci. Total Environ. 539, 313–321 (2016).
Zhai, G., Zhang, J., Zhang, K. & Chai, G. Impact of diurnal temperature range on hospital admissions for cerebrovascular disease among farmers in Northwest China. Sci. Rep. 12 (2022).
Luo, Y. et al. Lagged effect of diurnal temperature range on mortality in a subtropical megacity of China. PLoS ONE 8, e55280 (2013).
Lim, Y.-H., Park, A. K. & Kim, H. Modifiers of diurnal temperature range and mortality association in six Korean cities. Int. J. Biometeorol. 56, 33–42 (2012).
Ding, Z. et al. Impact of diurnal temperature range on mortality in a high plateau area in southwest China: A time series analysis. Sci. Total Environ. 526, 358–365 (2015).
Tang, J. et al. Effects of diurnal temperature range on mortality in Hefei city. China. Int. J. Biometeorol. 62, 851–860 (2018).
Bao, J., Wang, Z., Yu, C. & Li, X. The influence of temperature on mortality and its Lag effect: a study in four Chinese cities with different latitudes. BMC Public Health 16 (2016).
Zhang, Y. et al. The short-term effect of ambient temperature on mortality in Wuhan, China: A time-series study using a distributed lag non-linear model. Int. J. Environ. Res. Public. Health 13, 722 (2016).
Pan, W., Li, L. & Tsai, M. Temperature extremes and mortality from coronary heart-disease and cerebral infarction in elderly Chinese. Lancet 345, 353–355 (1995).
Yang, J., Ou, C.-Q., Ding, Y., Zhou, Y.-X. & Chen, P.-Y. Daily temperature and mortality: A study of distributed lag non-linear effect and effect modification in Guangzhou. Environ. Health 11, 63 (2012).
McMichael, A., Woodruff, R. & Hale, S. Climate change and human health: Present and future risks. Lancet 368, 842–842 (2006).
Guo, Y. et al. Extremely cold and hot temperatures increase the risk of ischaemic heart disease mortality: Epidemiological evidence from China. Heart 99, 195–203 (2013).
Nixdorf-Miller, A., Hunsaker, D. & Hunsaker, J. Hypothermia and hyperthermia medicolegal investigation of morbidity and mortality from exposure to environmental temperature extremes. Arch. Pathol. Lab. Med. 130, 1297–1304 (2006).
Zha, Q., Chai, G., Zhang, Z., Sha, Y. & Su, Y. Effects of diurnal temperature range on cardiovascular disease hospital admissions in farmers in China’s Western suburbs. Environ. Sci. Pollut. Res. 28, 64693–64705 (2021).
Xiao, Y. et al. Short-term effect of temperature change on non-accidental mortality in Shenzhen, China. Int. J. Environ. Res. Public. Health 18 (2021).
Basu, R. High ambient temperature and mortality: a review of epidemiologic studies from 2001 to 2008. Environ. Health 8 (2009).
Hu, Y. et al. Season-stratified effects of meteorological factors on childhood asthma in Shanghai, China. Environ. Res. 191 (2020).
Zhang, T., Qin, W., Nie, T., Zhang, D. & Wu, X. Effects of meteorological factors on the incidence of varicella in Lu’an, Eastern China, 2015–2020. Environ. Sci. Pollut. Res. 30, 10052–10062 (2023).
Funding
This research was funded by the National Natural Science Foundation of China (82273749 and 81773468), the Natural Science Foundation of Zhejiang Province, China (LTGY23H240001), the Opening Foundation of NHC Key Laboratory of Etiology and Epidemiology (Harbin Medical University) (NHCKLEE20230908).
Author information
Authors and Affiliations
Contributions
Manjin Xu and Yunfeng Xu wrote the main manuscript text and Zhe Mo prepared Figs. 1–3 and tables 1–4. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mo, Z., Xu, M., Xu, Y. et al. The effects of temperature variability on ischemic heart disease mortality in Hangzhou, China. Sci Rep 14, 30168 (2024). https://doi.org/10.1038/s41598-024-78902-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-78902-5
Keywords
This article is cited by
-
The mortality of ischemic heart disease attributable to temperature variability: findings from the Global Burden of Disease Study 2021
BMC Cardiovascular Disorders (2025)
