
Abstract
The Edinburgh Postnatal Depression Scale (EPDS) is the screening tool for perinatal depression, and its cut-off score varies according to context and population. In Cameroon, no study has yet defined a cut-off score or the prevalence of perinatal depression in adolescent mothers. Our aim is to determine the cut-off for teenage mothers in Cameroon. The study is cross-sectional and analytical in nature. The EPDS was used to screen for symptoms of depression and an interview based on the DSM-5 criteria for depression was conducted to diagnose the depressive syndrome. The data were processed with Epidata 3.1 and was analysed with SPSS 25. Positive and negative predictive values (PPV, NVP) were calculated. The optimal EPDS score was determined by taking into account the importance of false-negative and false-positive test results. 1633 adolescent mothers were recruited. The prevalence of perinatal depression was 60.8% (95% CI = 58.5, 63.2). The cut-off score for this population was ≥ 11. Sensitivity was 92.6% (95% CI = 0.913, 0.939) specificity 53.2% (95% CI = 0.508, 0.556), PPV 75.5% and NPV 80.2%. This score of ≥ 11 is retained because false-negative results have important adverse consequences. This study on the validation of the EPDS and the prevalence of perinatal depression in a population of teenage mothers is new in Cameroon and central Africa.
Similar content being viewed by others

Context
Maternal mental health, as defined by the WHO (World Health Organization), is the state of well-being in which a mother is aware of her own abilities, can cope with the normal stressors of life, can work productively and fruitfully, and is able to contribute to her community1. Several studies have highlighted the significant burden of maternal mental health, which is perinatal mental disorders, in low- and middle-income countries2. The prevalence of perinatal mental disorders is 15.6% in pregnant women and 19.8% in postnatal women2. Particularly in Cameroon, a study reveals that the prevalence of perinatal mental disorders is 53.6%. And, among these disorders, perinatal depression is by far the most prevalent, at 45.8%3. In particular, the prevalence among teenage mothers is high, sometimes even higher than the prevalence among adult mothers. For example, two studies in Nigeria show that prenatal prevalence is 6.9% among adult mothers, compared with 17.7% and 18.1% among teenage mothers In Cameroon4,5, in a study of a population of 1,365 teenage mothers in the perinatal period, 70% of them presented depressive symptoms6. Although the prevalence of mental disorders among adolescents has been determined in a study in Cameroon7, perinatal depression did not emerge in this study, nor in any other in Cameroon, to our knowledge.
The preferred instrument for screening for perinatal depression worldwide is the Edinburgh Postnatal Depression Scale (EPDS)8,9. Multiple versions have been developed and validated to adapt the tool to different contexts and environments. The cut-off values range from ≥ 7 to ≥ 158. In Cameroon, several studies and clinical interventions have used the EPDS as a screening instrument for depressive symptoms in perinatal mothers. The threshold used varied according to the studies and interventions, and ranged from ≥ 10 to ≥ 1310,11. However, no research in Cameroon has identified a validated EPDS cut-off score for a Cameroonian population. The cut-off scores used in both research and clinical projects are based on validations carried out in other countries.
The aim of this research is to identify in the Cameroonian context, the optimal cut-off and validate it specifically for a population of adolescent mothers. This involves determining the sensitivity, specificity, positive predictive value and negative predictive value of the EPDS test. Prior to this, the prevalence of perinatal depression will be assessed.
Results
The overall objective is to validate an EPDS threshold score in a population of perinatal adolescent mothers in Cameroon. Before doing so, we will identify socio-demographic characteristics.
Socio-demographic characteristics of teenage mothers
1633 teenage mothers took part in the study. 51.4% were pregnant (prenatal) and 48.5% had a child up to one year old (postnatal). The average age was 17.91 years, and the most represented age group was 18–20 years, i.e., 68.4% of participants. 75% of them were single mothers. The majority of these mothers (46.8%) were recruited from health facilities. Further details on socio-demographic characteristics are provided in Table 1. Given these characteristics, it would be interesting to determine the prevalence of depression in this population.
A specific objective was to assess perinatal depression, i.e., in pregnant and postpartum women. Clinical interviews, based on DSM-5 criteria, revealed that: 504/827 pregnant teenage mothers suffered from depression. This represents a prevalence of 60.9% for the prenatal population and 30.9% for the perinatal study population. Among mothers with babies aged 12 months or less, 490/783 were diagnosed with depression. This represents a prevalence of 62.5% for the nursing mother population alone, and 30% for all teenage mothers in the perinatal period. And so, the prevalence rate of perinatal depression for teenage mothers in this study is: 60.9% (994/1633). More details concerning the prevalence are given in Table 2. The diagnosis of depression established in teenage mothers will be used to conduct analyses to identify the EPDS cut-off score. To do this, we will begin by highlighting the results of the administration of the EPDS scale to teenage mothers.
To achieve the major objective of this study, which is to determine the cut-off score12 for the EDPS when used with adolescent mothers in the Cameroonian context, we proceeded in the following stages. First, we considered the likely adverse consequences of a false-negative result. Perinatal depression can have a negative impact on various aspects of the teenage mother’s private, school, and professional life. The mother-baby relationship may be altered and the baby’s development hampered, and there may be a risk of abuse and neglect of the baby. Marital and family conflicts may be triggered. There may be a risk of intergenerational transmission of dysfunctions13. There is also a risk of economic loss14. We then considered the likely adverse consequences of a false-positive result. They relate to the waste of human, financial, and time resources. With regard to the likely consequences described above, it emerges that those of a false negative result are much more important. This finding leads us to choose a threshold score that minimises the most harmful risks for teenage mothers. Hence the use of the most sensitive threshold score, as shown in Table 3. The optimal cut-off score for adolescent mothers during the perinatal period in Cameroon is 10.5, with a sensitivity of 0.926 (92.6%), a specificity of 0.532 (53.2%), a PPV of 75.5% and a NPV of 82.2%.
Discussion
As a reminder, our objective in this work is twofold: to validate the EPDS score and to determine the prevalence of perinatal depression in a population of adolescent mothers in Cameroon (Table 4).
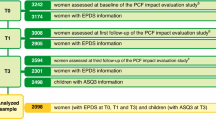
As mentioned above, 10.5 is an appropriate cut-off score. We also analysed the ROC curve to calculate the threshold score. Here, the threshold score in the ROC curve would correspond to the point closest to the ideal (1; 1), which is the point furthest from the diagonal12. In our case, 12.5 would correspond best, as shown in Table 5 and Fig. 1. However, as indicated in the results section, the method based on taking into account the importance of the likely adverse consequences of false-negative results, in comparison with the importance of the likely adverse consequences of false-positive results. It seems to us to be more relevant. Choosing a score above 10.5 would mean failing to detect a few cases that could be positive, and therefore false negatives. The likely adverse consequences of false-negative results are important enough to justify choosing this score of 10.5. By choosing that score, we reduce the likelihood of not identifying some adolescent mothers in Cameroon who are in fact suffering from depression. This is why we have chosen a sensitivity of 92.6%. Although the specificity 53% is lower, it is still acceptable to us and therefore a good compromise. Furthermore, as shown in Table 4, 92.7% (922 out of 994) of the adolescent mothers in our study population suffering from depression had a score of 11 or above. It should be noted that the calculated scores on the EPDS are given as whole numbers. With 10.5 being the threshold score chosen, we rounded up to 11, which is the nearest whole number to 10.5.

A receiver operating characteristic curve showing the EPDS cut-off score in teenage mothers. The black dot corresponds to the threshold score of 12.5 with the highest sensitivity and specificity. The red dot corresponds to the threshold score 10.5 resulting from a compromise between the consequences of false positives and false negatives.
According to our study, the valid cut-off score of the EPDS to screen for depression in adolescent mothers in Cameroon is ≥ 11. This is a scientific adjustment, because until now the EPDS cut-off scores used in Cameroon have varied between ≥ 10 and ≥ 133,6,10,11. The basis on which these scores were chosen by their authors was certainly scientific, but not tested or verified in the Cameroonian context.
The optimal threshold score for screening for perinatal depression obtained in our research is ≥ 11, and is different from the threshold in the original version15. This cut-off score found in our research is similar to that (≥ 11) of the EPDS validated in France16. Compared with the thresholds reported in other African contexts, our result is different. In Ghana and Zimbabwe, the cut-off is 10, and in Nigeria, neighbouring Cameroon, the threshold is 9 to more17,18. These variations further justify our study. It is not appropriate to base ourselves on African results, even those of a neighbouring country such as Nigeria. Determining precise measures is therefore essential. Without them, the burden may not be clearly defined, and health policy and services may suffer as a result, especially in a resource-poor context like Cameroon. This is all the more crucial given that the prevalence of perinatal depression among pregnant teenage mothers observed in our study is 60.9%, which seems extremely high to us. This is well below the 17.7% found among teenage mothers in Nigeria5. Also, this rate is higher than the 43.6% prevalence found among pregnant adult mothers living in the same geographical area (Yaoundé)3. Detecting perinatal depression and treating it is a matter of urgency, given the negative consequences for the health of the mother, the family, the baby and its development.
Methods
Study framework
Our research is part of a project to provide psychological and social care for teenage mothers in Yaoundé and the surrounding area. The project had two dimensions: clinical and research. The study is cross-sectional and analytical in nature. In fact, this study is the research dimension of an action research project, which combines, in a single movement, a research rationale to produce knowledge and an action rationale to act, modify and improve a situation or an activity19. In Cameroon, the partners involved were: the Ministry of Public Health (MINSANTE), the Ministry for the Promotion of Women and the Family (MINPROFF), Le Réseaux National des Associations de Tantines (RENATA), Uni-Psy et Bien-Être (UniPsy) an organization of mental health professionals. And in Geneva, the University of Geneva, Action en Santé Publique (ASP) a non-governmental organization, the Department of Child and Adolescent Psychiatry (SPEA) of the Geneva University Hospitals and the World Health Organisation (WHO). In the field a team of 71 front-line health workers (nurses, social workers, psychology students, junior psychologists) was trained in the use of the WHO mhGAP (mental health Global Action Plan) Guide, based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). She was also trained to administer the EPDS. These carers were supervised by 8 2nd line clinical psychologists and 3 3rd line psychiatrists. The former administered the EPDS, while the clinical psychologists and supervising psychiatrists made diagnoses based on clinical interviews.
Population and sampling
Our study population consisted of adolescent mothers in the perinatal period (from day 1 of pregnancy to the end of the child’s first year). They all lived in Yaoundé and the surrounding area. They were pregnant and in postpartum. Recruitment took place over a five-year period, from April 2014 to December 2018. Inclusion criteria were being no more than 20 years old, pregnant or having a child no more than 12 months old. Exclusion criteria were being over 20 years of age, having a child older than 12 months, not having fully completed the EPDS and not having been clinically assessed. The non-probability sampling technique was chosen. 2 types of sampling were carried out. These were purposive sampling for participants recruited at the hospital and through the personal network of health workers, and accidental sampling for those recruited by door-to-door canvassing20. The typical sample, also known as purposive sampling, is a sample of volunteers. Only people who volunteer are included in this type of sample. In our study, we selected only teenage mothers in the perinatal period from among all the mothers and other patients we could meet. Accidental sampling (sometimes called point sampling, convenience sampling or opportunity sampling) is a type of non-probability sampling that involves drawing the sample from the part of the population that is within reach. This meant that in the community it was the teenage mothers who were first met and available who were selected. As we mentioned, the project had two dimensions: clinical and research. It was to run for 5 years. We stopped selecting teenage mothers 4 years later, to give the care team time to take on teenage mothers who had been positively diagnosed. At that point, we had 1,633 teenage mothers, which was a very large number, so we no longer needed to calculate the sample size.
Procedure and data collection
Recruitment of 1633 teenage mothers took place in 3 contexts, including: 764 teenage mothers were recruited in the mother–child departments of 29 health centers. 639 adolescent mothers recruited in the community through door-to-door visits, and 213 by word-of-mouth in the personal network of health workers. As collection tools, we used the validated French version of the EPDS to screen for perinatal depression21. The DMS-V was used as a frame of reference for the diagnostic assessment of perinatal depression (pre- and post-partum)22,23. Indeed, front-line health workers administered the EPDS scale to participants. We preferred the EPDS to be interviewer-administered rather than self-administered because of its advantages, particularly for illiterate participants. The supervising clinical psychologists and psychiatrists made the diagnosis of perinatal depression following the clinical interviews.
Edinburgh postnatal depression scale (EPDS)
The EPDS is the most widely used instrument in the world for screening for prenatal and postnatal depression. This tool was originally developed in 1987 by Cox et al. It is a 10-item questionnaire, so the response to each question can be rated from 0 to 3, making a maximum value of 30 possible15. A systematic review of validation studies of the Edinburgh Postnatal Depression Scale (EPDS) was carried out. It showed that the sensitivity of this screening tool ranges from 0.65 to 1.00 and the specificity from 0.71 to 0.97, for positivity thresholds varying from 8.5 to 13.5 depending on the study24.
DSM-V
The Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, provides a clear, systematic description and classification of mental disorders23. It is intended for mental health professionals and is an international reference. Clinical psychologists and psychiatrists have used this reference to confirm the diagnosis of perinatal depression.
Data analysis
The data were processed and analysed using Epidata 3.1 and SPSS 25 respectively. We first performed descriptive statistics, which consisted in highlighting the different frequencies of the modalities of the variables. Then, to validate the EPDS for teenage mothers in Cameroon, we performed sensitivity and specificity tests, for several thresholds in relation to the DSM-V diagnosis of depression. Positive predictive values (PPV) and negative predictive values (NPV) were calculated. In fact, to determine the optimal cut-off score to validate for teenage mothers, we tested the sensitivity and specificity of several thresholds. In addition, PPV and NPV calculations were performed. The sensitivity of the EPDS refers to the proportion of teenage mothers actually diagnosed with depression according to the DSM-5. Specificity refers to the proportion of teenage mothers classified as not actually suffering from depression. Positive predictive value refers to the probability that a positive test result actually indicates that an individual has a pathology. The negative predictive value refers to the probability that a negative test result actually indicates that the individual is not ill. The optimal score12 on the EPDS was determined, taking into account the importance of the likely adverse consequences of false-negative results, in comparison with the importance of the likely adverse consequences of false-positive results.
Ethical oversight
Study procedures were implemented in conformity with ethical principles as set out in the Declaration of Helsinki25. All participants were informed of the study and provided informed written consent. They were informed that if they wished, they could withdraw from the study at any time. The ethic clearance was delivered by the National Ethics Committee on Research for Human Health (NECRHH) in Yaoundé after submission of our research protocol. 2014/03/436/L/CNERSH/SP was the approval number.
Limitations of the study
Our research has a number of limitations. The first concerns the environment in which the teenage mothers were recruited. It was carried out in the urban area of Yaoundé. Young mothers living in rural areas may experience other realities that could influence the results. With regard to the realities in rural areas, we could mention the fact that early pregnancies are seen by the community as a normal situation, so they are not stigmatised and excluded, there is less practical and social support and less loneliness, and the baby can be cared for by the grandmother or another more experienced woman, and so on. Secondly the participants were only teenage mothers; there were no adult mothers. Thirdly, the EPDS tested did not include a somatic item. In developing countries, psychological disorders, including depression, often take the form of significant somatic symptoms26. Fourthly, another important limitation is the generalizability of the findings since non-probability samplings were utilized.
Conclusion
The EPDS is a screening instrument for perinatal depression that was administered to a population of 1,633 teenage mothers. The prevalence rate of perinatal depression was 60.8%. This tool is valid for screening teenage mothers for pre- and post-natal depression in Cameroon. Sensitivity was 92.6% and specificity 53.2%. The cut-off score found was ≥ 11. Prior to our research, no study had been carried out on the validity of the EPDS in a Cameroonian population. Given the significantly high prevalence of perinatal depression among teenage mothers in this country, the use of a valid instrument that is precise with respect to the cut-off score is very important for screening (and management) at all levels of care, as well as for determining the real burden by the true positive rate.
Data availability
The data supporting the conclusions of this study are available on request from the corresponding author. The data is not publicly available due to confidentiality or ethical restrictions.
References
World Health Organization. Promoting Mental Health: Concepts, Emerging Evidence, Practice: Report of the World Health Organization, Department of Mental Health and Substance Abuse in Collaboration with the Victorian Health Promotion Foundation and the University of Melbourne (2005). https://iris.who.int/handle/10665/43286
Fisher, J. et al. Prevalence and determinants of common perinatal mental disorders in women in low-and lower-middle-income countries: A systematic review. Bull. World Health Organ. 90(2), 139–149. https://doi.org/10.2471/BLT.11.091850 (2012).
Djatche Miafo, J. et al. Epidemiological profile of perinatal mental disorders at a tertiary hospital in Yaoundé-Cameroon. Front. Glob. Womens Health 4, 999840. https://doi.org/10.3389/fgwh.2023.999840 (2023).
Al-abri, K., Edge, D. & Armitage, C. J. Prevalence and correlates of perinatal depression. Soc. Psychiat. Psychiatr. Epidemiol. https://doi.org/10.1007/s00127-022-02386-9 (2023).
Oladeji, B. D. et al. Prevalence and correlates of depression among pregnant adolescents in primary maternal care in Nigeria. Arch. Womens Ment. Health 25, 441–450. https://doi.org/10.1007/s00737-021-01198-1 (2022).
Nicolet, L. et al. Teenage mothers in Yaoundé, Cameroon—risk factors and prevalence of perinatal depression symptoms. J. Clin. Med. 10, 4164. https://doi.org/10.3390/jcm10184164 (2021).
Djatche, J. M. et al. A cross-sectional analysis of mental health disorders in a mental health services-seeking population of children, adolescents, and young adults in the context of ongoing violence and displacement in northern Cameroon. Compr. Psychiat. 113, 152293. https://doi.org/10.1016/j.comppsych.2021.152293 (2021).
Brooke, L., Negeri, Z., Sun, Y., Benedetti, A. & Thombs, B. D. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: Systematic review and meta-analysis of individual participant data. BMJ 371, 14022. https://doi.org/10.1136/bmj.m4022 (2020).
Tissier, J. et al. Dépistage de la dépression périnatale maternelle en protection maternelle et infantile: Un état des lieux et perspectives. Devenir 36, 2–18. https://doi.org/10.3917/dev.241.0002 (2024).
Nwana, T. D. et al. Prevalence and factors associated with post-partum depression in a rural area of Cameroon: A cross-sectional study. Pan Afr. Med. J. https://doi.org/10.11604/pamj.2022.42.138.3234 (2022).
Adama, N. D. et al. Prevalence and risk factors of postpartum depression in Yaounde, Cameroon. Open J. Obstet. Gynecol. 5, 608–617. https://doi.org/10.4236/ojog.2015.511086 (2015).
Zweig, M.H. Campbell, G. Receiver-operating characteristic (ROC) plots: a fundamental evaluation tool in clinical medicine. Clin Chem, 39(4), 561–77 (1993). Erratum in: Clin Chem, 39(8), 1589 (1993). PMID: 8472349.
Manzano, J., Palacio, F. & Zilkha, N. Les scénarios narcissiques de la parentalité (Presses Universitaire de France, 2009).
Chisholm, D. et al. Scaling up treatment of depression and anxiety: A global return on investment analysis. Lancet Psychiat. https://doi.org/10.1016/S2215-0366(16)30024-4 (2016).
Cox, J. L., Holden, J. M. & Sagovsky, R. Detection of postnatal depression: Development of the 10-item edinburgh postnatal depression scale. Br. J. Psychiatry 150, 782–786 (1987).
Guedeney, N., Fermanian, J., Guelfi, J. D. & Delour, M. Premiers résultats de la traduction de l’EPDS sur une population parisienne. A propos de la validation de la traduction et de la traduction de l’EPDS. Devenir 17, 69–92 (1995).
Weobong, B. et al. The comparative validity of screening scales for postnatal common mental disorder in Kintampo. Ghana. J Affect Disord 13(1–2), 109–117 (2009).
Uwakwe, R. Affective (depressive) morbidity in puerperal Nigerian women: validation of the Edinburgh Postnatal Depression Scale. Acta psychiatrica Scandinavica 107(4), 251–259 (2003).
Bouvet, C. & Battin, C. La recherche-action et l’étude psychosociale du rétablissement: l’exemple du Clubhouse Paris. Les méthodes qualitatives en psychologie clinique et psychopathologie https://doi.org/10.3917/dunod.casti.2021.01.0115 (2021).
Angers, M. Initiation pratique à la méthodologie des sciences humaines. (Illustrée : Centre Educatif et Culturel, 1992).
Teissedre, F. & Chabrol, H. Étude de l’EPDS (Échelle postnatale d’Edinburgh) chez 859 mères: dépistage des mères à risque de développer une dépression du post-partum. L’Encéphale 30(4), 376–381. https://doi.org/10.1016/S0013-7006(04)95451-6 (2004).
Guide d’intervention mhGAP pour la prise en charge des troubles mentaux, neurologiques et liés à l’utilisation de substances psychoactives dans les structures de soins non spécialisées - Version 1.0 [mhGAP intervention guide for mental, neurological and substance use disorders in nonspecialized health settings: mental health Gap Action Programme (mhGAP) – version 1.0]. Genève: Organisation mondiale de la Santé; (2011).
Association psychiatrique américaine. Manuel diagnostique et statistique des troubles mentaux, 5e, éd. American Psychiatric Publishing, DSM-V, Doi-org.db29.linccweb.org/https://doi.org/10.1176/appi (2013).
Jardri, R. Screening for postpartum depression: Qualitative review of the assessment studies of the edinburgh postnatal depression scale. Devenir 16, 245–262. https://doi.org/10.3917/dev.044.0245 (2004).
World Medical Association. World medical association declaration of helsinki: Ethical principles for medical research involving human subjects. JAMA 310(20), 191–194. https://doi.org/10.1001/jama.2013.281053 (2013).
Baubet, T., Taïeb, O., Moro, M.R., 15. Abord transculturel de la dépression », Michel Goudemand éd., Les états dépressifs. Lavoisier (2010), pp. 117–131.
Kaniz, G., Fisher, C., Algin, S. & Oosthuizen, J. Validation of the Bangla version of the Edinburgh postnatal depression scale for a Bangladeshi sample. J. Reprod. Infant Psychol. 25(4), 308–315. https://doi.org/10.1080/02646830701644896 (2007).
Acknowledgements
We would like to thank all the partners and staffs of the project in Cameroon for their role in contributing to the field and the teenage mothers for their participation.
Author information
Authors and Affiliations
Contributions
Joël Djatche Miafo: protocol design and conception; collection, analysis and interpretation of results; writing the first draft, revision and critical reading, have approved the version submitted and are responsible for it. Daniel Nzebou: conception, analysis and interpretation of results; writing the first draft, revision and critical reading, have approved the version submitted and are responsible for it. Beat Stoll: protocol design; analysis and interpretation of results; revision and critical reading, have approved the version submitted and are responsible for it. Joris Cathel Yimga Ngambia: writing the first draft, revision and critical reading, have approved the version submitted and are responsible for it. Marquise Kouo Ngamby Ekedy: writing the first draft, revision and critical reading, have approved the version submitted and are responsible for it. Saskia von Overbeck Ottino: writing the first draft, revision and critical reading, have approved the version submitted and are responsible for it. Amir Moayedoddin: protocol design and conception, writing the first draft, revision and critical reading, have approved the version submitted and are responsible for it.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Informed consent
Informed consent was obtained from all participants in involved in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Djatche Miafo, J., Nzebou, D., Stoll, B. et al. Validation of the Edinburgh postnatal depression scale and prevalence of depression among adolescent mothers in a Cameroonian context. Sci Rep 14, 30670 (2024). https://doi.org/10.1038/s41598-024-79370-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-79370-7
Keywords
This article is cited by
-
Depression among pregnant teenagers receiving antenatal care from primary healthcare facilities in Mbarara city, Southwestern Uganda
BMC Pregnancy and Childbirth (2025)
-
Prevalence and contributing factors of postpartum depression risk during the pandemic among women living in Baixo Alentejo at Portugal
Scientific Reports (2025)
