
Abstract
Particulate Matter (PM) pollution is a prime component of air pollution and poses a substantial risk to human health, including the eye. This work envisioned to show the impact of PM2·5 pollution on the Ophthalmic disease prevalence in India. This national-level observational-based cross-sectional retrospective study included the hospital-reported ophthalmic outpatients in 2019-20. The sector-wise high-resolution (0·1° × 0·1°) PM2·5 emission data along with the annual average PM2·5 concentration data for 2019 from NASA is adopted for the risk factor analysis. Nearly 32·6 million footfalls are recorded in various hospitals due to ophthalmic morbidity in 2019, out of which surprisingly ~ 80% of cases are registered in rural India. Half of the total ophthalmic disease burden comes from the top 100 districts out of the total 720 districts in India. The inferential analyses depicted a statistically significant positive correlation (r = 0·54, 95% CI 0·48 − 0·59, P < 0·001) between the PM2·5 emission and ophthalmic outpatients. The risk of eye disease in the exposed rural population is 4 times higher than the unexposed population 4·19 (4·19 − 4·2). The PM2·5 emission from household cooking activity shows a greater correlation (r2 = 0·28, 95% CI 0·22 − 0·35, P < 0·001) with the occurrence of ophthalmic cases in India followed by incense stick and mosquito coil burning (r2 = 0·28 (0·22 − 0·34)), and transportation (r2 = 0·24 (0·18 − 0·29)). The meteorological parameters like temperature and humidity show very little association and precipitation shows a negative correlation with the number of ophthalmic outpatients in India. This study suggests that surface emission data could be a potential tool to link prevailing diseases in India.
Similar content being viewed by others


Introduction
Clean air is a fundamental right for a healthy life, but unfortunately, almost the entire population breathes unhealthy air due to rapid changes in air quality across the globe. 9 out of 10 people reside in polluted regions, causing approximately ~ 7 million deaths a year worldwide1. It is evident from recent studies that considerable attention has been paid to understanding the long and short-term effects of exposure to ambient and indoor air pollution on human health2,3,4,5. Specifically, particulate matter (PM) pollution is exacerbating mortality and morbidity all over the world6,7,8,9,10,11. In India, the sources of PM include sectors like vehicular activity, resuspended road dust, coal combustion in power plants and industries, brick kilns, solid fuel in cooking activity, municipal solid waste burning, crop residue burning, etc12,13,14.
Air pollution is responsible for and aggravates various diseases linked to internal organs like cardiovascular, respiratory malfunction, maternal complexities and metabolic issues5,15,16,17. Similarly, it also immensely affects external organs like the eyes, which are directly and uninterruptedly exposed to contaminants for a prolonged time in polluted areas. As per the GBD 2019 dataset, after China, India placed second in ophthalmic cases prevalence in the world with ~ 18·4 cr cases annually18. The eye’s outermost portion, the ocular surface is comprised of the surface and glandular epithelia of the cornea, lacrimal gland, conjunctiva (mucous membrane), accessory lacrimal glands and meibomian gland, the eyelashes with the glands of Moll and Zeiss and the nasolacrimal duct. Any irregularity due to air pollutants in the operation of these leads to ophthalmic complexities. The most typical condition found in optical patients is conjunctivitis19,20. Long-term exposure to airborne pollutants promotes cellular damage, including hyperplasia of epidermis goblet cells on the surface of the eye21. The untreated chronic conjunctivitis could lead to severe dry eye syndrome, an increased propensity for conjunctival superinfection, and corneal complications. According to Fujishima et al. (2013), gasoline engine exhaust triggers inflammation in the conjunctiva by causing the epithelium’s cells to express more cytokines, chemicals, and growth factors22. A couple of studies conducted in developed countries like China and Canada confirmed the increased number of outpatients is positively associated with the concentration of PM23,24. The cornea is continuously exposed to particulates that stimulate oxidative stress, eventually damaging the cornea and causing vision impairment. A study reveals that fine particulate matter like PM2·5 (PM ≤ 2·5 μm) damages the DNA and deteriorates the functioning of corneal epithelium cells, acting as a genotoxic between 20 µg/mL to 200 µg/mL concentration25. Ambient particulate matter is responsible for various ophthalmic conditions like Cataracts, Glaucoma, Age-related macular degeneration, neoplasia etc26.
There are a couple of existing research-based evidence establishing the negative effects of air pollutants like PM on human eye health in India27,28,29,30,31,32. Most of the above studies investigated the regional scale/local air pollution level and its relationship with a particular kind of eye disease prevalence. Moreover, the satellite-retrieved or model-simulated PM concentrations considered in the above studies do not give the role of source types responsible for eye disease in that particular region. With the lack of sectoral pollutant load information which is vital for a country like India, where the cultural and lifestyle-related regional sources play an important role in disease prevalence. Moreover, the spatial pattern of sources keeps on changing with culture/lifestyle, fuel consumption pattern and energy needs. Recent studies suggest that windblown road dust emerged as the largest source of PM10 in the national capital megacity Delhi, unlike transport in Kolkata and Bengaluru14,33,34. In order to understand the role of each source type responsible for ophthalmic disease prevalence, high-resolution emission inventory could be a wonderful tool, which gives accountability of pollutants and their corresponding sources along with quantitative information across the country. The present study is a first-of-its-kind cross-sectional investigation to establish the association of source-wise PM2·5 emission load across the country and reported ophthalmic outpatients’ data in India. In order to strengthen the analysis, satellite-derived national-level PM concentration and effect of meteorological parameters are also analysed. We have performed a statistical analysis to calculate the correlation, and analytic epidemiological studies to determine the odds ratio and attributable proportions.
Methods
Study population and data collection
In this national-level observational-based cross-sectional retrospective study we have included the ophthalmic outpatients attending public or private hospitals in 2019-20. The regional (i.e. district-level) ophthalmic outpatient data are retrieved from the Ministry of Health and Family Welfare (MoHFW) (https://main.mohfw.gov.in/), released under the National Data Sharing and Accessibility Policy (NDSAP)35. Any identifiable parameter about the patient’s information has been excluded and was not considered for the analysis. A total of 32·59 million footfall has been registered in tertiary and secondary hospitals due to some ophthalmic morbidity between April 2019 and March 2020. The monthly ophthalmic outpatient data is utilized for spatiotemporal trend analysis with PM2·5 pollution load in the country. The age variability of ophthalmic disease onset has been retrieved from the census 2011 and extrapolated to 2019-20 (https://censusindia.gov.in/census.website/data/census-tables).
Exposure assessment
We have adopted an updated high-resolution (0·1° × 0·1°) IPCC-defined tiers II and III bottom-up approach based national EI of PM2·536. An EI is a broad catalogue of the amount of air pollutants emitted into the atmosphere, as a result of a distinctive anthropogenic or natural process in a specific geographical region during a specific time. The above EI includes activity data for 16 major and fugitive emission sources and country-specific emission factors are adopted to improve the estimation for 2019-20. Sectors like transportation, resuspended road dust, industry, power plant, residential and others comprising fugitive point sources like incense stick burning, cigarette burning, crematorium etc. are accounted for emission load estimation. The aggregated emission (E) from all individual sources is calculated as per the equation.
where, i, j, k = Fuel type, sector, technology, E = Total emission, F = Sector and fuel specific amount, Ef = Technology specific EFs, P = fractional part of fuel for a sector with particular technology, where \(\:\sum\:P=1\) for each fuel and sector.
The annual average PM2·5 concentration data for 2019 is collected from the Socioeconomic Data and Applications Center (SEDAC), NASA37. This dataset retrieved the Aerosol Optical Depth (AOD) by combining multiple satellite algorithms. It includes data from the NASA MODerate resolution Imaging Spectroradiometer Collection 6·1 (MODIS C6·1), MODIS Multi-Angle Implementation of Atmospheric Correction Collection 6 (MAIAC C6), Multi-angle Imaging Spectro Radiometer Version 23 (MISRv23), and the Sea-Viewing Wide Field-of-View Sensor (SeaWiFS) Deep Blue Version 4. The dataset is used to relate the total column of aerosol to the surface-level PM2·5 concentrations using the Goddard Earth Observing System - Chemistry model (GEOS-Chem).
Meteorological parameters
The effect of meteorological parameters like temperature, precipitation and humidity on modulating ophthalmic disease outpatients have been analyzed in this study. The temperature data has been retrieved from the MOD11A1 V6.1 dataset, which provides global land surface temperature data at 1 km resolution for 2019. The precipitation and humidity data have been accessed from the Reanalysis Data Services by the National Centre for Medium-Range Weather Forecasting (NCMRWF), Ministry Of Earth Sciences, Government Of India (https://rds.ncmrwf.gov.in/dashboard/download). The downloaded datasets are prepared according to the requirements of the GIS-based statistical software ArcGIS 10.6 (https://www.esri.com/en-us/home).
Statistical analysis
The published gridded PM2·5 emission data36 is scaled down to district-level emission using geographical information-based tool to establish the exposure-response relationship. Similarly, the satellite-derived annual average PM2·5 concentration data are adopted to differentiate between exposed and unexposed regions across the Indian subcontinent where the PM2·5 concentration greater than the National Ambient Air Quality Standards (NAAQS) i.e., > 40 µg/m3 is regarded as the exposed regions and people residing there are termed as the exposed population and rest are regarded as unexposed population. The PM2·5 exposure regions and their sources are identified from the high-resolution PM2·5 emission inventory where the relative contribution of 16 anthropogenic sectors is established and quantified. The schematic diagram of the methodology is presented in Fig. 1. The state-wise crude prevalence rate and direct age-standardized prevalence rate is estimated and presented in Fig. 2d, e.
In order to establish the ophthalmic disease prevalence, the descriptive statistics for the demographic data are expressed as mean ± Standard deviation, median and interquartile range. To strengthen the analysis, Pearson’s correlation coefficient is carried out to establish the association between PM2·5, ophthalmic outpatients, temperature, precipitation and humidity. Linear regression analysis is also carried out using the MedCalc software 22·0 (https://www.medcalc.org/). The two-sided p-value of < 0·001 is considered statistically significant and r2 values < 0·12 signified low, 0·13 to 0·25 signified medium and > 0·26 signified higher association37. Moreover, The results are compared with the Global Burden of Disease (GBD) data-2019.

Schematic representation of the data generation and analysis process.
Results
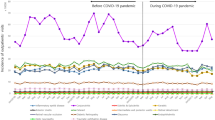
In this national-level cross-sectional study, ~ 32·59 million ophthalmic outpatient data are taken into account, where more than 80% have rural occurrence. Interestingly, due to the streamlined public healthcare infrastructure and medical consultation fee exemption, nearly 95% of the footfall for ophthalmic diagnosis in the country is well-recorded in public hospitals35. The district-wise spatial map of the number of ophthalmic outpatients per 10 km2 seeking medical advice is presented in Fig. 2a. The highest number of Ophthalmic outpatients was recorded in the districts of Central Delhi followed by Jaipur (Rajasthan), Bangalore (Karnataka), Prayagraj (Uttar Pradesh), Mumbai suburban (Maharashtra) and so on. Interestingly the top 100 districts out of 720 districts share nearly 50% of the total ophthalmic outpatients in the country. The prevalence rate of ophthalmic morbidity varies significantly across the country where the source of air pollutants is also very diverse. We have categorized all the states into 6 different regions viz. North, South, East, West, Northeast and Central. The highest mean prevalence is observed in the Southern region and the lowest is found in the Central region as shown in Fig. 2b. The seasonal variation of the occurrence of ophthalmic-related cases is higher in March in the year 2018-19 and July in 2019-20 with nearly 10% of the total cases in the respective years. The lowest ophthalmic cases are recorded in the month of April 2018-19 and March 2019-20 with 7·3% and 6·6% of the total cases respectively as shown in Fig. 2c.


(a) District-wise number of ophthalmic outpatients/10 km2. (b) Spatial variation of ophthalmic prevalence in the country in 2019-20. (c) Temporal variation of number of ophthalmic outpatients in India. (d) State-wise gender-specific crude prevalence rate of ophthalmic cases in various age groups. (e) Comparison of crude prevalence rate and age-standardized prevalence rates of State & UTs. (Figures are generated using software (a) ArcGIS 10.6 (https://www.esri.com/en-us/home), (b, c, d, e) Origin 2022 (https://www.originlab.com/))
The state-wise gender-specific crude prevalence of ophthalmic disease with varying age groups is estimated in this study. As depicted in Fig. 2d, the incidence of eye diseases escalates with advancing age. High-altitude states such as Himachal Pradesh, Sikkim, and Jammu & Kashmir exhibit a higher prevalence of ophthalmic cases. Furthermore, the data reveals that females in nearly all states are more prone to ophthalmic diseases than males. Alarmingly, more than half of the states, report a prevalence rate exceeding the national average. Conversely, Fig. 2e presents age-standardized prevalence rates (ASPR) per 100,000, indicating that union territories (UTs) demonstrate a higher prevalence due to the elevated number of ophthalmic cases, despite having a lower population across age groups. The North-Eastern states exhibit a higher age-standardized prevalence than the crude rate, suggesting that the inhabitants are more susceptible to developing ophthalmic diseases compared to the rest of India.
In the present study, the PM2·5 emission burden in the year 2019-20 is considered from published dataset and presented in a high-resolution (0·1° × 0·1°) gridded map (Fig. 3a). The calculated total emission is found to be ~ 8·32 Tg/yr of PM2·5, emitted from 16 major and unattended anthropogenic sources over ~ 30,000 grids using the statistical model. The satellite PM2·5 data retrieved from the SEDAC, NASA is presented in Fig. 3b. The maximum emission load is recorded from the Indo-Gangetic plain and Southern India as depicted in both maps. Aggravations in anthropogenic activities like transportation, industries, crop residue burning, and residential activities are responsible for increased PM2·5 emissions in the regions. Figure 3c shows the fuel-specific contribution to the annual PM2·5 emission in India. Biomass burning such as wood, crop residue burning, and cow dung is the major source of PM2·5 emissions followed by fossil fuel consumption in vehicles, industry and power plants.

(a) Spatial distribution of PM2·5 Emission in 2019-20 (t/yr). (b) Spatial distribution of PM2·5 concentration in 2019 (µg/m3). (c) Relative contribution of various activities in PM2·5 emission in India. (Figures are generated using software (a, b) ArcGIS 10.6 (https://www.esri.com/en-us/home), (c) Origin 2022 (https://www.originlab.com/))
The univariate linear regression analysis presented in Fig. 4a showed that an increase in the PM2·5 emission burden will lead to prolonged exposure to a larger population and is associated with the intensification of ophthalmic cases in India. The slopes of association between district-wise PM2·5 and district-wise Ophthalmic outpatients suggested a significant positive correlation (r = 0·54, 95% CI 0·48–0·59, P < 0·001). However, the top 20 districts with the highest ophthalmic cases show a greater association (r = 0·74, 0·43–0·89, P < 0·001) with the PM emission. An increase of 1% in the PM2·5 emission burden is responsible for nearly 0·25 million Ophthalmic cases in the country. However, the association between PM2·5 concentration and ophthalmic cases as shown in Fig. 4b is not statistically significant (r = 0·07, -0·002–0·15, P = 0·06). Figure 4c illustrates the relationship between PM2·5 Emission load and PM2·5 concentration which depicts a moderate correlation among them (r = 0·35, 0·29–0·42, P < 0·001). The relationship between the meteorological parameters like temperature, precipitation and humidity with ophthalmic outpatients are presented in Fig. 4d–f respectively. Temperature shows a statistically significant low association with the onset of ophthalmic cases (r = 0.15, 0.08–0.23, P < 0.001). Unlike temperature, precipitation shows a negative association with the occurrence of ophthalmic cases in India (r= -0.13, -0.21- -0.06, P < 0.001). The correlation between the number of hospital footfalls and humidity is very low and not statistically significant (r = 0.09, 0.01–0.16, P = 0.02). Figure 4g illustrates the correlation matrix of meteorological parameters and air pollution with the number of ophthalmic outpatients. The multivariate analysis shows the multiple correlation coefficient (r) is 0.52 in which the PM2.5 emission load is only statistically significant among all the parameters. The partial regression coefficients of PM2.5 emission, humidity, temperature, and precipitation are 0.49, 0.03, 0.05, and 0.08, respectively. As shown in Fig. 4h, it is evident that the maximum number of eye diseases recorded in the districts having 10,000 to 15,000 t/yr of PM2·5 emissions. Districts/megacities like Central Delhi, Bangalore, Mumbai, and Varanasi fall in this category, and it is noticed that the onset of eye disease is higher in these districts.


Scatter plot of (a) PM2·5 Emission load and number of Ophthalmic outpatients, (b) PM2·5 Concentration and number of Ophthalmic outpatients, (c) PM2·5 Emission load and PM2·5 Concentration, (d) Temperature and number of Ophthalmic outpatients, (e) Precipitation and number of Ophthalmic outpatients, (f) Humidity and number of Ophthalmic outpatients, (g) Correlation coefficients heatmap of all the variables, (h) PM2·5 emission and corresponding onset of Ophthalmic outpatients in India. (Figures are generated using software (a, b, c, d, e, f) MedCalc software 22·0 (https://www.medcalc.org/), (g, h) Origin 2022 (https://www.originlab.com/))
The prime importance of considering the emission inventory in health analysis lies in the understanding of source-specific regional/local level emission load and its relationship with disease exacerbation in a particular geographic area. In the analysis, all 16 types of major and unattended sources demonstrated their association with the onset of Ophthalmic cases across the country. Sectoral attribution as shown in Table 1, depicts that household cooking activity shows a greater correlation in the overall and rural occurrence of ophthalmic cases followed by indoor sources like smoking activities, incense stick and mosquito coil burning followed by outdoor sectors like the solid waste burning, street food vendor and transport are the other major sectors that shows good correlation.
On the basis of satellite based derived PM2·5 concentration data, districts are identified where the annual average PM2·5 pollution levels greater than the NAAQS level i.e., 40 µg/m3. People residing in those districts are considered exposed populations and the rest are considered unexposed populations (Table 2). The epidemiological analysis is carried out based on the above scenario and presented in Table 3.
Discussion
This first-of-its-kind national-level observational-based cross-sectional retrospective study demonstrates the relation between the onset of ophthalmic cases and sectoral PM2·5 emission load. The study established that there is a significant correlation between PM2·5 emission and eye disease i.e., with an increase in PM2·5 emission load there is a sizable chance of ophthalmic disease occurrence. It is observed that the prevalence of ophthalmic cases is prominent in the Southern part of India where industrial activities are dominating in contrast to transportation and residential sources in the rest of India. The monthly variation of the number of eye patients showed that there is a steady increase in cases with the onset of the winter season in both the years 2018-19 and 2019-20. In winter months, there are many new sources are added like brick kilns, crop residue burning in Northern India, waste burning, festivals, road dust, and cooking activities along with traditional sources like transport and industrial etc. Due to dry air in the winter season, the effect of PM2·5 becomes harsher, imposing a greater risk to eye health.
In the month of May to July, there is also an increased number of eye disease cases recorded as it is observed that industrial, transport and power are dominating followed by forest/biomass burning. There are summer holidays in those months, so outdoor activity of children increases during that period. Similarly, an exacerbation in eye health can be noticed in the month of September to November as the festive season in India is observed resulting in an increase in indoor cooking activities, outdoor activities, biomass and crackers burning, solid waste burning, road dust construction activities and transportation. With the increasing trend of emissions, it is found that there is a nearly 15% increment in ophthalmic cases compared to the previous year. However, March 2020 shows a steep decrease in ophthalmic cases as there is a lockdown imposed across the country at the onset of the COVID-19 pandemic. Figure 5 shows the spatial variation of state-wise prevalent Ophthalmic cases per 10 km2 and 100,000 population and its comparison with the GBD-2019 data depicted in the map. There are slight disparities that can be noticed between the current study and the GBD study. However, the total number of cases reported in the GBD-2019 study is nearly 6-fold (184 million) of the national level data recorded by MoHFW18. The states having lower populations like Union Territories, Sikkim, Jammu & Kashmir are showing a higher prevalence ratio.

(a) State-wise ophthalmic outpatient prevalent cases per 10 km2 in current study (b) State-wise ophthalmic outpatient prevalent cases per 100000 population in GBD-2019 study. (Figures are generated using software (a) ArcGIS 10.6 (https://www.esri.com/en-us/home), (b) GBD 2019 (https://vizhub.healthdata.org/gbd-compare/india#0))
Further, the satellite-based PM2·5 concentration data and eye disease prevalence are compared and related, which shows a very nominal correlation between them. Moreover, it does not provide any source-specific information that has closely linked with impact on health. In that case, emission inventory can provide both spatial and temporal variation of source-specific pollutant data. The emission inventory of PM2·5 shows a significant association with the number of ophthalmic outpatients across the country. In urban regions transportation, construction activity, solid waste burning and street food vendors and in rural areas road dust, brick kilns, biomass as cooking fuel, smoking, incense stick and mosquito coil burning are the sectors that predominately contribute to the PM2·5 emission and have shown a greater correlation with the rising eye disease.
It is also observed that the risk of ophthalmic disease in the rural is relatively higher than the urban. The risk of eye disease in the exposed rural population is 4 times higher than the unexposed population. Unlikely, in urban regions, both exposed and unexposed populations are equally vulnerable to eye disease. The contribution of PM2·5 in developing ophthalmic morbidity in rural populations is more than 70%, which rose to nearly 77% in the exposed rural people. It is also inferred from the above study that the districts having PM2·5 emissions load of range 5000 to 20,000 t/yr account for more than 60% of the total ophthalmic outpatients. However, there is no significant association found between the PM2·5 concentration and the number of Ophthalmic outpatients. This is the first-ever attempt to establish a nationwide study by analyzing the effect of PM2·5 exposure on the onset of Ophthalmic cases in India. However, there are several regional-level studies present, in which the effect of PM2·5 on eye health is studied. Das and Basu (2021) studied the effect of various meteorological and atmospheric pollutant parameters on the eye health of patients (< 21 years age) in Hyderabad. Their findings show no statistically significant correlation present between the PM2·5 concentration and Allergic eye disease (r2 = 0·15, P = 0·2118).31 According to the report of the ICMR-EYE SEE Study conducted by Tandon et al. (2020), Aerosol Optical Depth (AOD) has a possible positive correlation with the onset of cataracts in people (> 40 years age) in Delhi, Guwahati and Prakasam39. Gupta et al. (2002) demonstrated the association between air pollution and subclinical ocular surface. The clinical parameter like tear film break-up time was significantly reduced in the exposed group than in the unexposed group28. Similarly, in a population-based cohort study comprising people from Northern and Southern India of > 60 years old, Ravilla et al. (2016) established that women using biomass for cooking activity are three times more vulnerable than women cooked with cleaner fuel. A statistically significant association was found between PM2·5 and cataract eye disease among the study population30. Krishnan et al. (2019) studied the exacerbation of eye illness due to exposure of PM2·5, which is statistically significant as well in the study population aged 21–30 years for over 6 months in Kodungaiyur, Chennai40.
Unlike other studies, the current findings established that the source-specific PM2·5 emission pattern has a positive relationship with eye disease. The present study features significant strengths, including a robust sample size and a longitudinal cohort design. Present investigation establishes the correlation between the prevalence of Ophthalmic disease and the impact of sectoral PM2·5 exposure across India. We acknowledge there may be some lacunas in our stud;, firstly, the study design was cross-sectional. Thus, the results do not provide conclusive evidence for a cause-and-effect relationship. Secondly, the monthly variations of PM2·5 emission and its association with corresponding ophthalmic cases are not considered for the analysis. Thirdly, the effect of other comorbidities is also not taken into account. Despite the limitations, this study is important as the developed dataset will be used to locate the emission hotspots of PM2·5 and better quantify the role of different natural and anthropogenic sources and their impact on eye health.
Conclusion
The current approach aimed at describing the association of sectoral PM2·5 emission load with ophthalmic cases across India. The spatial pattern of ophthalmic disease occurrence illustrated that Southern India is the most vulnerable as compared to the rest of the country. The age-standardized prevalence rate suggests that people residing in high-altitude regions like North and North-east India and the UTs are more susceptible to developing eye disease. It is also evident from the analysis that ophthalmic disease becomes more prevalent with advancing age and females are the vulnerable group in almost all states. The sectoral emission suggested that residential cooking activities, solid waste burning, transportation and wind-blown road dust are the major sources responsible for the onset of ophthalmic disease. The findings demonstrated that a reliable emission inventory with detailed sectoral pollutant load could be the first line of scientific tool for health study in a country like India to counter the scarcity of air quality monitoring networks. The satellite-derived PM2·5 concentration is not found statistically significant and has a very nominal correlation with eye disease prevalence. The sectoral contribution of the disease prevalence dataset can be used for the benefit of policymakers and facilitate advanced technological mitigation measures to curtail the impact of specific sectors to control adverse health effects in a particular region.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Change history
02 June 2025
The original online version of this Article was revised: In the original version of this Article, Poonam Mangaraj, Ravi Yadav, Mahesh Chandra Sahu, Bhishma Tyagi, Sachin S. Gunthe and Madhusmita Mishra were incorrectly affiliated with “Department of Environmental Science, Berhampur University, Bhanja Vihar 760007, Vihar, India”.
References
World Health Organization: WHO. 9 out of 10 people worldwide breathe polluted air, but more countries are taking action. Who.int (2018). https://www.who.int/news-room/detail/02-05-2018-9-out-of-10-people-worldwide-breathe-polluted-air-but-more-countries-are-taking-action
Sinharay, R. et al. Respiratory and cardiovascular responses to walking down a traffic-polluted road compared with walking in a traffic-free area in participants aged 60 years and older with chronic lung or heart disease and age-matched healthy controls: A randomised, crossover study. Lancet 391, 339–349 (2018).
Su, C. et al. Short-term effects of fine particulate air pollution on cardiovascular hospital emergency room visits: A time-series study in Beijing, China. Int. Arch. Occup. Environ. Health. 89, 641–657 (2015).
Zhong, J. Y., Lee, Y. C., Hsieh, C. J., Tseng, C. C. & Yiin, L. M. Association between dry eye disease, air pollution and weather changes in Taiwan. Int. J. Environ. Res. Public Health. 15, 2269 (2018).
Lelieveld, J., Evans, J. S., Fnais, M., Giannadaki, D. & Pozzer, A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 525, 367–371 (2015).
Sagai, M. Toxic Components of PM2.5 and their toxicity mechanisms—on the toxicity of sulfate and carbon components—. Nippon Eiseigaku Zasshi (Japanese Journal of Hygiene) 74, n/a (2019).
Katsouyanni, K. et al. Short term effects of air pollution on health: A European approach using epidemiologic time series data: The APHEA protocol. J. Epidemiol. Community Health. 50, S12–S18 (1996).
Leitte, A. M. et al. Size-segregated particle number concentrations and respiratory emergency room visits in Beijing, China. Environ. Health Perspect. 119, 508–513 (2010).
Cohen, A. J. et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of diseases Study 2015. Lancet 389, 1907–1918 (2017).
Pandey, A. et al. Health and economic impact of air pollution in the States of India: The global burden of Disease Study 2019. Lancet Planet. Health 5, (2020).
Balakrishnan, K. et al. The impact of air pollution on deaths, disease burden, and life expectancy across the States of India: the global burden of Disease Study 2017. Lancet Planet. Health. 3, e26–e39 (2019).
Sahu, S. K., Beig, G. & Parkhi, N. Critical emissions from the largest on-road transport network in South Asia. Aerosol Air Qual. Res. 14, 135–144 (2014).
Sahu, S. K. et al. Quantifying the high resolution seasonal emission of air pollutants from crop residue burning in India. Environ. Pollut. 286, 117165 (2021).
Sahu, S. K., Mangaraj, P. & Beig, G. Decadal growth in emission load of major air pollutants in Delhi. Earth Syst. Sci. Data. 15, 3183–3202 (2023).
Mustafić, H. et al. Main Air pollutants and myocardial infarction. JAMA 307, 713 (2012).
Forouzanfar, M. H. et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the global burden of Disease Study 2015. Lancet 388, 1659–1724 (2016).
Sa, M. et al. Effect of environmental air pollution on type 2 diabetes mellitus. PubMed 19, 123–128 (2015).
Institute for Health Metrics and Evaluation & Compare, G. B. D. Healthdata.org (2019). https://vizhub.healthdata.org/gbd-compare/
Cohn, M. J. & Kurtz, D. L. Frequency of certain urgent eye problems in an emergency room in Massachusetts. PubMed 63, 628–633 (1992).
Watson, S., Cabrera-Aguas, M. & Khoo, P. Common eye infections. Australian Prescriber. 41, 67 (2018).
Novaes, P. et al. Ambient levels of air pollution induce goblet-cell hyperplasia in human conjunctival epithelium. Environ. Health Perspect. 115, 1753–1756 (2007).
Fujishima, H. et al. Effects of diesel exhaust particles on primary cultured healthy human conjunctival epithelium. Ann. Allergy Asthma Immunology: Official Publication Am. Coll. Allergy Asthma Immunol. 110, 39–43 (2013).
Fu, Q. et al. Air pollution and outpatient visits for conjunctivitis: A case-crossover study in Hangzhou, China. Environ. Pollut. 231, 1344–1350 (2017).
Szyszkowicz, M., Kousha, T. & Castner, J. Air pollution and emergency department visits for conjunctivitis: A case-crossover study. Int. J. Occup. Med. Environ. Health. 29, 381–393 (2016).
Gao, Z. X. et al. Assessment of DNA damage and cell senescence in corneal epithelial cells exposed to Airborne Particulate Matter (PM2.5) collected in Guangzhou, China. Investig. Ophthalmol. Vis. Sci. 57, 3093–3093 (2016).
Saxena, R. et al. Impact of environmental pollution on the eye. Acta Ophthalmol. Scand. 81, 491–494 (2003).
Ghosha, R., Ghosh, D., Ghosh, S. & Mukherjee, G. Impact of climate change and related environmental factors on eye health in India - A narrative review. Ecol. Environ. Conserv. 29, 845–850 (2023).
Gupta, S. K., Gupta, V., Joshi, S. & Tandon, R. Subclinically dry eyes in Urban Delhi: An impact of Air Pollution? Ophthalmologica 216, 368–371 (2002).
Gupta, S. et al. A multicentric case-control study on the impact of air pollution on eyes in a metropolitan city of India. Indian J. Occup. Environ. Med. 11, 37 (2007).
Ravilla, T. D. et al. Use of cooking fuels and cataract in a population-based study: The India eye disease study. Environ. Health Perspect. 124, 1857–1862 (2016).
Das, A. V. & Basu, S. Environmental and air pollution factors affecting allergic eye disease in children and adolescents in India. Int. J. Environ. Res. Public Health. 18, 5611 (2021).
Vashist, P. et al. Association of cataract and sun exposure in geographically diverse populations of India: The CASE study. First Report of the ICMR-EYE SEE Study Group. PLOS ONE. 15, e0227868 (2020).
Mangaraj, P., Sahu, S. K., Beig, G. & Yadav, R. A comprehensive high-resolution gridded emission inventory of anthropogenic sources of air pollutants in Indian megacity Kolkata. SN Appl. Sci. 4, (2022).
Mangaraj, P., Sahu, S. K., Beig, G. & Samal, B. Development and assessment of inventory of air pollutants that deteriorate the air quality in Indian megacity Bengaluru. J. Clean. Prod. 360, 132209 (2022).
MoHFW. Ministry of Health and Family Welfare | GOI. https://main.mohfw.gov.in/
Sahu, S. K. et al. Development and comprehensive analysis of spatially resolved technological high resolution (0.1°×0.1°) Emission Inventory of Particulate Matter for India: A step towards Air Quality Mitigation. doi: (2023). https://doi.org/10.5194/essd-2023-310
Hammer, M. S. et al. Global Annual PM2.5 Grids from MODIS, MISR and SeaWiFS Aerosol Optical Depth (AOD), 1998–2019, V4.GL.03. Palisades (NASA Socioeconomic Data and Applications Center (SEDAC, 2022).
Cohen, J. A power primer. Psychol. Bull. 112, 155–159 (1992).
Tandon, R. et al. Association of dry eye disease and sun exposure in geographically diverse adult (≥ 40 years) populations of India: the SEED (sun exposure, environment and dry eye disease) study - second report of the ICMR-EYE SEE study group. Ocul. Surf. 18, 718–730 (2020).
Krishnan, M. A. et al. Effects of ambient air pollution on respiratory and eye illness in population living in Kodungaiyur, Chennai. Atmos. Environ. 203, 166–171 (2019).
Funding
This full research work did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Saroj Kumar Sahu (SKS) conceived the present idea, analyzed the data and reviewed the manuscript; Ashirbad Mishra (AM) wrote the whole paper and analyzed and plotted the data for necessary discussion. Poonam Mangaraj (PM), Ravi Yadav (RY), Mahesh Kumar Sahu (MKS) and Gufran Beig (GB) reviewed the results and provided useful insight. Bhisma Tyagi (BT) and Sachin S Gunthe (SSG) reviewed the manuscript, B. Anjan Kumar Prusty (BAKP), and Madhusmita Mishra (MM) improved the writing and suggested a justified conclusion.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sahu, S.K., Mishra, A., Mangaraj, P. et al. Source-specific fine particulates emission linked to prevalence of ophthalmic cases in India. Sci Rep 15, 11183 (2025). https://doi.org/10.1038/s41598-024-82914-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-82914-6
