
Abstract
Dental plaque provides a proper environment for the growth and activity of bacteria responsible for periodontal diseases and caries. As a result, it should be removed by individuals to prevent periodontal diseases and caries. There are different mechanical and chemical plaque control methods. In one study is shown that dental plaque removal efficacy of dentifrice containing Ethylenediaminetetraaceticacid(EDTA)/Methylsulfonylmethane(MSM) was nearly five times that of commercially available fluoride toothpaste. In another study, authors found that xylitol-containing chewing gums caused a marked reduction in the count of Streptococcus Mutans compared to conventional ones. This difference was highly prominent in individuals with poor oral hygiene. In this study we assessed the synergic effects of Xylitol, EDTA and MSM in a chewing gum in comparison with chlorhexidine mouthwash. This study was a crossover, randomized clinical trial. Twenty-four patients were divided in two groups randomly. At the baseline scaling and root planing was done for each patient. Group1 used chlorhexidine mouthwash twice a day. Group2 used novel chewing gum for 15 min twice a day. After 14 days, for every patient O’leary plaque index, gingival index and sulcus bleeding index were reevaluated and recorded. Professional brushing was done for patients. 14 days were considered as wash-out period. After that, method of plaque control of groups was changed. After 14 days, all patients were reevaluated and recorded and were compared with previous data. Samples in 2 groups had no significant difference in age and sex. Paired sample t test revealed that there were significant differences between first and second period for O’leary plaque index, gingival index and sulcus bleeding index in Group1 (P < 0.05). But in Group2 there were no differences between first and second period for all indexes. Also independent sample t test showed that there were no significant differences between baseline, after first treatment and after second one for all indexes in both groups (P > 0.05). According to regression model results, type of treatment had no effect on mean of all indexes. According to our findings which showed the similar efficiency of novel chewing gum and chlorhexidine mouthwash in improving and reducing plaque and gingival indexes, we can conclude that novel chewing gum can be introduced as an effective, cheap and accessible tool for dental plaque control.
Similar content being viewed by others


Introduction
Dental plaque provides a favorable environment for the growth and activity of pathogenic bacteria causing periodontal diseases and dental caries1. Thus, the removal of this layer is necessary to prevent periodontal diseases and caries2.
Dental plaque is a pale-yellow biofilm that grows naturally on the surface of the teeth. Like any other biofilm, dental plaque is also formed by colonizing bacteria. Starter bacteria involved in developing the pellicle layer are usually gram-positive microorganisms, such as Actinomyces viscosus and Streptococcus sanguinis, which are replaced by secondary colonies of Prevotella intermedia, Capncytophaga, and Porphyromonas gingivalis strains during plaque maturation. Pathogenic species in chronic gingivitis are generally the gram-positives, including Streptococcus sanguinis, Streptococcus mitis, Streptococcus oralis, Actinomyces viscosus, and Actinomyces naeslundii, as well as the gram-negatives, including Fusobacterium nucleatum, Prevotella intermedia, Veillonella parvula, Haemophilus, Capncytophaga, and Campylobacter. The strains involved in dental caries are Streptococcus mutans, Streptococcus sobrinus, and Lactobacillus. Dental plaque mineralizes into calculus by absorbing mineral salts between 1 and 14 days after its formation. Calcium and phosphorus are the predominant ions in the calculus composition3.
Various mechanical and chemical methods exist for plaque control and eradication, including the toothbrush and dentifrice, dental floss, interdental brush, and mouthwash4,5.
Chlorhexidine (CHX) mouthwash is identified as the gold standard for preventing dental plaque formation6.
In recent years, chewing gums have been proven effective for caries control and plaque control7,8.
In addition to their mechanical plaque-removing capability, xylitol-containing gums can prevent plaque formation due to the bacteriostatic properties of xylitol and its effect on increasing salivary flow9.
Also according to the importance of oral microbiota and the incidence of pathogenic bacteria in the presence of dysbiosis, there are also chewing gums based on probiotics to maintain a state of homeostasis and reduce the incidence of bacterial plaque10.
Ethylenediaminetetraaceticacid (EDTA) as a chelating agent, is capable of bonding with calcium and phosphorus, thereby eliminating these two ions, which are necessary for plaque formation and maintenance11.
Methylsulfonylmethane (MSM) agent acts as a permeability enhancer for EDTA and improves its local performance12.
Xylitol, EDTA, and MSM are classified as Generally Regarded As Safe (GRAS) by the American Food and Drug Administration (FDA)13.
In a 2014 study by Ajdaharian et al. dental plaque removal efficacy of dentifrice containing EDTA/MSM was nearly five times that of commercially available Colgate Total® toothpaste14.
In 2015, Haghgoo et al. conducted a study and found that xylitol-containing chewing gums caused a marked reduction in the count of this bacterium compared to conventional ones. This difference was highly prominent in individuals with poor oral hygiene15.
Simmons et al. aimed to evaluate the efficacy of chewing gums containing Xylitol and Xylitol/chlorhexidine acetate on dental plaque and gingivitis. Plaque and gingival indices were significantly lower in groups using Xylitol/chlorhexidine acetate chewing gum than those using Xylitol chewing gum16.
Dadkhah et al. performed a comparative study on the effects of a novel dental gel on plaque and gingivitis compared to a commercially available triclosan-containing toothpaste. The novel EDTA-containing dental gel resulted in almost three times more plaque reduction and more than double bleeding on probing (BOP) reduction than conventional toothpaste17.
A study by Salomone et al. revealed that a combination of sodium hypochlorite and EDTA fully eradicated the calculus that was not removable by sodium hypochlorite alone18.
Given these considerations, this study investigates the synergistic effects of Xylitol, EDTA, and MSM combination as chewing gum on plaque control and compares its efficacy with chlorhexidine mouthwash. It is expected that this novel chewing gum be effective for dental plaque prevention.
Methods and materials
This study was an interventional and cross-over clinical trial. Study Protocol was approved by ethics committee of Hamedan university under IR.UMSHA.REC.1396.306 code and registered in IRCT database under IRCT2017070234849N1 code on 28/08/2017: https://irct.behdasht.gov.ir/trial/26521.
We confirm that all methods were performed in accordance with the relevant guidelines and regulations. This study was conducted in accordance with the Helsinki Declaration.
Sample size was determined according to former similar studies and the study design14,15,16,17.
Alpha, beta, sigma1,sigma2,mu1,mu2, Sample size (01, 2, 0.36, 0.141, 0.824, 1.2), α = 0.01, β = 0.2, n = 12.
Twenty-four patients with gingivitis presenting to the Periodontics Department of the Dental School of Hamadan University of Medical Sciences were recruited in this study. Inclusion criteria were having no systemic diseases, having no periodontal disease and having O’leary plaque index of above 50%. Exclusion criteria were adding any oral hygiene routine or need to any additional dental procedures, and occurrence of any disease requiring systemic medicines.
Randomization was computer generated using http://www.studyrandomizer.com.
The chewing gum production
The chewing gum base obtained from Pars-Minoo Industrial Company (Fig. 1) was used to prepare the chewing gum containing Na4EDTA, MSM, and Xylitol. These three agents were purchased from Pasargad Chemicals company, along with mint flavor and acesulfame sweetener. They were mixed with gum base by heating. Initially, the gum base was heated to 60 °C to reach a pasty state. Then, EDTA, MSM, and Xylitol were added and mixed thoroughly. After cooling to 40 °C, flavor, and sweetener were added to the gum paste. The paste was then flattened on a glass plate, from which 2.7 g pieces of chewing gum were separated (Fig. 2)19. Table 1 provides the composition and corresponding percentages of chewing gum19,20.
A 0.12% Chlorhexidine mouthwash manufactured by Behsa pharmaceutical company was used for the control group.

Chewing gum base.

The final samples of fabricated chewing gum.
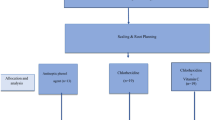
We confirm that informed consent was obtained from all subjects and/or their legal guardian(s). After obtaining written consent by signing the consent forms, scaling and root planing (SRP) with polishing were performed for each patient to reduce their plaque index to below 20%.
The O’leary plaque index, gingival index, and sulcus bleeding index21 were recorded for each patient. Then, the subjects were randomized into two groups of each twelve patients. This study carried out in the absence of any routine oral care procedure including brushing or flossing.
Group 1 (first chlorhexidine mouthwash, followed by chewing gum) used chlorhexidine mouthwash twice daily.
Group 2 (first chewing gum, followed by chlorhexidine mouthwash) used EDTA/MSM/Xylitol containing chewing gum twice daily for 15 min.
The plaque, gingival, and sulcus bleeding indices were recorded again for each patient after 14 days in the record forms. Polishing was repeated for each patient to reduce their plaque index to below 20%.
Then, a two-week wash-out period was given to the subject, in which they did not use any of the above plaque control methods. After this period, the assisted control plaque methods in the two groups were modified as follows:
Group 1 used EDTA/MSM/Xylitol-containing chewing gum twice daily for 15 min.
Group 2 used chlorhexidine mouthwash twice a day. As shown in Fig. 3.
The plaque, gingival, and sulcus bleeding indices were re-collected for each patient after 14 days in the record forms, and the obtained data were compared to previous data.
Lastly, polishing was repeated for each patient to reduce their plaque index to below 20%. The effective tooth brushing and plaque control methods were instructed to the patients. Moreover, the patients received a toothbrush and dental floss as a gift.

Allocation of patients to treatment groups.
All data was collected during January 2020 to June 2020 and all clinical periodontal parameters recorded by a single experienced clinician who was blind about groups and method of plaque control of each patient. Data analysis was carried out using SPSS software version 22. Statistical Analyst was blinded by hiding names of each group’s data.
Results
Descriptive statistics for the continuous variables were presented as mean, standard deviation, minimum and maximum values. The analyses on the patients achieved the following results.
Chi-square analysis revealed that study subjects in the two groups were not significantly different regarding gender (P > 0.05). (Supplementary Table 1)
An independent t-test suggested no significant difference in the mean age of study subjects between the two groups (P > 0.05). (Supplementary Table 2)
The paired t-test results found a significant difference in the mean O’leary plaque index of group 1 (mouthwash-chewing gum) between the first and second periods (P = 0.001), and the second treatment (chewing gum) showed the highest effectiveness. However, in the second group (chewing gum-mouthwash), there was no significant difference between the first and second periods regarding the mean O’leary plaque index (P = 0.275). Moreover, independent t-test analysis indicated no significant difference in the mean O’leary plaque index between groups 1 and 2 at baseline (P = 0.718). No significant difference in the mean O’leary plaque index was noticed between groups 1 and 2 after the first and second treatments (P > 0.05). (Supplementary Table 3)
The paired t-test results found a significant difference in the mean gingival index of group 1 (mouthwash-chewing gum) between the first and second periods (P = 0.001), and the second treatment (chewing gum) showed the highest effectiveness. However, in the second group (chewing gum-mouthwash), there was no significant difference between the first and second periods regarding the mean gingival index (P = 0.09). Moreover, independent t-test analysis indicated no significant difference in the mean gingival index between groups 1 and 2 at baseline (P = 0.29). No significant difference in the gingival index was noticed between groups 1 and 2 after the first and second treatments (P > 0.05). (Supplementary Table 4)
The paired t-test results found a significant difference in the mean sulcus bleeding index of group 1 (mouthwash-chewing gum) between the first and second periods (P = 0.001), and the second treatment (chewing gum) showed the highest effectiveness. However, in the second group (chewing gum-mouthwash), there was no significant difference between the first and second periods regarding the mean sulcus bleeding index (P = 0.08). Moreover, independent t-test analysis indicated no significant difference in the mean bleeding index between groups 1 and 2 at baseline (P = 0.422). No significant difference in the mean sulcus bleeding index was noticed between groups 1 and 2 after the first and second treatments (P > 0.05). (Supplementary Table 5)
However, given the regression model results in Supplementary Table 6, the treatment type did not affect the mean O’leary plaque index, i.e., the O’leary plaque index was not significantly different between the two treatments (P > 0.05).
Given the regression model results in Supplementary Table 7, the treatment type did not affect the mean gingival index, i.e., the gingival index was not significantly different between the two treatments (P > 0.05).
Given the regression model results in Supplementary Table 8, the treatment type did not affect the mean sulcus bleeding index, i.e., the sulcus bleeding index was not significantly different between the two treatments (P > 0.05).
Discussion
The results of a sub-group analysis by treatment type suggested no difference between the two groups regarding O’leary plaque, gingival, and sulcus bleeding indices. This means chewing gum had a similar effect to chlorhexidine mouthwash in reducing and improving these indices.
The treatment of periodontal diseases has evolved in recent years. Undoubtedly, non-surgical treatments significantly contribute to bacterial plaque reduction and tissue regeneration. Recently, herbal extracts, coenzymes, and specific vitamins have been utilized in non-surgical and non-mechanical (scaling and root planning) treatments to help regenerate oral tissue and enhance host resistance22.
Recently, Xylitol-containing chewing gums have found application as an efficient plaque control method in patients9.
Consistent with the findings of past studies22,23, the present study found no significant difference in age and gender between the two groups.
The analysis results for the O’leary plaque index found a significant difference in group 1 (mouthwash-chewing gum), which indicated the superiority of chewing gum in preventing dental plaque formation. However, this difference was non-significant in group 2 (chewing gum-mouthwash). The observed discrepancy can be due to the difference in using chewing gum and mouthwash between the two groups.
The same pattern was noticed for gingival and sulcus bleeding indices as well.
The analysis results indicated no difference in the mean O’leary plaque index at baseline between the two groups. Moreover, the obtained mean O’leary plaque index after the first period in group 1 (using mouthwash) was not significantly different from that of group 2 (using chewing gum), meaning that both interventions equally prevented plaque formation in the first period. Likewise, no significant difference was observed in the mean O’leary plaque index after the second period in group 1 (using chewing gum) compared to group 2 (using mouthwash). This finding reflects the similar effects of both treatments in preventing dental plaque formation.
In a similar observation, there was no significant difference in gingival and sulcus bleeding indices in the two treatment periods between groups 1 and 2, suggesting the similar effect of both treatments in improving patients’ gingival status.
A clinical study comparing the effect of Herboral (herbal extract) chlorhexidine mouthwash with chlorhexidine mouthwash showed the superiority of chlorhexidine for plaque control, despite the higher satisfaction of patients in using herbal mouthwash24. Another study examining the anti-plaque action of chlorhexidine-containing chewing gum highlighted its acceptable efficacy compared to a placebo25. However, this study lacked a comparison group using chlorhexidine mouthwash. So far, no better alternative has been introduced to replace chlorhexidine mouthwash26.
In this respect, we assessed the regression model of all indices to determine the superiority of treatments to each other. The results demonstrated that treatment type showed no difference in improving O’leary plaque, gingival, and sulcus bleeding indices, and both chlorhexidine mouthwash and the novel chewing gum produced similar efficacy.
The similar efficacy of this chewing gum to the mouthwash is considered a key achievement given that the chewing gum lacks the side effects of chlorhexidine mouthwash, including unpleasant taste, altered sense of taste, and staining of the teeth27. In addition, chewing gum is easily portable and can be consumed anywhere.
Conclusions
The findings of this study suggested the similar effectiveness of the novel chewing gum compared to chlorhexidine mouthwash in reducing and improving plaque and gingival indices. Thus,
This novel chewing gum can be considered an effective, inexpensive, and accessible way to control dental plaque and can be introduced as a daily routine for maintaining oral hygiene.
Suggestions
Further studies are suggested to compare the efficacy of this chewing gum with other commercially available chewing gums. Moreover, the long-term effects of this product need to be evaluated. Also we suggest expanded sample size and treatment time for further studies.
Data availability
Data is provided within the manuscript or supplementary information files.
References
Wolf, H. & Hassel, T. Color Atlas of Dental Hygiene. Thieme New York, 333 Seventh Avenue, New York, USA (2006).
Verkaik, M., Busscher, H., Jager, D. A., Abbas, F., & Van Der Mei, H. Efficacy of Natural antimicrobials in Toothpaste formulations against oral biofilms in Vitro. J. Dent.. 39 (3), 218–224 (2011).
Verkaik, M., Busscher, H., Jager, D., & Reddy, S. Essentials of clinical periodontology and periodontics. Third Edition (2011).
Pearce, E. Chemical methods of plaque control. Bull. N Z. Soc. Periodontal. 36, 15–17 (1973).
Westfelt, E. Rationale of mechanical plaque control. J. Clin. Periodontol. 23 (3), 263–267 (1996).
Balagopal, S. & Arjunkumar, R. Chlorhexidine: the gold standard antiplaque agent. J. Pharm. Sci. Res. 5 (12), 270 (2013).
Yeung, C. Y., Chu, C. H. & Yu, O. Y. A concise review of chewing gum as an anti-cariogenic agent. Front. Oral Health 2023 13(4), 1213523. https://doi.org/10.3389/froh.2023.1213523 (2023).
Pienihäkkinen, K., Hietala-Lenkkeri, A., Arpalahti, I. & Söderling, E. The effect of xylitol chewing gums and candies on caries occurrence in children: a systematic review with special reference to caries level at study baseline. Eur. Arch. Pediatr. Dentistry. 25(2), 145–160 (2024).
Makinen, K. K., Makinen, P.-L. & Pape, H. R., Allen, P., Bennet, C. A., Isokangas, P. J., & Isotupa, K. P. Xylitol chewing gums and Caries Rates:A 40-month Cohort Study. J. Dent. Res. 19, 55–63 (1995).
Butera, A. et al. Probiotic alternative to chlorhexidine in periodontal therapy: evaluation of clinical and microbiological parameters. Microorganisms. 9 (1), 69 (2020).
Fang, X., Keutgen, X. M., Jiang, Y., Sheretz, R., & Hachem, R. The role of chelators in preventing Biofilm formation and catheter-related Bloodstream Infections. J. Curr. Opin. Infect. Dis. 21(4), 385–392 (2008).
Zhang, M., Wong, I. G., Gin, J. B., & Ansari, N. H. Assessment of MethylSulfonylMethane as a permeability enhancer for Regional EDTA chelation therapy. J. Drug Deliv. 16(5), 243–248 (2009).
Kawashita, Y., Kitamura, M., & Saito, T. Early Childhood Caries. Int. J. Dent. 725320 (2011).
Ajdaharian, J., Dadkhah, M., & Wilder-smith, P. Multimodality imaging of the effects of a Novel dentrifrice on oral Biofilm. J. Lasers Surg. Med. 46 (7), 546–552 (2014).
Haghgoo, R., Afshari, E. & Ghanaat T,Aghazadeh, S. Comparing th efficacy of Xylitol-containing an conventional chewing gums in reducing Salivary counts of Streptococcus mutans:an in vivo study. J. Int. Soc. Prev. Commity Dent. 5 (2), 112–117 (2015).
Simmons, D., Beighton, D. & Kidd EA,Collier, F. I. The effect of xylitol and chlorehexidine acetate/xylitol chewing gum on plaque accumulation and gingival inflammation. J. Clin. Periodontal. 26 (6), 388–391 (1999).
Dadkhah, M., Chung, N. E., Ajdaharian,Wink, C., Klokkevold, P. & Wilder-Smith, P. Effects of a Novel Dental Gel on Plaque and Gingivitis:a comparative study. J. Dentistry. 4 (6), 239 (2014).
Salomone, J. L. & Brady, J. M. The Effects of EDTA on Denture Calculus: An Examination Using the Scanning Electron Microscope (Defense Technical Information Center, 1977).
Aslani, A. & Jalilian, F. Design, formulation and evaluation of caffeine chewing gum. Adv. Biomedical Res. 2 (1), 72 (2013).
Aslani, A., Jalilian, F., Gin, J., & Goswamy, A. Anti-plaque oral compositions. WO. 2014100775, A1 (2014).
Loe, H. The Gingival Index,the Plaque Index and the Retention Index systems. J. Periodontal. 38, 610–616 (1967).
Behfarnia, P., Aslani, A., Jamshidian, F. & Noohi, S. The efficacy of Green Tea chewing gum on Gingival inflammation. J. Dentistry (Shiraz Iran). 17 (2), 149–154 (2016).
Marchetti, E. et al. Alcohol-free essential oils containing mouthrinse efficacy on three-day supragingival plaque regrowth: a randomized crossover clinical trial. Trials. 18 (1), 154–156 (2017).
Malhotra, R., Grover, V., Kapoor, A. & Saxena, D. Comparison of the effectiveness of a commercially available herbal mouthrinse with chlorhexidine gluconate at the clinical and patient level. J. Indian Soc. Periodontology. 15 (4), 349–352 (2011).
Kolahi, J., Soolari, A., Ghalayani, P., Varshosaz, J. & Fazilaty, M. Newly formulated chlorhexidine gluconate chewing gum that gives both anti-plaque effectiveness and an acceptable taste: a double blind, randomized, placebo-controlled trial. J. Int. Acad. Periodontol. 10 (2), 38–44 (2008).
Mathur, S., Mathur, T., Srivastava, R. & Khatri, R. Chlorhexidine: The Gold Standard in Chemical Plaque Control. Natl. J. Physiol. Pharm. Pharmacol. 1 (2011).
Prasanna, S. V. & Lakshamanan, R. Characteristics, uses and side effect of chlorhexidine: a review. J. Dent. Med. Sci. 15 (6), 57–59 (2016).
Funding
No external funding, apart from the support of the authors’ institution, was available for this study.
Author information
Authors and Affiliations
Contributions
Morteza Shakhsi Niaee: Concept/Design, Data analysis/interpretation, Data collection, Drafting article.Morad Hedayatipanah: Critical revision of article, Approval of article.Parviz Torkzaban: Critical revision of article, Approval of article.Tayyeb Mohammadi: Statistics, Data analysis/interpretation.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Shakhsi Niaee, M., Hedayatipanah, M., Torkzaban, P. et al. A chewing gum containing ethylenediaminetetraaceticacid (EDTA), methyl sulfonyl methane (MSM) and xylitol works comparable to chlorehexidine mouthrinse. Sci Rep 14, 28200 (2024). https://doi.org/10.1038/s41598-024-79551-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-79551-4
