
Abstract
Anatomy-based guidelines for shoulder surgery have established the routine preoperative evaluation of the humeral head. Despite recognized sex differences in humeral head size, there has been limited investigation into sex-specific variations in acromiohumeral contact surface (AHCS) arc length. This study aims to assess sex differences in the AHCS arc length within a sample of the Chinese population. We retrospectively analyzed 169 normal shoulder CT images from a single medical center, collected between 2011 and 2021. The AHCS arc length was defined as the distance from the superior glenoid tubercle to the lateral edge of the greater tuberosity, measured using a three-dimensional reconstruction algorithm. Physiological reference values for the AHCS arc length were determined at three abduction angle intervals. Linear regression analysis was used to assess the correlation between the AHCS arc length and abduction angle in both sexes. The reference values for AHCS arc length were significantly lower in women across three abduction angle intervals (male 48.07 ± 3.37 mm vs. female 43.54 ± 2.54 mm, (0–10] °, p < 0.001; male 45.07 ± 2.34 mm vs. female 40.78 ± 2.06 mm, (10–20] °, p < 0.001; male 42.08 ± 2.03 mm vs. female 38.09 ± 2.44 mm, > 20 °, p = 0.001, respectively). Additionally, the AHCS arc length was linearly and negatively correlated with the abduction angle (male R2 = 0.436, p < 0.001; female R2 = 0.434, p < 0.001, respectively). The present study identified a significant sex difference in the anatomical AHCS arc length in a sample of the normal Chinese population. Preoperative assessment of the AHCS arc length may be necessary for certain shoulder surgeries in the future.
Similar content being viewed by others

Introduction
Understanding the morphological features of the proximal humerus is essential not only for the anatomical design of prosthetics in arthroplasty but also for enhancing preoperative planning to improve clinical outcomes for patients. In clinical practice, accurately measuring the humeral head diameter (HHD), posterior offset (PO), and retroversion angle is crucial for successful total shoulder arthroplasty1. Similarly, accurately determining the shoulder acromiohumeral contact surface (AHCS) arc length is crucial for managing tendon-graft length in superior capsule reconstruction2. The performance of postoperative shoulder functionality may be compromised by the inadequate assessment of the AHCS arc length of the proximal humerus. Despite anatomical deviations in the humeral head between females and males, there has been limited research on sex-specific differences in AHCS arc length3.
Measurements of the AHCS arc length may be biased by different surgeons during superior capsule reconstruction surgery. To accurately investigate the morphometric features of the AHCS arc length, measurements should be conducted at a shoulder abduction angle of 20–30°4. Tibone et al.. found that the AHCS arc length measured at 20° or 40° of glenohumeral abduction angle resulted in reduced postoperative subacromial pressure5. However, little is known about the correlation between shoulder abduction and the AHCS arc length in females and males6.
The objectives of this study were to evaluate sex differences in the AHCS arc length measurements of the shoulder and to characterize their correlation with shoulder abduction as assessed through three-dimensional (3D) computed tomography (CT) imaging.
Materials and methods
Ethics approval
All procedures involving human participants and/or human medical records were conducted in accordance with the ethical standards set forth by the local institutional ethics committee, as well as the 1975 Helsinki Declaration and its subsequent amendments or comparable ethical guidelines. The protocol received prior review and approval from the local Ethics and Research Committees.
Study design and patients
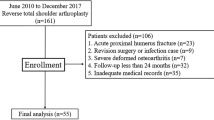
This retrospective observational study analyzed upper limb CT images obtained from January 2011 to January 2021 at the radiology department of an academic medical center in China. Eligible participants included all examinations conducted through the Picture Archiving and Communication System (PACS) during this period. Exclusion criteria encompassed patients with shoulder fractures, shoulder osteoarthritis, rotator cuff tears, shoulder deformities, shoulder instability, scoliosis, upper limb bone tumors, immunological disorders, and poor-quality imaging. Notably, patients aged under 20 years or over 49 years were also excluded. Additionally, images which were unable to perform shoulder abduction angle measurements (defined as the angle between the axis of the proximal humerus and the line of the spinous process of the spine) were excluded (Fig. 1). Following the application of these inclusion and exclusion criteria, a total of 169 cases from the normal Chinese population were included in the final analysis. All images were reviewed by two senior orthopedic surgeons, with independent examination results documented. Any discrepancies in interpretation were resolved by consensus. The study cohort was categorized into three interval of shoulder abduction angle groups (Table 1).

Flowchart diagram of the study. A total of 169 patients were included in the final analysis.
CT analysis parameters, methods of measurement and definition of shoulder AHCS arc length
Shoulder CT scans were performed using a 64-row CT scanner (Aquilion; Toshiba Medical Systems Corporation, Otawara, Japan). The CT data were stored in the Digital Imaging and Communications in Medicine (DICOM) format. The shoulder AHCS was measured using 3-Matic software (version 12.0; Materialise, Leuven, Belgium)6,7. We first imported three-dimensional surface models of the scapula and humerus into the 3-Matic software and selected six landmarks located around the articular surfaces to define the anatomical neck plane (the plane that best fits the selected landmarks). The epiphyseal sphere was defined as the sphere that best fits the articular surface, and the humeral head diameter (HHD) was defined as the diameter of this epiphyseal sphere. A coordinate system was then established based on the metaphyseal cylinder (the cylinder that best fits the proximal part of the humeral shaft). The proximal humeral shaft axis was designated as the inferior-superior axis (X-axis), the anterior-posterior axis (Z-axis) was defined as the axis on the plane of the anatomical neck perpendicular to the X-axis, and the mediolateral axis (Y-axis) was defined as the axis perpendicular to the X-Z plane. Finally, an arc was drawn in the X-Y plane connecting the superior glenoid tubercle, the superior vertex of the humeral head surface, and the lateral edge of the greater tuberosity, with the length of this arc defined as the shoulder AHCS arc length (Fig. 2). Additionally, we measured the acromiohumeral distance (AHD) as a reference value for established anatomical parameters of the shoulder joint between females and males7. AHD was used in relation to acomiohumeral distance as opposed to AHCS arc length. The AHD was measured using the same method as reported in previous studies8.
All imaging parameters were measured independently and in a standardized manner by two senior orthopedic surgeons. After a two-week interval from the initial measurement, both investigators conducted independent re-measurements using the same procedures and techniques to evaluate the reliability of all parameters.

Creation of the coordinate system for representative 3D surface models and measurement of AHCS arc length. (a) The plane of the anatomical neck was established using six landmarks located along the perimeter of the articular surface. The epiphyseal sphere is defined as the sphere that best fits the articular surface (center, O) and has a diameter equivalent to the humeral head diameter (HHD). (b) The coordinate system was defined based on the axis of the proximal humeral shaft and the plane of the anatomical neck. (c) The shoulder AHCS arc length, defined as the distance from the superior glenoid tubercle to the lateral edge of the greater tuberosity (DSGT), was measured in the X-Y plane (blue arc). (Not to scale).
Data process and statistical analysis
The data for both males and females were found to be non-normally distributed according to the Shapiro-Wilk test (p > 0.05). The Mann-Whitney U test was employed to evaluate the differences in AHCS arc length at the same abduction angle between sexes, as well as the differences across various abduction angles within the same sex. Pearson’s correlation coefficient and linear regression analyses were conducted to assess the relationship between shoulder AHCS arc length and shoulder abduction angles. Intra- and interobserver reliability were determined using intraclass correlation coefficients (ICC), with a 95% confidence interval. Results are presented as mean ± standard deviation. Statistical analyses were performed using SPSS Statistics version 22.0.0.0 (IBM Corp., Armonk, NY, USA), with statistical significance set at p < 0.05.
Results
Study population
This study included 169 participants, with a median age of 35.02 [26.29–43.75] (males: 33.42 ± 8.60 years, females: 37.46 ± 8.42 years, comprising 67 females (39.64%). The final analysis included a total of 77 left shoulders (45.56%) and 92 right shoulders (54.44%) (Table 2). The humeral head diameter (HHD) of the participants was measured as 43.67 ± 3.27 mm [38.40–50.50 mm] (males: 45.30 ± 2.87 mm, females: 41.07 ± 1.89 mm). The shoulder abduction angle was 8.52 ± 8. 18° [0.02–33.62] (males: 7.91 ± 7.83°, females: 9.44 ± 8.66°). The shoulder abduction group (0–10] ° accounted for 71.01% of the total participants (Table 1). The intra-observer reliability, as measured by the intraclass correlation coefficient (ICC), ranged from 0.896 to 0.971, indicating excellent reliability, while the inter-observer reliability ranged from 0.954 to 0.984 (Table 3).
Sex differences of the AHCS arc length
The mean reference value for the AHCS arc length was 45.09 ± 4.20 mm. We found no statistically significant difference in AHCS arc length between the left (45.10 ± 4.31 mm) and right (45.07 ± 4.13 mm) shoulders. However, the AHCS arc length was significantly greater in males (46.99 ± 3.69 mm) compared to females (42.19 ± 3.15 mm) (p < 0.001). Notably, significant differences were observed between females and males across all three abduction angle groups (all p < 0.01) (Fig. 3; Table 3). Additionally, the acromiohumeral distance (AHD) was assessed to provide reference values for established acromiohumeral anatomical measurements of the shoulder joint. The AHD was significantly greater in males (7.85 ± 0.95 mm) compared to females (7.40 ± 0.85 mm) (p = 0.016) in the abduction group (0–10].

Statistical analysis between the abduction angle and the AHCS arc length. The letters ‘a’ and ‘b’ denote the marking methods used for comparisons among different abduction angle groups. An asterisk (*) indicates a significant difference in comparisons within the female group, with p < 0.05.
The correlation between abduction angle and AHCS arc length
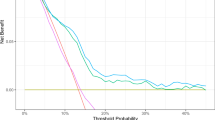
For subgroups analysis, a negative linear correlation was observed between the abduction angle and the AHCS arc length in both males (R2 = 0.436, AHCS arc length = 49.450 − 0.312 × abduction angle, p < 0.001) and females (R2 = 0.434, AHCS arc length = 44.457 − 0.240 × abduction angle, p < 0.001) (Fig. 4). In addition, a weak positive correlation (R² = 0.144, p = 0.020) was observed between the AHCS arc length and the humeral head diameter in females. However, this correlation was not present in males.

Linear regression analyses of the abduction angles and the AHCS arc length. Line-regression analysis was conducted to illustrate the relationship between abduction angles and AHCS arc length in both sexes.
Discussion
Accurate understanding of the anatomical acromiohumeral contact surface (AHCS) arc length is critical for diagnosing shoulder disorders, planning surgical interventions, and developing rehabilitation protocols aimed at restoring normal shoulder function9. Abnormalities or changes in AHCS arc length may indicate shoulder pathologies such as impingement syndrome, rotator cuff tears, or osteoarthritis10. However, little is known about sex differences in AHCS arc length. In this study, we performed 3D reconstructions of 169 CT images from healthy Chinese participants and measured anatomical parameters to establish reference values for the AHCS arc length (Fig. 5). Our findings revealed that the AHCS arc length was significantly shorter in females compared to males. Additionally, the AHCS arc length was negatively correlated with the abduction angle.

The study flowchart illustrates sex differences in AHCS arc length, which may inform future preoperative planning for shoulder surgeries.
Research has demonstrated sex-specific differences in musculoskeletal anatomy11. The acromion tends to be smaller and more hooked in females compared to males, potentially influencing the AHCS arc length and the subacromial space12. From an evolutionary perspective, males may have developed larger, stronger shoulders to support physically demanding tasks, while females may have evolved greater flexibility and range of motion for activities requiring dexterity. Males typically have a larger humeral head, which can result in variations in how the humerus interacts with the acromion. In our study, the AHCS arc length was significantly greater in men (46.99 ± 3.69 mm) than in women (42.19 ± 3.15 mm) (p< 0.001). This finding suggests that, in general, females may have a narrower subacromial space13. The reduced space could impact the arc length and contact surface during shoulder movements, potentially contributing to a higher incidence of impingement syndromes. Presumably if the subacromial space is narrower and the humerus lies superior then the AHCS arc length will be larger. Additionally, females typically exhibit greater shoulder flexibility and range of motion, which may further influencing the dynamics of the AHCS arc length during various activities14.
Biomechanical analyses suggest that males generally possess greater muscle mass and strength around the shoulder, which may influencing joint stability and the forces exerted on the AHCS15. These differences in muscle strength and mechanics can alter loading patterns, thereby affecting the AHCS. Another important factor is the effect of sex hormones. Estrogen may play a role in the development and maintenance of musculoskeletal tissues. Hormonal differences can impact bone density, ligament laxity, and muscle composition, contributing to variations in shoulder anatomy and biomechanics16.
Understanding sex differences is essential for developing personalized treatment plans. For instance, surgical techniques in superior capsule reconstruction may need to be tailored to account for anatomical variations. Notably, no geographically related differences were observed in the AHCS values (Table 4). Lee et al. and Cline et al. measured the AHCS arc length (at 30° shoulder abduction) on the surgical side in Korean and American patients, respectively17,18. No statistical differences were found between the AHCS arc lengths. Interestingly, the reported AHCS arc lengths in previous studies were similar to those in the current study at 0°, 15°, and 30° shoulder abduction angles, with variations ranging from 3.25 mm to 4.65 mm. Our results indicate that the reference value for AHCS arc length is linearly and negatively correlated with the abduction angle in both sexes, suggesting that preoperative planning should select the appropriate abduction angle for measuring the AHCS arc length19. Interestingly, our results revealed a weak positive correlation (R² = 0.144, p= 0.020) between the reference AHCS arc length and humeral head diameter in female participants. However, this correlation was not observed in males, suggesting that skeletal differences between male and female specimens may not directly account for the variation in AHCS arc length. Additionally, Pennington et al. reported that the AHCS arc length in patients undergoing superior capsule reconstruction was significantly smaller than before surgery20. Therefore, we hypothesize that the difference in AHCS arc length pre- and postoperatively may be attributed to the inferior displacement of the humeral head following surgery21.
We further analyzed AHD as a reference value for established acromiohumeral anatomical measurements in the shoulder joint between females and males. Notably, previous studies have suggested that thicker tendon grafts in superior capsule reconstruction patients may result in favorable outcomes24. However, Baek et al. found that using a tendon graft thicker than a patient’s preoperative AHD may increase the risk of graft retear and subacromial erosion post-surgery25. As the shoulder abduction angle increases from 0° to 34°, the AHD progressively decreases, consistent with the findings of Giphart et al.26. This may be attributed to the continuous change in the coordinates of the closest distance between the humeral head and the acromion, with muscle dynamics also playing a role. Overall, the similarity between AHD values reported in previous studies and our findings suggests that our measurement methods are reliable for further application.
This study has several limitations. First, we reported AHCS arc length measurements from a relatively small sample of 169 patients, which may not fully capture the sex differences across different age groups. However, it is worth noting that the sample included both male and female participants from a wide age range, indicating reasonable representation. Additionally, the unequal age distribution between male and female participants may have introduced bias, potentially influencing the interpretation of the retrospective findings. Considering the sex-based variances in bone structure may be the contributing factor to the difference in AHCS arc length, personal measurements maybe have a better predictive value of AHCS arc length than adjusting sex alone. Future studies should aim to include larger sample sizes and a more diverse population to improve the reliability and validity of the results. Finally, since the participants were recruited from a single academic medical center, further multi-institutional studies are needed to confirm these findings.
Conclusions
In summary, our study found that women had a shorter AHCS arc length compared to men across all three abduction angle intervals. Additionally, the reference values for AHCS arc length were linearly and negatively correlated with the abduction angle in both sexes. These findings support the need for sex-specific standardization of AHCS arc length measurements, which is crucial for individualized preoperative planning in shoulder joint surgery.
Data availability
The datasets used and/or analyzed in the current study are available from the corresponding author on reasonable request.
References
Cohn, M. R., Austin, L. S., Williams, G. R. & Abboud, J. A. Elliptical Humeral Head implants in Anatomic Total Shoulder Arthroplasty. J. Am. Acad. Orthop. Surg. 31 (21), 1112–1119 (2023).
Mihata, T. et al. Arthroscopic Superior Capsule Reconstruction for Irreparable Rotator Cuff tears: comparison of clinical outcomes with and without subscapularis tear. Am. J. Sports Med. 48 (14), 3429–3438 (2020).
Jung, S. W., Kim, D. H., Park, T. H., Park, J. Y. & Jeon, J. M. Humeral head coverage in arthroscopic partial repair of massive rotator cuff tears improves functional outcomes: an analysis of influential factors. J. Shoulder Elb. Surg. 31 (11), 2233–2241 (2022).
Pasqualini, I., Brinkman, J. C., Tokish, J. M. & Denard, P. J. Surgical Management of massive irreparable cuff tears: Superior Capsule Reconstruction and Rotator Cable Reconstruction. Curr. Rev. Musculoskelet. Med. 17 (4), 101–109 (2024).
Tibone, J. E. et al. Human dermal allograft Superior Capsule Reconstruction with graft length determined at Glenohumeral Abduction Angles of 20 degrees and 40 degrees decreases joint translation and subacromial pressure without compromising range of motion: a cadaveric biomechanical study. Arthroscopy 38 (5), 1398–1407 (2022).
Graichen, H. et al. Sex-specific differences of subacromial space width during abduction, with and without muscular activity, and correlation with anthropometric variables. J. Shoulder Elb. Surg. 10 (2), 129–135 (2001).
Ohta, S., Komai, O. & Onochi, Y. Outcomes of superior capsule reconstruction for massive rotator cuff tears and risk factors for postoperative retear. Arch. Orthop. Trauma. Surg. 140 (10), 1319–1325 (2020).
Chen, X. et al. He W and others. In Vivo Anatomical Research by 3D CT Reconstruction determines Minimum Acromiohumeral, Coracohumeral, and glenohumeral distances in the human shoulder: evaluation of Age and Sex Association in a sample of the Chinese Population. J. Pers. Med. 12 (11), 1804 (2022).
Herrmann, S. J., Izadpanah, K., Sudkamp, N. P. & Strohm, P. C. Tears of the rotator cuff. Causes–diagnosis–treatment. Acta Chir. Orthop. Traumatol. Cech. 81 (4), 256–266 (2014).
Takayama, K., Shiode, H. & Ito, H. Acromial and humeral head osteolysis following superior capsular reconstruction using autologous tensor fascia lata graft. J. Shoulder Elb. Surg. 31 (7), 1479–1487 (2022).
Tosi, L. L., Templeton, K., Pennington, A. M., Reid, K. A. & Boyan, B. D. Influence of sex and gender on Musculoskeletal conditions and how they are reported. J. Bone Joint Surg. Am. 106 (16), 1512–1519 (2024).
Gulcu, A., Aslan, A., Dincer, R., Ozmanevra, R. & Huri, G. Relationship between diagnostic anatomic shoulder parameters and degenerative rotator cuff tears: an MRI study. Orthop. J. Sports Med. 10 (11), 23259671221130692 (2022).
Kjaer, B. H., de Wandele, I., Spanhove, V., Juul-Kristensen, B. & Cools, A. M. Subacromial space outlet in female patients with multidirectional instability based on Hypermobile Ehlers-Danlos syndrome and hypermobility spectrum disorder measured by ultrasound. J. Shoulder Elb. Surg. 29 (3), 600–608 (2020).
Gruber, M. S. et al. Age- and gender-related differences in the morphology of Cuff tear Arthropathy: A Cross Sectional Analysis. J. Funct. Morphol. Kinesiol. 8 (1), 8 (2023).
Myers, N. L., Farnsworth, J. L., Kennedy, S. M. & Knudson, D. V. Upper Extremity Musculoskeletal profiles in Tennis players: a systematic review. Sports Health 16 (6), 931–937 (2024).
Tashjian, R. Z. et al. Estrogen and testosterone supplementation improves tendon healing and functional recovery after rotator cuff repair. J. Orthop. Res. 42 (2), 259–266 (2024).
Lee, S. J. & Min, Y. K. Can inadequate acromiohumeral distance improvement and poor posterior remnant tissue be the predictive factors of re-tear? Preliminary outcomes of arthroscopic superior capsular reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 26 (7), 2205–2213 (2018).
K, E. C. et al. Superior Capsule Reconstruction using Fascia Lata Allograft compared with double- and single-layer dermal allograft: a Biomechanical Study. Arthroscopy 37 (4), 1117–1125 (2021).
Bodine, M. et al. Arthroscopic latarjet procedure does not lead to loss of clinically significant external rotation at 0 degrees and 90 degrees of shoulder abduction. JSES Int. 6 (6), 1023–1028 (2022).
PenningtonWT, BartzBA, PauliJM, WalkerCE & SchmidtW Arthroscopic Superior Capsular Reconstruction with Acellular dermal allograft for the treatment of massive irreparable rotator cuff tears: short-term clinical outcomes and the Radiographic parameter of Superior Capsular Distance. Arthroscopy 34 (6), 1764–1773 (2018).
Baek, G. et al. Biomechanical Comparison between Superior Capsular Reconstruction and Lower Trapezius Tendon transfer in Irreparable Posterosuperior Rotator Cuff tears. Am. J. Sports Med. 52 (6), 1419–1427 (2024).
Mihata, T. et al. Biomechanical Effect of Thickness and Tension of Fascia Lata Graft on Glenohumeral Stability for Superior Capsule Reconstruction in Irreparable Supraspinatus tears. Arthroscopy 32 (3), 418–426 (2016).
Lee, S. J., Min, Y. K., Chung, I. K., Kang, S. W. & Banks, S. A. Comparison of dynamic in vivo shoulder kinematics before and after Superior Capsular Reconstruction for Irreparable Rotator Cuff tears. Orthop. J. Sports Med. 9 (1), 2325967120970502 (2021).
Hasegawa, A. et al. Postoperative graft integrity affects clinical outcomes after superior capsule reconstruction using fascia lata autograft in posterior-superior rotator cuff tears: a multicenter study. J. Shoulder Elb. Surg. 32 (7), 1476–1485 (2023).
Baek, C. H. & Kim, J. G. Shoulder Superior Capsular Reconstruction Hybrid Graft Thickness Greater Than Preoperative Acromiohumeral Distance increases Graft Retear Rate and Subacromial Erosion. Arthroscopy 38 (6), 1784–1792 (2022).
Giphart, J. E., van der Meijden, O. A. & Millett, P. J. The effects of arm elevation on the 3-dimensional acromiohumeral distance: a biplane fluoroscopy study with normative data. J. Shoulder Elb. Surg. 21 (11), 1593–1600 (2012).
Acknowledgements
The schematic diagram Fig. 5 was drawn by Figdraw (https://www.figdraw.com/static/index.html).
Funding
This research was supported by the Guangzhou Key Research and Development Project (No. 2023B03J0211) and the Science and Technology Planning Project of Guangdong Province (No. 2023A1515012621).
Author information
Authors and Affiliations
Contributions
X.C., Tz.L., C.L., and K.W. conceived and designed the experiments; Jh.R., Sw.S., and Xy.L. provided image data base, gave conceptual advice and commented on the manuscript; Xp.Y., Yb.C., and Sh.J. contributed to the experiments and the manuscript preparation; X.C, Tz.L., Sh.J. and K.W. analyzed the discussions and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Informed consent statement
Written informed consent was obtained from the patients to publish this paper.
Institutional review board statement
The protocol was previously reviewed and approved by Third Affiliated Hospital of Sun Yat-sen University Ethics and Research Committees ([2022]02-013-01), and with the 1975 Helsinki Declaration and its later amendments or comparable ethical standards.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, X., Liang, T., Liu, C. et al. Sex differences in shoulder acromiohumeral contact surface arc length on three-dimensional computed tomography imaging. Sci Rep 14, 28813 (2024). https://doi.org/10.1038/s41598-024-80336-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-80336-y
