
Abstract
COVID-19 ranks as one of the major pandemics in recent history, with healthcare workers disproportionately burdened by the disease. Vaccination emerged as the most effective measure to curb the spread and reduce COVID-19 morbidity and mortality. However, vaccine hesitancy presents a challenge to achieving optimal vaccination coverage in Nigeria. This study assessed the level of COVID-19-related stress and anxiety as well as factors associated with vaccine hesitancy among healthcare workers. A descriptive, cross-sectional study was conducted among 849 health workers of a tertiary hospital. Vaccine hesitancy, COVID-19 related stress and anxiety were assessed using the Vaccine Hesitancy Scale (VHS) and SAVE-6 scale respectively. Also, the WHO-5 index was used to assess the perceived mental wellbeing among study participants. Data analysis was conducted using SPSS 25 at univariate, bivariate and multivariate levels. There were slightly more males (479; 56.4%) than females and about four-fifth (674; 79.4%) of respondents were married. About one-quarter of health workers were vaccine hesitant, 236 (27.8%) while 96 (11.3%) had high levels of stress and anxiety. Also, 38 (4.5%) of respondents had poor mental wellbeing. Females when compared to males, had significantly higher odds (OR 1.50; 95% CI 1.10–2.10; p = 0.023) of having vaccine hesitancy while those who were married compared to their single counterparts had significantly lesser odds (OR 0.60; 95% CI 0.36–0.94; p = 0.026). However, there was no significant association between COVID-19 related anxiety and vaccine hesitancy. COVID-19 vaccine hesitancy exists even among health professionals. This study highlights that gender and marital status significantly influence vaccine hesitancy among healthcare workers. Healthcare workers need to receive vaccines to protect themselves and others. Given their role in educating patients and community members about vaccination against infectious diseases like COVID-19, targeted interventions are needed to address hesitancy and optimize vaccine acceptance among healthcare professionals.
Similar content being viewed by others


Introduction
COVID-19 posed a global threat and has continued to evolve in the last few years1,2,3. Newer strains have evolved and the common variants of interest are JN.1 and BA 2.86, which have been reported in many countries as of November 20244. Recently, the World Health Organization (WHO) declared that although the disease could no longer be viewed as a public health emergency, it had become endemic, emphasizing the need to sustain efforts in place to control it4. Despite noticeable reductions in disease morbidity and mortality globally, as of December 2024, there were about 777 million confirmed cases and over seven million deaths worldwide cumulatively since the pandemic began3.
In addressing the threat posed by COVID-19, vaccination remains the most important measure to prevent disease spread and reduce morbidity and mortality5,6,7. However, this measure has not been completely effective due to the problem of vaccine hesitancy8. The WHO defines vaccine hesitancy as the “delay in acceptance or refusal of vaccines despite the availability of vaccination services”9. Due to vaccine hesitancy, vaccination campaigns have not completely been effective, especially in low-and middle-income countries8. Findings from a study carried out among participants from 23 countries showed that 25% of the study population were vaccine-hesitant8. Also, in a scoping review of relevant literature to assess vaccine hesitancy among African countries, a number of studies found a vaccine acceptance rate lower than 50%10. Vaccine hesitancy is driven by misinformation and disinformation about the COVID-19 vaccine, lack of confidence in the institutions providing the vaccine, injection fears, and anxieties about possible side effects, amongst others7,10,11. In addition, studies around the world suggest that sociodemographic factors such as sex, age, income, employment, and perceived risk of being infected with COVID-19 may influence vaccine hesitancy12,13.
Psychological disorders such as anxiety, depression, and phobia were commonly reported in the general population and particularly among healthcare workers during the peak of the COVID-19 pandemic14,15. The disease’s novelty likely caused uncertainty and anxiety, while social restrictions such as lockdowns, social distancing, and quarantine measures disrupted routines and increased stress16. Beyond the pandemic, recent studies in Saudi Arabia and the United Kingdom have also shown significant correlations between vaccine hesitancy and anxiety10,14.
Healthcare workers play crucial roles in health education and more importantly, the administration of vaccines to clients in the hospital. They are expected to be knowledgeable about COVID-19 vaccination strategies and help alleviate misconceptions about the various vaccines. Despite this, some studies have shown that even health workers may sometimes be vaccine hesitant due to anxieties about the COVID-19 vaccine or its side effects14. According to Khubchandani et al., healthcare professionals who are skeptical about COVID-19 vaccination express worries about a lack of knowledge about the vaccine, its effectiveness, and any possible side effects17. During the pandemic, healthcare workers were mostly overworked, with reports of burnout among emergency workers amidst a shortage of personal protective equipment15. This may have contributed to psychological conditions such as undue anxiety and depression that may affect vaccine acceptance15.
While there have been a lot of studies on vaccine hesitancy in the general population and factors that may predispose to it18,19,20, studies are still needed in Nigeria on the relationship between vaccine hesitancy, mental well-being, and COVID-19-related anxiety among healthcare workers. Studies of this nature are important due to the low healthcare worker-to-population ratio and they may provide information on ways to maintain the health and well-being of this critical workforce. Vaccine hesitancy among healthcare workers has wider public health implications for disease control and may hinder the capacity of the country’s healthcare system to effectively meet the needs of the population. Hence this study assessed COVID-19-related stress, anxiety, and possible factors associated with vaccine hesitancy among health workers. The study findings may provide valuable information for policymakers and healthcare providers, helping to ensure a more resilient healthcare workforce and a more effective public health response.
Materials and methods
Study location and population
The research was carried out among 849 hospital staff of the Obafemi Awolowo University Teaching Hospital Complex (OAUTHC), Ile-Ife, Osun State, Nigeria. OAUTHC is a first-generation, tertiary facility that offers specialist medical care to its citizens. It has about 1800 clinical care providers and 800 administrative staff. The first batch of COVID vaccines was imported into Nigeria in March 2021, and vaccination of health workers was prioritized in the first phase of vaccinations.
Study design and sampling
This study utilized a descriptive, cross-sectional design. The sample size was determined using Leslie Fisher’s formula for estimating a single proportion. Sample size calculation for this study is based on 80% power, assuming a type I error of 3.5% and a non-response rate of 10% among respondents. According to a previous study among health workers in the United States of America, 63% were vaccine-hesitant21. Consequently, a sample size of 804 was estimated for this study.
All staff members who reported for COVID-19 vaccination at designated hospital points were pre-screened for eligibility. Hospital staff employed for at least one year with no contraindication to the COVID-19 vaccine were eligible for the study. Only staff in direct contact with patients were recruited using a systematic sampling technique.
Data collection and management
Data collection was done daily at all three vaccination points using a semi-structured questionnaire. Data collection was conducted between July and September 2021. The questionnaire contained four sections as follows: Section A assessed the socio-demographic information of the study participants, while Section B focused on the perceived risk of acquiring COVID-19 and the use of medications as chemoprophylaxis. In Section C, the Vaccine Hesitancy Scale (VHS) and the Stress and Anxiety to Viral Epidemics-6 items scale (SAVE-6) were used to assess vaccine hesitancy, stress, and anxiety among study participants. On the VHS, individuals who scored greater than 50% were deemed to be vaccine-hesitant. The SAVE-6 scale comprises 6 items rated on a five-point Likert scale ranging from 0 (never) to 4 (always). The maximum attainable score is 24, with higher scores reflecting higher levels of stress and anxiety. Individuals who scored above the reference cut-off of 15 were identified as being stressed and anxious. Section D assessed the perceived mental well-being of health workers using the WHO-5 well-being index. The index contains five items on a six-point Likert scale. Individuals who scored lower than the reference cut-off of 13 had poor well-being. The different scales (VHS, SAVE-6, and WHO-5 well-being index) used for this study were adapted from standard questionnaires that have been widely used and validated. The questionnaire was administered in English, and data collection was conducted by trained doctors, including senior registrars and consultants in public health. Before data collection, a two-day training session was held to familiarize the data collectors with the questionnaire and the proper methods for asking questions about the then-novel COVID-19 vaccine.
Data analysis
Data entry and cleaning were done using the Statistical Package for Social Sciences (SPSS) version 25 for analysis at univariate, bivariate and multivariate levels. The sociodemographic characteristics of respondents were summarized using frequency tables and percentages. The chi-square test was used to determine the association between sociodemographic characteristics, anxiety, stress, and well-being, and COVID-19 vaccine hesitancy among respondents. A multivariable binary logistic regression alongside an adjusted odds ratio was also done to identify the predictors of vaccine hesitancy. A p-value of 0.05 was considered statistically significant.
Results
Socio demographic characteristics
Table 1 shows the sociodemographic characteristics of respondents. A total of 849 eligible healthcare workers were sampled, with more than a fourth, 358 (42.2%), being in the age group of 30 to 39 years and more than half, 479 (56.4%), of male gender. Less than half, 389 (45.7%), had a bachelor’s degree and the majority, 674 (79.4%), were married, while 357 (42.0%), were physicians.
Table 2 shows the perceived risk of acquiring COVID-19 and the use of medications for chemoprophylaxis. The majority of health workers, 623 (73.4%), had a perceived elevated risk of contracting COVID, and more than half, 435 (51.2%), were directly involved in managing suspected or confirmed cases. More than two-thirds, 588 (69.3%), had never had a COVID-19 PCR test, while among persons who did the test, 78 (29.9%) had a positive PCR result. The majority, 620 (73.0%), were not currently on chemoprophylaxis for COVID-19 and among those using chemoprophylaxis, the majority, 182 (79.5%), used Ivermectin. Also, the majority, 171 (74.7%), believed that use of these medications was effective in preventing COVID-19.
Table 3 shows findings on vaccine hesitancy, and stress and anxiety. Most health workers, 613 (72.2%), and 753 (88.7%), were not COVID-19 vaccine hesitant nor were prone to stress and anxiety respectively.
The perceived mental wellbeing of health workers is presented in Table 4. Almost all health workers, 811 (95.5%) had good mental wellbeing.
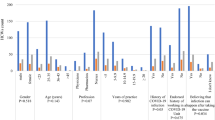
Table 5 shows the association between selected characteristics and COVID-19 vaccine hesitancy. Gender (χ2 = 5.478; p = 0.015), marital status (χ2 = 9.335; p = 0.009) and being directly involved in the care of suspected/confirmed COVID-19 patients (χ2 = 4.657; p = 0.031), were significantly associated with the COVID-19 vaccine hesitancy.
Table 6 shows a multivariable binary logistic regression model which shows the predictors of vaccine hesitancy among selected variables. Females compared to males, had significantly greater odds (OR:1.50; 95% CI: 1.10–2.10; p = 0.023) of being vaccine hesitant while those who were married compared to single persons had significantly lesser odds (OR: 0.60; 95% CI: 0.36–0.94; p = 0.026). However, there was no significant association between COVID-19 related anxiety and vaccine hesitancy.
Discussion
Vaccine hesitancy is a complex and dynamic issue that varies across individuals, contexts, and locations22,23. This study assessed the level of COVID-19-related anxiety and the possible factors associated with vaccine hesitancy among health workers in a tertiary hospital. Less than three out of ten healthcare workers (HCWs) were vaccine-hesitant. This finding is not unexpected given that HCWs play frontline roles in various vaccination campaigns and are key stakeholders in any healthcare program. Since this study was conducted in a hospital setting, most of the healthcare workers may be well-motivated to receive the vaccine, which may have positively influenced the study findings. A systematic review of the literature by Ramonfaur et al. showed that vaccine hesitancy was as low as 5.5% among HCWs22 although some other studies have reported much higher values17,24.
The majority of HCWs had an elevated perceived risk of contracting COVID-19, and more than half were involved in directly managing suspected or confirmed cases. Studies carried out in China, Vietnam, and Pakistan have shown that frontline workers directly involved in the management of COVID-19 cases had an elevated risk perception of getting the disease compared with non-clinical health workers and non-healthcare workers25,26,27. Due to the enormous mental and physical strain associated with managing patients in the hospital who may or may not have COVID-19, frontline health workers are often more prone to elevated risks of getting the disease15.
The use of chemoprophylaxis to prevent COVID-19 has been documented in the literature28,29,30. While our study showed that the majority of health workers were not on any form of chemoprophylaxis, they still believed that it was effective. A similar study among health workers in Nigeria also observed that the majority were not on any form of chemoprophylaxis;28 however, this was not the case among healthcare workers in another study conducted in Jordan31. A few of our respondents used Ivermectin, followed by vitamin C and zinc, to prevent COVID-19. Due to its anti-viral properties, Ivermectin has been proposed as a possible remedy in the management of COVID-1929. The chemoprophylactic roles of herbal remedies, antibiotics and antioxidants have also been studied; however, their use is not encouraged due to the paucity of valid and extensive studies on their effectiveness28,31.
Most of the health workers in our study were not prone to anxiety or stress, and almost all had good mental well-being. This finding is in contrast to research by Zangeneh et al., who documented that health workers in Iran and three European countries recorded high levels of stress and anxiety15. The observed differences may be due to the fact that the majority of health workers in our study were not vaccine-hesitant, as evidenced by their willingness to receive the COVID-19 vaccine. In addition, COVID-19 appeared to have a lesser burden in the study environment, evidenced by lower morbidity and deaths from COVID-19 in many African countries compared to high-income countries.
Gender, marital status, and being directly involved in the care of suspected/confirmed COVID-19 cases were associated with vaccine hesitancy. In the regression model, the females as compared to male health workers were more likely to be vaccine hesitant. While females were vaccine-hesitant in some studies12,22, in others, it was the males that had vaccine hesitancy7,32. Generally, women are often more conscious about their health and that of their family members, although how this translates to vaccine hesitancy has not been fully clarified in literature13. The association between marital status and vaccine hesitancy was also established on multivariate regression analysis, as health workers who were married had significantly lesser odds of vaccine hesitancy. This observation has been reported in studies done in Ghana and Pakistan33,34. Married health workers who may have children and loved ones at home may be more willing to take the vaccine due to fears of the disease affecting other family members.
In this study, the professional cadre of respondents was not significantly associated with vaccine hesitancy. However, this finding did not align with some past studies that indicated that physicians were less likely to be vaccine-hesitant compared to other professional cadres35,36. A possible reason for the observation may be due to the saturation of information regarding COVID-19 and the vaccines around the time of the study across all professional cadres. In addition, hospital staff were among the first to be vaccinated in the country, and they were perceived as reliable sources of information on the disease and vaccine. As a result of this, they were probably well-informed and therefore more accepting of vaccination.
The finding of no association between anxiety and vaccine hesitancy in our study population could be due to the very low numbers of health workers who were vaccine-hesitant or had anxiety. A study carried out by Fadhel et al., among adults in Saudi Arabia observed a significant correlation between anxiety and vaccine hesitancy14. In addition, some other studies have documented that vaccine-hesitant health workers were more likely to have anxiety or other psychological issues37,38. Although our study has found no relationship between vaccine hesitancy and anxiety, it is still important to monitor the psychological well-being of health workers who are expected to play a huge role in safeguarding and promoting the health of others.
Future studies may investigate broader perceptions regarding COVID-19 vaccination and other preventive measures adopted among healthcare workers since these insights are useful learning points for infection prevention and control in the healthcare environment. It is also important to assess broader issues such as the coping strategies employed by healthcare workers in low-resource settings during the peak of the pandemic. Support systems, policies, and interventions may then be better developed to prepare healthcare professionals for future public health emergencies with a greater understanding of how they handled and navigated the psychological and emotional difficulties they faced during the last pandemic.
Conclusion
Vaccine hesitancy exists among healthcare workers and poses a challenge to public health control efforts. This study identified gender and marital status as factors influencing vaccine hesitancy among healthcare professionals. Vaccination of healthcare personnel not only protects their own health but also safeguards patients and the broader community. As influential figures in health communication, healthcare professionals are pivotal in shaping public perceptions and acceptance of vaccination and other disease control measures.
To effectively address vaccine hesitancy among healthcare workers, a blend of approaches that includes training and support is necessary. Targeted training initiatives should provide healthcare professionals with evidence-based information to counteract misinformation and foster confidence in vaccine safety and efficacy. A supportive workplace culture that encourages open discussion of vaccine-related concerns is essential. By equipping healthcare workers with the necessary resources and opportunities to advocate for vaccination, public trust in immunization can be strengthened with the attendant public health benefits. Overcoming vaccine hesitancy among healthcare workers is essential for building resilient health systems capable of addressing future public health emergencies and optimizing public health outcomes.
Although the levels of COVID-19-related stress and anxiety among health workers were low in this study, continuous monitoring of their psychological well-being is still necessary. As front liners during outbreaks, health workers are likely to be more involved in work and become stressed which has mental health consequences. Providing periodic assessments and psychosocial support systems for health workers will help ensure resilience and boost their ability to deliver care effectively, especially in emergency situations and perhaps other future health crises.
Limitations
This study had some limitations. Data was collected from hospital staff who were offered free COVID-19 vaccinations, and concerns about repercussions for declining the vaccine may have introduced some social desirability bias. However, the study’s strengths include a relatively large sample size and robust data collection methods, with assurances of confidentiality that likely enhanced the quality of the data.
Data availability
Datasets supporting the findings of this study are available on request to the corresponding author.
Abbreviations
- CI:
-
Confidence interval
- COVID-19:
-
Corona Virus Disease 2019
- SARS-CoV2:
-
Severe Acute Respiratory Syndrome- Coronavirus 2
- SAVE-6:
-
Stress and Anxiety to Viral Epidemics-6 items scale
- SPSS:
-
Statistical Package for Social Sciences
- VHS:
-
Vaccine Hesitancy Scale
- WHO:
-
World Health Organization
References
Katella, K. 3 Things to know about JN.1, the new Coronavirus Strain. Yale Medicine. https://www.yalemedicine.org/news/jn1-coronavirus-variant-covid#: JN. has been tracking since August (Accessed 11 Jun 2024) (2024).
Harvey, W. T. et al. SARS-CoV-2 variants, spike mutations and immune escape. Nat. Rev. Microbiol. 19, 409–424 (2021).
WHO. WHO Coronavirus (COVID-19) Dashboard. https://covid19.who.int (accessed 3 Dec 2024) (2024).
Sarker, R., Roknuzzaman, A. S. M., Hossain, M. J., Bhuiyan, M. A. & Islam, M. R. The WHO declares COVID-19 is no longer a public health emergency of international concern: benefits, challenges, and necessary precautions to come back to normal life. Int. J. Surg. (Lond. Engl.) 109, 2851–2852 (2023).
Tenforde, M. W. et al. Effectiveness of SARS-CoV-2 mRNA vaccines for preventing Covid-19 hospitalizations in the United States. medRxiv: Preprint Serv. Health Sci. https://doi.org/10.1101/2021.07.08.21259776 (2021).
Maeda, H. et al. Effectiveness of mRNA COVID-19 vaccines against symptomatic SARS-CoV-2 infections during the Delta variant epidemic in Japan: Vaccine Effectiveness Real-time Surveillance for SARS-CoV-2 (VERSUS). medRxiv 1–29 (2022).
Madran, B., Kayi, I., Beser, A. & Ergönül, Ö. Uptake of COVID-19 vaccines among healthcare workers and the effect of nudging interventions: a mixed methods study. Vaccine https://doi.org/10.1016/j.vaccine.2023.06.022 (2023).
Lazarus, J. V. et al. Revisiting COVID-19 vaccine hesitancy around the world using data from 23 countries in 2021. Nat. Commun. 13, 1–14 (2022).
MacDonald, N. E. et al. Vaccine hesitancy: definition, scope and determinants. Vaccine 33, 4161–4164 (2015).
Freeman, D. et al. Injection fears and COVID-19 vaccine hesitancy. Psychol. Med. 53, 1185–1195 (2023).
Masele, J. J., Masele, J. J. & Misinformation COVID-19 vaccine uptake hesitancy among frontline workers in Tanzania: do demographic variables matter ? Misinformation and COVID-19 vaccine uptake hesitancy among frontline workers in. Hum. Vaccines Immunother.https://doi.org/10.1080/21645515.2024.2324527 (2024).
Khubchandani, J. et al. COVID-19 vaccination hesitancy in the United States: a rapid national assessment. J. Community Health 46, 270–277 (2021).
Pires, C. Global predictors of COVID-19 vaccine hesitancy: a systematic review. Vaccines. https://doi.org/10.3390/vaccines10081349 (2022).
Fadhel, F. H., Sufyan, N. S., Alqahtani, M. M. J. & Almaamari, A. A. Anxiety and fear of COVID-19 as potential mechanisms to explain vaccine hesitancy among adults. Front. Psychiatry 1–10 (2024).
Zangeneh Soroush, M. et al. Effects of COVID-19-related psychological distress and anxiety on quality of sleep and life in healthcare workers in Iran and three European countries. Front. Public. Health. https://doi.org/10.3389/fpubh.2022.997626 (2022).
Shahnawaz, M. G. et al. Individual and group level risk factors in preventive health and panic buying behaviors during COVID-19 pandemic in India. Curr. Psychol. 42, 19641–19657 (2023).
Khubchandani, J., Bustos, E., Chowdhury, S., Biswas, N. & Keller, T. COVID-19 vaccine refusal among nurses worldwide: review of trends and predictors. Vaccines. https://doi.org/10.3390/vaccines10020230 (2022).
Uzochukwu, I. C. et al. COVID-19 vaccine hesitancy among staff and students in a Nigerian tertiary educational institution. Ther. Adv. Infect. Dis. 8, 20499361211054923 (2021).
Amuzie, C. I. et al. COVID-19 vaccine hesitancy among healthcare workers and its socio-demographic determinants in Abia State, Southeastern Nigeria: a cross-sectional study. Pan Afr. Med. J. https://doi.org/10.11604/pamj.2021.40.10.29816 (2021).
Ojo, T. O., Ojo, A. O., Ojo, O. E., Akinwalere, B. O. & Akinwumi, A. F. Determinants of COVID-19 vaccine uptake among nigerians: evidence from a cross-sectional national survey. Arch. Public. Health 81, 95 (2023).
Kwok, K. O. et al. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: a survey. Int. J. Nurs. Stud. 114, 103854 (2021).
Ramonfaur, D. et al. COVID-19 vaccine hesitancy prevalence in Mexico: a systematic review and metanalysis. Vaccine 18, 18–20 (2024).
Orangi, S. et al. A qualitative inquiry on drivers of COVID-19 vaccine hesitancy among adults in Kenya. PLoS Glob. Public. Health 1–22 (2024).
Ackah, B. B. B. et al. COVID – 19 vaccine hesitancy in Africa: a scoping review. Glob. Health Res. Policy 1, 1–20 (2022).
Lam, S. C. et al. Perceived risk and Protection from infection and depressive symptoms among Healthcare workers in Mainland China and Hong Kong during COVID-19. Front. Psychiatry 11, 1–7 (2020).
Abid, A. et al. Perceived risk and distress related to COVID-19 in healthcare versus non-healthcare workers of Pakistan: a cross-sectional study. Hum. Resour. Health 20, 1–13 (2022).
Le, X. T. T. et al. Perception toward exposure risk of COVID-19 among Health workers in Vietnam: Status and correlated factors. Front. Public. Health 9, 1–10 (2021).
Udoette, S. B., Onukak, A. E., Umoh, V. A. & Akpabio, A. A. The practice of using repurposed medications as chemoprophylaxis for COVID-19 by healthcare workers in a tertiary hospital in Southern Nigeria. Afr. Health Sci. 23, 406–411 (2023).
Shoumann, W. M. et al. Use of Ivermectin as a potential Chemoprophylaxis for COVID-19 in Egypt: a Randomised Clinical Trial. J. Clin. Diagn. Res. 27–32 (2021).
Azeez, T. A. et al. Chemoprophylaxis against COVID–19 among health–care workers using ivermectin in low– and middle–income countries: a systematic review and meta–analysis. Indian J. Pharmacol. 49, 344–347 (2018).
Bulatova, N. et al. Use of traditional and complementary medicine for COVID 19 prophylaxis among healthcare professionals and students in Jordan: a cross-sectional study. PLoS ONE 17, 1–20 (2022).
Ndasauka, Y., Twabi, H. S., Kainja, J., Gunde, A. M. & Mtimuni, C. M. Knowledge, attitudes and demographic drivers for COVID – 19 vaccine hesitancy in Malawi. Sci. Rep. 1–12 (2024).
Zakar, R. et al. COVID-19 Vaccination Hesitancy or Acceptance and its Associated factors: findings from Post-vaccination cross-sectional survey from Punjab Pakistan. Int. J. Environ. Res. Public Health. https://doi.org/10.3390/ijerph19031305 (2022).
Alhassan, R. K. et al. COVID-19 vaccine hesitancy among the adult population in Ghana: evidence from a pre-vaccination rollout survey. Trop. Med. Health. https://doi.org/10.1186/s41182-021-00357-5 (2021).
Leigh, J. P. et al. Factors affecting COVID-19 vaccine hesitancy among healthcare providers in 23 countries. Vaccine 40, 4081–4089 (2022).
Gagneux-Brunon, A. et al. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: a cross-sectional survey. J. Hosp. Infect. 108, 168–173 (2021).
Di Prinzio, R. R. et al. The impact of vaccine hesitancy on psychological impairment among healthcare workers in a total Worker Health© approach. Front. Public. Health. https://doi.org/10.3389/fpubh.2024.1447334 (2024).
Akbulut, S. et al. Evaluation of vaccine hesitancy and anxiety levels among hospital cleaning staff and caregivers during COVID-19 pandemic. Vaccines (Basel) 10, 1426 (2022).
Acknowledgements
The authors are grateful to staff of the Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife for their cooperation during data collection for the study.The first author is supported by the Consortium for Advanced Research Training in Africa (CARTA) which is funded by the Carnegie Corporation of New York (Grant No--B 8606.R02), SIDA (Grant No:54100029) and the Developing Excellence in Leadership, Training and Science in Africa (DELTAS Africa) Initiative (Grant No: 107768/Z/15/Z). The views expressed in this publication are those of the authors and not necessarily those of the partners in the consortium.
Funding
details.
This research work was self-sponsored as authors received no specific grant or any funding support from agencies in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
T.O.O contributed to the study conceptualization, methodology, analysis and partly drafted the initial manuscript (introduction, methods and results). TAA, OF, OE, OII and TOO contributed to the study methodology, data collection and management and first draft of manuscript. SCE and BOA contributed to the data management, analysis, discussion and revised the first draft of the manuscript. SAO, OTA, and AAO contributed to the study conceptualization and revised the first draft of the manuscript. All authors reviewed and approved the final draft of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Ethical approval to conduct this study was obtained from the Ethics and Research Committee of the Obafemi Awolowo University Teaching Hospitals Complex (OAUTHC) with Approval number: ERC/2021/08/06. All respondents gave voluntary informed consent after being informed of the study’s risks and benefits. No personal identifying information was recorded and respondents’ data were carefully uploaded on a passworded computer reserved for the study while being assured of the confidentiality of the information provided. The study complied with the Declaration of Helsinki on conducting research among human subjects.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ojo, T.O., Adetunji, T.A., Eneh, S.C. et al. COVID-19-related stress, anxiety and vaccine hesitancy among healthcare workers in a tertiary hospital in South-Western Nigeria. Sci Rep 15, 4112 (2025). https://doi.org/10.1038/s41598-024-84195-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-84195-5
