
Abstract
The relationship between bicarbonate level and mortality in critically sick patients with infective endocarditis (IE) is currently not well established. The MIMIC-IV database was used to provide data for a retrospective cohort research. Included were patients with IE who were hospitalized to the critical care unit (ICU). Within the first 24 h following ICU admission, the serum bicarbonate was assessed. The 28-day mortality was the end-point result. To evaluate the relationship between the serum bicarbonate and 28-day mortality, multivariable Cox regression was employed. The study included 450 patients with IE in serious condition in the ICU, with a 57.4-year-old average and 64.2% male representation. The 28-day mortality rate stood at 20%. Unadjusted analysis revealed that higher serum bicarbonate levels upon ICU admission were significantly linked to reduced 28-day mortality (hazard ratio [HR], 0.90; 95% confidence interval [CI], 0.85–0.95; p < 0.001). This correlation remained significant after adjusting for potential confounding factors (adjusted HR, 0.94; 95% CI 0.89–0.99; p = 0.028). When categorizing bicarbonate levels, patients in the highest group (T3, ≥ 25 mEq/L) showed a significantly decreased adjusted HR of 0.55 (95% CI 0.33–0.93; p < 0.001) in relation to the control group (T1, ≤ 22 mEq/L) in the final model. Consistent results were observed in subgroup analyses across various groups. In patients with IE in the ICU, elevated serum bicarbonate upon admission was independently linked to a lower 28-day mortality. These findings indicate that serum bicarbonate can serve as a prognostic marker, supporting the process of risk assessment and providing direction for the clinical care of patients with IE.
Similar content being viewed by others

Introduction
Infective endocarditis (IE), typically caused by bacterial or fungal infections of the inner lining of the heart chambers and heart valves, can lead to serious complications such as heart damage, stroke, and organ failure1. Symptoms may include fever, chills, fatigue, weakness, and changes in heart rhythm. Treatment usually involves a combination of antibiotics and, in some cases, surgery to repair or replace damaged heart valves. The incidence of IE is 3–10 per 100,000 people2,3,4. Despite advancements in diagnostic tools and therapeutic measures, the in-hospital mortality rate due to IE remains at approximately 25%5, leading to a high economic burden with average hospitalization costs ranging from $37,000 to $55,000 per patient6. The prognosis of patients with infective endocarditis is often influenced by multiple factors, including the severity of the infection and the timeliness of early diagnosis and treatment. Various factors, including individual patient characteristics, cardiac and non-cardiac comorbidities, infecting microbial species, and echocardiographic disease status, contribute to the poor prognosis of IE4,7. Early diagnosis is critical to improving patient outcomes and reducing mortality associated with IE8. However, research on risk factors for infective endocarditis is limited, presenting a challenge. In clinical practice, it is crucial to identify reliable risk factors to assess disease progression and prognosis, which can guide treatment decisions.
Bicarbonate measurements are widely recognized as a valuable clinical biomarker for evaluating acid–base balance9,10. Previous research has shown that serum bicarbonate levels are a significant factor correlated with prognosis in sepsis11, stroke12,13, diabetes14,15, hypertension16, heart failure17, and chronic kidney disease (CKD)patients18,19. Nonetheless, the relationship between serum bicarbonate levels and overall clinical results in patients with IE remains unclear. The purpose of this study was to assess the correlation between the serum bicarbonate levels at admission and the 28-day mortality for patients with IE in the ICU. We hypothesized that serum bicarbonate levels are linked to 28-day mortality in patients in serious condition with IE.
Methods
Database
This study utilized the version 2.2 database of the Medical Information Mart for Intensive Care IV (MIMIC-IV) (https://mimic.mit.edu/), which comprises data from 73,181 critically sick individuals’ hospital stays at Boston’s Beth Israel Deaconess Medical Center from 2008 to 201920. Numerous factors are included in the database, including vital signs, diagnosis, treatment plans, test findings, and survival status. Due to its extensive and superior-quality data, the MIMIC database has become increasingly popular among researchers for conducting studies21,22,23. After successfully completing an online course and test, Yingxiu Huang (Certificate ID: 56,513,391) and Ting Ao (Certificate ID: 58,844,105) were granted access to the database. Given the anonymized nature of the database, obtaining informed consent was waived. This cohort analysis strictly followed the protocols outlined in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations24.
We performed a retrospective cohort examination, leveraging data from MIMIC-IV v2.2. The study encompassed all individuals with infective endocarditis (IE) who were initially admitted to the intensive care unit (ICU). The key result we focused on was the 28-day mortality rate.
Study population
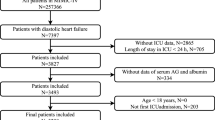
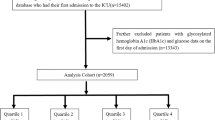
Patients admitted to the ICU with infective endocarditis (IE) from 2008 to 2019 were included in our study. The diagnosis was ascertained based on the criteria from the International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) (code = 03,642, 07,422, 0932X, 09,884, 11,281, 11,504, 11,514, 11,594, 3911, 421X, 4249X, A3282, A3951, A5203, B3321, B376, I011, I38, I33,I39, M3211). In the case of patients with IE who had multiple ICU admissions, only their initial admission was considered for inclusion in the study. The analysis was confined to individuals whose serum electrolytes were assessed within the first 24 h following their ICU admission, which facilitated the determination of their bicarbonate levels (Fig. 1).

The flow chart of the study.
Exposure
The study’s primary outcome variable was the serum bicarbonate level, evaluated as a continuous variable. It was also divided into three tertile groups based on admission values from the MIMIC-IV database: T1 (≤ 22 mEq/L), T2 (23–24 mEq/L), T3 (≥ 25 mEq/L). Baseline serum bicarbonate concentration was determined by the initial measurement taken within 24 h of admission to the ICU.
Covariates
Data pertaining to patients was extracted from the MIMIC-IV database utilizing Structured Query Language (SQL) and was then stored in a PostgreSQL database for further analysis. This dataset encompassed various demographics including age, sex, and race, as well as comorbid conditions such as renal disease, sepsis, diabetes, congestive heart failure, acute kidney injury within 2 day of ICU admission, and shock. Intervention measures were also recorded, including continuous renal replacement therapy (CRRT), and surgery. Additionally, the dataset included the left ventricular ejection fraction (LVEF), sequential organ failure assessment (SOFA) score, Charlson Comorbidity Index (CCI), result of blood culture, and laboratory measurements from the initial day of ICU stay, such as serum bicarbonate, anion gap, pH, glucose, blood urea nitrogen (BUN), hemoglobin, white blood cell count, and platelet count. Illness severity was evaluated using the CCI. For variables with missing data rates below 50%, we utilized the K-Nearest Neighbors (KNN) imputation method25.
Statistical analysis
Patient characteristics were summarized using descriptive statistics. Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range [IQR]), while categorical variables were shown as counts and percentages. To assess the baseline characteristics, we used the Mann–Whitney U test to evaluate the differences in continuous variables, while the chi-square test was applied to analyze categorical variables across the groups.
Multiple Cox regression models were employed to evaluate the correlation between serum bicarbonate levels and the risk of 28-day mortality. An extended Cox proportional hazards model was utilized to incorporate time-varying covariates into the analysis. Model 1 was crude model without adjustment. Model 2 included adjustments for race, sex and age. Model 3 incorporated adjustments for age, sex, race, diabetes, sepsis, LVEF, CCI, and surgical intervention to refine the analysis. Curve fitting methods were utilized to explore the relationship between serum bicarbonate and the probability of 28-day death. Additionally, Kaplan–Meier curves were constructed to depict survival differences among patient groups categorized by bicarbonate tertiles.
All analyses were performed using R version 4.2.2, which can be accessed from The R Foundation at http://www.R-project.org, and the Free Statistics software, version 1.9.2, available at http://www.clinicalscientists.cn/freestatistics. A two-tailed p-value of less than 0.05 was used as the threshold for statistical significance26.
Results
Baseline characteristics of patients
This study included an overall of 450 critically ill patients with IE. Baseline bicarbonate levels were categorized into three groups based on tertiles: T1 (≤ 22 mEq/L), T2 (23–24 mEq/L), and T3 (≥ 25 mEq/L) (see Table 1). The average age of the cohort was 57.4 years, with 64.2% being male. Among the 450 patients, 360 survived (survival group) and 90 did not (non-survival group), resulting in an overall 28-day mortality rate of 20%. Individuals in the non-survival cohort exhibited reduced serum bicarbonate concentrations, with an average of 22.7 ± 5.4 mEq/L, in contrast to those in the survival cohort, who demonstrated higher levels at 24.4 ± 3.8 mEq/L. Additionally, the non-survival group exhibited higher prevalence of comorbid conditions such as chronic renal disease, acute kidney injury and sepsis.
Association of serum bicarbonate with mortality
Within the multivariable Cox hazard regression analysis, (Table 2), higher bicarbonate levels at admission were significantly associated with reduced 28-day mortality in the model 1 without adjustment (HR, 0.90; 95% confidence interval [CI], 0.85–0.95; p < 0.001). 28-day mortality decreased by 10 per cent per mEq/L increase in bicarbonate in model 1 (HR, 0.90; 95% CI 0.85–0.95; p < 0.001). This correlation remained significant even after accounting for variables such as age, gender, race, comorbid conditions (diabetes, and sepsis), the CCI, LVEF, and treatment variables (surgery) (model 3 adjusted HR, 0.94; 95% CI 0.89–0.99; p = 0.028). When the analysis categorized bicarbonate levels, the adjusted hazard ratios for bicarbonate levels in T2 (23–24 mEq/L) and T3 (≥ 25 mEq/L) compared to the lowest group (T1, bicarbonate ≤ 22 mEq/L) were 0.54(95% CI 0.31–0.91, p = 0.027) and 0.55 (95% CI 0.33–0.93, p = 0.02) respectively, in the final model. Significantly, the general trend demonstrated a statistical significance (p < 0.05), as ascertained by the trend test (Table 2).
The analysis of curve fitting uncovered a “L-shaped” of non-linear correlation between serum bicarbonate and the rate of mortality within a 28-day period (p for non-linearity = 0.004, Fig. 2). Through the integration of graphical analysis and clinical significance, we identified the optimal inflection point for bicarbonate levels to be 27 mEq/L. In patients with serum bicarbonate levels below this threshold, each 1 mEq/L increase in bicarbonate is associated with a 14% reduction in the risk of mortality (HR, 95% CI: 0.86 [0.79–0.94]; p < 0.001). However, this relationship does not hold true for bicarbonate levels at or above 27 mEq/L (HR, 95% CI 1.13 [0.93–1.37]; p = 0.223), as indicated in Table 3.

The non-linear relationship between serum bicarbonate levels and the risk of 28-day mortality was analyzed, with adjustment for age, sex, race, diabetes, sepsis, CCI, surgery, LVEF, and SOFA score. Only 99% of the data is displayed.
Kaplan–Meier survival curve analysis
The Kaplan–Meier curves for the three groups are illustrated in Fig. 3. These curves reveal that the survival probabilities within 28 days were notably reduced in the lowest tertile (T1) compared to the highest tertile (T3) (log-rank test, p < 0.0001) (Fig. 3).

Kaplan–Meier survival curves for critically ill patients with IE based on serum bicarbonate.
Subgroup analysis
Subgroup analysis indicated consistent results various subgroups based on sex, age, race, diabetes, congestive heart failure, CCI, sepsis, and shock (Fig. 4). The interaction analysis showed an interaction between the congestive heart failure and age (< 65 years and ≥ 65 years) (Fig. 4).

Subgroup analyses for the association of serum bicarbonate with 28-day mortality in the patients with IE. Each stratification factor was adjusted for age, sex, race, diabetes, sepsis, CCI, surgery, and LVEF.
Discussion
This research highlights the correlation between blood bicarbonate concentrations and the risk of death within a 28-day period in ICU patients suffering from IE. Our analysis revealed that, even after adjusting for other variables, bicarbonate levels were inversely related to 28-day mortality. Based on our understanding, this research marks a pioneering effort in exploring the relationship between serum bicarbonate levels and mortality in IE.
Bicarbonate plays a crucial role in maintaining the body’s acid–base balance, and disturbances in this balance are closely associated with outcomes in critically ill patients4,12,27. Prior research indicates that diminished serum bicarbonate concentrations correlate with heightened mortality rates among patients with stroke 12,13, acute aortic dissection27, diabetes15,28, chronic kidney disease19. Patients in the lowest tertile of serum bicarbonate were facing an elevated mortality risk. Our findings are consistent with these studies, highlighting an independent association between serum bicarbonate levels and mortality.
We hypothesize that the elevated mortality observed in critically ill patients with IE with low bicarbonate levels may be attributed to several factors. Low bicarbonate levels often signify metabolic acidosis or an increased risk of it29. Metabolic acidosis can exacerbate endothelial cell dysfunction and has a spectrum of adverse impacts on bodily functions. It may impair myocardial contractility, increase the risk of cardiac arrhythmias, decrease vascular tone, diminish the body’s sensitivity to stress hormones and trigger constriction of the pulmonary blood vessels30. Additionally, metabolic acidosis may impair the immune system and impede the activity of white blood cells, thereby increasing the susceptibility to infections among patients31. These findings highlight the significance of closely monitoring bicarbonate levels in patients with IE and indicate that healthcare providers should contemplate specialized interventions for individuals exhibiting decreased bicarbonate levels.
This research possesses numerous advantages. Firstly, it boasts a considerable sample size, leveraging data from the MIMIC-IV database, a comprehensive and high-quality real-world dataset. Secondly, the robustness of the findings is supported by subgroup analyses, which reinforce the reliability of the results. However, this research encounters certain constraints. Firstly, being a retrospective analysis, it is potentially prone to selection bias. Secondly, data on bicarbonate were only available for patients admitted to the ICU, limiting our ability to evaluate how fluctuations in bicarbonate after ICU stay might impact death rates, potentially affecting the accuracy of our results. Thirdly, while our study focuses on the association between bicarbonate levels and 28-day mortality, we acknowledge that variability in treatment approaches can affect patient outcomes. In future studies, we will explore this aspect in greater depth. Lastly, being an observational study, we were unable to validate the proposed mechanisms linking bicarbonate levels to the degree of seriousness and the likely outcome of IE.
Conclusion
Upon admission, elevated serum bicarbonate levels were significantly and independently linked to a reduction in the risk of mortality within a 28-day for critically ill patients afflicted with IE. These findings indicate that measure of serum bicarbonate may support the process of risk assessment and providing direction for the clinical care of patients with IE.
Data availability
Data in the article can be obtained from mimic-IV database (https://mimic.physionet.org/). The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Cahill, T. J. & Prendergast, B. D. Infective endocarditis. Lancet 387, 882–893. https://doi.org/10.1016/S0140-6736(15)00067-7 (2016).
Malakan Rad, E. et al. Infective endocarditis in North Africa and the middle east, 1990–2019: Updates from the global burden of disease study 2019. Arch. Iran. Med. 27, 229–238 (2024).
Ambrosioni, J. et al. Hospital Clinic Infective Endocarditis Investigators, The changing epidemiology of infective endocarditis in the twenty-first century. Curr. Infect. Dis. Rep. 19, 21. https://doi.org/10.1007/s11908-017-0574-9 (2017).
Che, D., Hu, J., Zhu, J., Lyu, J. & Zhang, X. Development and validation of a nomogram for predicting in-hospital mortality in ICU patients with infective endocarditis. BMC Med. Inform. Decis. Mak. 24, 84. https://doi.org/10.1186/s12911-024-02482-7 (2024).
Chen, H. et al. The global, regional, and national burden and trends of infective endocarditis from 1990 to 2019: Results from the global burden of disease study 2019. Front. Med. 9, 774224. https://doi.org/10.3389/fmed.2022.774224 (2022).
Alkhouli, M., Alqahtani, F., Alhajji, M., Berzingi, C. O. & Sohail, M. R. Clinical and economic burden of hospitalizations for infective endocarditis in the United States. Mayo Clin. Proc. 95, 858–866. https://doi.org/10.1016/j.mayocp.2019.08.023 (2020).
Habib, G. et al. 2015 ESC guidelines for the management of infective endocarditis. Kardiol. Pol. 73, 963–1027 (2015).
Baumgartner, H. et al. ESC/EACTS guidelines for the management of valvular heart disease. Eur. Heart J. 38(2017), 2739–2791. https://doi.org/10.1093/eurheartj/ehx391 (2017).
Spears, R. C. et al. Alterations in local peri-infarct blood gases in stroke patients undergoing thrombectomy. World Neurosurg. 158, e317–e322. https://doi.org/10.1016/j.wneu.2021.10.171 (2022).
Wang, T. et al. Risk potential for organ dysfunction associated with sodium bicarbonate therapy in critically ill patients with hemodynamic worsening. Front. Med. 8, 665907. https://doi.org/10.3389/fmed.2021.665907 (2021).
Paudel, R., Bissell, B., Dogra, P., Morris, P. E. & Chaaban, S. Serum bicarbonate: Reconsidering the importance of a neglected biomarker in predicting clinical outcomes in sepsis. Cureus 14, e24012. https://doi.org/10.7759/cureus.24012 (2022).
Du, W., Yang, J., Lou, Y., You, J. & Wang, Q. Relationship between baseline bicarbonate and 30-day mortality in patients with non-traumatic subarachnoid hemorrhage. Front. Neurol. 14, 1310327. https://doi.org/10.3389/fneur.2023.1310327 (2023).
Huang, X. & Zhang, Y. Relationship between serum bicarbonate levels and the risk of death within 30 days in ICU patients with acute ischemic stroke. Front. Neurol. 14, 1125359. https://doi.org/10.3389/fneur.2023.1125359 (2023).
Chubb, S. A. P., Davis, W. A. & Davis, T. M. E. Serum bicarbonate concentration and the risk of death in type 2 diabetes: The fremantle diabetes study phase II. Acta Diabetol. 60, 1333–1342. https://doi.org/10.1007/s00592-023-02130-y (2023).
Li, Y., Gao, R., Zhao, B. & Zhang, Y. Low serum bicarbonate levels increase the risk of all-cause, cardiovascular disease, and cancer mortality in type 2 diabetes. J. Clin. Endocrinol. Metab. 107, 3055–3065. https://doi.org/10.1210/clinem/dgac504 (2022).
Dobre, M. et al. SPRINT Research Group, Serum bicarbonate and cardiovascular events in hypertensive adults: Results from the systolic blood pressure intervention trial. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 35, 1377–1384. https://doi.org/10.1093/ndt/gfz149 (2020).
Kendrick, J. B. et al. Serum bicarbonate is associated with heart failure in the multi-ethnic study of atherosclerosis. Am. J. Nephrol. 45, 118–126. https://doi.org/10.1159/000454783 (2017).
Chang, K. Y. et al. The impact of high serum bicarbonate levels on mortality in hemodialysis patients. Korean J. Intern. Med. 32, 109–116. https://doi.org/10.3904/kjim.2015.168 (2017).
Fukasawa, H., Kaneko, M., Uchiyama, Y., Yasuda, H. & Furuya, R. Lower bicarbonate level is associated with CKD progression and all-cause mortality: A propensity score matching analysis. Bmc Nephrol. 23, 86. https://doi.org/10.1186/s12882-022-02712-y (2022).
Johnson, A. E. W. et al. MIMIC-III, a freely accessible critical care database. Sci. Data 3, 160035. https://doi.org/10.1038/sdata.2016.35 (2016).
Hu, Y., Zhao, Y., Zhang, J. & Li, C. The association between triglyceride glucose-body mass index and all-cause mortality in critically ill patients with atrial fibrillation: A retrospective study from MIMIC-IV database. Cardiovasc. Diabetol. 23, 64 (2024).
Wang, H., Gao, C., Dantona, C., Hull, B. & Sun, J. DRG-LLaMA : Tuning LLaMA model to predict diagnosis-related group for hospitalized patients. NPJ Digit. Med. 7, 16. https://doi.org/10.1038/s41746-023-00989-3 (2024).
Liu, K. et al. Association between the ROX index and mortality in patients with acute hypoxemic respiratory failure: A retrospective cohort study. Respir. Res. 25, 143. https://doi.org/10.1186/s12931-024-02771-9 (2024).
Field, N. et al. Strengthening the reporting of molecular epidemiology for infectious diseases (STROME-ID): An extension of the STROBE statement. Lancet Infect. Dis. 14, 341–352. https://doi.org/10.1016/S1473-3099(13)70324-4 (2014).
El-Menyar, A., Naduvilekandy, M., Asim, M., Rizoli, S. & Al-Thani, H. Machine learning models predict triage levels, massive transfusion protocol activation, and mortality in trauma utilizing patients hemodynamics on admission. Comput. Biol. Med. 179, 108880. https://doi.org/10.1016/j.compbiomed.2024.108880 (2024).
Gou, E. et al. Association between albumin-bilirubin score and in-hospital mortality in patients with sepsis: Evidence from two large databases. Heliyon 10, e34697. https://doi.org/10.1016/j.heliyon.2024.e34697 (2024).
Tan, L., Xu, Q., Li, C., Chen, X. & Bai, H. Association between the admission serum bicarbonate and short-term and long-term mortality in acute aortic dissection patients admitted to the intensive care unit. Int. J. Gen. Med. 14, 4183–4195. https://doi.org/10.2147/IJGM.S321581 (2021).
Paul Chubb, S. A., Davis, W. A., Peters, K. E. & Davis, T. M. E. Serum bicarbonate concentration and the risk of cardiovascular disease and death in type 2 diabetes: The fremantle diabetes study. Cardiovasc. Diabetol. 15, 143. https://doi.org/10.1186/s12933-016-0462-x (2016).
Wang, Y., Chen, L., Guo, G., Gao, Y. & Gan, H. Effect of sodium bicarbonate infusion on hospital mortality in acute kidney injury patients with metabolic acidosis. Front. Med. 10, 1268252. https://doi.org/10.3389/fmed.2023.1268252 (2023).
Dong, L. et al. Acidosis activation of the proton-sensing GPR4 receptor stimulates vascular endothelial cell inflammatory responses revealed by transcriptome analysis. PLoS One 8, e61991. https://doi.org/10.1371/journal.pone.0061991 (2013).
Crimi, E. et al. Effects of intracellular acidosis on endothelial function: An overview. J. Crit. Care 27, 108–118. https://doi.org/10.1016/j.jcrc.2011.06.001 (2012).
Acknowledgements
The authors thanks Dr. Qilin Yang of Department of Critical Care, The Second Affiliated Hospital of Guangzhou Medical University for guidance on data extraction and analysis.
Author information
Authors and Affiliations
Contributions
Yingxiu Huang: Designed the protocol, write the manuscript. Ting Ao: Extracted, collected and analyzed data. Peng Zhen: Prepared tables and figures. Ming Hu: Designed the protocol, write the manuscript, reviewed and edit the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
Two of the authors, Yingxiu Huang and Ting Ao, were given access to the database following successful completion of an online course and test (Certificate ID: 56513391, Yingxiu Huang, Certificate ID: 58844105 Ting Ao). MIMIC-IV database used in the present study was approved by the Institutional Review Boards (IRB) of Institutional Review Boards of Beth Israel Deaconess Medical Center(2001-P-001699/14) and the Massachusetts Institute of Technology (No. 0403000206) both approved the use of the database for research. We have also complied with all relevant ethical regulations regarding the use of the data for our study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Huang, Y., Ao, T., Zhen, P. et al. Association between serum bicarbonate and 28-day mortality in critically ill patients with infective endocarditis: a cohort study from MIMIC-IV. Sci Rep 15, 312 (2025). https://doi.org/10.1038/s41598-024-84385-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-84385-1
