
Abstract
Humeroradial joint fixation (HJF) has been employed during elbow surgery to maintain stability. Kirschner wire (K-wire) fixation is the most commonly used method in children; however, there are valid concerns regarding complications such as breakage. In this study, we retrospectively analyzed the safety of humeroradial fixation using K-wires in children. In total, 249 patients diagnosed with Monteggia fractures underwent HJF at our institute from January 2013 to November 2021. All relevant clinical data were collected after applying the inclusion and exclusion criteria. Skin irritation, incision infection, elbow instability, and ulnar healing were followed up. The elbow function was evaluated using Mackay standards. There were 81 females and 168 males (average age, 6.6 ± 2.8 years). Of these patients, 67 did not have ulna fixation, whereas 127 were fixed with K-wires after osteotomy of the proximal ulna or correction of the deformity. The K-wire sizes used for HJF were 1.6, 1.8, and 2 mm in 6, 125, and 118 patients, respectively. The duration of K-wire fixation of the humeroradial joint was 6.6 ± 2.5 weeks on average. Two patients suffered from K-wire breakage and underwent reoperation. There were three patients with K-wire end irritation. According to Mackay standards, the elbow function score was excellent, good, and poor in 188, 41, and 20 patients, respectively, at 6 months postoperatively. No bone bridge was found at the capitellum and radial head fixation sites in any patient. HJF using K-wires combined with a cast is a safe method with a low incidence of complications in children and should be considered a reliable option when humeroradial joint fixation is required.
Level of evidence
IV.
Similar content being viewed by others


Introduction
Humeroradial joint fixation (HJF) has been performed in children1 and is used to stabilize the elbow2,3. Several situations require HJF2: patients with acute high-energy elbow injuries, ligaments, or bones that are unstable or still fragile after surgery; patients with complex joint dislocation in which the joint is still unstable after surgical repair; and finally, patients with severe elbow trauma that requires complex vascular, nerve, and bone reconstruction surgery in which it is necessary to maintain a relatively stable elbow environment. Several fixation techniques can be used, including Kirschner wires (K-wires) and an external fixation system4 (Fig. 1). Among them, K-wires are the most commonly used; however, some surgeons are concerned about the associated complications. To the best of our knowledge, there has been no study on the safety of K-wires in HJF. Monteggia fracture involves a fracture of the proximal one-third of the ulna combined with dislocation of the radial head and is more common in young adults and children5. If not diagnosed early, these lesions can progressively lead to forearm deformities and dysfunction, eventually resulting in neglected Monteggia fractures5. The current consensus on the treatment of recent or neglected Monteggia fractures with an unstable humeroradial joint does not mandate the use of K-wire fixation4,6,7. However, for patients with unstable humeroradial joints after reduction, our surgeons preferred to perform HJF using K-wires7. In this study, we retrospectively analyzed patients undergoing HJF using K-wires at our hospital and identified any complications associated with this method.

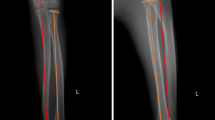
Different fixation materials for the treatment of Monteggia fractures. All humeroradial joints were fixed using a Kirschner wire (K-wire, red arrow). (a) Ulnar fixation using a steel plate (green arrow). (b) Ulnar fixation using a K-wire. (c) Ulnar fixation using an external fixation system.
Patients and methods
Patients
A retrospective analysis was performed on 249 children with neglected Monteggia fractures who underwent HJF in our hospital from January 2013 to December 2021 (Table 1). The inclusion criteria were (a) the presence of Monteggia fracture, (b) patients aged 0–18 years who were hospitalized for surgical treatment and for whom the surgical method included using K-wires to fix the humeroradial joint, and (c) patients with intact clinical data. The exclusion criteria were (a) recent Monteggia fractures with successful non-surgical treatment, (b) Monteggia fractures in children without K-wire fixation, and (c) incomplete follow-up data. This study was approved by Ethics Committee of Children’s hospital of Chongqing Medical University under the field approval number CHCMU-2024-128. The guardians of all patients provided written informed consent to publish the data. All methods were performed in accordance with the Declaration of Helsinki.
Surgical methods
After anesthesia, the patients were placed in a supine position, and surgery was performed according to the neglected Monteggia fracture classification. The purpose was to obtain a stable humeroradial joint. Various management methods were used based on the degree of ulna deformity and dislocation and stability of the humeroradial joint. Ulna reduction or osteotomy and/or reconstruction of annular ligaments was performed depending on the elbow stability of the humeroradial joint8. During the operation and after reducing the humeroradial joint, the elbow was bent at 90°. A K-wire was inserted from the posterior of the elbow, and the humeroradial joint was fixed through the center of the humeral to the radial head to stabilize the joint. Finally, the K-wire was bent and cut short, and the tail was left outside the skin. After the operation, cast fixation was routinely applied.
Postoperative management and follow-up
All patients were followed up at 2, 4, 6, and 8 weeks postoperatively, and radiographs were performed. Skin incision infection, K-wire tract infection, ulna healing, and stability of the humeroradial joint were evaluated. After K-wire removal, elbow joint exercises were initiated, and the function was evaluated 6 months postoperatively. Radiographic examination was performed 6 months and 1 year postoperatively.
According to Mackay’s functional evaluation criteria9, elbow function was classified into three grades: excellent (no elbow pain, elbow flexion and extension, forearm pronation and supination disorders < 20°, and elbow muscle and grip strength were normal), good (mild elbow and wrist pain, elbow extension and flexion disorders, forearm pronation and supination disorders < 30°, and weakened elbow muscle and grip strength), and poor (severe elbow and wrist pain, elbow extension and flexion, forearm pronation and supination disorders > 30°, and significantly decreased elbow muscle and grip strength).
Statistical analysis
The SPSS 20.0 statistical software (IBM, USA) was used for data analysis. A chi-square test was performed for normally distributed data. Count data were analyzed using chi-square or Fisher’s exact tests. P < 0.05 was considered statistically significant.
Results
In total, 249 patients were included in the study (81 females and 168 males, aged 6.6 ± 2.8 years). All patients were grouped according to the Bado classification of Monteggia fractures10,11: 147 patients had type I, 11 patients had type II, 90 patients had type III, and 1 patient had type IV Monteggia fracture. A total of 249 patients with Monteggia fractures underwent HJF in our hospital. The lateral approach was performed in all selected patients. The annular ligaments were explored intraoperatively, and the humeroradial joint was confirmed via K-wires under direct vision. Among them, 67 patients did not have ulna fixation, whereas 127 were fixed with K-wires after osteotomy of the proximal ulna or correction of the deformity (33 patients with one K-wire, 77 patients with two K-wires, 17 patients with three K-wires). The Orthofix external fixator system (Via delle Nazioni, Verona, Italy) was used in 50 patients, and reconstruction plates were used in five patients. The K-wire sizes used for HJF were 1.6, 1.8, and 2 mm in 6, 125, and 118 patients, respectively (Table 2). The average length of the K-wire from the tip to the humeral cortex was 53.2 ± 24.4 mm. After the operation, all patients were fixed with long-arm casting. Among them, 172 patients were fixed with a posterior elbow cast, 74 with an anterior and posterior elbow cast, and 3 with a short-arm cast. The duration of K-wire fixation of the humeroradial joint was 6.6 ± 2.5 weeks. There were ten children with symptoms of radial nerve injury before the operation, and all children recovered within 3 months postoperatively. Two patients suffered from K-wire breakage and underwent reoperation (Figs. 2 and 3; Table 2). Re-dislocation of the humeroradial joint occurred in both patients. Three patients experienced skin irritation around the K-wire end without purulent secretion, and all recovered after K-wire removal. According to Mackay standards9, the elbow function score was excellent, good, and poor in 188, 41, and 20 patients, respectively, at 12 months postoperatively. Notably, all 20 patients with poor function had neglected fractures. No bone bridge was found at the capitellum and radial head fixation sites in any patient (Table 2).

An eight-year-old boy with an old right elbow Monteggia fracture. (a) Radiograph of the old Monteggia fracture before surgery. (b) Humeroradial joint fixation using a Kirschner wire (K-wire; green arrow) combined with a posterior and anterior plaster cast postoperatively. (c) Break in the K-wire (green arrow) 35 days postoperatively. (d) K-wire was kept in the radius.

Nine-year-old boy with a right Monteggia fracture. (a) The fracture was reduced, and the supracondylar humerus fracture was fixed by a Kirschner wire (K-wire) applied to the humeroradial joint (green arrow), (b) Broken K-wire at 22 days postoperatively. (c) Partial removal of the broken K-wire (green arrow). (d) Partial K-wire in the proximal radius. (e) The K-wire was removed by opening the radial window.
Discussion
In our study, we retrospectively analyzed 249 patients who underwent HJF and proved that K-wire fixation is a safe method when combined with cast fixation. In clinical practice, in special cases such as dislocation of the elbow or complex fractures, instability of the elbow may still exist despite a reduction in fracture and ligament repair12,13. Traditional external fixation has been used to meet these needs, and orthopedic surgeons may try to use fixation across the joint to maintain joint reduction14. Presently, static and dynamic hinged external fixators can be used to treat unstable elbow fractures and dislocations14,15. However, many surgeons have observed several postoperative complications of external fixation, including inconsistent joint reduction, nerve injury, and pin-tract infection and fracture1,2,3,16,17,18,19,−20. In this study, we chose K-wires combined with casting as the fixation materials (Table 2).
A study by Rao et al.20 found that using static elbow external fixation to treat complex elbow fractures, dislocations, and chronic instability resulted in most patients eventually achieving a stable elbow with effective joint mobility. In their study, external fixation was retained for an average of 37 (from 19 to 47) days, but additional surgery to improve elbow stiffness was performed in 25% of patients after removal of the fixator. In our study, the duration of HJF was 6.6 ± 2.5 weeks, consistent with that of the study by Rao et al.19, but no patients underwent reoperation due to ankylosis. This may also be related to the fact that all children in this study had Monteggia fractures, the brachioulnar joint was unaffected, and the effect on postoperative joint function was limited.
Some studies propose that static fixation causes potential joint stiffness and other conditions16. However, a study by Al Qahtani et al.16 found no significant difference between static and dynamic external fixation in the treatment of unstable fracture/dislocation of the elbow in terms of postoperative joint range of motion and complication and reoperation rates, with both groups having similar outcomes.
Ring et al.1 found that although using hinged external fixators and crossed K-wires to fix the elbow joint was feasible and achieved similar postoperative elbow function scores, hinged external fixators were associated with more postoperative adverse events. Among the 19 patients treated with external fixators, three had pin-tract infections, two had nerve problems, one had a needle fracture, one had an ulnar pin-tract fracture, and one had a surgical site infection. Among the ten children who received crossed K-wire fixation in the study by Ring et al.1, only one had pin-tract inflammation, which resolved after removal. In our study, K-wire reactions occurred in three patients (1.2%), and needle breakage occurred in two patients (0.8%). The incidence of postoperative complications in our study was low, aligning with the findings of Ring et al.1. Additionally, several studies on hinged external fixators have found that the learning curve for this technique is relatively long. Many surgeons have insufficient understanding of the elbow joint axis of rotation, often leading to difficulty or even failure in its placement. Furthermore, although the device can stabilize the elbow joint, it is at the cost of normal motion trajectory21,22,23. Therefore, this technique is not suitable for junior surgeons without systematic training.
Some scholars suggest using K-wires larger than 2 mm to fix the humeroradial joint and reduce complications24. However, in a study by Cao et al.25, a 1.6-mm K-wire was used in 11 patients for humeroradial joint fixation, and the K-wire was removed after 6 weeks of cast fixation without any occurrences of K-wire breakage. In our study of 249 patients, two cases of K-wire breakage were observed: one with a 1.8-mm K-wire and the other with a 2.0-mm K-wire. Notably, no breakage occurred among the six patients treated with 1.6-mm K-wires. There was no significant difference in the incidence of K-wire breakage across groups (P = 0.975). K-wire breakage occurred in the two patients after 47 and 31 days, respectively. The former had been immobilized with a posterior elbow plaster cast and the latter with an anterior and posterior plaster cast. The incidence of K-wire breakage did not significantly differ among cast fixation methods (P = 0.818). However, we believe that proper cast support is essential for postoperative fixation.
K-wires are the most common fixation material for pediatric fractures. They have a smooth tip, do not cause epiphyseal injury in children, and are inexpensive. Combined with the advantages of their ease of use, few postoperative complications, and no need for reoperation to remove the internal osteosynthetic fixation, we conclude that short-term use of K-wire fixation is a safe, effective, and simple method for treating humeroradial joint fractures.
This study had some limitations. It was a single-center retrospective study with limited statistical power. Further prospective, multicenter studies may be needed to strengthen the findings. Our primary aim was to evaluate the safety of using K-wires for fixation of the humeroradial joint, demonstrating that this method is safe for unstable HFJ in Monteggia fractures. To achieve this, we specifically analyzed patients who underwent K-wire fixation of the humeroradial joint to assess the occurrence of complications afterward and provide safety insights for those who may require such fixation. Moreover, HJF was performed only on Monteggia fractures, and there were no children with severe elbow trauma. Lastly, K-wires were not compared with other fixation materials, such as external fixators.
Conclusions
Short-term use of a single K-wire combined with a cast in HJF is a safe method for treating elbow injuries in children.
Data availability
The datasets generated and analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
References
Ring, D., Bruinsma, W. E. & Jupiter, J. B. Complications of hinged external fixation compared with cross-pinning of the elbow for acute and subacute instability. Clin. Orthop. Relat. Res. 472 (7), 2044–2048 (2014).
Potini, V. C., Ogunro, S., Henry, P. D., Ahmed, I. & Tan, V. Complications associated with hinged external fixation for chronic elbow dislocations. J. Hand Surg. Am. 40 (4), 730–737 (2015).
Hopf, J. C., Berger, V., Krieglstein, C. F., Müller, L. P. & Koslowsky, T. C. Treatment of unstable elbow dislocations with hinged elbow fixation-subjective and objective results. J. Shoulder Elb. Surg. 24 (2), 250–257 (2015).
Ma, C. H., Hsueh, Y. H., Wu, C. H., Yen, C. Y. & Tu, Y. K. Does an internal joint stabilizer and standardized protocol prevent recurrent instability in Complex Persistent Elbow instability. Clin. Orthop. Relat. Res. 480 (7), 1354–1370 (2022).
Zhang, R., Wang, X., Xu, J., Kang, Q. & Hamdy, R. C. Neglected Monteggia fracture: a review. EFORT Open. Rev. 7 (4), 287–294 (2022).
Weber, M. M., Rosteius, T., Schildhauer, T. A., Königshausen, M. & Rausch, V. Monteggia fractures and monteggia-like-lesions: a systematic review. Arch. Orthop. Trauma. Surg. 143 (7), 4085–4093 (2023).
Tan, S. et al. Surgical Management of missed Pediatric Monteggia fractures: a systematic review and Meta-analysis. J. Orthop. Trauma. 36 (2), 65–73 (2022).
Gryson, T., Van Tongel, A. & Plasschaert, F. The management of chronic paediatric Monteggia fracture-dislocation. J. Orthop. 24, 65–76 (2021).
Mackay, I., Fitzgerald, B. & Miller, J. H. Silastic replacement of the head of the radius in trauma. J. Bone Joint Surg. Br. 61-B (4), 494–497 (1979).
Josten, C. & Freitag, S. Monteggia and Monteggia-like-lesions: classification, indication, and techniques in Operative Treatment. Eur. J. Trauma. Emerg. Surg. 35 (3), 296–304 (2009).
Bado, J. L. The Monteggia lesion. Clin. Orthop. Relat. Res. 50, 71–86 (1967).
Masquijo, J. J., Sanchez Ortiz, M., Ponzone, A., Fernández Korosec, L. & Arkader, A. Management of lateral Condyle Humeral Fracture Associated with Elbow dislocation in children. A Retrospective International Multicenter Cohort Study. J. Pediatr. Orthop. 44 (2), 82–88 (2024).
Pincin, A. et al. Elbow dislocation with and without an associated fracture in children: a prospective study of functional outcomes following 3 weeks of immobilization. Orthop. Traumatol. Surg. Res. : 103538. (2022).
Loose, O. et al. Radial head distalisation with an external ring fixator as a therapy option in children with chronic posttraumatic radiocapitellar dislocations. Eur. J. Trauma. Emerg. Surg. 49 (4), 1803–1810 (2023).
Lu, S., Wang, Y., Rui, B. & Ding, J. Comparison of different treatment approaches for coronoid process fracture in terrible triad injury: a multicenter, randomized controlled study. Int. Orthop. 47 (8), 2103–2111 (2023).
AlQahtani, S. et al. Static and dynamic external fixation are equally effective for unstable elbow fracture-dislocations. J. Orthop. Trauma. 35 (3), e82–e88 (2021).
Van Tunen, B., Van Lieshout, E., Mader, K. & Den Hartog, D. Complications and range of motion of patients with an elbow dislocation treated with a hinged external fixator: a retrospective cohort study. Eur. J. Trauma. Emerg. Surg. 48 (6), 4889–4896 (2022).
Cheung, E. V., O’Driscoll, S. W. & Morrey, B. F. Complications of hinged external fixators of the elbow. J. Shoulder Elb. Surg. 17 (3), 447–453 (2008).
Iordens, G. I. et al. Good functional recovery of complex elbow dislocations treated with hinged external fixation: a multicenter prospective study. Clin. Orthop. Relat. Res. 473 (4), 1451–1461 (2015).
Rao, A. J. & Cohen, M. S. The use of static external fixation for chronic instability of the elbow. J. Shoulder Elb. Surg. 28 (8), e255–e264 (2019).
Brownhill, J. R., Furukawa, K., Faber, K. J., Johnson, J. A. & King, G. J. Surgeon accuracy in the selection of the flexion-extension axis of the elbow: an in vitro study. J. Shoulder Elb. Surg. 15 (4), 451–456 (2006).
Stavlas, P., Jensen, S. L. & Søjbjerg, J. O. Kinematics of the ligamentous unstable elbow joint after application of a hinged external fixation device: a cadaveric study. J. Shoulder Elb. Surg. 16 (4), 491–496 (2007).
Wiggers, J. K. et al. Surgical accuracy in identifying the elbow rotation axis on fluoroscopic images. J. Hand Surg. Am. 39 (6), 1141–1145 (2014).
Di Gennaro, G. L., Martinelli, A., Bettuzzi, C., Antonioli, D. & Rotini, R. Outcomes after surgical treatment of missed Monteggia fractures in children. Musculoskelet. Surg. 99 (Suppl 1), S75–82 (2015).
Cao, S. et al. Missed Monteggia fractures in children treated by open reduction of the radial head and corrective osteotomy of the ulna. Sci. Rep. 12 (1), 16819 (2022).
Acknowledgements
None.
Funding
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Author information
Authors and Affiliations
Contributions
YS conceived the study, participated in its design and drafted the manuscript. XC and KC helped in collecting the clinical data and help drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of interest
The authors declare that they have no conflict of interest.
ICMJE conflict of interest statement
None of the authors have any conflict of interest to declare.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, K., Chen, X. & Su, Y. The safety of humeroradial fixation using Kirschner wires in children. Sci Rep 14, 30317 (2024). https://doi.org/10.1038/s41598-024-81397-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-81397-9
