
Abstract
The physiological and functional changes from aging affect the systemic and swallowing muscles. While ultrasound is used to examine muscle characteristics, no previous studies have examined the relationship between age and perioral and trunk muscle characteristics, including stiffness. This study aimed to investigate the relationship between age and the characteristics of perioral and trunk muscles, including quality, quantity, and stiffness, using ultrasound. A total of 215 participants were recruited for this cross-sectional study: 98 younger adults (20–64 years) and 117 older adults (≥ 65 years). Muscle characteristics were assessed along with data on age, sex, body mass index, and number of teeth. The correlation between age and muscle characteristics was examined. Multiple linear regression was performed with muscle characteristics as dependent variables and age, body mass index, and number of teeth as explanatory variables. We found that only trunk muscle stiffness was associated with age, with a stronger correlation in quality and quantity than perioral muscles. Masseter muscle quality and quantity showed a higher correlation with age than those of the geniohyoid muscle. In conclusion, characteristics of the trunk and perioral muscles exhibit differences in age-related changes, highlighting the importance of maintaining both trunk and perioral muscle activity in older adults to prevent functional decline.
Similar content being viewed by others

Introduction
Aging is the main factor for the physiological and functional changes that affect the mass, quality, and function of the skeletal muscles1,2, as well as swallowing-related muscles3. The masseter muscle, crucial for mastication, decreases in mass with age, leading to reduced occlusal force and chewing ability. This decline contributes to eating difficulties and increases the risk of malnutrition4. Similarly, the geniohyoid muscle, essential for the elevation of the hyoid bone and larynx closure during swallowing, experiences atrophy associated with aspiration in older adults5. The trunk muscles play a vital role in stabilizing the body and spine6 and maintaining proper posture during eating7. The deterioration of skeletal and swallowing-related muscles significantly contributes to sarcopenia and dysphagia, conditions that are linked to increased mortality rates in older adults8,9.
To prevent these issues, early screening for muscle atrophy using ultrasound is beneficial. Ultrasound is a widely used and reliable technique with high repeatability for examining the quantity, quality, and stiffness of muscles across populations, as it is affordable, non-invasive, and portable10,11. This makes ultrasound suitable for examining the masseter12, geniohyoid13, and abdominal muscles14, which are superficial and effectively measurable in older adults in community settings.
Many studies have shown a relationship between skeletal muscle mass and swallowing function. Skeletal muscle mass is closely linked to swallowing function, with low skeletal muscle mass as a predictor of dysphagia in hospitalized older patients15. Trunk muscle mass is more relevant to swallowing muscle function than appendicular muscle mass16. Homebound older adults who spend more time in bed tend to have lower swallowing function and lower trunk muscle mass17. Additionally, the perioral muscles are connected to systemic factors; for instance, the geniohyoid and tongue muscles are associated with grip strength and whole-body skeletal muscle mass, respectively18. The cross-sectional area of the geniohyoid muscle is also related to the mass of the trunk and skeletal muscles19. Masseter muscle thickness is related to sarcopenia and malnutrition20.
Recent studies have highlighted muscle stiffness as a novel area of interest in ultrasound research21,22, especially in the neurological patient population23,24 and people with temporomandibular problems25. Increased muscle stiffness weakens muscle contractile performance, affecting the mobility of older individuals26. Myotonometric measurements indicate that masseter muscle stiffness is associated with maximum bite force in healthy older adults27. However, there is still inadequate comprehensive research on muscle stiffness24, especially regarding the perioral muscles. Furthermore, no studies have examined differences in perioral and trunk muscle characteristics, including stiffness, in relation to age using ultrasound. To better understand the impact of aging on these muscles and search for early preventive measures, this study aimed to investigate the relationship between age and the characteristics of perioral and trunk muscles, focusing on their quality, quantity, and stiffness in a healthy population. We hypothesized that all muscle characteristics are significantly related to aging.
Materials and methods
Study design
In this cross-sectional study, the research protocol was explained, and informed consent was obtained from the participants before data collection. This study was approved by the Ethics Committee of the Tokyo Medical and Dental University (ref: D2017-063). All procedures performed in this study, which involved human participants, followed the ethical standards of the Institutional Research Committee and the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Participants
In accordance with the conventional definition used in Japan, people 65 years of age and older were considered to be part of the older population28. The participants were divided into two groups: young adults aged 20–64 years and older adults aged ≥ 65 years. The young adults were recruited from Tokyo Medical and Dental University. The older adults were community residents recruited through data collection in Kyoto, Yokohama, and Tokyo between 2022 and 2023. We collected data primarily from older adults who participated in local measurement events, where no strict participation limitations were imposed. The inclusion criteria for older adults were (1) independence in carrying out the activities of daily living and (2) ability to follow verbal commands. The exclusion criteria for both groups were (1) severe temporomandibular disorders, (2) a history of neurological and musculoskeletal conditions, and (3) recent treatment with botulinum toxin. Those with missing data were excluded.
Ultrasound measurements of the muscles
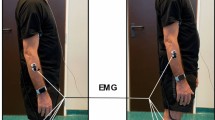
The thickness of the right masseter and rectus abdominis muscles, the cross-sectional area of the geniohyoid muscle, and the echo intensity of the three muscles were measured using an ultrasound strain elastography (USE) in B-mode (Noblus; Hitachi-Aloka Medical Japan, Tokyo, Japan), with a 6–14-MHz linear probe and acoustic coupler (EZU-TECPL1; Hitachi-Aloka Medical Japan) made of elastomer resin. An image depth of 4.0 cm was used for perioral muscles, and a depth of 5.0 cm was used for trunk muscles. A water-soluble transmission gel was applied to the acoustic coupler before measuring. Three images of each muscle captured with ultrasonography were analyzed using ImageJ (National Institutes of Health, Bethesda, MD, USA) to determine the muscle thickness in millimeters (mm), cross-sectional area in square millimeters (mm2), and echo intensity (Fig. 1). The average values of the three images were calculated and used as values for the variables.

Ultrasonographic measurements of the muscles. (a) Masseter muscle thickness (b) Geniohyoid muscle cross-sectional area (c) Rectus abdominis muscle thickness (d) Real-time elastography shows the strain ratio of the masseter muscle by comparing the strain of the acoustic coupler with the muscle.
The stiffness was obtained from the elastography mode of the USE with the same linear probe and acoustic coupler. The examiner manually compressed the ultrasound transducer against the skin surface while monitoring the strain graph of the pressing force shown on the monitor to ensure consistency. Five elastography images were selected based on the clear color of the muscle tissue, the acoustic coupler, and a constant pressing force on the strain graph during compression and release cycles29. Tissue deformation, represented by strain, is shown via elastography (Fig. 1). Soft tissue shows more deformation, resulting in a larger strain than that of stiffer tissue21. To determine the stiffness, strain ratio (SR), a semi-quantitative output that compares the strain of the reference: acoustic coupler; and that of a region of interest (ROI): muscle, was calculated with the built-in software. Higher SR values indicate softer tissue29. The average value of three SR readings represented the muscle stiffness. To maximize the reliability, the measurements were taken by one well-trained dentist23. Before this study, the dentist practiced elastography using 20 volunteers. The intra-rater reliability was tested, and intraclass correlation coefficients (ICCs) were also obtained.
Landmarks: masseter muscle
Participants were instructed to sit upright with their heads in a natural position. They were then asked to clench their teeth to make the masseter muscle more prominent and palpable, allowing for the identification of the muscle contraction point. Following this, they were directed to relax and refrain from biting during the measurement. The probe was placed perpendicular to the skin surface at the midpoint between the zygomatic arch and mandibular angle, approximately parallel to the plane of the camper, along a line connecting the point under the nasal wing with the ear tragus. The participants were instructed to relax and look straight ahead in a sitting position12.
Landmarks: geniohyoid muscle
Participants were instructed to sit facing forward with their mouths lightly closed and to swallow once. The probe was then gently placed vertically on the lower surface of the mandible without applying pressure. Afterward, it was positioned at one-third of the distance between the parotid gland and the mandible, and a cross-section of the muscle was captured30.
Landmarks: trunk muscle
The rectus abdominis trunk muscle is one of the primary abdominal muscles. In this study, measurements of the right rectus abdominis were obtained with participants in a supine position, arms and legs extended, and muscles fully relaxed. The probe was placed on the abdominal skin, approximately 3 cm lateral to the umbilicus. The images were captured during full expiration to ensure the muscles were in a relaxed state10.
Other confounding factors
Body mass index (BMI) and the number of natural teeth were included in the analysis. BMI has been correlated with swallowing muscle mass31. BMI was calculated by using the participants’ weight divided by their squared height. Tooth loss, as well as age, affects the perioral muscle32. The number of teeth present was thus confirmed by dentists and dental hygienists.
Statistical analyses
We calculated the sample size using G*Power 3.1 software (Kiel University, Kiel, Germany) for linear multiple regression with a fixed mode, R-squared deviation from zero. The required sample size was calculated to be 157 participants, based on an α-value of 0.05, a power of 0.8, and an effect size of 0.106, as used in a previous study32.
The normality of each variable was tested using the Shapiro–Wilk test. The distribution of each variable comparing the younger and older groups of adults was calculated by using the Mann–Whitney U test. The correlation coefficients of the perioral and trunk muscle characteristics with age, BMI, and number of teeth were calculated using Spearman’s rank correlation test. Multivariate analysis using multiple linear regression was conducted to investigate the relationship between each muscle type and age based on sex. The explanatory variables were age, BMI, and number of teeth. The muscle characteristics were included in the model as dependent variables. The entry method was used as the input method for the analysis. The level of statistical significance was set at a p-value < 0.05. SPSS for Windows (version 18; IBM Corp., Armonk, NY) was used for all statistical analyses.
Results
ICCs were determined to evaluate the examiner’s reliability. The ICCs for masseter muscle thickness (MMT), masseter muscle echo intensity (MEI), and masseter muscle strain ratio (MSR) were 0.84, 0.88, and 0.93, respectively. The ICC of the geniohyoid muscle cross-sectional area (GSA), geniohyoid muscle echo intensity (GEI), and geniohyoid muscle strain ratio (GSR) were 0.73, 0.82, and 0.83, respectively. The ICC of rectus abdominis muscle thickness (RT), rectus abdominis muscle echo intensity (REI), and rectus abdominis muscle strain ratio (RSR) were 0.98, 0.93, and 0.82, respectively. All ICC values showed high reliability in all the muscle variables.
A total of 215 participants were included in this study, comprising 108 men (53 younger adults and 55 older adults) and 107 women (45 younger adults and 62 older adults). The distribution of the participants’ characteristics for each variable is presented in Table 1. All muscle quantities (MMT, GSA, and RT) were significantly lower in older adults than in younger adults (p < 0.001). The echo intensities of the three muscles (MEI, GEI, and REI) were significantly higher in older adults, indicating lower muscle quality (p < 0.001 for MEI and REI and 0.001 for GEI). The RSR was significantly larger in younger adults, indicating softer muscle in the younger group (p < 0.001). However, the BMI, MSR, and GSR were not significantly different between the two groups.
Table 2 shows the correlation between age and muscle characteristics using Spearman’s correlation coefficient. In a total number of 108 men and 107 women, age was significantly correlated with the characteristics of all muscles. MMT, GSA, and RT, which indicate muscle quantity, tended to significantly decrease with age (p < 0.01). Conversely, MEI, GEI, and REI significantly increased with age (p < 0.01), indicating decreased muscle quality at older age. A decrease in MSR and RSR was associated with harder muscles (p < 0.01), while GSR slightly increased with age (p < 0.05) (Fig. 2). However, the correlation coefficients of MSR, GSR, and GSA in women showed no correlations, with RSR showing a weak correlation. Nevertheless, the results showed a higher coefficient in the trunk muscle than in the masseter and geniohyoid muscles, implying that the trunk muscle had a stronger correlation with age compared to that of the perioral muscles. Moreover, the coefficients of the masseter muscle were slightly larger than those of the geniohyoid muscle, implying that age relates to the masseter more than it does to the geniohyoid muscle.

Scatter plots and regression equations of age and muscle characteristics. (a) Scatter plot of age and MMT. (b) Scatter plot of age and MEI (c) Scatter plot of age and MSR. (d) Scatter plot of age and GSA. (e) Scatter plot of age and GEI. (f) Scatter plot of age and GSR. (g) Scatter plot of age and RT. (h) Scatter plot of age and REI. (i) Scatter plot of age and RSR. The bivariate regression equation p-values of the model are shown in each scatter plot. MMT masseter muscle thickness, MEI masseter muscle echo intensity, MSR masseter strain ratio, GSA geniohyoid muscle cross-sectional area, GEI geniohyoid muscle echo intensity, GSR geniohyoid muscle strain ratio, RT rectus abdominis muscle thickness, REI rectus abdominis muscle echo intensity, RAS rectus abdominis muscle strain ratio.
In examining the correlation coefficients, the relationships between quantity and quality were stronger and more significant in the total sample than in the narrower age groups. This indicates that aging is associated with notable changes in these variables. However, within a narrower age range, these changes appear to be less pronounced. In contrast, for stiffness, there was no significant difference between the narrower age groups and the total sample, suggesting that age-related changes in stiffness are less pronounced compared to those observed for quantity and quality.
The results of the multiple linear regression analysis showing the relationship between age and muscle strain ratio, stratified by sex, are shown in Table 3. Age was significantly associated with only the RSR in men (β = − 0.405, p < 0.01) and women (β = − 0.371, p < 0.01), showing increasing stiffness in the trunk muscle with aging. However, MSR and GSR showed low correlation coefficients in the correlation analysis and did not show significant associations with age in the regression analysis.
Discussion
We examined the impact of age on the characteristics of the perioral and trunk muscles regarding quantity, quality, and stiffness. Our findings revealed that trunk muscle stiffness was associated with age, but not that of perioral muscles. Moreover, the decline in the quantity and quality of the trunk muscle was more strongly correlated with age than those of the perioral muscles, and those of the masseter muscle showed a greater correlation with age than the geniohyoid muscle.
The present data showed an association between increases in trunk muscle stiffness with age but not in perioral muscle stiffness (Table 3). This finding is consistent with other studies on skeletal muscles33,34,35. Increased muscle stiffness contributes to the change in mechanical properties of muscle fibers36, extracellular matrix, and connective tissues37,38. However, no difference in resting mechanical properties has been found comparing slow and fast single fibers of healthy human muscles39. A study in patients with spasticity showed increased muscle rigidity, partially caused by an excessive stretch reflex and altered muscle mechanical properties at rest26. Changes in tissue stiffness also arise from disuse, progressive diseases and disorders, or spasticity following neurological insult23.
In contrast, our findings in the perioral muscle, for which stiffness and age were not related, aligned with the findings of a study40 that found no alteration in the contractile property of masseter and geniohyoid muscles of rats. Another study41 also reported no significant difference in quadriceps muscle stiffness between younger and older adults since the viscoelastic characteristics and muscle compliance may not be affected by aging. A previous study also stated that age-related muscle stiffness remains controversial26. Increased stiffness and tension of the perioral muscle is often associated with hypertrophy, soreness, and pain in patients with temporomandibular disease25,26,42. Our participants comprised a healthy population without underlying conditions, allowing for minor changes in the contractile mechanism of the muscle that did not influence overall stiffness with age. There is limited research on the stiffness of the geniohyoid muscle40,43; thus, to the best of our knowledge, this study is the first to demonstrate that age is not associated with geniohyoid muscle stiffness.
In ultrasonography, muscle thickness and cross-sectional area indicate muscle quantity. Echo intensity, representing the fat and fibrous tissue in muscles, indicates muscle quality, whereas a whiter image represents less contractile muscle tissue and lower muscle quality44. Muscle stiffness shows the relationship between possible deformation and muscle compression and can be measured using ultrasound elastography10. Previously, the quantitative evaluation of muscle stiffness was conducted using compression-type tissue stiffness meters. However, the presence of subcutaneous fat and the inability to evaluate deep tissue could be a limitation27. Compared to magnetic resonance elastography (MRE), ultrasound elastography has many advantages as it is less expensive, less time-consuming, non-invasive, and has the potential for wider clinical availability45. The USE with an acoustic coupler is proven to be feasible and reproducible for detecting the elasticity of skeletal muscles46,47,48 and masseter muscle stiffness25. The SR or the elastic index ratio obtained from USE was verified to be sufficient to make comparisons of the hardness of the masseter muscle between individuals42,49.
Even though shear wave ultrasound is widely used, USE has also been proven to be reliable and reproducible in measuring muscle stiffness and elasticity and shows good convergent validity with relevant clinical assessment21,23,24,29,42. USE also has an advantage in selecting the ROI to cover the muscle area as much as possible. It is useful to obtain more general hardness representing the whole muscle, which may be limited in shear wave elastography21. The present results using USE are also consistent with those of previous studies.
The second finding regarding the differences in changes in the trunk and perioral muscles with age (Table 2) could be explained by a complex process of muscle deterioration with variations between different muscle groups and individuals. This can be influenced by individual factors2 as well as the specific functions and usage patterns of different muscles40. Healthy younger and older adults who engage in daily use of the perioral muscles experience more frequent stimulation compared to the abdominal muscles50,51, potentially leading to less deterioration in the perioral muscles. Differences in muscle size and fiber composition could contribute to this effect52, as the rectus abdominis is a larger muscle predominantly composed of Type II fibers. These fibers are more susceptible to age-related changes and are more prone to atrophy compared to other fiber types1. The jaw-closing muscles have a different composition of muscle fibers52. Additionally, the presence of intramuscular adipose tissue in the swallowing muscles may have a lesser impact on function compared to that observed in limb muscles53.
Moreover, we found that the quantity and quality of the masseter muscles showed stronger correlation with age than the geniohyoid muscle (Table 2). Muscle size and differences in function could be responsible for this, as the masseter muscle primarily contains Type II fibers, which are more prone to atrophy with aging and larger than the geniohyoid muscle1. Furthermore, different adaptive responses to altered functional demands are associated with aging40. We assume that as masseter muscles are involved in repetitive movement, they are more prone to muscle fatigue and overuse-related deterioration than the geniohyoid muscles54.
The finding of age-related decreases in the quantity and quality of all muscles analyzed aligns with previous studies13,14,32. Age-related muscle atrophy arises from a combination of physiological and behavioral factors, combined with age-related anabolic resistance and denervation of the muscle2. Additionally, myokines produced by skeletal muscles and triggered by exercise and physical activity55 are key factors in regulating muscle growth. In terms of muscle quality, echo intensity reflects noncontractile components like intramuscular fat and fibrous tissue. Muscle satellite cells support muscle fiber generation and inhibit progenitor cells from becoming fat cells, but this inhibition weakens with a decline in satellite cells or muscle atrophy56.
There were some limitations in this study. First, the cross-sectional study design may not define causal relationships between age and muscle characteristics. Therefore, longitudinal studies may be necessary for a more comprehensive understanding. Second, while the strain ratio obtained from ultrasound elastography (USE) has been validated, it differs from stiffness measurements obtained through shear wave elastography, making quantitative comparisons impractical. Nonetheless, a notable strength of this research is its inclusion of a large sample size comprising both younger and older adults. The findings demonstrate that perioral muscle stiffness is not influenced by age in healthy individuals, providing a valuable baseline for future research. However, the findings emphasize the importance of focusing on trunk muscles to maintain muscle quantity and quality due to their stronger association with aging, particularly for the older population at risk of rapid muscle deterioration.
Conclusions and implications
Age relates to trunk muscle stiffness but not that of perioral muscles. Furthermore, trunk muscle quality and quantity had stronger correlations with age than those of the perioral muscles. It is important to acknowledge that age-related characteristics in trunk and perioral muscles do not necessarily exhibit parallel changes but rather demonstrate differences. Maintaining physical activity for both trunk and perioral muscles is essential to prevent age-related muscle decline.
Data availability
The data that supports the findings of this study are available from the corresponding author upon reasonable request.
References
Deschenes, M. R. Effects of aging on muscle fibre type and size. Sports Med. 34, 809–824 (2004).
Wilkinson, D. J., Piasecki, M. & Atherton, P. J. The age-related loss of skeletal muscle mass and function: Measurement and physiology of muscle fibre atrophy and muscle fibre loss in humans. Ageing Res. Rev. 47, 123–132 (2018).
Ogawa, N. et al. Ultrasonography to measure swallowing muscle mass and quality in older patients with sarcopenic dysphagia. J. Am. Med. Dir. Assoc. 19, 516–522 (2018).
Özsürekci, C. et al. Relationship between chewing ability and malnutrition, sarcopenia, and frailty in older adults. Nutr. Clin. Pract. 37, 1409–1417 (2022).
Feng, X. et al. Aging-related geniohyoid muscle atrophy is related to aspiration status in healthy older adults. J. Gerontol. A Biol. Sci. Med. Sci. 68, 853–860 (2013).
Akuthota, V. & Nadler, S. F. Core strengthening. Arch. Phys. Med. Rehabil. 85, S86-92 (2004).
Tamura, F. et al. The survey on the feeding functions of the housebound elderly: Relationship between feeding conditions and choking. Jpn. J. Dysphagia Rehabil. 1, 57–68 (1997).
Beaudart, C., Zaaria, M., Pasleau, F., Reginster, J. Y. & Bruyère, O. Health outcomes of sarcopenia: A systematic review and meta-analysis. PLoS ONE 12, e0169548 (2017).
Maeda, K., Takaki, M. & Akagi, J. Decreased skeletal muscle mass and risk factors of sarcopenic dysphagia: A prospective observational cohort study. J. Gerontol. A Biol. Sci. Med. Sci. 72, 1290–1294 (2017).
Perkisas, S. et al. Application of ultrasound for muscle assessment in sarcopenia: 2020 SARCUS update. Eur. Geriatr. Med. 12, 45–59 (2021).
Nijholt, W., Scafoglieri, A., Jager-Wittenaar, H., Hobbelen, J. S. M. & van der Schans, C. P. The reliability and validity of ultrasound to quantify muscles in older adults: A systematic review. J. Cachex. Sarcopenia Muscle 8, 702–712 (2017).
Serra, M. D., Duarte Gavião, M. B. & dos Santos Uchôa, M. N. The use of ultrasound in the investigation of the muscles of mastication. Ultrasound Med. Biol. 34, 1875–1884 (2008).
Mori, T., Izumi, S., Suzukamo, Y., Okazaki, T. & Iketani, S. Ultrasonography to detect age-related changes in swallowing muscles. Eur. Geriatr. Med. 10, 753–760 (2019).
Fukumoto, Y. et al. Age-related ultrasound changes in muscle quantity and quality in women. Ultrasound Med. Biol. 41, 3013–3017 (2015).
Maeda, K. & Akagi, J. Sarcopenia is an independent risk factor of dysphagia in hospitalized older people. Geriatr. Gerontol. Int. 16, 515–521 (2016).
Yoshimi, K. et al. Relationship between swallowing muscles and trunk muscle mass in healthy elderly individuals: A cross-sectional study. Arch. Gerontol. Geriatr. 79, 21–26 (2018).
Ishii, M. et al. time spent away from bed to maintain swallowing function in older adults. Gerontology 69, 37–46 (2023).
Yamaguchi, K. et al. Associations of swallowing-related muscle quantity and quality with sarcopenic parameters. Eur. Geriatr. Med. 14, 195–201 (2023).
Yamaguchi, K. et al. Association between characteristics of swallowing-related muscles and trunk muscle mass. Sci. Rep. 13, 7814 (2023).
González-Fernández, M. et al. Masseter muscle thickness measured by ultrasound as a possible link with sarcopenia, malnutrition and dependence in nursing homes. Diagnostics (Basel) 11, 1587 (2021).
Brandenburg, J. E. et al. Ultrasound elastography: The new frontier in direct measurement of muscle stiffness. Arch. Phys. Med. Rehabil. 95, 2207–2219 (2014).
Creze, M. et al. Shear wave sonoelastography of skeletal muscle: Basic principles, biomechanical concepts, clinical applications, and future perspectives. Skelet. Radiol. 47, 457–471 (2018).
Miller, T., Ying, M., Sau Lan Tsang, C., Huang, M. & Pang, M. Y. C. Reliability and validity of ultrasound elastography for evaluating muscle stiffness in neurological populations: A systematic review and meta-analysis. Phys. Ther. 101, 188 (2021).
Roots, J., Trajano, G. S. & Fontanarosa, D. Ultrasound elastography in the assessment of post-stroke muscle stiffness: A systematic review. Insights Imaging 13, 67 (2022).
Olchowy, A. et al. Great potential of ultrasound elastography for the assessment of the masseter muscle in patients with temporomandibular disorders. A systematic review. Dentomaxillofac. Radiol. 49, 20200024 (2020).
Marcucci, L. & Reggiani, C. Increase of resting muscle stiffness, a less considered component of age-related skeletal muscle impairment. Eur. J. Transl. Myol. 30, 8982 (2020).
Hara, K. et al. Association between myotonometric measurement of masseter muscle stiffness and maximum bite force in healthy elders. J. Oral. Rehabil. 47, 750–756 (2020).
Orimo, H. et al. Reviewing the definition of “elderly”. Geriatr. Gerontol. Int. 6, 149–158 (2006).
Inami, T. et al. Relationship between isometric contraction intensity and muscle hardness assessed by ultrasound strain elastography. Eur. J. Appl. Physiol. 117, 843–852 (2017).
Kajisa, E. et al. The relationship between jaw-opening force and the cross-sectional area of the suprahyoid muscles in healthy elderly. J. Oral. Rehabil. 45, 222–227 (2018).
Yamaguchi, K. et al. Ultrasonography shows age-related changes and related factors in the tongue and suprahyoid muscles. J. Am. Med. Dir. Assoc. 22, 766–772 (2021).
Yamaguchi, K. et al. Relationship of aging, skeletal muscle mass, and tooth loss with masseter muscle thickness. BMC Geriatr. 18, 67 (2018).
Trappe, S. et al. Single muscle fibre contractile properties in young and old men and women. J. Physiol. 552, 47–58 (2003).
D’Antona, G. et al. The effect of ageing and immobilization on structure and function of human skeletal muscle fibres. J. Physiol. 552, 499–511 (2003).
Ochala, J., Frontera, W. R., Dorer, D. J., Van Hoecke, J. & Krivickas, L. S. Single skeletal muscle fiber elastic and contractile characteristics in young and older men. J. Gerontol. A Biol. Sci. Med. Sci. 62, 375–381 (2007).
Lim, J. Y., Choi, S. J., Widrick, J. J., Phillips, E. M. & Frontera, W. R. Passive force and viscoelastic properties of single fibers in human aging muscles. Eur. J. Appl. Physiol. 119, 2339–2348 (2019).
Gao, Y., Kostrominova, T. Y., Faulkner, J. A. & Wineman, A. S. Age-related changes in the mechanical properties of the epimysium in skeletal muscles of rats. J. Biomech. 41, 465–469 (2008).
Wood, L. K. et al. Intrinsic stiffness of extracellular matrix increases with age in skeletal muscles of mice. J. Appl. Physiol. 1985(117), 363–369 (2014).
Olsson, M. C. et al. Fibre type-specific increase in passive muscle tension in spinal cord-injured subjects with spasticity. J. Physiol. 577, 339–352 (2006).
Kaneko, S., Iida, R. H., Suga, T., Morito, M. & Yamane, A. Age-related changes in rat genioglossus, geniohyoid and masseter muscles. Gerodontology 31, 56–62 (2014).
Ikezoe, T., Asakawa, Y., Fukumoto, Y., Tsukagoshi, R. & Ichihashi, N. Associations of muscle stiffness and thickness with muscle strength and muscle power in elderly women. Geriatr. Gerontol. Int. 12, 86–92 (2012).
Ariji, Y. et al. Use of sonographic elastography of the masseter muscles for optimizing massage pressure: A preliminary study. J. Oral Rehabil. 36, 627–635 (2009).
Arens, P., Fischer, T., Dommerich, S., Olze, H. & Lerchbaumer, M. H. Ultrasound shear wave elastography of the tongue during selective hypoglossal nerve stimulation in patients with obstructive sleep apnea syndrome. Ultrasound Med. Biol. 47, 2869–2879 (2021).
Pillen, S. et al. Skeletal muscle ultrasound: Correlation between fibrous tissue and echo intensity. Ultrasound Med. Biol. 35, 443–446 (2009).
Drakonaki, E. E., Allen, G. M. & Wilson, D. J. Ultrasound elastography for musculoskeletal applications. Br. J. Radiol. 85, 1435–1445 (2012).
Muraki, T. et al. Ultrasound elastography-based assessment of the elasticity of the supraspinatus muscle and tendon during muscle contraction. J. Shoulder Elbow Surg. 24, 120–126 (2015).
Yanagisawa, O., Niitsu, M., Kurihara, T. & Fukubayashi, T. Evaluation of human muscle hardness after dynamic exercise with ultrasound real-time tissue elastography: A feasibility study. Clin. Radiol. 66, 815–819 (2011).
Niitsu, M., Michizaki, A., Endo, A., Takei, H. & Yanagisawa, O. Muscle hardness measurement by using ultrasound elastography: A feasibility study. Acta Radiol. 52, 99–105 (2011).
Nakayama, M., Ariji, Y., Nishiyama, W. & Ariji, E. Evaluation of the masseter muscle elasticity with the use of acoustic coupling agents as references in strain sonoelastography. Dentomaxillofac. Radiol. 44, 20140258 (2015).
McPhee, J. S. et al. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 17, 567–580 (2016).
McCormick, R. & Vasilaki, A. Age-related changes in skeletal muscle: Changes to life-style as a therapy. Biogerontology 19, 519–536 (2018).
Schiaffino, S. & Reggiani, C. Fiber types in mammalian skeletal muscles. Physiol. Rev. 91, 1447–1531 (2011).
Yamaguchi, K. et al. Age-related changes in swallowing muscle intramuscular adipose tissue deposition and related factors. Exp. Gerontol. 153, 111505 (2021).
Sciote, J. J. et al. Masseter function and skeletal malocclusion. Rev. Stomatol. Chir. Maxillofac. Chir. Orale. 114, 79–85 (2013).
Pedersen, B. K., Akerström, T. C., Nielsen, A. R. & Fischer, C. P. Role of myokines in exercise and metabolism. J. Appl. Physiol. 1985(103), 1093–1098 (2007).
Shefer, G., Van de Mark, D. P., Richardson, J. B. & Yablonka-Reuveni, Z. Satellite-cell pool size does matter: Defining the myogenic potency of aging skeletal muscle. Dev. Biol. 294, 50–66 (2006).
Acknowledgements
We would like to thank all the staff of our department for helping with the research and the individuals who participated in this research.
Funding
This research was supported by the Japan Society for the Promotion of Science (24K20097 and 20K18801).
Author information
Authors and Affiliations
Contributions
Ko.Y. and H.T. contributed to the study concept and design. The acquisition of data was done by Ko.Y., R.M., and S.A. Data analysis and interpretation were performed by S.A. and Ko.Y. The first draft of the manuscript was written by S.A. The manuscript was critically reviewed and edited by Ko.Y. and S.A. All authors commented on previous versions of the manuscript, read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Amornsuradech, S., Yamaguchi, K., Nakagawa, K. et al. Aging-associated differences between perioral and trunk muscle characteristics. Sci Rep 14, 27745 (2024). https://doi.org/10.1038/s41598-024-79268-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-79268-4
