
Abstract
Subarachnoid hemorrhage (SAH) is a severe cerebrovascular disorder characterized by the sudden influx of blood into the subarachnoid space. The use of sedatives may be associated with the prognosis of SAH patients. We obtained SAH data from the MIMIC-IV database. The receiver operating characteristic curve, Delong test, and decision curve analysis were used to assess the predictive value of sedatives. Propensity score matching (PSM) method was applied to match samples at a 1:1 ratio. Logistic regression analysis, generalized linear regression analysis, and stratified analysis were used to investigate the association of the sedative with in-hospital mortality and length of hospital stay (LOS). Finally, a competing risk analysis was performed to evaluate the survival probability with two potential outcomes. Dexmedetomidine had a better prognosis value than Propofol and Midazolam. After PSM analysis, the Dexmedetomidine and the non-Dexmedetomidine groups had 248 samples each. The application of Dexmedetomidine reduced the risk of in-hospital mortality but might prolong the LOS. When considering in-hospital mortality as a competing risk factor for LOS, Dexmedetomidine was a protective factor for in-hospital mortality but had no significant relationship with LOS. In conclusion, treatment of Dexmedetomidine could reduce the risk of in-hospital mortality with satisfactory predictive efficiency.
Similar content being viewed by others

Introduction
Subarachnoid hemorrhage (SAH) is a severe cerebrovascular disorder characterized by the sudden influx of blood into the subarachnoid space, leading to a rapid increase in intracranial pressure and posing a significant threat to the patient’s life1. The pathogenesis of SAH is complex and often associated with the rupture of cerebral aneurysms, vascular malformations, hypertension, and other factors2,3. Despite advancements in medical technology, diagnostic and therapeutic approaches for SAH continue to evolve, with advanced imaging techniques such as computed tomography scans, magnetic resonance imaging, and digital subtraction angiography enabling rapid and accurate diagnosis4,5,6. Surgery and endovascular treatments also offer more options for patients7,8. However, the morbidity and mortality rates of SAH remain high, particularly for patients with massive bleeding and rapidly deteriorating conditions, whose prognosis is often poor9. Recent studies have highlighted the importance of early intervention and aggressive management in improving outcomes for SAH patients10.
During the management of SAH, the care of patients is particularly critical. Sedative drugs are widely used in intensive care units (ICUs) to alleviate patient anxiety, pain, and discomfort, aiding patients in better cooperating with treatment11. The use of sedatives can reduce the patient’s stress response, lessen the physiological and psychological burden caused by pain and anxiety, and help maintain stable vital signs12. Nevertheless, the use of sedatives is controversial. On the one hand, excessive or inappropriate sedation may delay the recovery of consciousness and affect the assessment and recovery of neurological function13; on the other hand, appropriate sedation may help control intracranial pressure, reduce the occurrence of complications such as cerebral edema and vasospasm14,15. Therefore, the application of sedatives in SAH patients requires more refined management to ensure effective symptom control.
In this context, this study aims to explore the use of sedative drugs in SAH patients and their impact on clinical outcomes. By analyzing the use of sedatives, and the clinical responses of patients, we hope to provide more scientific and personalized guidance for the treatment of SAH patients, thereby improving their prognosis and quality of life.
Methods
Study population and data collection
This retrospective cohort study was obtained from the Medical Information Mart for Intensive Care (MIMIC) IV database. According to the requirements of the MIMIC database, one author extracted the data using structure query language with Navicat after completing the Collaborative Institutional Training Initiative course and passing both the “Conflicts of Interest” and “Data or Specimens Only Research” exams.
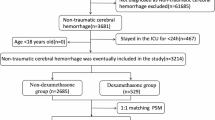
A total of 2808 samples with SAH in MIMIC IV were finally screened and included according to the progress as shown in Fig. 1. The extracted data included: (1) demographics, including age (years) and gender; (2) the length of in-hospital stay (LOS, days), which is the difference between admission time and discharge time; (3) vital signs, such as heart rate, systolic blood pressure (SBP), diastolic blood pressure (DBP), and percutaneous arterial oxygen saturation (SpO2); (4) laboratory indicators, including white blood cells (WBC), platelet count (PLT), creatinine, partial thromboplastin time (PTT); (5) severity of illness scores at admission, including the Simplified Acute Physiology Score II (SAPS II), Glasgow Coma Scale (GCS), and WFNS grade. (6) comorbidities, including cerebrovascular disease, chronic pulmonary disease, paraplegia, renal disease, malignant cancer, hyperlipemia, diabetes, and coronary heart disease; (7) treatment: sedative drugs, including Propofol, Midazolam, and Dexmedetomidine; mechanical ventilation; (8) etiology: traumatic brain injury and aneurysmal subarachnoid hemorrhage.

Workflow of exclusion and inclusion as utilized to select the 527 patients.
To avoid possible bias, variables were excluded if they had more than 20% missing values. Variables with less than 20% missing data were processed by multiple imputations using a random forest algorithm (trained by other non-missing variables) by the “mice” package of R software.
Exposure and outcomes
According to the use of sedative drugs, the patients were divided into seven groups. Three single drug groups: the patients were only treated with Propofol, Midazolam, or Dexmedetomidine. The combination of two drug groups: the patients were treated with Propofol + Midazolam, Propofol + Dexmedetomidine, or Midazolam + Dexmedetomidine. The last group was treated with three drugs.
The primary endpoint of the present study was in-hospital all-cause mortality, and the second endpoint was LOS.
Statistical analysis
The statistical analysis of the data extracted from the MIMIC-IV database was conducted using SPSS (version 19.0) and R software (version 4.1.3), with the aid of various packages specifically designed for biomedical research, such as ‘dplyr’ and ‘pROC’. Continuous variables were presented as mean (standard deviation) or median (interquartile range) depending on their distribution, as assessed by the Shapiro-Wilk test. Categorical variables were expressed as frequencies and percentages. To compare baseline characteristics between different groups, independent t-tests or Mann-Whitney U tests were used for continuous variables, and chi-square tests or Fisher’s exact tests were employed for categorical variables, as appropriate. To assess the discriminative ability of the sedatives, receiver operating characteristic (ROC) curves were constructed, and the area under the curve (AUC) was calculated. The Delong test was used to assess the difference in AUCs. Decision curve analysis (DCA) was also adopted to evaluate their clinical efficacy and select an optimal sedative.
Then, propensity score matching (PSM) was applied to minimize the imbalance of variables between the two sedative groups using the ‘Statsmodels’ package in Python. Patients were matched at a 1:1 ratio by the nearest neighbor matching method. Absolute standardized difference (ASD) was used to assess the balance of variables. ASD value was divided into four sections: <0.2, 0.2 ≤ ASD ≤ 0.5, 0.5 < ASD ≤ 0.8, and > 0.8, which respectively indicates excellent, good, sub-optimal, and poor balance between the two groups16. Adjusted variables: the variables significantly distributed between patients treated with or without Dexmedetomidine before PSM including SAPS II, PTT, cerebrovascular disease, hyperlipemia, gender, age, and WFNS grade were adjusted. Subsequently, logistic regression and generalized linear regression analyses were adopted to analyze the association of the sedative with in-hospital mortality and LOS. Crude model 1; model 2: adjusted for remaining unbalanced variables after PSM analysis; model 3: adjusted for balanced variables after PSM. Moreover, stratified analysis was conducted to compare the deaths and LOS between the two sedative groups. As a competing risk event, in-hospital death might shorten the LOS. Therefore, we employed the cumulative incidence function (CIF) and competing risk model to compare in-hospital mortality and LOS between groups using the ‘tidycmprsk’, ‘rms’, ‘survival’, and ‘ggsurvfit’ packages in R. The cumulative incidence of discharge from the hospital was determined by the Fine-Gray test with in-hospital mortality as a competing risk. Statistical significance was set at p < 0.05 for all analyses.
Results
Population and baseline characteristics
The baseline characteristics of patients with SAH are shown in Table S1 according to in-hospital mortality (yes or no). Patients in the death group had an older age but without gender differences. Compared to the survival group, the death group exhibited lower DBP, SpO2, and PLT levels, but higher creatinine and PTT levels (P < 0.05). Besides, there was an obvious increase in SAPS II in the death group. The death group was more likely to have cerebrovascular disease, renal disease, diabetes, and coronary heart disease (P < 0.05). Other factors were not differentially distributed in the two groups with no statistical significance (P > 0.05). No significant differences in sedative use were observed except for Dexmedetomidine, Propofol + Midazolam, and Midazolam + Dexmedetomidine. There were 52.323% Dexmedetomidine users in the survival group, while only 28.814% of individuals in the death group used Dexmedetomidine (P < 0.05) (Table 1). Besides, the two groups had no significant difference in mechanical ventilation (Table 1).
The selection of key sedative drugs
Due to the limited number of patients receiving combined sedative drugs, the patients who were only treated with Dexmedetomidine, Propofol, and Midazolam were compared for further analysis. As shown in Fig. 2A, Dexmedetomidine had the highest AUC value (0.617), followed by Propofol (AUC = 0.534) and Midazolam (AUC = 0.532). Moreover, the Delong test results exhibited that the AUC of Dexmedetomidine in predicting in-hospital death of SAH was significantly better than Propofol and Midazolam. The P values from the Delong test are shown in Table 2. Similarly, the DCA curve showed that Dexmedetomidine had the best net benefits (Fig. 2B).

The assessment of the clinical value of three sedative drugs. (A) The ROC curve of three sedative drugs in predicting in-hospital death of SAH. (B) The DCA curve of three sedative drugs in predicting the death of SAH. Model1 indicated Propofol; Model2 indicated Midazolam; Model3 indicated Dexmedetomidine. SAH subarachnoid hemorrhage, ROC receiver operating characteristic curve, AUC area under the curve, DCA decision curve analysis.
Comparison of characteristics between the original cohort and the adjusted cohort
The superior role of Dexmedetomidine in predicting in-hospital death of SAH triggered us to deep into its clinical function. Before PSM, it was obvious that patients treated with Dexmedetomidine were significantly younger than those without Dexmedetomidine treatment, and were more likely to be men (P < 0.05). Besides, more patients were diagnosed with cerebrovascular disease and hyperlipemia in the non-Dexmedetomidine group (P < 0.05). In addition, the patients treated with Dexmedetomidine had significantly lower PTT and SAPS II scores than the non-Dexmedetomidine group (P < 0.05) (Table 3). In addition, the non-Dexmedetomidine group had a lower proportion of WFNS grade IV-IV cases (P < 0.05). Therefore, we enrolled age, gender, cerebrovascular disease, hyperlipemia, PTT, SAPS II scores, and WFNS grade for PSM analysis to balance the variables between the two groups.
After PSM analysis, the ASD of WFNS grade, hyperlipemia, SAPS II, PTT, gender, and age was < 0.2, indicating excellent balance. Although significant differences in age, cerebrovascular disease, WFNS grade, and SAPS II still existed in the two groups, their ASDs were < 0.25 with good balance (Fig. S1). Other factors had no obvious difference between the two groups (all P > 0.05) (Table 4).
Dexmedetomidine independently predicted primary and secondary outcomes
Then, we constructed three different models to assess the correlation between clinical characteristics and primary or secondary outcomes. The univariable analysis showed that Dexmedetomidine use was associated with a reduced risk of in-hospital mortality with an odds ratio of 0.381 (P < 0.001). After adjusting unbalanced factors in model 2, Dexmedetomidine use was an independent predictor for decreased in-hospital mortality (P < 0.05) (Table 5). However, the use of Dexmedetomidine increased the LOS of SAH patients in both crude and adjusted models (P < 0.001) (Table 5).
Subgroup analysis
According to previous studies, SAPS II is one of the important indexes to judge the severity of SAH17. Thus, further analysis was performed with patients stratified into four groups according to SAPS II quartiles. The results showed that the in-hospital mortality in the Dexmedetomidine users was lower compared to non-Dexmedetomidine users in the four SAPS II groups. Besides, among four SAPSII groups, the in-hospital mortality was highest in SAPSII quarter 1 whether patients were treated with Dexmedetomidine. As the SAPS II rose (except in quarter 1), the non-Dexmedetomidine group had increasing deaths (Fig. 3A-D). Whereas, the LOS in the Dexmedetomidine group was longer than the non-Dexmedetomidine group (all P < 0.05) (Fig. 4A-D). Consistent with the regression results, the use of Dexmedetomidine might reduce in-hospital deaths but prolong the LOS.

The in-hospital deaths of subarachnoid hemorrhage patients treated by Dexmedetomidine or not. (A) SAPS II quarter (1) (B) SAPS II quarter (2) (C) SAPS II quarter (3) (D) SAPS II quarter 4. DEX Dexmedetomidine.

The LOS of subarachnoid hemorrhage patients treated by Dexmedetomidine or not. (A) SAPS II quarter (1) (B) SAPS II quarter (2) (C) SAPS II quarter (3) (D) SAPS II quarter (4) DEX Dexmedetomidine, LOS length of in-hospital stays.
Analysis of the competitive risk models
When taking in-hospital mortality as a competing risk factor, the CIF analysis exhibited that the cumulative incidence of in-hospital mortality was more than discharge within 50 days of admission (Fig. 5A). After the treatment of Dexmedetomidine was included in competitive risk models, the results showed that Dexmedetomidine use was significantly related to hospital mortality (P < 0.001), but not LOS (P = 0.750) (Table 6). Moreover, patients with Dexmedetomidine use had a lower cumulative incidence of hospital mortality than those without Dexmedetomidine use (Fig. 5B). These results indicated that Dexmedetomidine provides a protective effect on in-hospital mortality.

The analysis of the competitive risk models based on outcomes and the use of Dexmedetomidine. (A) The cumulative incidence of in-hospital mortality and discharge for all subarachnoid hemorrhage (SAH) patients. (B) The cumulative incidence of in-hospital mortality and discharge for SAH patients treated with Dexmedetomidine or not. Yes: SAH patients were treated with Dexmedetomidine; No: SAH patients were treated without Dexmedetomidine.
Dexmedetomidine dose and duration were related to LOS
To further investigate the value of Dexmedetomidine use in SAH patients, we analyzed the association of sedative drug dose and duration with in-hospital mortality and LOS. Dexmedetomidine dose and duration were not related to in-hospital mortality but were associated with LOS (Table 7). Since Midazolam and Propofol doses have been described by different scopes from the MIMIC database, which are not definitive, we only investigated the association of their duration with outcomes. As shown in Table 7, Midazolam duration was not significantly linked to both outcomes. Propofol duration was not related to in-hospitality but had a connection with LOS.
Discussion
Based on the MIMIC-IV database, this retrospective study sought to analyze the impact of Propofol, Midazolam, and Dexmedetomidine on the prognosis in SAH patients. Among the various medications, patients treated solely with Dexmedetomidine exhibited a remarkable reduction in in-hospital mortality.
In comparison with Propofol and Midazolam, Dexmedetomidine demonstrated a more effective ability for SAH prognosis. The widespread use of Dexmedetomidine in clinical settings has yielded remarkable outcomes. Evidence from animal experiments supported the protective effects of Dexmedetomidine on the brain18. Additionally, certain clinical studies indicated its potential protective role in patients with intracranial aneurysms19. These findings underscore the potential importance of Dexmedetomidine in SAH treatment. Further investigations revealed that patients with ischemic brain damage may benefit from Dexmedetomidine, as it reduces the release of neuroendocrine hormones and inflammatory cytokines, maintains intracranial metabolism, and protects the brain20,21,22. Inada et al. observed dose-dependent inhibition of tumor necrosis factor (TNF)-α and interleukin (IL)-6 production by Dexmedetomidine, along with a reduction in recruited white blood cells23. However, it was noted that the white blood cell levels did not significantly differ between patients treated with Dexmedetomidine and those without, suggesting that the function of Dexmedetomidine may operate through alternative pathways.
In addition to its anti-inflammatory properties, Dexmedetomidine also exhibited a crucial role in reducing blood flow and oxygen requirements18,24. Blood flow rate is a significant factor exacerbating the course of subarachnoid hemorrhage25, and increased blood pressure leads to heightened blood flow rates26. Konar et al. found that blood pressure could effectively predict the prognosis of SAH27. Moreover, a clinical study demonstrated a correlation between low blood pressure and cardiovascular complications2. Gao et al. identified that the use of Dexmedetomidine could significantly reduce injury to other organs28. In the present study, it was observed that blood pressure was significantly reduced in patients with in-hospital mortality compared to those without, accompanied by an increased incidence of coronary heart disease. This suggests a close relationship between blood pressure, the severity of SAH, and the incidence of coronary heart disease. However, further analysis revealed no significant difference in blood pressure between SAH patients treated with or without Dexmedetomidine, although the PTT was significantly reduced in patients treated with Dexmedetomidine. This indicates that the effects of Dexmedetomidine may directly impact the blood flow of SAH patients without affecting blood pressure.
In previous decades, severity scores such as APACHE II, SAPS II, GCS, and WFNS scale have been used to predict the prognosis of SAH patients29. A meta-analysis demonstrated that the GCS had a superior prognostic value compared to SAPS II for SAH patients30. However, SAPS II exhibited a significant predictive value for SAH patients in other studies31. Herein, it was observed that SAPS II significantly decreased after Dexmedetomidine treatment and had a more stable predictive value than the GCS score. Regression analysis revealed that Dexmedetomidine use may reduce the risk of in-hospital mortality but increase the LOS for SAH patients, triggering us to further investigate their relationships by using competing risk analysis. By taking in-hospital mortality as a competing outcome, the use of Dexmedetomidine was protective of in-hospital mortality, but not related to LOS. Based on these findings, it is inferred that Dexmedetomidine may reduce deaths of SAH by regulating blood coagulation.
For strengths, PSM analysis was adopted to balance the variables between the two groups and reduce bias. Both unbalanced and balanced factors were adjusted in the multivariable regression analysis to reveal the predictive value of Dexmedetomidine for SAH prognosis. In addition, we used competing risk analysis to process survival data and calculate the cumulative incidence of multiple potential outcomes with in-hospital mortality as the competing risk event by Fin-Gray test and explored the association of Dexmedetomidine use with the two outcomes. For limitations, the retrospective study yielded a correlation rather than causality. Therefore, the results should be further validated in a prospective study with an independent cohort. Besides, in vitro and in vivo experiments are required to explore the mechanism of how Dexmedetomidine reduces in-hospital deaths.
In conclusion, the sole use of Dexmedetomidine exhibited the best efficiency in predicting in-hospital mortality. Moreover, SAH patients who received Dexmedetomidine treatment had a reduced risk of in-hospital death. Our study helps to guide sedative use and improve the prognosis of SAH patients.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Chaudhry, S. R., Shafique, S., Sajjad, S., Hanggi, D. & Muhammad, S. Janus Faced HMGB1 and post-aneurysmal subarachnoid hemorrhage (aSAH) inflammation. Int. J. Mol. Sci. 23. https://doi.org/10.3390/ijms231911216 (2022).
Wang, J. et al. Intraoperative blood pressure and cardiac complications after aneurysmal subarachnoid hemorrhage: a retrospective cohort study. Int. J. Surg. 110, 965–973. https://doi.org/10.1097/JS9.0000000000000928 (2024).
Young, B. J., Seigerman, M. H. & Hurst, R. W. Subarachnoid hemorrhage and aneurysms. Semin Ultrasound CT MR 17, 265–277. https://doi.org/10.1016/s0887-2171(96)90039-6 (1996).
Howard, B. M., Hu, R., Barrow, J. W. & Barrow, D. L. Comprehensive review of imaging of intracranial aneurysms and angiographically negative subarachnoid hemorrhage. Neurosurg. Focus 47, E20. https://doi.org/10.3171/2019.9.FOCUS19653 (2019).
Heit, J. J. et al. Cerebral angiography for evaluation of patients with CT angiogram-negative subarachnoid hemorrhage: an 11-Year experience. AJNR Am. J. Neuroradiol. 37, 297–304. https://doi.org/10.3174/ajnr.A4503 (2016).
Marshall, S. A., Kathuria, S., Nyquist, P. & Gandhi, D. Noninvasive imaging techniques in the diagnosis and management of aneurysmal subarachnoid hemorrhage. Neurosurg. Clin. N Am. 21, 305–323. https://doi.org/10.1016/j.nec.2009.10.005 (2010).
Murgova, S. & Balchev, G. Ophthalmic manifestation after SARS-CoV-2 vaccination: a case series. J. Ophthalmic Inflamm. Infect. 12, 20. https://doi.org/10.1186/s12348-022-00298-y (2022).
Anokwute, M. C. et al. Endovascular treatment of ruptured tiny (⩽3 mm) intracranial aneurysms in the setting of subarachnoid hemorrhage: a case series of 20 patients and literature review. J. Clin. Neurosci. 40, 52–56. https://doi.org/10.1016/j.jocn.2017.01.011 (2017).
Iwaasa, M. et al. Safety and feasibility of combined coiling and neuroendoscopy for better outcomes in the treatment of severe subarachnoid hemorrhage accompanied by massive intraventricular hemorrhage. J. Clin. Neurosci. 20, 1264–1268. https://doi.org/10.1016/j.jocn.2012.09.042 (2013).
Qureshi, A. I. & Frankel, M. R. Recognition and management of subarachnoid hemorrhage. Heart Dis. Stroke 3, 270–274 (1994).
Taylor, D. Iatrogenic drug dependence–a problem in intensive care? Case study and literature review. Intensive Crit. Care Nurs. 15, 95–100. https://doi.org/10.1016/s0964-3397(99)80005-6 (1999).
Walder, B. & Tramer, M. R. Analgesia and sedation in critically ill patients. Swiss Med. Wkly. 134, 333–346. https://doi.org/10.4414/smw.2004.10319 (2004).
Panahi, Y. et al. Analgesic and sedative agents used in the intensive care unit: a review. J. Cell. Biochem. 119, 8684–8693. https://doi.org/10.1002/jcb.27141 (2018).
McKeage, K. & Perry, C. M. Propofol: a review of its use in intensive care sedation of adults. CNS Drugs 17, 235–272. https://doi.org/10.2165/00023210-200317040-00003 (2003).
Yang, A. & Liu, B. May sevoflurane prevent the development of neurogenic pulmonary edema and improve the outcome? Or as a new sedation method for severe brain injury patients. Med. Hypotheses 137, 109538. https://doi.org/10.1016/j.mehy.2019.109538 (2020).
Paiella, S. et al. Modified Frailty Index to Assess Risk in Elderly patients undergoing distal pancreatectomy: a retrospective single-center study. World J. Surg. 46, 891–900. https://doi.org/10.1007/s00268-021-06436-2 (2022).
Schuiling, W. J., de Weerd, A. W., Dennesen, P. J., Algra, A. & Rinkel, G. J. The simplified acute physiology score to predict outcome in patients with subarachnoid hemorrhage. Neurosurgery 57, 230–236. https://doi.org/10.1227/01.neu.0000166536.42876.9c (2005).
Du, X., Yu, J. & Mi, W. The effect of dexmedetomidine on the perioperative hemodynamics and postoperative cognitive function of elderly patients with hypertension: study protocol for a randomized controlled trial. Med. (Baltim). 97, e12851. https://doi.org/10.1097/MD.0000000000012851 (2018).
Li, Y. C. et al. Cerebrospinal fluid metabolic profiling reveals divergent modulation of pentose phosphate pathway by midazolam, propofol and dexmedetomidine in patients with subarachnoid hemorrhage: a cohort study. BMC Anesthesiol 22, 34. https://doi.org/10.1186/s12871-022-01574-z (2022).
Zhu, J. et al. Lund exhaust on hemodynamic parameters and inflammatory mediators in patients undergoing cardiac valve replacement under cardiopulmonary bypass. Exp. Ther. Med. 16, 1747–1752. https://doi.org/10.3892/etm.2018.6354 (2018).
Lee, J. M. et al. Immunomodulatory effects of intraoperative dexmedetomidine on T helper 1, T helper 2, T helper 17 and regulatory T cells cytokine levels and their balance: a prospective, randomised, double-blind, dose-response clinical study. BMC Anesthesiol 18, 164. https://doi.org/10.1186/s12871-018-0625-2 (2018).
Hu, Y. et al. Feasibility study of use of desflurane combined with dexmedetomidine in inhibiting postoperative neurocognitive disorders in elderly patients under general anesthesia: a perspective study. Ibrain 10, 186–196. https://doi.org/10.1002/ibra.12073 (2024).
Inada, T. et al. Mitigation of inflammation using the intravenous anesthetic dexmedetomidine in the mouse air pouch model. Immunopharmacol. Immunotoxicol 39, 225–232. https://doi.org/10.1080/08923973.2017.1327964 (2017).
Lin, J. et al. The Sedative effects of Inhaled Nebulized Dexmedetomidine on children: a systematic review and Meta-analysis. Front. Pediatr. 10, 865107. https://doi.org/10.3389/fped.2022.865107 (2022).
Tone, O., Tomita, H., Tamaki, M., Hara, M. & Inaji, M. Correlation between cardiac output and cerebral blood flow following subarachnoid hemorrhage. Keio J. Med. 49 (Suppl 1), A151–153 (2000).
Minhas, J. S., Moullaali, T. J., Rinkel, G. J. E. & Anderson, C. S. Blood pressure management after Intracerebral and Subarachnoid Hemorrhage: the knowns and known unknowns. Stroke 53, 1065–1073. https://doi.org/10.1161/STROKEAHA.121.036139 (2022).
Konar, S. et al. Blood pressure variability and prognosis in aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis. J. Neurosurg. Sci. 67, 10–17. https://doi.org/10.23736/S0390-5616.21.05477-1 (2023).
Gao, L., Xiao, C., Cheng, T., Wang, Z. & Xia, W. Cellular Imaging Analysis Algorithm-based Assessment and Prediction of Disease in patients with Acute Lung Injury. Contrast Media Mol. Imaging 2022 (3193671). https://doi.org/10.1155/2022/3193671 (2022).
Basile-Filho, A. et al. The use of SAPS 3, SOFA, and Glasgow Coma Scale to predict mortality in patients with subarachnoid hemorrhage: a retrospective cohort study. Med. (Baltim). 97, e12769. https://doi.org/10.1097/MD.0000000000012769 (2018).
Ting, H. W., Chen, M. S., Hsieh, Y. C. & Chan, C. L. Good mortality prediction by Glasgow Coma Scale for neurosurgical patients. J. Chin. Med. Assoc. 73, 139–143. https://doi.org/10.1016/S1726-4901(10)70028-9 (2010).
Malinova, V. et al. The value of comorbidities and illness severity scores as prognostic tools for early outcome estimation in patients with aneurysmal subarachnoid hemorrhage. Neurosurg. Rev. 45, 3829–3838. https://doi.org/10.1007/s10143-022-01890-5 (2022).
Author information
Authors and Affiliations
Contributions
ZJW: conceptualization, investigation, supervision, project administration, data curation, original draft preparation and writing review and editing. THL: methodology, formal analysis, original draft preparation, writing review and editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The Ethics Committee of Longyan First Hospital Affiliated to Fujian Medical University deemed that this research is based on open-source data, so the need for ethics approval was waived.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, Zj., Lin, Th. A competing risk model analysis of dexmedetomidine of in-hospital mortality in subarachnoid hemorrhage patients. Sci Rep 14, 29590 (2024). https://doi.org/10.1038/s41598-024-81025-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-81025-6
Keywords
This article is cited by
-
Competing risk analysis of dexmedetomidine use and postoperative outcomes in non-traumatic subarachnoid hemorrhage patients
European Journal of Medical Research (2025)
-
Administration of dexmedetomidine in critically ill adult patients with hemorrhagic stroke: a retrospective cohort study of the MIMIC-IV database
Anesthesiology and Perioperative Science (2025)
