
Abstract
This study explores the dynamic of emergency department (ED) access during heat waves. Given the importance of avoiding overcrowding and long waits in an ED, it is important to explore all the possible determinants of ED inflows. We shed some light on the impact that heat waves have on this dynamic, via a quantitative analysis of the number of ED visits in the Campania region of Italy during the summers between 2016 and 2019. Aggregating individual-level data, we examine the relationship between extreme heat events and number of ED visits, controlling for social, demographic and economic characteristics. Our findings, obtained through Random Effects Poisson and fractional probit estimations, show that heat waves above 39 perceived degrees Celsius significantly increase the number of ED visits, revealing the impact that heat waves have on ED utilization in Campania. Insights for local public health strategies and emergency preparedness initiatives are discussed.
Similar content being viewed by others

Introduction
Emergency departments (ED) are one of the most important parts of a national health system. As with all scarce goods, EDs operate with limited resources1, and in consequence resource optimization is crucial. Moreover, EDs are a significant public cost in countries that have public health systems that provide their citizens with healthcare. Optimizing the delivery of health services, and emergency care in particular, is thus paramount. It is even more important in contexts where services are publicly funded, as market-driven incentives for efficiency are largely absent. A trivial implication of this is the importance of studying the determinants of public inflows at hospitals, as a means of optimizing their efficiency. Indeed, being able to forecast increases in demand for health services makes it possible to modulate the presence of medical and paramedical personnel more efficiently, and generally to prepare for public demand, thereby delivering better health services.
While such improvement would seem to be of use to many kinds of health services, the case of EDs is of special interest for at least three reasons. First, understanding the determinants that influence the public’s use of EDs is essential for enhancing departmental functionality in addressing emergent health needs. Given that by their very nature these departments work with emergencies, it seems crucial to improve their functionality as much as possible. Second, efficient allocation of medical and nursing personnel is vital from an economic point of view, given the significant resource allocation and costs associated with ED operations. These must be optimized to prevent unnecessary expenditure, and obtain the most from investments. Given the resources allocated to this crucial sector, their optimization seems fundamental if the best possible outcomes are to be obtained. Third, optimizing ED functions would reduce patients’ waiting time, and hence mitigate any premature departures. This also seems to be a crucial point, as such departures signal deficiencies in the delivery of urgent medical care; the importance of quality assurance measures is to be emphasized. The departure of a patient from an ED before completion of treatment indicates shortcomings in the ability of the emergency care system to fulfil its mandate2. It has already been proposed that such premature departures serve as a valuable metric for assessing the quality of emergency care delivery3. More generally, early departures from EDs have been an important focus of health policy researchers’ attention, given the importance of this subject when it comes to optimizing EDs4,5,6,7,8. Recognizing the significance of these factors underscores how imperative it is to understand ED utilization patterns comprehensively, thereby informing policy interventions aimed at enhancing departmental efficacy.
Given all the above, in order to optimize the delivery of high-quality services in EDs, it seems very important to understand what affects inflows to these departments. Indeed, only when (at least some of) the determinants of ED demand have been unveiled, will it be possible to design policies that can improve the efficacy of ED departments. Previous studies have recognized that there are many factors that influence the dynamic of ED crowding. These go from substance abuse9, to the strategic behaviour of hospitals in aiming to serve insured patients10. It logically follows that many of these determinants are not predictable, and hence are of questionable use when it comes to structuring policies to improve ED services and functioning.
On the other hand, the literature has also suggested that climate has an important impact on ED visits, and in particular that heat waves can affect inflows of patients to hospitals. Over the last two decades advancements in atmospheric observations, numerical weather prediction, and data assimilation techniques have significantly improved the accuracy of weather forecasts11, and day by day the models continue to improve12. Heat waves produce an increased risk of hospitalizations13, adverse birth outcomes14, as well as catastrophic death tolls, as suggested by the over 14,000 excess deaths that occurred during the 2003 French heat wave15. Hence, the literature suggested that heat waves cause significant death tolls, and that policies are needed that address this16. It follows that a study on the impact of heat waves on ED inflows is important, providing findings that may give policymakers indications on how climate changes affect the inflows of patients to these finely balanced departments.
Previous literature has already highlighted that heat waves have a significant impact on hospital emergency departments, leading to an increase in admissions and mortality. Studies in various locations, including hospitals in the state of Virginia in the USA17, Australia18, and in England19(Johnson et al., 2004), have all reported a rise in ED presentations and hospital admissions during heat waves. These studies also highlight the specific health issues that are exacerbated by heat, such as diabetes, pregnancy complications, and injuries. Moreover, examining the impact of heat waves on health, some studies have provided findings that shed light on the repercussions on ED visits and mortality rates across various regions. Notably, a study conducted in Brisbane, Australia, investigated the surge in ED visits during heat wave events between 2000 and 201220. Defined by consecutive days with daily maximum temperatures surpassing 34–37 °C, heat waves saw a substantial increase in ED presentations, with vulnerable demographics such as children and the elderly facing heightened risks. Moreover, the severity of cases, as indicated by high-acuity visits, escalated significantly during these periods, as did prolonged ED stays. Similarly, an analysis of the 2006 California heat wave21 underscored the statewide surge in ED visits, which was particularly pronounced in the Central Coast region. Children aged 0–4 years and individuals aged over 65 were particularly susceptible, with a rise observed in presentations related to acute renal failure, cardiovascular diseases, and diabetes. Correspondingly, hospitalization rates for heat-related illnesses surged, highlighting the pervasive impact of heat waves on morbidity. A parallel study in Brisbane22 reaffirmed the increase in ED visits during heat waves, accentuating the vulnerability of specific age groups and the persistence of high-acuity cases. Concurrently, investigations in Izmir, Turkey23 underscored the disproportionate toll heat waves exact on the elderly, amplifying mortality rates among individuals aged 75 and above. Ozturk et al.24 also found an increase in mortality, particularly among elderly males, in their study of the heatwaves in the Fethiye province in Turkey. Other articles have focused, meanwhile, on the impact of heat waves on patients’ conditions. Waheed and co-authors25 found that heat waves may lead to a higher mortality rate, particularly among those with a history of cerebrovascular accidents. These findings underscore the need for hospitals to be prepared for increased demand during heat waves, and for public health interventions to mitigate the impact on vulnerable populations. Collectively, all these studies elucidate the profound ramifications of heat waves on public health, necessitating tailored interventions to mitigate risks, particularly among vulnerable populations. The findings underscore the imperative of evidence-based thresholds and action plans to safeguard communities against the escalating health impacts of heat waves. Such insights stress the pressing need for preparedness and adaptation strategies to mitigate the burgeoning health risks associated with heat wave events.
Nonetheless, to the best of our knowledge no study so far has focused on a number of hospitals, observed for a time span lasting several years, with previous studies focusing mostly on exceptional heat waves as a sort of natural experiment. This seems to be a very important gap in the literature, given that these exogenous shocks may have other effects, which may in turn lead to an increase (or decrease) in ED visits. Moreover, observing short time frames may hinder these studies’ external validity, and hence the generalization of the results. Furthermore, to the best of our knowledge no study has analysed Italy as a case study, even though it seems a highly suitable candidate. It is a country with a temperate Mediterranean climate, which means that heat waves, when they occur, have a significant impact on the population. At the same time, in Italy most citizens use public healthcare, which is funded largely by taxpayers’ contributions, and final users typically encounter minimal or no direct fees for services rendered26. This implies smaller differences between EDs than those observed in countries with other kinds of healthcare systems. Moreover, in Italy EDs operate around the clock, receiving patients either through ambulance services or by self-referral. Upon assessment, triage categorizes patients for admission, prioritization, or discharge, assigning a colour code based on severity (white, green, yellow, red, or black). This system reflects the urgency of treatment needed. However, it is important to highlight that Italian EDs face challenges from increased demand, resulting in higher costs and operational constraints due to limited staffing and budget al.locations1. All these aspects, taken jointly, would seem to make Italy a very interesting case study to analyse, and one that would help to fill the aforementioned gap in the empirical literature.
Data limitations make a nationwide analysis infeasible and would likely introduce biases due to variations in health governance, as health affairs in Italy are managed at the regional, and not national, level. Within Italy, Campania stands out as an intriguing case study. Located in southern Italy along the Tyrrhenian Sea, it is the country’s third-most populous region and includes some of Europe’s most densely populated urban areas. Campania experiences hot, dry summers and mild winters, with considerable disparities in healthcare access and quality between rural and urban areas, potentially influencing ED usage across different sub-populations. Additionally, the region faces significant socioeconomic challenges, including one of Italy’s highest poverty rates, which could heighten vulnerability to climate-related health issues. These factors make Campania a compelling focus for this study, with its distinctive climate, socioeconomic conditions, and healthcare infrastructure’s adaptive capacity. The region’s Mediterranean climate, population density, urban structure (particularly in Naples), and aging population amplify its vulnerability to heatwaves, offering a distinct context to examine the impact of extreme heat on healthcare systems.
By means of a quantitative analysis, with the use of Poisson and Fractional Probit estimators, exploiting data about all the patients that went to hospital in Campania in the summers from 2016 to 2019 (to ensure the COVID-19 crisis and relevant policies do not have any effect on our results), we aim to study the effect of heat waves on ED visits. Our results suggest that heat waves above 39 perceived degrees Celsius lead to a statistically significant increase in the number of ED visits. Given the predictability of heat waves thanks to improvements in meteorological forecasting, this finding may be a useful first step for policymakers interested in fine-tuning ED resources and personnel to improve the performance of these departments.
Methods
To identify the impact of a heat wave on ED inflows within a quantitative framework, we first needed to define what a heat wave is. This is unfortunately still a debated topic in the literature. Heat waves, defined as periods of excessively hot weather, are a growing concern due to their potential to cause weather-related deaths and their likely increase in frequency, severity, duration, and territorial extent in the future27. The impacts of heat waves are wide-ranging, and include drought, urban heat islands, excess hospital admissions, and mortality28. These events have been linked to climate change, with a significant increase in the number of heat wave days per year29. Despite their potential to cause harm, there is still a lack of a unified index for defining heat waves, a fact that in itself underscores the need for further research and the development of strategies for adaptation to hot weather29. Several studies have proposed their own definitions30,31, but a commonly agreed one remains elusive, in part because of the very nature of heat waves, which are a phenomenon that varies from place to place, and whose impact depends to a large extent on local characteristics and the meteorological norm32.
There is no universally accepted definition for heatwaves. The World Meteorological Organization defines a heatwave as a period where local excess heat accumulates over a sequence of unusually hot days and nights. Researchers commonly rely on similar parameters, such as daily maximum, minimum, or average temperatures. Threshold values - either fixed or relative - determine whether a temperature qualifies as a heatwave. A third key factor is the duration of elevated temperatures, typically assessed over consecutive days. Setting the appropriate threshold is critical, as what constitutes extreme heat varies by region; for example, 35 °C might be typical for Mediterranean areas but extreme for Baltic regions32. After setting the temperature threshold, the duration must also be defined, as consecutive temperatures above the threshold over shorter periods identify more frequent heatwaves, while longer periods result in fewer instances. Thus, it is essential to carefully determine the duration criteria24.
Existing studies utilize various indices to gauge heat exposure. Among these, Steadman’s apparent temperature33,34,35, also known as the Heath Index (HI), stands out as a widely-used index in environmental health research, forming the basis for heat advisories in numerous US communities, probably also thanks to its adoption by the National Oceanic and Atmospheric Administration. We chose to adopt this index in this work, thereby focusing on so-called “perceived temperature”, rather than atmospheric temperature. The HI index combines air Temperature (T) and Relative Humidity (RH) to measure how hot the weather actually feels to a human being, which makes it appropriate for studying the impact heat has on human health. When RH is high, the evaporation rate of perspiration slows, the body cools less efficiently, and thus humans retain heat, with damaging consequences for health. HI translates prevailing weather conditions into a single scale akin to the temperature that humans perceive when the dew point temperature is 14 °C33,36. By restricting the variables to air temperature and moisture, HI provides a practical measure of heat exposure33. HI is most effective for temperatures over 26 °C and relative humidity over 40%, making it perfect for assessing the perceived temperature in the southern Italian summer, where these thresholds are always met.
Several algorithms have been proposed to approximate Steadman’s original apparent temperature values37, which are not always coherent or equivalent38. In this study we computed HI using the algorithm employed by the NWS online heat index calculator (https://www.wpc.ncep.noaa.gov/html/heatindex.shtml, URL accessed on 13/5/24) to determine HI based on air temperature in degrees Celsius (T) registered during the day, and relative humidity as a percentage (H). The following Eq. (1) results:
We applied this transformation to data about temperature and humidity gathered from NASA Power, with T the maximum registered temperature during the day, bilinearly interpolated to obtain T and H in the centre of each of the 550 municipalities in the Campania region for every day of the summers from 2016 to 2019. We thus obtained a HI, an index measuring the perceived temperature value, for each of the municipalities and days included in the study. Using these data, we built a set of dichotomous dummies for different perceived temperatures, which assume the value of 1 when the HI had a value in a municipality equal or superior to each HI value between 36 °C and 44 °C for three consecutive days. In this way we built the variables signalling the HW for each of these different thresholds. Three days of high temperatures is the threshold adopted by several countries (Denmark, where the threshold is 28 °C (https://web.archive.org/web/20080723170544/http://www.dmi.dk/dmi/danmark_faar_varme-_og_hedeboelge, URL accessed on 13/5/24); Greece, where the threshold is 39 °C (http://www.emy.gr/emy/el/, URL accessed on 13/5/24), and the North-East of the US, with a threshold of 32.2 °C). Other countries, such as Sweden or the Netherlands, adopt 5 consecutive days of heat as their definition of a heat wave, usually with a lower threshold in terms of temperature; nonetheless, in line with a part of the literature24,39, we prefer the former standard, since the latter definition seems to be oriented more towards agriculture and other more resilient fields, and has less of an impact on human health.
As well as these, the key independent variables in our regression analysis, we also required information about ED inflows. These were gathered from the STAR-EMUR dataset for Regione Campania on ED admissions in each hospital of the region. This source, the only official one for Italy, is compiled for the Italian Superior Institute of Health (Istituto Superiore di Sanità, ISS) by each hospital, and offers micro-level data about every patient in all the hospital EDs in the Campania region.
To control for other possible determinants of this relationship, we included a set of control variables on the right-hand side of our equation. To prevent demographic differences in the population from affecting the analysis, following previous literature on the subject40, and assuming that differently aged people have different demands for EDs, we included five variables representing the share of the population of the municipality (residents on 1 January of each year) aged between 25 and 34 years old, 35 and 44, 45 and 54, 55 and 64, and 65 and 74 (data taken from the Italian National Statistical Agency, ISTAT). Furthermore, both income and education levels (which are usually considered as being correlated to health literacy) have been suggested as being important determinants of ED visits5,8,41,42,43); hence, we included an operationalization of the former via the average personal taxable income from work for the municipality (data taken from the Italian Revenue Agency), and an operationalization of the latter via the share of population that holds a secondary level diploma (high school level, data taken from ISTAT). Finally, to complete this matrix of municipality-level demographic controls we included population density (data taken once again from ISTAT). To discriminate for less important ED visits, we also included a variable representing the share of patients that have been coded as green during the triage process. Finally, to prevent temporary or geographical effects from affecting our analysis, we included a matrix of fixed effects composed of dichotomous dummies signalling July, August, and September of each year (hence excluding June, which serves as a reference modality), and each province into which the 550 municipalities are divided (with the exclusion of Napoli, the region’s capital and its biggest city, which is the omitted, and hence reference, modality). Both the exclusions are motivated by the need to avoid multicollinearity and the so-called dummy trap. By including fixed effects we aim to prevent any local or temporary specificity from affecting our results.
All these operations led to the creation of a dataset composed of observations for each of the 550 municipalities of the Campania region, observed in each of the 94 days of summer (from 21 June to 22 September), for each of the four years analysed (2016–2019, when we decided to interrupt the analysis to prevent the COVID-19 emergency from affecting our results), giving a total of 206,800 observations. Descriptive statistics about these variables are presented in Table 1.
Once this dataset was built, we ran a number of regressions to estimate the correlations between HW and ED inflows. In more formal terms, we estimated the following Eq. (2):
where ED is the dependent variable, operationalized in four different ways. In the main regressions, ED is either the bare number of ED admissions from a given municipality m per each day d, or the per capita number of ED admissions (ED pc) for each municipality m per each day d. As a further investigation, we assessed whether heat waves lead to more severe cases in the ED. Accordingly, we modified the dependent variable in Eq. (2), calculating it not as the sum of all the cases, but rather only the cases that were labelled as Red (hence severe) in the triage process at the ED check-in.
This dependent variable is modelled as a function of four matrixes:
-
Demo, a matrix composed of eight variables, describing the demographic characteristics of the municipality’s population in each year y. Five identify the demographic composition of the population (25–34 y.o., 35–44 y.o., 45–54 y.o., 55–64 y.o., and 65–74 y.o.); Log Income pc expresses the logarithm of the per capita income of the municipality; Secondary expresses the share of the population with a secondary school diploma (high school level); Dens computes the population density of the municipality. All data are from ISTAT with the exception of Log Income pc, which is computed by the authors from data from the Italian Revenue Agency;
-
Green, a variable indicating the share of ED admissions from the municipality m on day d that were labelled as green (and hence less severe) codes during the triage;
-
HW_X, a dichotomous dummy variable identifying whether there was a heat wave in municipality m on day d, i.e. whether the temperature was at least X in the last three days. X assumes, in different regressions, any value between 36 and 44 degrees Celsius, to study the different effects of heat waves with different levels of intensity;
-
Fixed, a matrix of dichotomous dummy variables comprising both province-level fixed effects, and month-level fixed effects, to reduce the impact of any specificity of the geographical or temporal characteristics on the results.
Since the dependent variable in Eq. (2) is a count variable, namely, the total number of ED admissions from a given municipality, we opted to use a Poisson (with random effects) as an estimator. Moreover, to prevent the different sizes of the municipalities studied from biasing the results, we also used the number of ED admissions for the municipality divided by the population, i.e. in per capita terms, using in this case a Fractional Probit as estimator. Both choices are the most obvious ones, given the nature of our dependent variable, which is either a count variable or a share if expressed in per capita terms44,45.
Results
Our quantitative analysis, utilizing both Poisson and Fractional Probit estimators, examined the dynamic of ED visits in Campania during the summer months spanning from 2016 to 2019, excluding more recent data, which are likely to be affected by the COVID-19 emergency and which may thus potentially bias the findings. Heat waves were defined as three consecutive days of warm temperatures, following the definition of the meteorological services of a number of countries. We observed a statistically significant increase in ED visits during these heat waves, when these reached at least 39 °C of perceived temperature. This indicates that temperature extremes have a discernible impact on ED utilization. This finding underscores the importance of understanding climate-related factors in healthcare resource management and policy formulation to enhance ED efficiency.
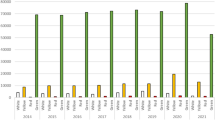
The marginal effects of the estimation of Eq. (2) through a population-averaged Poisson estimator are summarized in Fig. 1, which illustrates the impact of various heat wave thresholds, ranging from 36 °C to 44 °C. Detailed results of the regression are provided in Table A1 in the appendix. Furthermore, employing the Fractional Probit estimator, which takes per capita ED visits from each municipality as the dependent variable, we present the corresponding marginal effects of the estimation in Fig. 2, covering the same range of heat wave thresholds. These results are also tabulated in detail in Table A2 in the appendix. In both figures, solid and dashed lines denote 95% and 90% confidence intervals, respectively.

Random Effect Poisson estimation – All cases – Marginal Effects.

Fractional Probit estimation – All cases - Marginal Effects.
An examination of Fig. 1 reveals a consistent trend indicating an increase in ED visits with increasingly intense heat waves, which becomes particularly noticeable from 39 °C upwards, when the coefficient becomes statistically significant. This observation is generally corroborated by the findings depicted in Fig. 2, although variations at specific temperatures (in particular 42 °C and 43 °C) may be attributed to the limited statistical power of the regression, resulting from data scarcity for this particular temperature threshold. This is why it was not advisable to replicate the analysis with temperatures over 44 °C, since heat waves with such high temperatures are uncommon.
Overall, these results suggest a robust correlation between heat waves and ED visits, with the critical temperature threshold for observing this effect identified at 39 °C. The similarity in trend and dynamics of marginal effects across both estimators lends further support to the reliability of our findings and indicates their independence from the choice of estimation method.
As a further result, we investigated whether heat waves cause an increase in the severe cases that arrive in EDs. It may be that heat waves only cause mild symptoms, which cause more people to go to the ED without really needing to do so. Figures 3 and 4 present results for the replication of the previous analysis, with the dependent variable this time the number, and the variable in per capita terms, of ED visits coded as red during the triage process, in other words the most severe. As can be seen in the figures, in this case too there is an increase of red cases once more intense heat waves have begun. This suggests that the increase noticed in Figs. 1 and 2 is not composed of milder cases, but also includes more severe cases.

Random Effects Poisson estimation – Only Red Cases - Marginal Effects.

Fractional Probit estimation – Only Red Cases - Marginal Effects.
Discussion
This research, conducted using observational data from Campania, Italy, from 2016 to 2019, explores the impact that heat waves have on ED visits. The findings underscore the vulnerability of healthcare systems to climate-related events, emphasizing the need for proactive measures in resource allocation and personnel management within EDs. These results align with previous literature highlighting the heightened burden on EDs during heat waves17,18,19. Moreover, our study contributes to existing knowledge by identifying that, in the case of Campania, a critical temperature threshold of 39 °C was that beyond which the increase in ED visits becomes statistically significant. Furthermore, we confirmed that these are not only mild cases (which would, nonetheless, be dangerous in any case due to the potential overcrowding of the ED), since when we observe the dynamic for red cases only, i.e. the most severe cases, the dynamic is very similar to that overall due to the increase in non-specified cases once more intense heat waves are underway.
These findings have two principal implications for healthcare providers and policymakers. First, healthcare providers must anticipate and prepare for the surge in ED visits during heat waves by augmenting staffing levels and allocating resources accordingly. Proactive measures such as implementing heat wave response plans and enhancing community outreach programs can help mitigate the strain on EDs and ensure timely and efficient patient care. Second, policymakers must integrate climate adaptation strategies into healthcare policy frameworks to address the emerging challenges posed by climate change. Initiatives such as investing in climate-resilient infrastructure and promoting public awareness campaigns on heat wave preparedness can enhance the resilience of healthcare systems as a beneficial side effect, and minimize adverse health outcomes associated with extreme heat events.
In comparing our findings with previous literature, it is evident that the impact of heat waves on ED visits is a global phenomenon, transcending geographical boundaries and healthcare settings. Studies conducted in various regions, including the USA, Australia, and England, have consistently reported a surge in ED presentations during heat wave periods20,21,22. The universality of this trend underscores the urgency of adopting proactive measures to mitigate the impact of climate change on healthcare systems worldwide.
The present study provides empirical evidence of the significant impact of heat waves on ED visits, highlighting the need for coordinated action from healthcare providers and policymakers to enhance the resilience of healthcare systems against climate-related events. By leveraging insights from this research and building upon existing knowledge, stakeholders can collaboratively develop and implement strategies to safeguard public health and improve the effectiveness of emergency healthcare services in the face of climate change.
More precisely, our findings indicate that, on average, in the Campania region of Italy, in the summers from 2016 to 2019, a HW with temperatures reaching 39 °C resulted in an increase of approximately 0.0458 ED visits per day of residents from the affected municipalities. This increment holds significance when considered in the context of the numerous municipalities potentially affected by such extreme weather events, as well as the escalating frequency and intensity of heat waves in recent years. Moreover, the impact becomes even more pronounced with higher temperatures, with daily ED visits rising to approximately 0.0977 and 0.0957 during heat waves reaching 43 °C and 44 °C, respectively. These escalating figures underscore the escalating strain on healthcare systems during extreme heat events, and show that proactive measures are needed to bolster emergency healthcare preparedness and resilience.
Conclusions
In conclusion, our study sheds light on the substantial impact of heat waves on ED visits in a large Italian region, with our quantitative analysis revealing a statistically significant increase in ED utilization during prolonged periods of elevated perceived temperatures, particularly when they exceed 39 °C. These findings provide critical insights for healthcare providers and policymakers, highlighting the urgency of proactive measures to manage the surge in ED visits during heat wave events.
While it offers insights into the ED dynamic that may lead to an optimization of these crucial departments, it is however imperative to acknowledge that our analysis is not exempt from some limitations. These include a reliance on observational data from a specific Italian region and a relatively limited time span, which may introduce some bias, although it is important to highlight that a four-year span is a longer timeframe than any considered in previous similar studies.
Moving forward, further research is needed to explore the underlying mechanisms driving the observed increase in ED visits during heat waves and to evaluate the effectiveness of interventions aimed at mitigating this phenomenon. Future studies could focus on the category most affected by heat waves while adopting a multi-disciplinary approach, integrating meteorological data with socio-economic indicators to gain a comprehensive understanding of the factors influencing ED utilization during extreme weather events. Longitudinal studies spanning multiple regions and time periods would also be valuable in assessing the temporal and spatial variability of heat wave effects on ED visits, enabling the development of more targeted and effective policy interventions to enhance healthcare system resilience in the face of climate change. By addressing these research gaps, stakeholders can develop evidence-based strategies to improve emergency healthcare delivery and safeguard public health amidst the growing challenges posed by climate variability and change.
Data availability
Data will be made available upon reasonable request from the correspondent author (vincenzo.alfano@uniparthenope.it).
References
Scaletti, A. Evaluating investments in health care systems: health technology assessment (Springer, 2014).
Hsia, R. Y. et al. Hospital determinants of emergency department left without being seen rates. Ann. Emerg. Med. 58(1), 24–32 (2011).
Mataloni, F., Colais, P., Galassi, C., Davoli, M. & Fusco, D. Patients who leave Emergency Department without being seen or during treatment in the Lazio Region (Central Italy): Determinants and short term outcomes. PLoS One 13(12), e0208914 (2018).
Carmel, A., Amital, H., Shemer, Y. & Sahar, A. Why do they leave? Clinical characteristics of patients who leave the emergency room against medical advice. Harefuah 134(6), 445–449 (1998).
Khanna, R., Chaudhry, M. & Prescott, M. V. Emergency department patients who leave the department without being seen by a doctor. Eur. J. Emergency Med.: Off. J. Eur. Soc. Emergency Med. 6(3), 233–235 (1999).
Lee, K. M., Wong, T. W., Chan, R. P. & Lau, C. C. A study of patients who leave without notice in an A & E department. Accid. Emerg. Nurs. 6(2), 118–121 (1998).
Lerner, B. H. Patients leaving emergency departments without being seen by a physician. JAMA 267(2), 231–232 (1992).
Liao, H. C. et al. Emergency department patients who leave without being seen by a doctor: The experience of a medical center in northern Taiwan. Chang Gung Med. J. 25(6), 367–373 (2002).
D’Onofrio, G., Becker, B. M. & Woolard, R. H. The impact of alcohol, tobacco, and other drug use and abuse in the emergency department. Emergency Med. Clin. North Am. 24(4), 925–967 (2006).
Handel, D. A. et al. Emergency department throughput, crowding, and financial outcomes for hospitals. Acad. Emergency Med.: Off. J. Soc. Acad. Emergency Med. 17(8), 840–847 (2010).
Schulze, G. C. Atmospheric observations and numerical weather prediction. South African J. Sci. 103, 318–323 (2007).
Wiston, M. & Mphale, K. M. Weather forecasting: From the early weather wizards to modern-day weather predictions. J. Climatol. Weather Forecast. 6, 1–9 (2018).
Anderson, G. B., Bell, M. L. & Peng, R. D. Methods to calculate the heat index as an exposure metric in environmental health research. Environ. Health Perspect. 121(10), 1111–1119 (2013).
Basu, R., Malig, B. & Ostro, B. High ambient temperature and the risk of preterm delivery. Am. J. Epidemiol. 172, 1108–1117 (2010).
Hémon, D. et al. Surmortalité liée a la canicule d’août 2003 en France. Bull Epidémiol Hebd. 45–46, 221–225 (2003).
Zhao, Q. et al. Global, regional, and national burden of heatwave-related mortality from 1990 to 2019: A three-stage modelling study. PLoS Med. 21(5), e1004364 (2024).
Davis, R. E. & Novicoff, W. M. The impact of heat waves on emergency department admissions in Charlottesville, Virginia, U.S.A. Int. J. Environ. Res. Public Health, 15, (2018).
Lindstrom, S. J., Nagalingam, V. & Newnham, H. H. Impact of the 2009 Melbourne heatwave on a major public hospital. Internal Medicine Journal, 43, (2013).
Johnson, H., Kovats, S., McGregor, G.R., Stedman, J.R., Gibbs, M., Walton, H. & Cook, L. The Impact Of The 2003 Heat Wave On Mortality And Hospital Admissions In England. Epidemiology, 15. (2004)
Toloo, G. S., Yu, W., Aitken, P., FitzGerald, G. & Tong, S. The impact of heatwaves on emergency department visits in Brisbane, Australia: A time series study. Critical Care 18, R69–R69 (2014).
Knowlton, K. et al. The 2006 California heat wave: Impacts on hospitalizations and emergency department visits. Environ. Health Perspect. 117, 61–67 (2008).
Wang, X. Y. et al. The impact of heatwaves on mortality and emergency hospital admissions from non-external causes in Brisbane, Australia. Occup. Environ. Med. 69, 163–169 (2011).
Oray, N. Ç., Oray, D., Aksay, E., Atilla, R. & Bayram, B. The impact of a heat wave on mortality in the emergency department. Medicine 97, e13815 (2018).
Ozturk, Y., Baltaci, H. & Akkoyunlu, B. O. The impacts of heat waves on hospital admissions and mortality in the Fethiye Province of Turkey. Portuguese J. Public Health 41(2), 94–101 (2023).
Waheed, S., Baig, M. A., Khursheed, M. & Awan, S. Impact of heat waves on patients presenting to the emergency department of a tertiary care hospital - A single center cross-sectional study. JPMA J. Pakistan Med. Associat. 69(5), 741–744 (2019).
France, G., Taroni, F. & Donatini, A. The Italian healthcare system. Health Econ. 14(S1), S187–S202 (2005).
Robinson, P. J. On the definition of a heat wave. J. Appl. Meteorol. 40, 762–775 (2001).
Marx, W., Haunschild, R., Bornmann, L. Heat Waves - a hot topic in climate change research. ArXiv, abs/2106.13537 (2021).
Smith, T. T., Zaitchik, B. F. & Gohlke, J. M. Heat waves in the United States: definitions, patterns and trends. Climatic Change 118, 811–825 (2013).
Raei, E.S., Nikoo, M.R., Aghakouchak, A., Mazdiyasni, O., Sadegh, M. (2018). GHWR, a multi-method global heatwave and warm-spell record and toolbox. Scientific Data, 5.
Tomczyk, A. M. & Bednorz, E. Heat waves in Central Europe and tropospheric anomalies of temperature and geopotential heights. Int. J. Climatol. 39, 4189–4205 (2019).
Kilbourne, E.M. Heat Waves and Hot Environments (2011).
Baltaci, H., Ozturk, Y. & Akkoyunlu, B. O. Long-term variations and synoptic features of heat waves in Turkiye. Int. J. Global Warm. 33(1), 51–68 (2024).
Steadman, R. G. The assessment of sultriness. Part I: A temperature-humidity index based on human physiology and clothing science. J. Appl. Meteorol. 18, 861–873 (1979).
Steadman, R. G. The assessment of sultriness. Part II: Effects of wind, extra radiation and barometric pressure on apparent temperature. J. Appl. Meteorol. 18, 874–885 (1979).
Steadman, R. G. A universal scale of apparent temperature. J. Climate Appl. Meteorol. 23, 1674–1687 (1984).
Rothfusz, L. P. The Heat Index “Equation” (or, More Than You Ever Wanted to Know About Heat Index). SR 90–23. Fort Worth, TX: National Oceanic and Atmospheric Administration, National Weather Service, Office of Meteorology. (1990)
Ahrens, C. D. Meteorology Today: An Introduction to Weather, Climate, and the Environment (Brooks/Cole, 2007).
Anderson, G. B. et al. Heat-related emergency hospitalizations for respiratory diseases in the Medicare population. Am. J. Respiratory Critical Care Med. 187, 101098–101103 (2013).
Agovino, M., Musella, G., Pisano, S. & Scaletti, A. Assessing the impact of tourist flows on emergency department treatment speed for residents and tourists. The case of Sorrento. Socio-Econ. Plan. Sci. 77, 101004 (2021).
Cognetti, G., Poltronieri, E., De Castro, P., Scarinci, V. & Perilli, R. Searching health information on the Internet: Results of a survey in a cohort of 414 elderly people in Italy. J. Med. Internet Res. Preprints 04(08/2019), 15760 (2019).
Palumbo, R., Annarumma, C., Adinolfi, P., Musella, M. & Piscopo, G. The Italian Health Literacy Project: Insights from the assessment of health literacy skills in Italy. Health Policy 120(9), 1087–1094 (2016).
Velasco, V., Gragnano, A., Vecchio, L. P., HBSC Gruppo Regionale Lombardia 2018. Health Literacy Levels among Italian Students: Monitoring and Promotion at School. Int. J. Environ. Res. Public Health 18, 9943 (2021).
Cameron, A. C. & Trivedi, P. K. Microeconometrics Using Stata Rev. (Stata Press, 2010).
Pampel, F. C. Logistic Regression: A Primer (SAGE, 2000).
Funding
This research was funded by the University of Naples “Parthenope” within the Competitive Research Project “A multidisciplinary approach to the study of the relationship between heat waves and the population’s health.”
Author information
Authors and Affiliations
Contributions
V.A. cured the data and performed the analysis, V.A., F.S. and A.S. conceptualized the idea and wrote the main manuscript text and F.S. and A.S. secured fundings and provided supervision. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Alfano, V., Serini, F. & Scaletti, A. Addressing heatwave impacts on hospital admissions in an Italian region. Sci Rep 14, 27994 (2024). https://doi.org/10.1038/s41598-024-79652-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-79652-0
Keywords
This article is cited by
-
People-centered cooling: protecting health against hazardous heat, from the person to the planet
International Journal of Biometeorology (2025)
