
Abstract
Sepsis-associated encephalopathy (SAE) represents a severe neurological complication in sepsis, characterized by high mortality and cognitive impairment. Although clinical significance, SAE lacks effective diagnostic and prognostic tools. This study evaluates the predictive value of neuron-specific enolase (NSE) and regional cerebral oxygen saturation variability (rSO₂%) as indicators for diagnosing and prognosing SAE. A prospective observational study enrolled 70 sepsis patients, classified into SAE and non-SAE groups. Serum NSE levels and rSO₂% were measured alongside clinical data and 28-day mortality outcomes. NSE and rSO₂% were identified as independent indicators of SAE (P < 0.05). Combined analysis achieved a higher diagnostic accuracy, with an area under the ROC curve of 0.749, compared to single indicators. Kaplan-Meier survival analysis reveals that elevated NSE levels and increased rSO₂% are associated with significantly reduced 28-day survival (P < 0.001). These findings suggest that NSE and rSO₂%are valuable indicators for the diagnosis and prognosticating SAE. Their combined application significantly improves diagnostic efficacy, providing a basis for personalized early intervention strategies.
Similar content being viewed by others

Introduction
Sepsis is a systemic inflammatory response to infection that may progress to multiple organ dysfunction syndrome (MODS) in severe cases. Despite significant progress in early identification and treatment, the global incidence and mortality rates of sepsis remain alarmingly high1. According to The Lancet, there were approximately 49 million cases of sepsis globally in 2017, resulting in 11 million deaths—accounting for 19.7% of all global deaths2. While significant progress has been made in modern medicine, the challenges of high mortality and long-term complications associated with sepsis persist.Sepsis-associated encephalopathy (SAE)is one of the most prevalent neurological complications in sepsis patients, occurring in 50–70% of cases and is strongly associated with high mortality, long-term cognitive impairment, and diminished quality of life3,4. The precise mechanisms underlying SAE remain unclear, likely involving impaired cerebral perfusion, inflammation, oxidative stress, and neuronal injury. However, the nonspecific symptoms, combined with a lack of sensitive and specific diagnostic tools and effective early risk assessment methods, present a significant challenge in the clinical management of SAE5,6,7,8,9. Recent research on indicators provides new directions for the early identification and monitoring of SAE. Among these, neuron-specific enolase (NSE) and regional cerebral oxygen saturation (rSO₂) have garnered particular attention10,11.
Regional cerebral oxygen saturation (rSO₂), measured using near-infrared spectroscopy (NIRS), serves as a key physiological indicator of the oxygen supply-demand balance in brain tissue. It has shown significant application value in the study of SAE and is widely utilized in critical care monitoring12. Research indicates that a decrease in rSO₂ in sepsis patients is closely associated with cerebral hypoxia, providing a crucial reference for the early identification of SAE13. Furthermore, rSO₂ serves as an effective perfusion assessment tool; its reduction may reflect low perfusion states in shock, guiding intervention strategies14. When combined with central venous oxygen saturation (ScvO₂) and lactate levels, rSO₂ significantly enhances the ability to predict disease severity in sepsis patients, particularly in assessing cerebral dysfunction15. Although the sensitivity of rSO₂ alone is limited, its integration with other neurological monitoring techniques, such as somatosensory evoked potentials (SEP), can improve diagnostic accuracy for SAE-related neurological complications and contribute to better patient outcomes16.
Neuron-specific enolase (NSE), a specific biomarker of neuronal injury, plays a critical role in the diagnosis and prognostic assessmets of SAE17,18.Studies suggest that NSE is not only valuable for diagnosing acute brain injuries but also serves as a predictor of neuronal damage in sepsis patients, with a strong correlation to mortality and delirium19. Therefore, NSE, as a monitoring indicator, offers potential clinical value for the early diagnosis and precise treatment of SAE.
Although previous studies have explored the monitoring value of rSO₂ and NSE in critically ill patients, their application in SAE and combined predictive capability remain unclear. Therefore, this study aims to investigate the association of rSO₂ and NSE with SAE in patients with sepsis and evaluate their potential value in the diagnosis and prognosis of SAE.
Results
Study population
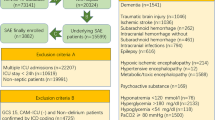
A total of 111 sepsis patients were evaluated, of whom 36 did not meet inclusion criteria, 2 declined participation, and 3 had incomplete data. Ultimately, 70 patients met the eligibility criteria and were successfully enrolled (Fig. 1).

Study flow diagram. A total of 111 patients with septic shock were screened, of whom 41 met various exclusion criteria. Ultimately, 70 patients were included in our study, with 31 (44%) classified in the SAE group and 39 (56%) in the non-SAE group.
Clinical characteristics and outcomes
The study cohort comprised 70 sepsis patients, including 31 in the SAE group and 39 in the non-SAE group. No significant differences were observed between the two groups in terms of age, sex distribution, or infection sources (P > 0.05). However, the SAE group exhibited significantly higher APACHE II and SOFA scores compared to the non-SAE group (P < 0.05). Additionally, ICU length of stay and 28-day mortality were significantly elevated in the SAE group (P < 0.05). No statistically significant differences were identified between the two groups regarding maximum norepinephrine dosage, white blood cell count, hemoglobin levels, platelet count, electrolyte levels, or lactate levels (P > 0.05) (Table 1).
Differences in NSE and rSO₂
Serum neuron-specific enolase (NSE) levels were significantly higher in the SAE group compared to the non-SAE group (P = 0.005). Although no significant differences were observed between the two groups in terms of minimum, maximum, or mean rSO₂ values (P > 0.05), the rSO₂% variability was significantly greater in the SAE group (P = 0.003) (Table 2; Fig. 2).

Comparison of NSE and rSO2% Levels Between SAE and Non-SAE Groups: A Box Plot Analysis.
Multivariable logistic regression analysis for predicting SAE
Multivariable logistic regression analysis identified both NSE and rSO₂% as independent predictors of SAE.The regression coefficient for NSE was 0.058 (SE = 0.028, Wald χ² = 4.389, P = 0.036), with an odds ratio (OR) of 1.060 (95% CI: 1.004–1.120). Similarly, the regression coefficient for rSO₂% was 0.126 (SE = 0.063, Wald χ² = 4.051, P = 0.044), corresponding to an OR of 1.135 (95% CI: 1.003–1.283) (Table 3).
Diagnostic performance of NSE and rSO₂%
Receiver operating characteristic (ROC) curve analysis demonstrates the independent diagnostic utility of NSE and rSO₂% for SAE. The AUC for NSE is 0.658 (95% CI: 0.519–0.796), with an optimal cutoff value of 21.85 ng/mL, yielding a sensitivity of 64.5% and specificity of 76.9%. For rSO₂%, the AUC was 0.695 (95% CI: 0.568–0.821), with an optimal cutoff value of 12.205%, achieving a sensitivity of 64.5% and specificity of 71.8%. When NSE and rSO₂% are combined, the AUC increased to 0.749 (95% CI: 0.633–0.866), with a sensistivity of 71.8% and specificity of 74.2% (Table 4; Fig. 3).

Receiver Operating Characteristic (ROC) curves for the diagnostic performance of NSE and rSO₂% in predicting SAE.
Association of rSO₂% and NSE levels with survival
Kaplan-Meier survival analysis reveals that patients with higher rSO₂% (> 12.205%) and elevated NSE levels (> 21.85 ng/mL) exhibit significantly lower 28-day survival rates compared to those with lower values (P < 0.001) (Fig. 4).

Kaplan-Meier survival curves showing overall survival probability stratified by rSO₂% and NSE thresholds.
Discussion
Sepsis-associated encephalopathy (SAE) is a frequent and severe complication of sepsis, characterized by disturbances in consciousness, cognitive dysfunction, and poor clinical outcomes20,21. Although the precise pathophysiological mechanisms remain unclear, multiple studies have shown that cerebral microcirculatory dysfunction, increased blood-brain barrier permeability, neuroinflammation, oxidative stress, and neuronal injury all contribute to SAE pathogenesis22. For instance, the systemic inflammatory response induced by sepsis can impair cerebral vascular endothelial function and reduce microvascular perfusion, leading to cerebral hypoxia and energy metabolism disruptions, ultimately causing neuronal damage23,24. Moreover, large amounts of inflammatory mediators (e.g., TNF‐α, IL‐1β, IL‐6) further compromise the blood‐brain barrier and exacerbate central nervous system inflammation25,26. Excessive activation of microglial and astrocyte cells releases reactive oxygen species and various inflammatory factors, disrupting synaptic transmission and significantly worsening cognitive function and consciousness27,28. Meanwhile, oxidative stress can intensify neuronal injury via lipid peroxidation, protein oxidation, and DNA damage, thus accelerating the clinical progression of SAE29.Given these complex pathophysiological processes, the present study identified and verified the pivotal value of neuron-specific enolase (NSE) and cerebral oxygen saturation variability (rSO₂%) in the diagnosis and prognosis of SAE. When analyzed in combination, these biomarkers demonstrated markedly enhanced diagnostic performance, achieving an area under the receiver operating characteristic (ROC) curve (AUC) of 0.749 and improved sensitivity and specificity. Furthermore, Kaplan‐Meier survival analysis revealed a significant association between both NSE and rSO₂% and 28‐day mortality, indicating their potential utility as reliable short‐term prognostic indicators. In summary, this study not only highlights a promising multi‐biomarker strategy for early SAE identification and risk stratification but also paves the way for developing multi‐parameter diagnostic models that may advance clinical practice and future research.
Patients in the SAE group exhibited significantly higher Physiology and Chronic Health Evaluation II (APACHE II) score and Sequential Organ Failure Assessment (SOFA) score than the non-SAE group, emphasizing a strong association between disease severity and SAE incidence, consistent with previous findings. For example, studies by Stubbs et al. and Rudd et al. demonstrated that elevated APACHE II and SOFA scores not only reflect the severity of systemic inflammatory responses but also indicate an increased risk of central nervous system dysfunction2,21. Furthermore, SAE patients in this study experienced prolonged ICU stays and significantly higher 28-day mortality rates. These findings are in line with those of Gofton et al., who reported higher mortality rates and an elevated risk of long-term neurological dysfunction in patients with SAE30,31.
This study underscores the diagnostic significance of NSE and rSO₂% in SAE. Serum NSE levels and rSO₂% were significantly elevated in SAE patients compared to non-SAE controls (P = 0.005 and P = 0.003, respectively), highlighting their clinical relevance. NSE, a well-established biomarker of neuronal injury, is strongly associated with neuroinflammation and cerebral dysfunction. This finding aligns with Nguyen et al.‘s research, which demonstrated NSE’s ability to stratify brain injury severity in severe sepsis17. Furthermore, Weigand et al. identified NSE as a robust predictor of adverse neurological outcomes, and our study further substantiates its independent prognostic value in SAE32.In contrast, the dynamic variability of rSO₂% provides a more nuanced reflection of cerebral oxygen supply-demand imbalances compared to absolute values. Ehler et al. demonstrated a significant link between cerebral oxygen fluctuations and impaired perfusion, supporting variability monitoring as a pivotal tool for assessing SAE risk33. Consistently, our results show that rSO₂% not only effectively distinguishes SAE patients but also highlights the role of dynamic cerebral perfusion variability in SAE pathophysiology, offering fresh insights into its potential clinical applications.
This study identifies NSE and rSO₂% as independent predictors of SAE through multivariable logistic regression (P = 0.036 and P = 0.044, respectively), emphasizing their value in early SAE diagnosis. The independent predictive role of NSE aligns with previous studies. For instance, Hsu et al. highlighted NSE as a critical biomarker of neuronal injury in pediatric septic encephalopathy, significantly linked to severe pathological states34. Guo et al. further associated cerebral oxygen dynamics with perfusion imbalance and upregulated inflammatory factors, supporting the predictive utility of rSO₂%35. Combining NSE and rSO₂% improved diagnostic sensitivity and specificity, echoing Barichello et al.‘s findings on the advantages of multidimensional biomarker approaches in complex pathologies35. Mechanistically, these results support the roles of neuroinflammation and cerebral oxygen metabolism imbalance in SAE, as literature points to the synergistic effects of neuronal injury and hypoperfusion as key pathological drivers2,33. NSE and rSO₂% levels offers novel insights into SAE pathogenesis and provides a foundation for personalized therapeutic strategies.
In this study, receiver operating characteristic (ROC) analysis showed that both neuron-specific enolase (NSE) and variability in regional cerebral oxygen saturation (rSO₂%) have value in diagnosing sepsis-associated encephalopathy (SAE), with areas under the curve (AUC) of 0.658 and 0.695, respectively. When analyzed together, their combined AUC rose significantly to 0.729, yielding a sensitivity of 71.8% and a specificity of 74.2%, thus highlighting the advantages of multi-biomarker testing for diagnostic efficiency and accuracy. Nguyen et al. discovered that elevated NSE levels correlate with the severity of sepsis-induced brain injury17, while Anderson et al. indicated that higher NSE levels may increase the risk of mortality and delirium18. This study adopted a cutoff of 21.85 ng/mL for NSE, which, though slightly different from the 24.15 ng/mL reported by Yao et al.36. and the 27.02 ng/mL proposed by Zhang et al.37., remains broadly consistent overall, further supporting the diagnostic value of elevated NSE in SAE. Meanwhile, rSO₂%, an important measure of the balance between cerebral oxygen supply and demand, also shows promise for SAE evaluation. Qian et al. reported that regional cerebral oxygen saturation (rScO₂) demonstrates good predictive value for SAE (AUC = 0.77)10.Sun et al. emphasized that combining rScO₂ and NSE can improve prediction of neurological outcomes after cardiac arrest38, and Zhang et al. found that multi-dimensional biomarker testing significantly boosts diagnostic performance37. Although there is no standardized cutoff for rSO₂%, a study has shown that patients with SAE or delirium typically have lower rSO₂ levels than those without neurological dysfunction, suggesting that insufficient cerebral oxygen supply may be closely related to SAE onset39. The rSO₂% variability threshold of 12.205% employed in this study, while not universally reported in the literature, generally aligns with existing findings and serves as a useful reference. Taken together, this study enriches the evidence for using NSE and rSO₂% in diagnosing and assessing the prognosis of SAE, and offers new insights into SAE pathophysiology from the perspective of neuroinflammation and abnormal cerebral oxygen regulation.
Kaplan-Meier survival analysis reveals that patients with higher rSO₂% or NSE levels exhibit significantly lower 28-day survival rates (P < 0.001). Elevated rSO₂% likely reflects severe cerebral oxygen imbalance and metabolic dysfunction, consistent with Li et al., who emphasized maintaining adequate cerebral oxygenation to reduce sepsis mortality40. Similarly, NSE’s prognostic value aligns with studies by Guo et al., who linked elevated NSE to delirium and long-term neurological dysfunction in sepsis41. Combining rSO₂% and NSE further extends previous findings on the significance of oxygen metabolism monitoring and neuronal injury markers in SAE. This multi-biomarker approach significantly enhances predictive accuracy, consistent with Mewes et al.’s findings on the value of multidimensional analyses in improving survival predictions42. The interplay between cerebral perfusion and neuroinflammation, as revealed by changes in rSO₂% and NSE, offers deeper insights into the pathophysiology of SAE, paving the way for personalized diagnostic and therapeutic strategies while laying the groundwork for exploring the link between brain injury and oxygen metabolism dysregulation.
The findings of this study suggest that NSE and rSO₂%—as indicators of neuronal injury and cerebral oxygenation status—hold potential value for the early identification and risk assessment of SAE. In clinical practice, serum NSE measurement may be incorporated into routine evaluation after ICU admission in septic patients, serving as an early marker of neurological impairment. Meanwhile, rSO₂% can be continuously monitored at the bedside using near-infrared spectroscopy (NIRS), providing real-time insights into cerebral perfusion and oxygen supply.When elevated NSE levels or significant fluctuations in rSO₂% are detected, clinicians should be alerted to the possibility of developing SAE and consider timely interventions. These may include adjusting sedation strategies, optimizing hemodynamic management, and initiating additional neurological monitoring (e.g., EEG or neuroimaging) as needed. Such multimodal approaches may help mitigate secondary brain injury and improve neurological outcomes. In terms of cost-effectiveness, monitoring NSE and rSO₂% offers advantages such as being non-invasive, repeatable, and suitable for bedside application. Compared to high-cost, equipment-dependent methods like MRI, EEG, or invasive intracranial monitoring, these biomarker-based tests are more practical and economical in critical care settings such as the ICU, making them effective tools for early screening and risk stratification of SAE.
This study has several limitations: 1) it was conducted at a single center, which may limit generalizability due to regional biases.2) Despite a larger sample size, it remains relatively small, potentially affecting statistical power. 3) The focus was on NSE and rSO₂% without exploring their correlation with disease severity scores like APACHE II and SOFA, limiting independent predictive evaluation. 4) rSO₂% was measured at specific points, not reflecting dynamic changes, and NSE may be influenced by non-neurological factors. 5) The study only assessed 28-day survival, without examining long-term recovery, quality of life, or microcirculatory changes in other organs. 6) SAE diagnosis relying on CAM - ICU and RASS may be affected by subjective assessment bias despite evaluator training 7) Common confounding factors were included, but specific treatments and comorbidities may not be fully controlled, affecting study results. Despite these limitations, the study offers valuable insights into NSE and rSO₂% for SAE diagnosis and prognosis, guiding future studies. Compared with traditional tools such as EEG, CT/MRI, and S100B, the combined use of NSE and rSO₂% offers advantages in diagnostic accuracy, cost-effectiveness, and bedside applicability, making it a promising and practical supplement for SAE evaluation in the ICU.
Conclusion
This study systematically evaluates the significant advantages of NSE and rSO₂% in the early diagnosis and prognostic assessment of SAE, demonstrating their correlation with short-term survival. Their combined application notably enhanced the diagnostic efficiency of SAE, highlighting the clinical importance of multi-indicators analysis. These findings offer new perspectives for future research and establish a foundation for the application of precision medicine in the management of SAE. Despite limitations such as a small sample size, single-center design, and restricted dynamic monitoring periods, this study provides direction for future multicenter, large-scale prospective studies and offers a scientific basis for optimizing personalized diagnostic and therapeutic strategies for SAE.
Materials and methods
Study Design. This single-center, prospective, observational study was conducted in the Intensive Care Unit (ICU) of the Fourth Hospital of Hebei Medical University, from October 2023 to October 2024. The study protocol was approved by the Ethics Committee of the Fourth Hospital of Hebei Medical University (Approval No: 2020YK351) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the legal representatives of all participants.
Study Population. Patients diagnosed with sepsis according to the Sepsis-3 criteria were enrolled and classified into two groups based on the presence or absence of SAE. Inclusion criteria were as follows included: age ≥ 18 years, continuous monitoring of rSO₂, and NSE testing. The exclusion criteria were as follows: A history of craniotomy or psychiatric disorders, neurological diseases (e.g., intracranial infections, stroke, traumatic brain injury, subarachnoid hemorrhage, intracerebral hemorrhage), other systemic or metabolic factors causing altered mental status (e.g., severe hyperglycemia [blood glucose > 300 mg/dL] or hypoglycemia [blood glucose < 50 mg/dL], significant electrolyte disturbances [serum sodium < 125 mmol/L or > 160 mmol/L], severe hepatic failure, hepatic encephalopathy, severe uremia, intoxication, or drug-induced consciousness disorders), lung cancer, significant missing or incomplete data(), and scalp injuries interfering with near-infrared spectroscopy (NIRS) electrode placement were strictly excluded.
Diagnosis and Assessment of Sepsis-Associated Encephalopathy (SAE).All ICU-admitted sepsis patients were evaluated for SAE from the first day of admission through day 7. Mental status was assessed twice daily (7:00–8:00 AM and 2:00–8:00 PM) using the Confusion Assessment Method for the ICU (CAM-ICU), administered by two trained researchers. A positive result in both assessments confirmed the diagnosis of SAE43. For sedated patients, the Richmond Agitation-Sedation Scale (RASS) was used in combination with the daily Spontaneous Awakening Trial (SAT)44. If the RASS score was inconsistent with the target sedation level (≥ 2 points) or if the patient failed to awaken within 24 h, SAE was suspected45. Based on this diagnosis, patients were divided into the SAE and non-SAE groups(Figure 5).

Diagnostic Flowchart for SAE.
Data collection
Demographic and clinical characteristics Basic demographic information, including age, sex, and sepsis-related clinical parameters, were recorded. These parameters included the Acute Physiology and Chronic Health Evaluation II (APACHE II) score, Sequential Organ Failure Assessment (SOFA) score, maximum norepinephrine dosage, and the number of organ failures.
Regional cerebral oxygen saturation (rSO₂) parameters rSO₂ was monitored using near-infrared spectroscopy (NIRS, model ECO-N17-C22L), with sensors placed bilaterally on the frontal lobes. After the patients were admitted to the ICU, rSO₂ was continuously monitored for at least 24 h, with the device automatically recording rSO₂ values every two seconds and generating a data log. Following this 24-hour period, the minimum (rSO₂min) and maximum (rSO₂max) values were extracted from the log, and both the average rSO₂ and rSO₂ variability were calculated. The rSO₂ variability (rSO₂%) was calculated using the following formula: rSO2% = (rSO2max − rSO2min)/rSO2max*100.
Biochemical indicators Blood samples were collected upon enrollment for measurement of white blood cell count (WBC), hemoglobin (Hb), platelet count (PLT), sodium (Na), potassium (K), lactate (Lac), and NSE levels.
Outcome measures Primary outcomes included 28-day mortality. Secondary outcomes included ICU length of stay, hospital length of stay, and duration of mechanical ventilation (MV).
Statistical analysis
Missing data were addressed using multiple imputation to ensure dataset completeness. Statistical analyses were performed using R software (version 4.2.0), with a two-tailed significance level set at P < 0.05. Continuous variables were summarized as mean ± standard deviation (SD) or median (interquartile range, IQR), depending on data distribution, and compared using the t-test or Mann-Whitney U test, as appropriate. Categorical variables were expressed as frequencies and percentages, with comparisons made using the Chi-square test or Fisher’s exact test. To identify risk factors for septic-associated encephalopathy (SAE), univariate logistic regression analysis was first performed. Variables with a P-value less than 0.20 were included in the multivariate logistic regression model, with adjustments made for potential confounding factors. The results of the logistic regression analysis are presented as odds ratios (OR) with 95% confidence intervals (CI).The predictive performance of significant variables was evaluated using receiver operating characteristic (ROC) curve analysis, with the area under the curve (AUC), optimal cutoff values, sensitivity, and specificity reported. Kaplan-Meier survival analysis was employed to assess the impact of NSE levels and rSO₂% variability on 28-day survival outcomes, with survival curve differences tested using the Log-rank test. Data visualization was carried out using R software and its associated packages.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Singer, M. et al. The third international consensus definitions for Sepsis and septic shock (Sepsis-3). JAMA-J Am. Med. Assoc. 315, 801–810 (2016).
Rudd, K. E. et al. Global, regional, and National sepsis incidence and mortality, 1990–2017: analysis for the global burden of disease study. Lancet 395, 200–211 (2020).
Lu, X. et al. CLINICAL PHENOTYPES OF SEPSIS-ASSOCIATED ENCEPHALOPATHY: A RETROSPECTIVE COHORT STUDY. Shock 59, 583–590 (2023).
Sonneville, R. et al. The spectrum of sepsis-associated encephalopathy: a clinical perspective. Crit. Care. 27, 386 (2023).
Manabe, T. & Heneka, M. T. Cerebral dysfunctions caused by sepsis during ageing. Nat. Rev. Immunol. 22, 444–458 (2022).
Tsuruta, R. & Oda, Y. A clinical perspective of sepsis-associated delirium. J. Intensive Care. 4, 18 (2016).
Souza-Dantas, V. C., Póvoa, P., Bozza, F., Soares, M. & Salluh, J. Preventive strategies and potential therapeutic interventions for delirium in sepsis. Hosp. Pract. (1995). 44, 190–202 (2016).
Hughes, C. G., Patel, M. B. & Pandharipande, P. P. Pathophysiology of acute brain dysfunction: what’s the cause of all this confusion? Curr. Opin. Crit. Care. 18, 518–526 (2012).
Sonneville, R. et al. Potentially modifiable factors contributing to sepsis-associated encephalopathy. Intensive Care Med. 43, 1075–1084 (2017).
Qian, Y., Li, J., Dong, D. & Gu, Q. Clinical study on the predictive value of regional cerebral oxygen saturation for the occurrence of sepsis-associated encephalopathy. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 34, 412–415 (2022).
Cao, Z. G., Huang, X. & Chen, F. X. Diagnostic values of glial fibrillary acidic protein, neuron-specific enolase and protein S100β for sepsis-associated encephalopathy. Revista Romana De Med. De Laborator. 31, 107–112 (2023).
Irani, F., Platek, S. M., Bunce, S., Ruocco, A. C. & Chute, D. Functional near infrared spectroscopy (fNIRS): an emerging neuroimaging technology with important applications for the study of brain disorders. Clin. Neuropsychol. 21, 9–37 (2007).
Fischer, G. W. Recent advances in application of cerebral oximetry in adult cardiovascular surgery. Semin Cardiothorac. Vasc Anesth. 12, 60–69 (2008).
Das, B. P., Sharma, M., Bansal, S., Philip, M. & Rao, G. S. U. Prognostic value of tissue oxygen monitoring and regional cerebral oxygen saturation monitoring and their correlation in neurological patients with sepsis: A preliminary, prospective, observational study. J. Neurosurg. Anesthesiol. 32, 77–81 (2020).
Al Tayar, A., Abouelela, A. & Mohiuddeen, K. Can the cerebral regional oxygen saturation be a perfusion parameter in shock? J. Crit. Care. 38, 164–167 (2017).
Oki, A., Ohtake, H., Okada, Y., Kawada, T. & Takaba, T. Simultaneous monitoring of somatosensory evoked potentials and regional cerebral oxygen saturation combined with serial measurement of plasma levels of cerebral specific proteins for the early diagnosis of postoperative brain damage in cardiovascular surgery. J. Artif. Organs: Official J. Japanese Soc. Artif. Organs. 7, 13–18 (2004).
Nguyen, D. N. et al. Elevated serum levels of S-1000 protein and neuron-specific enolase are associated with brain injury in patients with severe sepsis and septic shock. Crit. Care Med. 34, 1967–1974 (2006).
Anderson, B. J. et al. Admission plasma levels of the neuronal injury marker neuron-specific enolase are associated with mortality and delirium in sepsis. J. Crit. Care. 36, 18–23 (2016).
Zhang, L. T. et al. The value of NSE to predict ICU mortality in patients with septic shock: A prospective observational study. Med. (Baltim). 101, 6 (2022).
Gofton, T. E. & Young, G. B. Sepsis-associated encephalopathy. Nat. Rev. Neurol. 8, 557–566 (2012).
Stubbs, D. J., Yamamoto, A. K. & Menon, D. K. Imaging in sepsis-associated encephalopathy-insights and opportunities. Nat. Rev. Neurol. 9, 551–561 (2013).
Mazeraud, A. et al. Septic-Associated encephalopathy: a comprehensive review. Neurotherapeutics 17, 392–403 (2020).
Crippa, I. A. et al. Impaired cerebral autoregulation is associated with brain dysfunction in patients with sepsis. Crit. Care. 22, 327 (2018).
Brown, L. S. et al. Pericytes and neurovascular function in the healthy and diseased brain. Front. Cell. Neurosci. 13, 282 (2019).
Guo, F. et al. GEF-H1-RhoA signaling pathway mediates LPS-induced NF-κB transactivation and IL-8 synthesis in endothelial cells. Mol. Immunol. 50, 98–107 (2012).
Weighardt, H. & Holzmann, B. Role of Toll-like receptor responses for sepsis pathogenesis. Immunobiology 212, 715–722 (2007).
Chung, H. Y. et al. Microglia mediate neurocognitive deficits by eliminating C1q-tagged synapses in sepsis-associated encephalopathy. Sci. Adv. 9, eabq7806 (2023).
Shulyatnikova, T. & Verkhratsky, A. Astroglia in Sepsis associated encephalopathy. Neurochem Res. 45, 83–99 (2020).
Griton, M. et al. Experimental sepsis-associated encephalopathy is accompanied by altered cerebral blood perfusion and water diffusion and related to changes in cyclooxygenase-2 expression and glial cell morphology but not to blood-brain barrier breakdown. Brain Behav. Immun. 83, 200–213 (2020).
Zhang, L. N. et al. Epidemiological features and risk factors of sepsis-associated encephalopathy in intensive care unit patients: 2008–2011. Chin. Med. J. (Engl). 125, 828–831 (2012).
Feng, Q. et al. Characterization of Sepsis and Sepsis-Associated encephalopathy. J. Intensive Care Med. 34, 938–945 (2019).
Weigand, M. A. et al. Neuron-specific enolase as a marker of fatal outcome in patients with severe sepsis or septic shock. Anesthesiology 92, 905–907 (2000).
Ehler, J. et al. Diagnostic value of NT-proCNP compared to NSE and S100B in cerebrospinal fluid and plasma of patients with sepsis-associated encephalopathy. Neurosci. Lett. 692, 167–173 (2019).
Hsu, A. A. et al. Neurological injury markers in children with septic shock. Pediatr. Crit. Care Med. 9, 245–251 (2008).
Barichello, T., Generoso, J. S., Singer, M. & Dal-Pizzol, F. Biomarkers for sepsis: more than just fever and leukocytosis-a narrative review. Crit. Care. 26, 31 (2022).
Yao, B., Zhang, L. N., Ai, Y. H., Liu, Z. Y. & Huang, L. Serum S100β is a better biomarker than neuron-specific enolase for sepsis-associated encephalopathy and determining its prognosis: a prospective and observational study. Neurochem Res. 39, 1263–1269 (2014).
Zhang, L. N. et al. Diagnostic and predictive levels of Calcium-binding protein A8 and tumor necrosis factor Receptor-associated factor 6 in Sepsis-associated encephalopathy: A prospective observational study. Chin. Med. J. (Engl). 129, 1674–1681 (2016).
Sun, H. et al. [Changes of regional saturation of cerebral oxygenation and neuron specific enolase in patients after cardiopulmonary resuscitation]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 33, 1094–1098 (2021).
Wood, M. et al. Brain tissue oxygenation in patients with septic shock: a feasibility study. Can. J. Neurol. Sci. 43, 65–73 (2016).
Li, Y. et al. Conservative oxygen therapy in critically ill and perioperative period of patients with sepsis-associated encephalopathy. Front. Immunol. 13, 10 (2022).
Guo, W., Li, Y. H. & Li, Q. Relationship between miR-29a levels in the peripheral blood and sepsis-related encephalopathy. Am. J. Translational Res. 13, 7715–7722 (2021).
Mewes, C. et al. CTLA-4 genetic variants predict survival in patients with Sepsis. J. Clin. Med. 8, 14 (2019).
Ely, E. W. et al. Evaluation of delirium in critically ill patients: validation of the confusion assessment method for the intensive care unit (CAM-ICU). Crit. Care Med. 29, 1370–1379 (2001).
Sessler, C. N. et al. The Richmond Agitation-Sedation scale: validity and reliability in adult intensive care unit patients. Am. J. Respir Crit. Care Med. 166, 1338–1344 (2002).
Girard, T. D. et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and breathing controlled trial): a randomised controlled trial. Lancet 371, 126–134 (2008).
Acknowledgements
We are thankful to the participants for their participation. We also acknowledge the dedicated research professionals who contributed to the intervention and assessment of the participants in this study.
Author information
Authors and Affiliations
Contributions
Q.Z. and Y.H. conceptualized and designed the study. X.Z. Y.L. and L.Z. conducted the experiments and collected data, with Y.H. L.L. and Y. X. performing data analysis and validation. Q.Z. drafted the manuscript, and Z.H. revised it critically while supervising the project and providing resources. All authors reviewed and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from Ethics Committee of the Fourth Hospital of Hebei Medical University(Approval No: 2020YK351). Written informed consent was obtained from all participants before their inclusion in the study.
Funding
Funding Declaration: 20230158 Improvement of the diagnosis and treatment process of sepsis patients based on big data analysis, Medical Science Research Project of Hebei.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, Q., Zhang, X., Li, Y. et al. Combined cerebral oxygen saturation and neuron-specific enolase evaluation for diagnosis and prognosis of sepsis-associated encephalopathy. Sci Rep 15, 15369 (2025). https://doi.org/10.1038/s41598-025-00353-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-00353-3
