
Abstract
Accumulating evidence has shown an increased risk of suicide among people living with HIV/AIDS (PLWHA). However, few studies have explored the risk factors associated with completed suicide among PLWHA. This study aimed to identify the characteristics and causes of completed suicide among PLWHA to guide future targeted suicide prevention and intervention programs. A 1:1 matched case–control psychological autopsy study was conducted among PLWHA in Hunan Province. We recruited 63 PLWHA who died by suicide from January 1, 2013, to December 31, 2019, and 63 living controls matched for age, gender, and employment. Two informants for each participant were interviewed to collect data on participants’ sociodemographic characteristics, depressive symptoms, HIV-related stress, hopelessness, and social support. The median survival time from HIV diagnosis to completed suicide was 3.9 months (IQR: 0.57–14.13). Most completed suicides occurred within six months of HIV diagnosis (71.4%), with poisoning (34.9%) and hanging (22.2%) as the primary methods. After controlling for confounding factors, we identified four risk factors of completed suicide: not receiving antiretroviral treatment (OR = 6.805; 95% CI: 1.227 to 37.738), receiving low-income subsidy (OR = 16.272; 95% CI: 3.245 to 81.598), HIV-related stress (OR = 1.332; 95% CI: 1.089 to 1.629), and hopelessness (OR = 2.910; 95% CI: 1.378 to 6.144). PLWHA are at a high risk of suicide within the first six months of HIV diagnosis, indicating an urgent need for immediate suicide screening and timely intervention. Suicide risk is affected by multiple factors, including sociodemographic, clinical, and psychological factors, indicating the need for a multifactorial approach to suicide prevention, which may involve early initiation of ART treatment and provision of economic and psychosocial support.
Similar content being viewed by others

Introduction
With a growing population of people living with HIV/AIDS (PLWHA), HIV will continue to be a major threat to public health for years to come1. By the end of 2022, 39 million people were living with HIV/AIDS (PLWHA) worldwide, with around 1.3 million new infections reported in 20222. The United Nations Programme on Acquired Immune Deficiency Syndrome (UNAIDS) has estimated that approximately 6.5 million (5.3–7.8 million) people in the Asia-Pacific region were living with HIV in 2022, and 150 000 (110,000–220,000) of them died from AIDS-related illnesses. By the end of 2022, China had reported a total of 1.2 million PLWHA, 418,000 deaths, and 107,800 new cases3. The number of PLWHA continues to rise, posing significant challenges to the global goal of ending the HIV/AIDS epidemic.
In recent years, with the widespread and effective implementation of highly active antiretroviral therapy (HAART) has contributed to new patterns of mortality among PLWHA have changed. The number of AIDS-related deaths has steadily declined, while the proportion of deaths unrelated to AIDS, such as suicides, has increased4,5. PLWHA are at an increased risk of suicide, and their suicide mortality is much higher than the general population and people with other chronic illnesses such as cancer6,7,8,9. A meta-analysis reported that the global suicide mortality for PLWHA was 10.2‰10, 100 times higher than the general population (0.09‰)11. Another meta-analysis showed that the suicide rate of PLWHA ranged from 2.9 to 112 deaths per 100,000 individuals, accounting for 2.6–8.5% of the total deaths in this population12. A retrospective national cohort study conducted in China revealed that the suicide mortality among PLWHA was 142.8 per 100,000 person-years, approximately 20.9 times higher than the general population13.
Suicide can be conceptualized as a process or continuum ranging from suicide ideation, suicide plan, and attempted suicide to completed suicide14. Previous studies have identified various of risk factors for suicide (mainly focusing on suicide ideation, plan, and attempt), which can be generally classified into sociodemographic, clinical, and psychosocial factors. Demographic factors such as younger age, female gender, unemployment, lower education, being unmarried, and living alone have been demonstrated to be directly associated with an increased risk of suicide15,16. Clinical factors, including AIDS-related symptoms, antiretroviral (ART) treatment, mental illness, substance abuse, chronic diseases, and a family history of suicide, are reported to be significant risk factors for suicide12,15,16,17,18. In addition, multiple psychosocial factors have been identified to contribute to the risk of suicide among PLWHA, including HIV-related stress, HIV-related stigma and social discrimination, low social support, low quality of life, stressful or traumatic events (STLEs), and depression12,17,18,19,20.
Although suicide and associated risk factors of PLWHA have been extensively studied and widely reported in PLWHA, most previous studies focused only on the first three stages, from suicide ideation to suicide attempt, and little is known about completed suicide and associated risk factors. The few existing studies on completed suicide are mainly cross-sectional or qualitative in design21,22. For instance, a study21 on suicide rates among newly diagnosed PLWHA in China revealed that suicide risk was the highest within the first week after diagnosis, and risk factors of committing suicide included younger age, Han nationality, being single, higher education, and homosexual infection route. Another qualitative study22 by our research group has summarized three levels of risk factors influencing completed suicide among PLWHA: (1) individual levels, such as personality traits and physical and mental health; (2) interpersonal levels, such as family dynamics, social support, and life events; (3) environment levels, such as the community’s tolerance towards HIV/AIDS. Although these cross-sectional and qualitative studies have elucidated some valuable information on suicide, a more robust and efficient approach to gain an in-depth understanding of the mechanism and determinants of completed suicide among PLWHA is needed.
To address the research gaps, we conducted a psychological autopsy study with a 1:1 case–control design to identify the characteristics and causes of completed suicide among PLWHA in Hunan Province. Based on the literature, we included three types of potential influencing factors: sociodemographic (e.g., age, gender, education, and employment), clinical (e.g., ART treatment and symptoms related to AIDS), and psychosocial factors (e.g., depressive symptoms, HIV-related stress, hopelessness, and social support). To the best of our knowledge, this was the first psychological autopsy study focusing on completed suicides among PLWHA. Our findings would provide important insight into the characteristics and risk factors for suicide among PLWHA and guide the future development of suicide prevention and intervention plans among high-risk populations.
Methods
Study design
Psychological autopsy is one of the most efficient ways to explore the psychological and contextual determinants preceding suicide retrospectively and systematically23,24. Case–control psychological autopsy studies have become a standard method widely used in suicide research to quantitatively explore the ongoing or recent risk factors for completed suicide22. The method involves collecting all available information on the deceased via structured interviews of family members, friends, and neighbors, extracting interview information, and reconstructing the deceased’s thoughts, feelings, and other psychological states before death to determine the manner of death and assess factors related to death25. Psychological autopsy has been widely used to explore risk factors of completed suicide among other populations in China, with well-established reliability and validity26,27,28,29. A 1:1 matched case–control study was conducted to compare two groups of PLWHA: those who died by suicide (the case group) and living controls (the control group).
Study setting
The study was conducted in Hunan Province, China, which includes 14 prefectures and cities. In 2021, the HIV incidence rate in Hunan Province was 4.54 per 100,000, and the mortality rate was 1.60 per 100,000. These rates are most similar to the national epidemiological situation among all provinces and municipalities in China30. This region was selected due to the availability of comprehensive HIV/AIDS data from the Hunan Province Integrated AIDS Prevention and Control Information System, which enabled the identification of completed suicide cases among PLWHA. The study setting is considered suitable because it provides a well-established dataset for identifying both cases and controls, with support from local health authorities.
Study population
The study focused on PLWHA, which refers to individuals who have been diagnosed with HIV infection or AIDS. Inclusion criteria for suicide cases were (a) age ≥ 18, (b) the death occurring within 14 prefectures and cities of Hunan Province, (c) the cause of death being verified as ‘suicide’ by death records, informants, staff of the Center for Disease Control and Prevention (CDC), or village doctors, and (d) the death occurring within the study period between January 1, 2013, and December 31, 2019, within the study period. Exclusion criteria were: (a) cases with misreported or missing data during verification processes; (b) cases in which the informant indicated that the deceased did not die by suicide and provided a precise cause of death; (c) cases in which the informant could not be contacted.
Sampling
We retrieved data on all suspected completed suicide cases among PLWHA from the Hunan Province Integrated AIDS Prevention and Control Information System during the study period. A total of 96 completed suicide cases were confirmed by local health authorities and district-level CDC, and on-site investigations, 96 cases of completed suicide were confirmed. During the investigation, 16 cases were lost to follow-up, and 17 cases refused participation, resulting in a final sample of 63 cases (effective response rate: 65.6%). Living controls were 1:1 matched with the suicide cases by age (± 3 years old), gender, and employment. When a suicide case was identified, investigators listed all living PLWHA from the same 14 prefectures in the information system who matched with the case by gender, birth year, and employment status. One control was then randomly selected from this list using a computer program.
Two informants for each target individual were selected for psychological autopsy. The first informant was usually a direct relative of the target individual, such as their spouse, child, or other family members, and the second informant was mainly their best friends or neighbors. For each suicide case, two informants were interviewed, while for the living control, two informants and the control himself/herself served as the sources of information. Among the 63 cases, 18 had two informants, while the other 45 had only one informant, leading to 81 informant interviews. Among the 63 controls, 57 completed the interviews by themselves, 7 had two informants, 20 had one informant, and the other 36 had no informant available, leading to 34 informant interviews.
Measures
Sample characteristics
An investigator-designed questionnaire was used to collect information on the following sample characteristics: (a) sociodemographic characteristics, such as gender, age, place of residence, marital status, education, and employment; (b) clinical characteristics, such as ART treatment and symptoms related to AIDS; and (c) suicidal-related characteristics, such as the time and method of suicide, history of attempted suicide, and the most likely reasons for suicide, as judged by informants.
Depressive symptoms
The 9-item Patient Health Questionnaire (PHQ-9) was used to assess depressive symptoms in study subjects over the past two weeks31. The total score ranges from 0 to 27, with a higher scores indicating more depressive symptoms. A cutoff of 10 was used to distinguish those with or without depressive symptoms32. The PHQ-9 showed good internal consistency in the current study, with a Cronbach’s α coefficient of 0.926.
HIV-related stress
HIV-related stress was assessed by the Chinese HIV/AIDS Stress Scale (CSS-HIV)33, which includes 17 items under three dimensions: emotional stress (7 items), social stress (10 items), and instrumental stress (6 items). The total score ranges from 0 to 68, with a higher scores indicating a higher levels of HIV-related stress. The CSS-HIV showed good internal consistency in the current study, with a Cronbach’s α coefficient of 0.934.
Hopelessness
The Paul-revised brief version of Beck’s Hopelessness Scale (BHS-4) was utilized to measure the sense of hopelessness among research subjects34. It consists of four items related to success, dark future, breaks, and faith. The total score ranges from 4 to 20, with a higher scores indicating a higher levels of hopelessness. The Cronbach α coefficient for the scale in this study was 0.804, indicating good internal consistency.
Social support
The 10-item Social Support Rating Scale (SSRS) was used to assess perceived social support from three domains: objective support (3 items), subjective support (4 items), and support utilization (3 items). The total score ranges from 11 to 66, with a higher scores indicating a higher levels of social support. The SSRS has been widely used in China and has demonstrated good reliability and validity35. The SSRS showed good internal consistency in the current study, with a Cronbach’s α coefficient of 0.778.
Ethics
All study procedures were approved by the Ethics Committee of Xiangya School of Public Health, Central South University (XYGW-2018-34, XYGW-2019-057). In accordance with the ethical principles outlined in the Declaration of Helsinki, all participants provided informed consent before participating in the study. All researchers and staff involved in the study signed confidentiality agreements, ensuring that they adhered to strict privacy and confidentiality protocols.
Research procedure
The county-level CDCs directly managed PLWHA and were chosen as the investigation site for this study. We confirmed the accuracy of suicide case information with local CDC staff before approaching informants for interviews. After obtaining written informed consent from the informants, we conducted face-to-face interviews or telephone interviews for individuals unable to meet in person or located remotely. Two trained interviewers interviewed each informant based on a pre-determined interview outline. After the interview, each interviewee received a gratitude fee of 6.87 dollars. A total of 114 face-to-face and 58 telephone interviews were conducted.
After the interviews, the information obtained from the first and second informants is combined, with priority given to the first informant. In instances of conflicting responses between informants, the information was combined by selecting those responses that were most likely to be associated with an increased suicide risk, based on the assumption that any informant could observe symptoms or behaviors related to the risk.
We transcribed the interview information into data and stored it in a secure, encrypted device in Microsoft Excel format. Only authorized personnel with appropriate clearance had access to the data. All sensitive personal information (e.g., names and contact details) was either anonymized or removed during data entry, ensuring that only non-identifiable data were stored for further analysis.
Statistical analysis
Data were analyzed using IBM SPSS version 26.0 (SPSS; Inc., Chicago, IL, USA). Descriptive analyses, χ2 tests, t-tests, and Mann–Whitney tests were used to describe and compare the sociodemographic, clinical, and psychosocial characteristics of the cases and controls. Significant variables were then entered into a conditional logistic regression model. The logistic regression model was used to investigate the influencing factors of suicide and to obtain the adjusted odds ratios (ORs) and their 95% confidence intervals (CIs) for each independent variable. A stepwise elimination method was used to identify a stable model. All the reported p-values were two-sided, with P-values less than 0.05 considered statistically significant.
Results
Characteristics of cases and controls
A total of 63 suicide cases and 63 living controls were assessed in this study. As shown in Table 1, the case group had a mean (SD) age of 50 (15) years, with most being male (84.12%). Compared to the living controls, more suicide cases were not receiving antiretroviral treatment, receiving low-income subsidies, and having symptoms related to AIDS (all P-values < 0.001). No statistically significant difference was found in the residence, marital status, time from diagnosis to death or the study time point, and education between the suicide cases and living controls (all P-values > 0.05). However, the suicide cases had significantly lower social support, higher HIV-related stress, more depressive symptoms, and higher levels of hopelessness (all P-values < 0.001).
Suicide characteristics of the case group
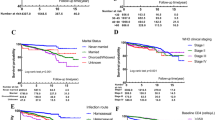
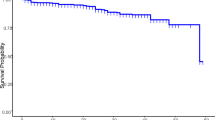
The median survival time from HIV diagnosis to death for cases was 3.9 months (interquartile ranges [IQR]: 0.57–14.13). Four cases (6.3%) died on the day of diagnosis, 12 (19.0%) died within one week of diagnosis, 20 (31.7%) died within one month of diagnosis, 40 (63.5%) died within six months of diagnosis, and 45 (71.4%) died within one year of diagnosis. The main methods of suicide were poisoning (34.9%) and hanging (22.2%), followed by jumping from height (7.9%) and drowning (7.9%). 66.7% of cases committed suicide at home, followed by the hospital (11.1%).
In this study, 41 suicide cases (65.1%) did not inform others of their suicide attempts. In contrast, 8 (12.7%) had informed others of their suicide attempts, and another 8 (12.7%) had contacted others before attempting suicide but did not explicitly mention their suicide attempts. Of the suicide cases, 42 (66.7%) committed suicide without anyone present, while 15 (23.8%) had someone present who did not notice the suicide. In addition, 9 cases (14.28%) had a history of previous suicide attempts, while 4 (6.3%) had made suicide preparations before their suicide, as shown in Table 2.
The causes of death by suicide were mainly physical illness (23.8%) and psychological stress (14.3%), followed by HIV infection (11.1%) and fear of discrimination (11.1%), as shown in Table 3.
Risk factors of completed suicide
A conditional logistic regression was used to determine the risk factors of suicide. Variables that were significant in the univariate analysis were included in this model for further analysis. The results revealed that not receiving antiretroviral treatment (OR = 6.805; 95% CI: 1.227 to 37.738), receiving low-income subsidy (OR = 16.272; 95% CI: 3.245 to 81.598), higher emotional stress (OR = 1.332; 95% CI: 1.089 to 1.629), and higher levels of hopelessness (OR = 2.910; 95% CI: 1.378 to 6.144) were risk factors for completed suicide. Depressive symptoms and social support were not significantly associated with completed suicide (Table 4).
Discussion
To the best of our knowledge, this is the first psychological autopsy study to explore the risk factors for completed suicide among PLWHA. Our results showed that 63.5% of the suicide cases died within the first six months after HIV diagnosis and 71.4% within the first year. This finding was consistent with national data showing that the suicide mortality among PLWHA was highest within the first year of HIV diagnosis17,21,36. It has been unanimously acknowledged that the first year of HIV diagnosis is a critical period for suicide prevention and intervention among PLWHA. Being diagnosed with HIV is a traumatic event that can cause significant emotional distress due to HIV stigma, physical symptoms, and the burden of lifelong medication, which may contribute to depression, hopelessness, and even suicide37,38. Our findings suggest that it is crucial to initiate immediate suicide screening among newly diagnosed PLWHA and provide timely intervention for those at high risk of suicide.
Consistent with previous findings, our results indicated that the main methods of suicide deaths were poisoning (34.9%) and hanging (22.2%); both were highly aggressive and lethal. In addition, 66.7% of PLWHA died at home alone, and 65.1% did not inform anyone of their suicide attempt. This finding was congruent with a similar study28 in Hong Kong, reporting that most of the suicides (119, 79.3%) died at home, and half of them did not express their suicidal plan.
Unlike previous studies showing that a large proportion of suicide cases had mental illness that may contribute to an increased risk of suicide29,39, our study only identified five suicide cases with diagnosed mental illnesses (8%). This low number should be interpreted as an underestimate of the true prevalence of mental illness among suicide cases. In China, due to the discrimination and stigmatization of mental illnesses and a lack of mental health literacy, many individuals with psychological problems are unaware of, unwilling to, or ashamed to seek help from mental health professionals before committing suicide40. Therefore, most of the suicide victims in China do not have a psychiatric diagnosis29. In our study, PLWHA with mental illnesses are faced with the double stigma of both mental illnesses and HIV infection and are thus less likely to seek treatment, leading to an underestimate of mental illness diagnosis.
According to our data, the main reason for completed suicide was physical illnesses. This finding aligns with Jia et al.‘s study showing that PLWHA frequently used healthcare services and had a higher suicide risk than uninfected individuals36. One explanation may be that PLWHA experience more physical symptoms requiring frequent hospital visits, which burdens their physiology, psychology, economy, and daily life. Furthermore, abundant evidence revealed that physical illness was associated with psychiatric illness41, especially depression41,42, which was a major risk factor for suicide28,43,44. In addition to the challenges mentioned above, most PLWHA in China do not disclose their infection status45,46. They may also be concerned about unexpected HIV disclosure due to physical illnesses, which can lead to discrimination, isolation, and bullying47,48, resulting in increased psychological stress and even suicide. These findings highlight the importance of healthcare professionals paying attention to the mental health of PLWHA and providing timely psychological support to reduce suicide risk.
Multivariate regression analysis has identified four risk factors of completed suicide: not receiving antiviral treatment, receiving low-income subsistence, higher HIV-related stress, and higher levels of hopelessness. Considering that 32% of suicides died within the first month after diagnosis without initiating ART treatment, the result may overestimate the risk of not receiving ART treatment. A cohort study in China also showed that not receiving ART treatment was an independent risk factor for completed suicide among PLWHA13. These findings suggest that efforts to promote early initiation of ART among PLWHA may contribute to better health outcomes and potentially reduce the risk of suicide, though further research is needed to confirm this relationship.
Our study found that PLWHA who receive low-income subsistence were 16 times more likely to die from suicide than those who did not, indicating poverty as a strong risk factor for completed suicide49. Although China has a free ART treatment policy covering certain medications, PLWHA may still need to bear the additional costs of physical examinations, transportation, and some self-paid medications. The economic burden on families further increases the risk of suicide. A psychological autopsy study conducted in rural Hunan indicated that there was a significant association between family economic conditions and suicidal behavior50. PLWHA may face the challenge of becoming impoverished or exacerbating existing poverty due to their illness, thereby increasing the risk of suicide. This suggests that more attention should be given to PLWHA with low income. In addition to promoting the national free HIV treatment policies, efforts should be made to mobilize material resources and increase financial support for low-income patients to alleviate their economic pressures.
Consistent with reports in other studies, our study illustrated that HIV-related stress could elevate the risk of completed suicide. PLWHA often experience various chronic and uncontrollable sources of stress, including social discrimination, social isolation, and unemployment, which can accumulate and make them feel that living with this stigmatized disease is intolerable51. Compared to other disease populations, PLWHA are more likely to suffer the stress mentioned above and commit suicide52. Additionally, HIV-related stress can exacerbate existing depressive and anxiety symptoms among PLWHA, contributing to an increased risk of suicide53. This finding suggests that more psychosocial support needs to be provided to PLWHA under stress.
In line with previous psychological autopsy studies49,54,55, we discovered that hopelessness was a significant risk factor for suicide. A meta-analysis of longitudinal studies56 found that hopelessness significantly predicted suicide ideation, suicide attempt, and completed suicide; depressive symptoms were significant predictors of ideation and attempt but not death. We also did not find a correlation between depressive symptoms and completed suicide. This may be because hopelessness has a greater predictive value than depression54. Another explanation may be that hopelessness is a core component of depressive symptoms and thus explains the association between depression and suicide57.
This study provides a deeper understanding of the specific psychological, social, and clinical factors contributing to suicide, which may be more complex and distinctive within this particular population. Investigating these factors helps identify high-risk individuals and offers valuable insights for the design of public health policies and mental health interventions tailored to PLWHA. However, several limitations should be considered when interpreting our results. First, psychological autopsy studies have methodological limitations as all information was collected based on informants instead of suicide cases themselves. In our study, most suicide cases did not inform their family or friends about their HIV infection, leading to relatively fewer informants of the cases, and they may have an insufficient understanding of the cases’ actual conditions. Second, this study did not collect vital indicators such as CD4 count and viral load, which provide essential information about the treatment history of the suicide cases. Third, the number of female participants in this study was limited, making it challenging to compare gender differences in suicidal risk factors. Fourth, the control group primarily consists of individuals living with HIV who have not yet developed AIDS. This may influence the comparison of outcomes between the cases and controls, and could limit the generalizability of some of our findings.
Conclusions
Within the first six months of being diagnosed, PLWHA are at high risk of suicide. It is necessary to conduct suicide screening among newly diagnosed PLWHA as early as possible to guide timely intervention to prevent suicide. Suicide risk was affected by multiple factors, including sociodemographic factors such as low income, clinical factors such as ART treatment, and psychological factors such as HIV-related stress and hopelessness. These findings suggest that effective suicide prevention and intervention need a multifactorial approach, which may involve early initiation of ART treatment and provision of economic and psychosocial support.
Data availability
The datasets generated during and/or analysed during the current study are not publicly available due to privacy or ethical restrictions but are available from the corresponding author on reasonable request.
References
Frank, T. et al. Global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2017, and forecasts to 2030, for 195 countries and territories: a systematic analysis for the global burden of diseases, injuries, and risk factors study 2017. Lancet HIV 6(12), e831–e59 (2019).
UNAIDS. AIDS BY THE NUMBERS [internet]. https://www.unaids.org/en (2023).
UNAIDS. The path that ends AIDS: UNAIDS Global AIDS Update 2023. Geneva: Joint United Nations Programme on HIV/AIDS. Licence: CC BY-NC-SA 3.0 IGO (2023).
Chen, L. et al. HIV cause-specific deaths, mortality, risk factors, and the combined influence of HAART and late diagnosis in Zhejiang, China, 2006–2013. Sci. Rep. 7(1), 42366 (2017).
Croxford, S. et al. Mortality and causes of death in people diagnosed with HIV in the era of highly active antiretroviral therapy compared with the general population: an analysis of a national observational cohort. Lancet Public Health 2(1), e35–46 (2017).
Heinrich, M. et al. Suicide risk and mortality among patients with cancer. Nat. Med. 28(4), 852–859 (2022).
Hofmann, L. et al. Suicide mortality risk among patients with lung cancer—a systematic review and meta-analysis. Int. J. Environ. Res. Public Health 20(5) (2023).
Brunckhorst, O. et al. Depression, anxiety, and suicidality in patients with prostate cancer: a systematic review and meta-analysis of observational studies. Prostate Cancer Prostatic Dis. 24(2), 281–289 (2021).
Guo, Z. et al. Incidence and risk factors of suicide among patients diagnosed with bladder cancer: a systematic review and meta-analysis. Urol. Oncol. 39(3), 171–179 (2021).
Pelton, M. et al. Rates and risk factors for suicidal ideation, suicide attempts and suicide deaths in persons with HIV: a systematic review and meta-analysis. Gen. Psychiatry 34(2), e100247 (2021).
WHO. Suicide Worldwide in 2019: Global Health Estimates (World Health Organization, 2021).
Smith, A. et al. A systematic review of risk factors for suicide among persons living with HIV (1996–2020). AIDS Behav. 26(8), 2559–2573 (2022).
Chen, F. et al. Trends in suicide mortality among people with HIV after diagnosis during 2012–18: a retrospective, national cohort study in China. Lancet HIV 9(2), e102–e11 (2022).
Sveticic, J. & De Leo, D. The hypothesis of a continuum in suicidality: a discussion on its validity and practical implications. Ment Illn. 4(2), e15 (2012).
Tsai, Y. T. et al. Suicidality among people living with HIV from 2010 to 2021: a systematic review and a meta-regression. Psychosom. Med. 84(8), 924–939 (2022).
Wei, L. & Jia, C. Research progress in the epidemiological status and the influencing factors of suicidal behaviors of PLWHA. Med. Philos. 36 (1), 42–44 (2015).
Croxford, S. et al. Mortality and causes of death in people diagnosed with HIV in the era of highly active antiretroviral therapy compared with the general population: an analysis of a national observational cohort. Lancet Public Health 2(1), e35–e46 (2017).
Whetten, K., Reif, S., Whetten, R. & Murphy-McMillan, L. K. Trauma, mental health, distrust, and stigma among HIV-positive persons: implications for effective care. Psychosom. Med. 70(5), 531–538 (2008).
O’Donnell, J. K. et al. Ongoing life stressors and suicidal ideation among HIV-infected adults with depression. J. Affect. Disord. 190, 322–328 (2016).
Ogundipe, O. A., Olagunju, A. T. & Adeyemi, J. D. Suicidal ideation among attendees of a west African HIV clinic. Arch. Suicide Res. 19(1), 103–116 (2015).
Zhang, H., Feng, Y., Li, Z., Xiu, X. & Wang, L. Spatial analysis and risk factors of suicide among people living with HIV/AIDS who committed suicide. Int. J. STD AIDS. 32(6), 490–500 (2021).
Bi, F., Yan, D. Q., Chen, X. & Luo, D. Theoretical framework of suicide risk factors among people living with HIV/AIDS: a qualitative study based on grounded theory. J. Shandong Univ. (Health Sci.). 60(1), 109–117 (2022).
Conner, K. R. et al. The next generation of psychological autopsy studies. Part I. Interview content. Suicide Life Threat Behav. 41(6), 594–613 (2011).
Arensman, E. et al. Psychosocial, psychiatric and work-related risk factors associated with suicide in Ireland: optimised methodological approach of a case–control psychological autopsy study. BMC Psychiatry 19(1), 275 (2019).
Conner, K. R. et al. Introducing the psychological autopsy methodology checklist. Suicide Life Threat Behav. 51(4), 673–683 (2021).
Zhang, J., Xiao, S. & Zhou, L. Mental disorders and suicide among young rural Chinese: a case–control psychological autopsy study. Am. J. Psychiatry 167(7), 773–781 (2010).
Niu, L. et al. Loneliness, hopelessness and suicide in later life: a case–control psychological autopsy study in rural China. Epidemiol. Psychiatr. Sci. 29, e119 (2020).
Chen, E. Y. et al. Suicide in Hong Kong: a case–control psychological autopsy study. Psychol. Med. 36(6), 815–825 (2006).
Phillips, M. R. et al. Risk factors for suicide in China: a national case–control psychological autopsy study. Lancet 360(9347), 1728–1736 (2002).
National Health Commission of the People’s Republic of China. China Health Statistics Yearbook 2022 (Peking Union Medical College, 2022).
Wang, W. et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen. Hosp. Psychiatry 36(5), 539–544 (2014).
Manea, L., Gilbody, S. & McMillan, D. A diagnostic meta-analysis of the Patient Health Questionnaire-9 (PHQ-9) algorithm scoring method as a screen for depression. Gen. Hosp. Psychiatry 37(1), 67–75 (2015).
Niu, L. et al. Cross-culture Validation of the HIV/AIDS stress scale: the development of a revised Chinese Version. PLoS One. 11(4), e0152990 (2016).
Yip, P. S. & Cheung, Y. B. Quick assessment of hopelessness: a cross-sectional study. Health Qual. Life Outcomes 4, 13 (2006).
Xiao, S. The theory basis and application of the social support rating scale. J. Clin. Psychiatry 4(2), 98–100 (1994).
Jia, C. X., Mehlum, L. & Qin, P. AIDS/HIV infection, comorbid psychiatric illness, and risk for subsequent suicide: a nationwide register linkage study. J. Clin. Psychiatry 73(10), 1315–1321 (2012).
Neigh, G. N., Rhodes, S. T., Valdez, A. & Jovanovic, T. PTSD co-morbid with HIV: separate but equal, or two parts of a whole? Neurobiol. Dis. 92(Pt B), 116–123 (2016).
Martinez, J., Lemos, D. & Hosek, the Adolescent Medicine S. Stressors and sources of support: the perceptions and experiences of newly diagnosed latino youth living with HIV. AIDS Patient Care STDs 26(5), 281–290 (2012).
Keiser, O. et al. Suicide in HIV-infected individuals and the general population in Switzerland, 1988–2008. Am. J. Psychiatry 167(2), 143–150 (2010).
Zhou, C. & Xu, Y. Time to break mental illness-related stigma and discrimination in China. Asian J. Psychiatr 66, 102881 (2021).
Scott, K. M. et al. Association of mental disorders with subsequent chronic physical conditions: World Mental health surveys from 17 countries. JAMA Psychiatry 73(2), 150–158 (2016).
Holahan, C. J. et al. Depression and vulnerability to incident physical illness across 10 years. J. Affect. Disord. 123(1–3), 222–229 (2010).
Jia, C. X., Wang, L. L., Xu, A. Q., Dai, A. Y. & Qin, P. Physical illness and suicide risk in rural residents of contemporary China: a psychological autopsy case–control study. Crisis 35(5), 330–337 (2014).
Yeh, S. T., Ng, Y. Y. & Wu, S. C. Association of psychiatric and physical illnesses with suicide in older adults in Taiwan. J. Affect. Disord. 264, 425–429 (2020).
Zhou, Y., Zhang, L., Li, X. & Kaljee, L. Do Chinese parents with HIV tell their children the truth? A qualitative preliminary study of parental HIV disclosure in China. Child Care Health Dev. 39(6), 816–824 (2013).
Fan, S. et al. Behavioral and serologic survey of men who have sex with men in Beijing, China: implication for HIV intervention. AIDS Patient Care STDS. 26(3), 148–155 (2012).
Cloete, A., Simbayi, L. C., Kalichman, S. C., Strebel, A. & Henda, N. Stigma and discrimination experiences of HIV-positive men who have sex with men in Cape Town, South Africa. AIDS Care 20(9), 1105–1110 (2008).
Li, L. et al. Disclosure of HIV status is a family matter: field notes from China. J. Fam Psychol. 21(2), 307–314 (2007).
Zhang, J., Conwell, Y., Zhou, L. & Jiang, C. Culture, risk factors and suicide in rural China: a psychological autopsy case control study. Acta Psychiatr. Scand. 110(6), 430–437 (2004).
Xu, H. L. Psychosocial Autopsy Study of Suicides by People Aged 15–5 in rural Hunan. Ph.D. Thesis (Central South University, 2009).
Carrico, A. W. Elevated suicide rate among HIV-positive persons despite benefits of antiretroviral therapy: implications for a stress and coping model of suicide. Am. J. Psychiatry 167(2), 117–119 (2010).
Genberg, B. L. et al. A comparison of HIV/AIDS-related stigma in four countries: negative attitudes and perceived acts of discrimination towards people living with HIV/AIDS. Soc. Sci. Med. 68(12), 2279–2287 (2009).
Chandra, P. S., Ravi, V., Desai, A. & Subbakrishna, D. K. Anxiety and depression among HIV-infected heterosexuals—a report from India. J. Psychosom. Res. 45(5), 401–409 (1998).
Beck, A. T., Steer, R. A., Kovacs, M. & Garrison, B. Hopelessness and eventual suicide: a 10-year prospective study of patients hospitalized with suicidal ideation. Am. J. Psychiatry 142(5), 559–563 (1985).
Wang, J. et al. The mediating role of depressive symptoms, hopelessness, and perceived burden on the association between pain intensity and late-life suicide in rural China: a case–control psychological autopsy study. Front. Psychiatry 12, 779178 (2021).
Ribeiro, J. D., Huang, X., Fox, K. R. & Franklin, J. C. Depression and hopelessness as risk factors for suicide ideation, attempts and death: meta-analysis of longitudinal studies. Br. J. Psychiatry 212(5), 279–286 (2018).
Waszczuk, M. A., Coulson, A. E., Gregory, A. M. & Eley, T. C. A longitudinal twin and sibling study of the hopelessness theory of depression in adolescence and young adulthood. Psychol. Med. 46(9), 1935–1949 (2016).
Acknowledgements
The authors would like to express gratitude to Fengying Bi, Yunxiang Huang, Rui Luo, Long Yang, Yumin Chen and Yanlin Liu for their preliminary investigative work, the staffs of Changsha Infectious Disease Hospital and the Changsha Center for Disease Control and Prevention for their kindest contributions and assistance to this study.
Funding
This study was supported by the Natural Science Foundation of Hunan Province(2019J40401), and National Natural Science Foundation of China (81202290). The funders played no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
D.L. conceived and designed the study. Xl.C. was involved in data collection and analysis. Z.Y. and XI.C wrote the first version of the manuscript with critical review and revision from D.L. X.C and Z.X. assisted in reviewing protocol and study coordination in the field and reviewed the manuscript. All authors contributed to the acquisition, analysis, or interpretation of data. All authors revised the report and approved the final version before submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, Z., Chen, X., Chen, X. et al. Completed suicide risk factors among people living with HIV in Hunan Province identified through a psychological autopsy case–control study. Sci Rep 14, 30988 (2024). https://doi.org/10.1038/s41598-024-82101-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-82101-7
