
Abstract
Alexithymia, a cognitive and emotional deficit characterized by difficulty in expressing emotions and identifying feelings, poses significant challenges in healthcare settings. Developing a reliable and valid tool to measure alexithymia in post-prostatectomy patients would not only aid healthcare professionals in identifying at-risk individuals but also facilitate early intervention and targeted support. This study aimed to translate the Brief Form of the Normative Male Alexithymia Scale (NMAS-BF) into Simplified Chinese, evaluate the reliability and validity of the Chinese version, and explore its influencing factors. The English version of the NMAS-BF was translated into Chinese according to Brislin’s translation guidelines. A survey was administered to 430 patients who had undergone radical prostatectomy across four tertiary-grade A hospitals in China. To assess test-retest reliability, 30 patients completed the survey twice. Data analysis was performed using SPSS 26.0 and AMOS 22.0. Exploratory and confirmatory factor analyses were conducted to evaluate the content validity, construct validity, reliability, and concurrent validity of the translated NMAS-BF. Additionally, Pearson’s correlation, t-tests, and analysis of variance (ANOVA) were used to identify factors influencing the NMAS-BF. The Cronbach’s alpha coefficient for the Chinese version of the NMAS-BF was 0.856. The intra-class correlation coefficient (ICC) for the total scale was 0.938, indicating good stability. Content validity was satisfactory, with exploratory factor analysis revealing a single-factor model that accounted for 58.965% of the variance. Confirmatory factor analysis (χ²/df = 1.371, RMSEA = 0.041) demonstrated acceptable construct validity. Statistically significant differences in alexithymia levels were observed across patients with varying educational levels, family residence, household monthly income, and number of children. Perceived stress, mutuality, social impact, and self-esteem were identified as significant factors influencing alexithymia. This study initially translated the Brief Form of the Normative Male Alexithymia Scale (NMAS-BF) into Chinese and demonstrated its psychometric validity for assessing alexithymia in patients post-radical prostatectomy. By identifying alexithymic patterns and their contributing factors, the research aims to improve emotional expression and enhance the mental well-being of Chinese patients undergoing this procedure. Furthermore, the factors identified in the Chinese version of the NMAS-BF may provide valuable theoretical insights for future intervention studies.
Similar content being viewed by others

Introduction
Prostate cancer is the second most commonly diagnosed cancer and the sixth leading cause of cancer-related death among men worldwide. By 2040, the incidence of prostate cancer is projected to increase to nearly 2.3 million new cases and 740,000 deaths, primarily due to population growth and aging1.Radical prostatectomy (RP) is a widely performed curative treatment aimed at preventing metastasis, with a 5-year survival rate of 95%. Although RP improves survival rates and reduces metastasis, it is associated with a high incidence of complications. Nearly 80% of men experience incontinence following RP, with many remaining incontinent for more than 12 months2. Additionally, patients report a decline in role and social functioning, and 61.4% experience sexual impotence3. Mungovan also asserted that most men who undergo RP face predictable functional impairments, including urinary incontinence and erectile dysfunction, which significantly reduce their quality of life and psychosocial well-being4.
More than half of cancer patients experience difficulty articulating and expressing their emotions, a condition known as alexithymia5. Alexithymia is a complex trait characterized by challenges in identifying emotions, difficulty expressing feelings, and a tendency to focus on external events rather than internal experiences. It is one of the most common emotional symptoms found among cancer survivors, strongly associated with depressive symptoms, pain, and somatic symptom disorders. Moreover, it serves as a unique predictor of men’s fear of heterosexual intimacy6,7,8. Cancer patients exhibit higher average scores on the Toronto Alexithymia Scale compared to healthy controls, indicating more severe levels of alexithymia9. This condition is also linked to a tendency to suppress emotions and negative feelings in response to stress10, as well as to neurobiological characteristics unique to men, such as heightened noradrenergic activity and reduced baseline hypothalamic-pituitary-adrenal (HPA) axis activity11,which may jointly contribute to the development of alexithymia. Furthermore, men are often socialized to conform to traditional masculine norms, which emphasize qualities such as toughness, aggression, competitiveness, dominance, independence, and emotional restraint. Social Identity Theory suggests that individuals who place high value on these masculine norms are more likely to avoid emotional expression12. One study found that the prevalence of alexithymia in male cancer patients is 40%, exceeding that in female cancer patients (33.8%)7.
Nearly 60% of individuals with prostate cancer experience psychological distress, including symptoms such as fear, anxiety, sleep disturbances, and a sense of isolation. These symptoms typically begin at diagnosis and can persist for up to eight years after treatment13. Postoperative complications can significantly affect men with prostate cancer, leading to depressive symptoms that are four times more prevalent in these patients compared to healthy individuals14. However, prostate cancer patients are generally less likely to disclose feelings of depression and anxiety than those with other types of cancer13. Social Role Theory posits that individuals are assigned different roles based on their gender15. Patients following radical prostatectomy often emphasize the significance of their role as the head of the family. Although fulfilling this role has become more challenging, they continue to cling to it, feeling obligated to remain courageous and strong for their families. However, they are no longer able to perform this role effectively, as they feel compelled to conceal their true emotions and maintain the façade of normalcy, which limits their ability to express themselves16. Urinary, sexual, and bowel dysfunctions after radical prostatectomy can significantly affect a patient’s social relationships, including those with intimate partners, family, and friends16. These dysfunctions may also create social barriers that inhibit emotional expression17. For instance, openly discussing sexual dysfunctions is often stigmatized, as it may be perceived as a loss of masculinity and threaten a man’s sense of identity16. Recognizing alexithymia and promptly implementing interventions are crucial for mitigating depressive symptoms and improving the overall well-being of post-prostatectomy patients.
The most commonly used self-assessment tools for diagnosing alexithymia in adults include the Toronto Alexithymia Scale (TAS-20)18, the Toronto structured interview for alexithymia (TSIA)19, and the Bermond-Vorst alexithymia questionnaire (BVAQ)20. However, these instruments primarily focus on the general experience of alexithymia without explicitly addressing its gender-specific aspects, particularly from a male perspective. The Normative Male Alexithymia Scale, developed by Levant to assess men’s difficulties in recognizing, articulating, and especially expressing emotions, consists of 20 items, with responses rated on a 7-point scale (1 = strongly disagree; 7 = strongly agree)21, In 2019, a simplified version, the NMAS-BF, was created by removing duplicate items. The revised version demonstrated good reliability, with a Cronbach’s alpha coefficient of 0.80024. This study aims to validate and assess the reliability of the NMAS-BF in Chinese patients following radical prostatectomy, and to explore the factors influencing alexithymia, thereby providing a theoretical basis for developing interventions to alleviate alexithymia and associated negative emotions.
Materials and methods
Study design
A cross-sectional study was conducted in four hospitals in Henan Province, China, from January 2023 to May 2024.
Sample
Patients who underwent radical prostatectomy at four tertiary-grade A hospitals participated in this study. All patients met the inclusion criteria and were selected through convenience sampling. This study included 13 independent variables (Seven demographic variables, six factors: NMAS-BF, Twenty-item Tronto alexithymia scale, Mutuality Scale, Perceived stress Scale, Self-Esteem Scale and Social Impact Scale) after a literature review and expert consultation. The sample size of multi-factor analysis should be 5–10 times the number of independent variables23. Considering a 20% sample loss rate, the required sample size ranged from 78 to 156 participants. In practice, 430 patients were enrolled. Inclusion criteria: Inclusion criteria: ①Diagnosed with prostate cancer through biopsy; ②Patients who underwent radical prostatectomy; ③Voluntarily agreed to participate in the study after being informed; ④Expected survival of more than 1 year; ⑤Cognitively normal patients who are capable of regular communication. Exclusion criteria: ①Patients with concurrent other types of tumors; ②With other severe physical illnesses who are unable to cooperate with the investigation; ③Patients whose family members request that the diagnosis be concealed from them.The study was approved by the Ethics Committee of Henan Provincial People’s Hospital [(2019) Review No.74]. Informed consent was obtained from all participants, who took part in the study voluntarily and anonymously.
Measures
General information questionnaire
Designed by the researchers themselves, including: age, marital status, education level, family income, medical insurance form, residence, quantity of children, etc.
NMAS-BF
The Normative Male Alexithymia Scale-Brief Form (NMAS-BF), a unidimensional scale consisting of six items that assess men’s difficulties in recognizing, articulating, and especially expressing emotions22 This scale uses a seven-point Likert rating method (1 = Strongly disagree,7 = Strongly agree). Item 1“I feel comfortable expressing my affection to family members and friends”, and Item 3 “When someone close to me hurts my feelings, I am able to tell them that I am hurt” are reverse-scored items. To obtain the total score (mean item score), reverse the scores of the reverse-scored items and calculate the mean. A higher score indicates a higher level of alexithymia.
Twenty-item tronto alexithymia scale
The 20-item Toronto Alexithymia Scale (TAS-20) consists of three dimensions: difficulty identifying and distinguishing emotions, difficulty describing feelings, and externally oriented thinking. It uses a five-point Likert scale, with responses ranging from “strongly agree” (5) to “strongly disagree” (1). The total score ranges from 20 to 100, with higher scores indicating greater levels of alexithymia18. Yi24 translated and validated the scale into Chinese, demonstrating good reliability and validity. In this study, the Cronbach’s ɑ of the scale is 0.920.
Mutuality scale
The tool, developed by Archbold in 199027, was introduced to Taiwan by Liu26. It includes four dimensions: love and affection, sharing happiness, sharing values, and reciprocity, with a total of 15 items. Each item is scored on a scale from 0 (not at all) to 4 (very much). The scoring method uses the average score, with a range of 0 to 4. Higher scores indicate a stronger interdependence relationship, while a score below 2.5 suggests a poor interdependence relationship. In this study, the Cronbach’s alpha of the scale was 0.972.
Perceived stress scale
The Perceived Stress Scale (PSS), originally developed by Cohen, is a globally recognized instrument for measuring general stress perception. Yang later adapted the PSS for Chinese cultural and national contexts27. The Chinese Perceived Stress Scale (CPSS) consists of two dimensions and 14 items. Respondents rate each item on a 5-point Likert scale, ranging from 0 to 4, with a total score range of 0 to 56. In this study, the Cronbach’s alpha of the scale was 0.877.
Social impact scale
The Social Impact Scale (SIS), developed by American scholar Wright, was translated into Chinese in 2007 for widespread use in China28. This scale uses a 4-point Likert scale to measure various aspects of patients’ feelings of stigma across four dimensions. The total score is the sum of the scores from the four dimensions, with higher scores indicating greater perceived social impact. The SIS is widely used to measure illness-related stigma in patients with chronic diseases such as cancer. In this study, the Cronbach’s alpha of the scale was 0.931.
The self-esteem scale
The Self-Esteem Scale (SES), developed by Rosenberg in the United States, was initially designed to assess adolescents’ feelings of self-acceptance and self-worth. It was later translated into Chinese to evaluate individuals’ levels of self-esteem29. The scale consists of 10 items, with a total score ranging from 10 to 40, with higher scores indicating higher levels of self-esteem. In this study, the Cronbach’s alpha of the scale was 0.853.
Translation procedure
Permission to translate and use the scale was obtained from the original author via email. The translation process followed Brislin’s model strictly30. First, two native Chinese speakers independently translated the scale into two Chinese versions (A and B). One translator, a nurse with a master’s degree, and the other holding a master’s degree in a non-medical field, worked autonomously. Afterward, the research team and translators discussed and integrated the two versions into a single draft (Version C), which aligned with the original scale both linguistically and conceptually. Second, two nursing Ph.D. candidates, who were not familiar with the original scale, independently back-translated Version C into English, resulting in two back-translations (D and E). The research team then compared the back-translations with the original scale, integrating and revising them iteratively to ensure consistency with the original English version. This process culminated in the final integrated Chinese translation (Version F).
Scale cultural adaptation
Six nursing experts with expertise in alexithymia were invited to evaluate the Chinese Version F using a 4-point Likert scale. The evaluation focused on the clarity of item descriptions, the relevance of content, and other aspects. The rating scale was as follows: 4 = highly relevant, 3 = moderately relevant, 2 = weakly relevant, and 1 = irrelevant. Of the six experts, one was a graduate student and five were undergraduates. Two held senior titles, and four held intermediate titles. All experts had at least eight years of work experience. Based on their feedback, revisions were made to produce the pre-test version of the translated scale.
Pretest
A pilot study was conducted using a general information questionnaire and the pre-test version of the scale. Prior to the survey, patients were informed about the questionnaire requirements, the research objectives, and confidentiality procedures. After completing the test, interviews were conducted with participants to gather feedback on the questionnaire instructions, individual items, and options. Based on their input, revisions were made to the questionnaire, resulting in the final Chinese version of the NMAS-BF.
Data collection
Data collection was conducted through on-site surveys, which were distributed to eligible patients along with prior information on the survey’s significance, research objectives, and completion instructions. Patients were instructed to complete the survey honestly, and their anonymity was ensured. The completeness of the surveys was verified on-site, and data entry was double-checked for accuracy. Additionally, 30 patients were randomly selected to complete the survey again two weeks later to assess retest reliability.
Data analyses
Statistical analysis was performed using SPSS 26.0 and AMOS 22.0. Descriptive statistics are presented as means and percentages. Continuous variables are reported as means with standard deviations, while categorical variables are expressed as frequencies and percentages.
The internal consistency of the scale was assessed using Cronbach’s α coefficient and split-half reliability. Test-retest reliability and inter-rater reliability were evaluated using intra-class correlation coefficients (ICCs). Evaluation criteria for Cronbach’s α coefficient are as follows: ≥0.9 indicates very high reliability, 0.8–0.9 indicates high reliability, and 0.7–0.8 indicates acceptable reliability31. Thirty participants were selected for a retest two weeks later, and the correlation coefficient was calculated based on their scores from both tests. An ICC greater than 0.7 indicates good test-retest reliability for the scale32. Content validity was evaluated using the item-level content validity index (I-CVI). Six experts were invited to rate the relevance of each item in the Chinese version of the scale. An I-CVI of ≥ 0.78 was considered indicative of good content validity33. Discriminant validity was assessed using the critical ratio method. The total scale scores were sorted from highest to lowest, with the top 27% forming the high-score group and the bottom 27% forming the low-score group. Independent samples t-tests were performed to compare item scores between the two groups. Items with statistically significant differences were retained. For exploratory factor analysis (EFA), half of the data was randomly allocated, while the other half was used for confirmatory factor analysis (CFA). The structural validity was assessed using EFA with principal component analysis and maximum variance orthogonal rotation. Factor extraction was based on eigenvalues ≥ 1.0, and item selection was determined by factor loadings ≥ 0.4036. CFA was conducted using AMOS 22.0, employing the maximum likelihood method. The common factors were treated as latent variables, and the items were treated as observed variables to construct the model. The structural validity of the scale was further assessed using several fit indices, including Chi-square/df (χ²/df), Root Mean Square Error of Approximation (RMSEA), Goodness of Fit Index (GFI), Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), Adjusted Goodness of Fit Index (AGFI), and Normed Fit Index (NFI). Simultaneously, we constructed a multi-group model to further analyze the validity of the NMAS-BF across different demographic groups. We assumed equal measurement weights, equal structural covariances, and equal measurement residuals, and tested for significant changes in the chi-square values. If P > 0.05, it would indicate that the increase in chi-square values does not reach the 0.05 significance level, suggesting that the two models can be considered equivalent34.
The TAS-20, a widely used measure of alexithymia, includes difficulties in identifying and describing feelings, while the NMAS-BF focuses on normative alexithymia in men. Both scales share conceptual overlap in the challenges related to identifying and expressing emotions. Levant’s research demonstrated that NMAS-BF scores significantly predicted variance in restrictive emotionality scores, beyond what was predicted by TAS-20 scores22. Therefore, criterion-related validity was assessed through Pearson or Spearman correlation analysis between the TAS-20 and NMAS-BF, with a correlation coefficient closer to 1 indicating higher criterion-related validity.T-tests and analysis of variance (ANOVA) were conducted to examine the factors influencing alexithymia. A p-value of less than 0.05 was considered statistically significant.
Results
Cultural adaptation of the scale
During the cultural adaptation phase, experts, drawing on clinical practice, provided feedback on the draft version of the Chinese NMAS-BF. Their suggestions focused on whether the conceptual expressions were clear and easy to understand and whether they aligned with clinical practice for the six items in the draft. Item 1, “I feel comfortable expressing my affection to family members and friends,” was revised from “我可以很自然地向家人和朋友表达我的爱意” to “我能自在地向家人和朋友表达我的情感.” This change was made because “情感” encompasses a broader range of emotional types covered by “affection,” such as love, familial bonds, friendship, concern, care, gratitude, and other nuanced sentiments. The phrase faithfully reflects this inclusiveness, capturing various emotions expressed to family and friends. In contrast, “爱意” is relatively limited, focusing mainly on love or fondness. The revised expression “能自在地表达情感” better aligns with the need for comprehensive and multifaceted emotional expression, making it applicable to a wider range of scenarios. Item 2, “I have difficulty telling others that I care about them” was revised from “我感觉很难告诉别人我关心他们” to “我很难向别人表达我对他们的关心”. This change was made because the latter emphasizes the behavioral aspect of expressing care, focusing on the core action. It highlights the challenge of translating internal care into external forms such as verbal communication, visible gestures, or practical actions. This aligns closely with the common struggle people face in figuring out how to convey their concern. And it’s phrasing is concise, straightforward, and semantically clear, making it smooth and natural to read. The preliminary survey results showed that all four nurses were able to independently complete the scale rating, indicating an understanding of the meaning of each item. Furthermore, interviews revealed no discrepancies between their interpretation of the items and the intended meaning. Therefore, no modifications were made to the scale content.
General information of the respondents
This study investigated 430 patients who underwent radical prostatectomy, and 426 (99.1%) were effectively recovered. The patients’ ages ranged from 58 to 78 years, with a mean age of 69.9 ± 4.71 years. The Chinese versions of the NMAS-BF and TAS-20 yielded total scores of 4.37 ± 1.06 and 53.59 ± 9.70, respectively. Detailed information is presented in Table 1.
Reliability
The Cronbach’s α coefficient for the Chinese version of the NMAS-BF scale was 0.856. Removing any item did not increase the Cronbach’s α value. The split-half reliability was 0.837, demonstrating that the scale possesses high internal consistency. The retest results from 30 patients, obtained 2 weeks later, showed an intraclass correlation coefficient (ICC) of 0.938 (95% CI: 0.874–0.970), indicating that the scale has good stability and internal consistency (Table 2).
Validity
Content validity
In this study, the mean content validity index (CVI) was 0.83, with individual item assessments by six experts ranging from 0.83 to 1.00. The scale demonstrated strong relevance, representativeness, and comprehensibility. All items effectively reflected the level of alexithymia in patients following radical prostatectomy.
The discrimination validity
The results revealed that the critical ratio values for all items ranged from − 23.94 to -12.69 (P < 0.05), indicating significant differences between the high- and low-score groups for each item. These findings demonstrate good discrimination and representativeness of the items.
Construct validity
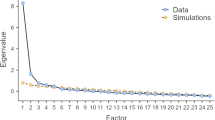
The results of the exploratory factor analysis indicated a Kaiser-Meyer-Olkin (KMO) value of 0.877 and a Bartlett’s test of sphericity χ² value of 486.962 (P < 0.001), confirming the suitability of the data for factor analysis. One factor with an eigenvalue greater than 1 was extracted, and the abrupt rise in the scree plot slope suggested the presence of a single factor (Fig. 1). The analysis confirmed that the scale is unidimensional, with a cumulative variance explained of 58.965%. The factor loadings for items 1 through 6 were 0.679, 0.771, 0.767, 0.775, 0.771, and 0.837, respectively, consistent with the theoretical model of the original scale.

Lithotripsy map of principal component analysis for the Chinese version of NMAS-BF (n = 205).
Confirmatory factor analysis indicated that the model fit indices, χ²/df = 1.371, RMSEA = 0.041, were within acceptable limits, suggesting that the unidimensional scale model fits the data well (Table 3). Figure 2 presents the structural equation model (SEM) and standardized regression coefficients for the one-factor model.

Standardized single factor structural model of the Chinese version of NMAS-BF (n = 221). e1-e6, the errors in measuring each observed variable to estimate latent variables.
Measurement invariance testing
The three models include multi-group measurement invariance fit indices, as shown in Table 4 below. As indicated by the results of the benchmark model tests, the chi-square change and corresponding p-values are all greater than 0.05, with none reaching statistical significance. This suggests that the model demonstrate good structural validity across both groups.
Concurrent validity
The TAS-20 was used as the criterion to assess alexithymia in patients following radical prostatectomy. A strong correlation was observed between the TAS-20 and the NMAS-BF (r = 0.84, P < 0.001). The correlation coefficients between the NMAS-BF items and the total TAS-20 score ranged from 0.55 to 0.70. Item 1 exhibited the weakest correlation with the TAS-20 (r = 0.35, P < 0.01), whereas items 2 and 3 showed the strongest correlations (r = 0.70, P < 0.01 for both).
Influencing factors of alexithymia
The correlations between age, perceived stress, mutuality, social impact, self-esteem and alexithymia were shown in Table 5. Perceived stress and social impact were positively correlated with alexithymia in patients following radical prostatectomy (P < 0.05), while mutuality and self-esteem were negatively correlated with alexithymia (P < 0.05).
Discussion
This study provides a comprehensive account of the adaptation and validation process for the NMAS-BF within a Chinese population. The findings indicate that the NMAS-BF possesses robust psychometric properties.
Reliability reflects the dependability, stability, and consistency of a scale. In this study, the internal consistency of the Chinese version of the NMAS-BF was assessed using Cronbach’s α coefficient and the Guttman split-half coefficient. Among patients post-radical prostatectomy, both coefficients exceeded 0.800, indicating high internal consistency for measuring alexithymia. Notably, the Cronbach’s α coefficient was higher than that of the original scale (0.800)22. Test-retest reliability, evaluated over a two-week interval, was greater than 0.900, demonstrating the scale’s robustness in reliably assessing alexithymia with only six items35. Unlike the original scale, which did not assess stability, this study addressed that gap. Additionally, two trained researchers conducted assessments to ensure good inter-rater reliability. In summary, the Chinese version of the NMAS-BF exhibits excellent reliability.Validity assesses a scale’s effectiveness and accuracy. This study examined the validity of the Chinese version of the NMAS-BF through discriminant, construct, content, and criterion-related validity. Item analysis revealed significant differences between high and low subgroups for all items, confirming effective discrimination. Exploratory factor analysis extracted one common factor with a cumulative variance contribution rate exceeding 50%, and factor loadings ranged from 0.669 to 0.844, surpassing the threshold of 0.439, which indicates strong structural stability. We conducted measurement invariance testing across various demographic groups, and the results indicated that the scale demonstrates strong validity in assessing the NMAS-BF across these groups. Content validity testing yielded a mean CVI of 0.83, demonstrating the scale’s ability to effectively measure alexithymia. The correlation coefficient between the NMAS-BF and TAS-20 was 0.84 (P < 0.001), exceeding the criterion-related validity of the English version (r = 0.49)24. Validation through confirmatory factor analysis showed that fit indices met statistical standards, further supporting the scale’s strong construct validity37.
Demographic factors, including educational level, family residence, household monthly income, and number of children, were found to significantly influence alexithymia among patients after radical prostatectomy. Patients with a primary school education or lower had the lowest alexithymia scores, while those with a secondary or technical school education exhibited the highest scores, contradicting previous studies. Pasini38 reported that individuals with higher education levels tend to exhibit lower alexithymia, while De Vries39 found no association between education and alexithymia in cancer patients. These discrepancies may partly stem from cultural differences within the studied populations. Rural patients had higher alexithymia scores than urban counterparts, potentially due to reduced access to education and professional opportunities, which may limit awareness and support for emotional expression40. Patients with a monthly income below 1,000 yuan showed the lowest scores, while those earning 1,001–3,000 yuan had the highest scores, contrasting with Erdem’s findings, which reported no significant relationship between income and alexithymia41. Regarding family structure, patients with one child had the highest alexithymia scores, whereas those with two children had the lowest. These findings suggest that interventions targeting alexithymia in radical prostatectomy patients should focus on individuals from rural areas, those with only one child, and those with a junior high school or technical school education.
The results showed that perceived stress, and stigma are positively correlated with alexithymia. Patients with higher levels of alexithymia experience greater perceived stress, as individuals with alexithymic traits are more vulnerable to stress, particularly during periods of heightened health-related challenges42. Stigma was also significantly and positively associated with alexithymia, consistent with the findings of Chen43. Among patients undergoing radical prostatectomy, symptoms such as incontinence and erectile dysfunction often regarded as sensitive topics contribute to stigma. Additionally, various researches indicate that self-stigma correlates with social isolation and heightened psychological susceptibility15. The recurrent, persistent, and concealable nature of these symptoms can lead to feelings of shame, which are often internalized and kept private. This reluctance to disclose their condition reinforces a culture of silence, further exacerbating the development of alexithymia. Mutuality and self-esteem are negatively correlated with alexithymia. Mutuality, which refers to the positive relationship between the caregiver and the care recipient, helps patients who receive greater love and emotional support better manage health-related stress25. As self-esteem decreases, alexithymia levels increase, consistent with the findings of Polat44. Individuals with high self-esteem exhibit a positive self-assessment, self-acceptance, and confidence in recognizing and expressing their emotions. These findings suggest that higher levels of perceived stress and stigma, as well as lower mutuality and self-esteem, contribute to increased alexithymia in patients undergoing radical prostatectomy. Therefore, these factors should be prioritized when designing targeted interventions.
Conclusion
The Chinese version of the NMAS-BF comprises six items and a single dimension, preserving the theoretical structure of the original questionnaire. It exhibits robust reliability and validity, making it a scientifically sound tool for assessing alexithymia in patients following radical prostatectomy. Significant factors influencing alexithymia include educational level, family residence, household monthly income, number of children, perceived stress, stigma, mutuality, and self-esteem. Identifying alexithymic patterns and their influencing factors enables healthcare providers to implement targeted interventions, such as psychotherapy, mindfulness practices, or emotion-focused coping strategies, to improve emotional expression and mental well-being.
Limitations
This study has several limitations. First, it employs a cross-sectional design and relies exclusively on self-reported data, which may introduce response bias. Future research could adopt a longitudinal design with repeated measures to analyze trends and changes in alexithymia over time, thereby enhancing our understanding of how alexithymia levels fluctuate as a result of treatment or other influencing variables. Second, the sample is drawn from a single province in China and is limited to patients who underwent prostatectomy, restricting the generalizability of the findings to more diverse populations. Future research should include broader, more diverse samples to enhance the tool’s applicability and support cross-cultural validation. Third, the study did not evaluate the sensitivity and specificity required to establish an appropriate cutoff value for identifying lower levels of alexithymia. Future studies should incorporate larger sample sizes to determine this cutoff value and further validate the scale’s reliability and validity. Additionally, retest data were collected via telephone interviews rather than face-to-face, which may have weakened the robustness of the findings.
Data availability
The original contributions of this study are included in the article and supplementary material. For further inquiries, please contact the corresponding author.
References
Culp, M. B., Soerjomataram, I., Efstathiou, J. A., Bray, F. & Jemal, A. Recent global patterns in prostate Cancer incidence and mortality rates. Eur. Urol. 77, 38–52 (2020).
Hodges, P. W. et al. Reconsideration of pelvic floor muscle training to prevent and treat incontinence after radical prostatectomy. Urol. Oncol. Semin Orig Investig. 38, 354–371 (2020).
Anguas-Gracia, A. et al. Quality of life after radical prostatectomy: a longitudinal study. Nurs. Rep. 13, 1051–1063 (2023).
Mungovan, S. F. et al. Preoperative exercise interventions to optimize continence outcomes following radical prostatectomy. Nat. Rev. Urol. 18, 259–281 (2021).
Okanli, A., Karabulutlu, E. Y., Asi Karakaş, S., Şahin Altun, Ö. & Yildirim, N. Alexithymia and perception of illness in patients with cancer. Eur. J. Cancer Care (Engl). 27, e12839 (2018).
Preece, D. A. et al. Why is alexithymia a risk factor for affective disorder symptoms? The role of emotion regulation. J. Affect. Disord. 296, 337–341 (2022).
Liu, Y., Du, Q. & Jiang, Y. Prevalence of alexithymia in cancer patients: a systematic review and meta-analysis. Support Care Cancer. 31, 675 (2023).
Karakis, E. N. & Levant, R. F. Is Normative Male Alexithymia Associated with relationship satisfaction, fear of Intimacy and Communication Quality among men in relationships? J. Mens Stud. 20, 179–186 (2012).
Porcelli, P., Tulipani, C., Maiello, E., Cilenti, G. & Todarello, O. Alexithymia, coping, and illness behavior correlates of pain experience in cancer patients. Psychooncology 16, 644–650 (2007).
O’Loughlin, J. I., Cox, D. W., Kahn, J. H. & Wu, A. D. Attachment avoidance, alexithymia, and gender: examining their associations with distress disclosure tendencies and event-specific disclosure. J. Couns. Psychol. 65, 65–73 (2018).
Spitzer, C., Brandl, S., Rose, H. J., Nauck, M. & Freyberger, H. J. Gender-specific association of alexithymia and norepinephrine/cortisol ratios. A preliminary report. J. Psychosom. Res. 59, 73–76 (2005).
Kantar, A. & Yalçin, İ. Masculinity and seeking psychological help: a review based on Social Identity Theory. Psikiyatr Güncel Yaklaşımlar. 15, 677–686 (2023).
Imm, K. R. et al. African American prostate cancer survivorship: exploring the role of social support in quality of life after radical prostatectomy. J. Psychosoc Oncol. 35, 409–423 (2017).
Weber, B. A., Roberts, B. L., Mills, T. L., Chumbler, N. R. & Algood, C. B. Physical and emotional predictors of Depression after Radical Prostatectomy. Am. J. Mens Health. 2, 165–171 (2008).
Kantar, A. & Yalçın, İ. Masculine gender role stress and attitudes towards seeking psychological help: serial mediation by Self-Stigma and Self-Compassion. Curr. Psychol. 43, 6114–6124 (2024).
Eymech, O. et al. The impact of radical prostatectomy on the social well-being of prostate cancer survivors: a qualitative meta-synthesis. Eur. J. Cancer Care (Engl). 31, e13630 (2022).
Darabos, K. & Hoyt, M. A. Masculine norms about emotionality and social constraints in young and older adult men with cancer. J. Behav. Med. 40, 259–270 (2017).
Bagby, R. M., Parker, J. D. A. & Taylor, G. J. The twenty-item Toronto Alexithymia scale—I. item selection and cross-validation of the factor structure. J. Psychosom. Res. 38, 23–32 (1994).
Bagby, R. M., Taylor, G. J., Parker, J. D. A. & Dickens, S. E. The development of the Toronto structured interview for Alexithymia: item selection, factor structure, reliability and concurrent validity. Psychother. Psychosom. 75, 25–39 (2006).
Vorst, H. C. M. & Bermond, B. Validity and reliability of the bermond–vorst Alexithymia Questionnaire. Personal Individ Differ. 30, 413–434 (2001).
Levant, R. F. et al. The normative male Alexithymia Scale: measurement of a gender-linked syndrome. Psychol. Men Masculinity. 7, 212–224 (2006).
Levant, R. F. & Parent, M. C. The development and evaluation of a brief form of the normative male alexithymia scale (NMAS-BF). J. Couns. Psychol. 66, 224–233 (2019).
Wang, F. et al. Factor Analysis and psychometric properties Adaption of Chinese Version of the Decisional Engagement Scale (DES-10). Patient Prefer Adherence. 14, 2027–2034 (2020).
Yi, J. Y., Yao, S. Q. & Zhu, X. Z. The Chinese version of the TAS-20: reliability and validity. Chin. Mental Health J. 17, 763–767 (2003).
Archbold, P. G., Stewart, B. J., Greenlick, M. R. & Harvath, T. Mutuality and preparedness as predictors of caregiver role strain. Res. Nurs. Health. 13, 375–384 (1990).
Liu, J. Y. Relationships between Mutuality and Role Strain from Caregiving Activities in Family Caregivers of Patients with Dementia (2006). http://thesis.lib.cgu.edu.tw/thesis/detail/a9185932a1e74e37ddcc72eb87154950/>
Yang, T. Z. & Huang, H. T. An epidemiological study on stress among urban residents in social transition period. Chin. J. Epidemiol. 24, 760–764 (2003).
Pan, A. W., Chung, L., Fife, B. L. & Hsiung, P. C. Evaluation of the psychometrics of the Social Impact Scale: a measure of stigmatization. Int. J. Rehabil Res. 30, 235–238 (2007).
Yang, Y. & Wang, D. F. Retest of the Bidimensional Model of Rosenberg Self-Esteem Scale. Chin. Mental Health J. 21, 603–605 (2007).
Jones, P. S., Lee, J. W., Phillips, L. R., Zhang, X. E. & Jaceldo, K. B. An Adaptation of Brislin???s Translation Model for Cross-cultural Research. Nurs. Res. 50, 300–304 (2001).
Karakasidou, E., Raftopoulou, G., Pezirkianidis, C., Stalikas, A. & Validity Reliability and Factorial Structure of the Self Compassion Scale-Youth Version in the Greek Population. Psychology 12, 536–553 (2021).
Chen, D. D. et al. Cross-cultural adaptation and validation of the caregiver contribution to self-care of chronic illness inventory in China: a cross-sectional study. BMJ Open. 11, e048875 (2021).
Wu, M. L. Questionnaire statistical analysis practice: SPSS operation and application (Chongqing:Chongqing University, 2010).
Wu, M. L. Questionnaire statistical analysis practice: Amos operation and application (Chongqing:Chongqing University, 2010).
Morley, D., Dummett, S., Kelly, L. & Jenkinson, C. Test-retest reliability of the PDQ-Carer. Parkinsonism Relat. Disord. 102, 16–18 (2022).
Tropea, J., Brand, C. A., Lim, W. K., Hepworth, G. & Finch, S. Exploratory and confirmatory factor analysis of the questionnaire on Palliative Care for Advanced Dementia (qPAD) using a large sample of staff from Australian residential aged care homes. Int. J. Older People Nurs. 18, e12505 (2023).
Jackson, D. L., Gillaspy, J. A. & Purc-Stephenson, R. Reporting practices in confirmatory factor analysis: An overview and some recommendations. Psychol. Methods. 14, 6–23 (2009).
Pasini, A., Chiaie, R. D., Seripa, S. & Ciani, N. Alexithymia as related to sex, age, and educational level: Results of the Toronto Alexithymia Scale in 417 normal subjects. Compr. Psychiatry. 33, 42–46 (1992).
De Vries, A. M. M., Forni, V., Voellinger, R. & Stiefel, F. Alexithymia in cancer patients: review of the literature. Psychother. Psychosom. 81 (2), 79–86 (2012).
Faye, A. et al. Assessment of alexithymia and cognition in elderly patients with depression: A cross-sectional exploratory study. J. Geriatr. Ment Health. 9, 100–108 (2022).
Erdem, H. & Eker, E. Examination of the level of alexithymia in adult individuals in terms of different demographic factors. (2020).
Gürsoy, B., Çakaloğullari, N. & Üzer, A. The effect of alexithymic characteristics on perceived stress and health anxiety during the COVID-19 pandemic. Eur. Rev. Med. Pharmacol. Sci. 25, 7127–7134 (2021).
Chen, L., Zhang, B., Wang, J. & Mei, Z. Study of Alexithymia and Stigma in Patients with Inflammatory Bowel Disease. Acad. J. Manag Soc. Sci. 2, 203–206 (2023).
Polat, F., Delibas, L. & Ekren, A. Examining the Relationship Between Alexithymia, Anger, and Self-Esteem in Patients Undergoing Hemodialysis. Arch. Health Sci. Res. 10, 168–174 (2023).
Acknowledgements
We extend our gratitude to all participants who generously contributed their time to support this research endeavor.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors listed on the title page were actively involved in the entire process of designing, planning, and executing the study. Feijie Wang and Lijie Huang: carried out the conception and design of the study, were involved in the statistical analysis and interpretation of data, and in the elaboration of the manuscript. Xiangsheng Zhang, Xiaoli Zhang, Wanning Jie, Xiaoxia-Chang, Yinping-Chu, Lu-Wang, Wenwen-Jia, and Beibei-Zhang helped in the acquisition and interpretation of data, and contributed to the elaboration of the manuscript. Feijie Wang, Lijie Huang, and Xiangsheng Zhang contributed to the elaboration of the protocol of study, helped in the interpretation of data and were responsible for the final drafting and elaboration of the manuscript. All authors have approved the final article. Feijie Wang and Lijie Huang contributed equally to this manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study followed the guidelines established in the Declaration of Helsinki Declaration and obtained approval from the Ethics Committee (2019 Ethics Review No. 74). All participants involved in this study provided informed consent prior to their inclusion. Participants were thoroughly informed about the purpose, procedures, risks, and benefits of the study. They were also informed of their right to withdraw from the study at any time without penalty. Consent was obtained in in written form and in accordance with the ethical guidelines and regulations set forth by Ethics Committee (2019 Ethics Review No. 74). Participation in the study was voluntary and anonymous for all individuals involved.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, F., Zhang, X., Huang, L. et al. Validity and reliability of the brief form of the normative male alexithymia scale among Chinese patients after radical prostatectomy. Sci Rep 15, 719 (2025). https://doi.org/10.1038/s41598-024-82958-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-82958-8
