
Abstract
This study employed network analysis to investigate the complex relationship between emotion regulation strategies and depression, with particular focus on digital burnout as a contemporary stressor and the moderating role of various psychological protective factors. Based on a large sample of 9400 Chinese participants, we constructed a psychological network model incorporating depression, digital burnout, psychological resilience, self-compassion, emotion suppression, mindfulness, and sleep quality using EBIC-GLASSO regularization technique. Results revealed emotion suppression as the most central node in the network, demonstrating the highest betweenness (2.268), closeness (1.302), and strength (1.157) centrality. The network exhibited significant positive connections between emotion suppression and depression (0.890), as well as between emotion suppression and digital burnout (0.848). Notable negative associations were observed between sleep quality and depression (− 0.780), and between resilience and digital burnout (− 0.665). Network stability analysis yielded CS-coefficients exceeding 0.75 for all centrality measures, substantially above the recommended threshold of 0.5, confirming the reliability of our findings. Community detection analysis identified two distinct clusters: a Risk Factor Community (depression, digital burnout, emotion suppression) and a Protective Factor Community (resilience, self-compassion, mindfulness). The average predictability of nodes was 39.5%, ranging from 23.8% for cognitive reappraisal to 74.4% for depression. The innovation of this research lies in being the first to integrate digital burnout into a depression network, revealing its significant role as a connecting variable. Our findings suggest that interventions targeting emotion regulation may be particularly effective; digital wellness initiatives might produce cascading benefits for mental health; and comprehensive interventions simultaneously addressing resilience, self-compassion, and mindfulness may be more effective than those focusing on single protective factors. These findings provide novel insights into understanding depression in the digital age and offer important implications for both clinical practice and public health policy.
Similar content being viewed by others

Introduction
Human behavior is inherently complex by nature, and its understanding and analysis requires increasingly sophisticated psychological models that transcend linear, static, and unicausal perspectives. It is well established that human behavior does not conform well to linear and unilateral explanations. Mental health and emotional well-being, as fundamental aspects of human experience, require approaches that are open to different and novel ways of analyzing, understanding, and intervening upon mental health problems1,2. This study aims to examine the relationship between emotion regulation strategies and depression within the context of digital burnout, with a focus on how protective psychological factors may buffer these relationships. Depression represents a particularly compelling case for network analysis, given its complex etiology and the multiple pathways through which it develops and maintains itself. Recent global estimates indicate that approximately 280 million people worldwide suffer from depression, with rates increasing dramatically in recent years3,4. The societal burden is substantial, with depression ranking as a leading cause of disability worldwide and contributing significantly to the global burden of disease.
The emergence of digital-age stressors has added new layers of complexity to our understanding of depression. Digital burnout, characterized by emotional and psychological fatigue resulting from excessive technology use, has become increasingly prevalent, particularly in the wake of global digitalization trends. Recent studies suggest that digital burnout affects between 20–30% of adults in developed nations, with higher rates among younger populations5. In China specifically, recent surveys indicate that digital burnout affects approximately 25–35% of urban professionals, with rates among university students reaching up to 40% in major metropolitan areas6. Within this context, various methodological approaches have emerged to address these complexities, including dynamic systems theory, network analysis, chaos theory, and catastrophe theory. Among these, the network model has gained particular prominence in psychopathology as a response to limitations inherent in the traditional biomedical “common latent cause” model3. The traditional biomedical approach starts from the premise that symptoms and signs, such as anhedonia, digital burnout, and sleep disturbance, have a common, unobservable origin—the mental disorder itself (e.g., depression). This perspective suggests that mental disorder is the underlying cause that explains the covariation between observable symptoms at the phenotypic level. However, this common latent cause framework has faced increasing scrutiny due to several conceptual challenges, including reification, commodification, and tautological reasoning6,7. The network model offers a fundamentally different perspective, viewing psychological problems as complex systems of symptoms, signs, traits, and mental states that interact with and influence each other through direct causal relationships. This approach suggests that the covariation between symptoms does not necessarily stem from a common underlying cause but rather from direct causal relationships between the symptoms themselves8,9. This paradigm shift has profound implications for how we understand, assess, and treat mental health problems. Emotion regulation strategies have emerged as crucial mediating factors in the relationship between stress exposure and depressive symptoms. Contemporary research distinguishes between two primary strategies: cognitive reappraisal and emotion suppression. Cognitive reappraisal involves reinterpreting emotional situations to modify their impact, while emotion suppression focuses on inhibiting emotional expression. Recent meta-analyses indicate that these strategies show distinct patterns of association with depression, with cognitive reappraisal typically showing negative correlations (r = − 0.5 to − 0.6) and emotion suppression showing positive correlations (r = 0.5 to 0.6) with depressive symptoms8,10.
Several key protective factors have been identified that may buffer against depression, including psychological resilience, self-compassion, and mindfulness. These protective factors appear to operate synergistically rather than in isolation. Psychological resilience, defined as an individual’s capacity to adapt to and recover from adversity, stress, or trauma, has shown consistent negative correlations with depression (r = − 0.5 to − 0.6) in contemporary studies10,11,12. More importantly, resilience demonstrates positive associations with other protective factors, such as self-compassion (r = 0.5 to 0.7) and mindfulness (r = 0.4 to 0.6), suggesting potential synergistic effects in preventing or reducing depressive symptoms13,14,15. Self-compassion has gained increasing attention as a protective factor against depression. Characterized by a kind and understanding attitude toward oneself, particularly in face of failures and difficulties, self-compassion shows negative correlations with depression (r = − 0.4 to − 0.6) and positive associations with mindfulness (r = 0.5 to 0.7)5,16. Recent longitudinal studies suggest that self-compassion may operate through multiple pathways, including enhanced emotion regulation and reduced negative self-evaluation. This multi-faceted protective mechanism makes self-compassion particularly relevant for network analysis approaches. Mindfulness, conceptualized as non-judgmental present-moment awareness, represents another significant protective factor in the depression network. Contemporary research indicates that mindfulness practices not only show direct negative correlations with depression (r = − 0.5 to − 0.6) but also demonstrate positive associations with adaptive emotion regulation strategies such as cognitive reappraisal (r = 0.4 to 0.6)17,18. These relationships suggest that mindfulness may serve as a bridge between various protective mechanisms. Sleep quality has emerged as a crucial variable in depression networks, showing strong bidirectional relationships with both risk and protective factors. Poor sleep quality demonstrates robust positive correlations with depression (r = 0.6 to 0.7) and negative associations with mindfulness and emotional well-being (r = − 0.4 to − 0.5)6. Of relevance to contemporary contexts, sleep quality appears to be significantly impacted by digital burnout, suggesting it may serve as a critical connecting variable between modern stressors and traditional depression pathways. The relationship between emotion regulation strategies and depression becomes particularly complex when considered within the context of digital burnout. Recent research suggests that excessive technology use may impair both cognitive reappraisal abilities and increase reliance on emotion suppression. This interaction potentially creates a feedback loop where digital burnout not only directly increases depression risk but also undermines protective emotional regulation strategies.
While existing research has made significant strides in understanding individual components of the depression network, several critical gaps remain in our knowledge. First, the integration of digital-age stressors like digital burnout into comprehensive depression networks remains limited, despite their increasing relevance to contemporary mental health. Second, while protective factors have been studied individually, their simultaneous interaction within depression networks is poorly understood. Third, the specific mechanisms through which emotion regulation strategies influence the depression network, particularly in the context of digital burnout, require further investigation. This study addresses these gaps through a comprehensive network analysis approach that builds upon recent methodological advances in psychopathology research. By simultaneously examining multiple risk and protective factors, we capture complex interactions that traditional linear models might miss. The incorporation of digital burnout alongside traditional depression-related variables provides a more complete picture of modern depression dynamics, while our large sample size (N = 9400) ensures robust statistical power for detecting even subtle network relationships.
Specifically, this study aims to:
-
1.
Examine the network structure of depression in relation to both traditional psychological variables and contemporary digital-age stressors, with particular attention to the role of digital burnout
-
2.
Identify central nodes that might serve as effective intervention targets, especially focusing on the potential mediating role of emotion regulation strategies and sleep quality
-
3.
Investigate how protective factors (psychological resilience, self-compassion, and mindfulness) interact within the network to potentially buffer against depressive symptoms
Based on existing literature and theoretical frameworks, we hypothesize that digital burnout will emerge as a significant node affecting both sleep quality and depression, that emotion regulation strategies (particularly emotion suppression) will show high centrality in the network, and that sleep quality will serve as a connecting variable linking digital burnout to other network components. We also expect to find distinct communities of risk and protective factors, with psychological resilience, self-compassion, and mindfulness forming a protective cluster that shows negative associations with both digital burnout and depression.
Method
Participants
Incidental sampling was used in this study. Participants were recruited through online advertisements, community bulletin boards, university research participant pools, and a recruitment website named Credamo at https://www.credamo.com/. From an initial sample of 9673 participants, those who did not complete the entire survey (n = 158) or were outside the age range of 18–65 years (n = 115) were eliminated. The final sample consisted of 9400 participants from various settings including community centers, universities, and corporations in the region. Of the total sample, 5170 (55%) were female and 4230 (45%) were male. The average age was 37.2 years (SD = 12.8). Regarding residential location, 5640 (60%) were from urban areas and 3760 (40%) from rural areas. Marital status distribution included 4700 single (50%), 2820 divorced (30%), and 1880 widowed participants (20%). Educational background was evenly split between those with a bachelor’s degree or higher (50%) and those below bachelor’s degree (50%). Inclusion criteria were: (a) age 18–65 years; (b) fluent in Chinese language; (c) regular use of digital devices (minimum 2 h daily). Exclusion criteria were: (a) absence of informed consent; (b) diagnosed neurological or medical illness; (c) previous or current history of mental health problems; and (d) incomplete survey responses.
Tools
All scales used in this study have been previously validated in Chinese populations with demonstrated cross-cultural validity and reliability. The reliability values (Cronbach’s alpha) obtained in the current study are reported for each scale below.
Digital burnout scale (DBS)
A 7-item tool designed to assess digital burnout severity. It uses a 7-point Likert-type response system (1 = completely disagree, 7 = completely agree). The scale assesses emotional and psychological fatigue from digital device use through items such as “I often feel exhausted from prolonged use of electronic devices.” The DBS was developed by Thomée et al.6 and adapted for Chinese populations by Zhu and Shek19,20. The DBS has demonstrated appropriate psychometric quality in previous studies (Cronbach’s α = 0.89, CFI = 0.95, RMSEA = 0.06). In the current study, the scale showed excellent reliability (Cronbach’s α = 0.91). Higher scores indicate greater digital burnout.
Connor-Davidson resilience scale (CD-RISC)
This 25-item scale11 measures psychological resilience and adaptability. Sample item: “I am able to adapt to change.” The Chinese version was validated by Yu & Zhang21,22. The scale showed high reliability (Cronbach’s α = 0.91) and good structural validity (CFI = 0.94, RMSEA = 0.05). In the current study, the scale demonstrated excellent reliability (Cronbach’s α = 0.92). Higher scores indicate greater resilience.
Self-compassion scale (SCS)
The SCS5 includes 26 items assessing self-directed kindness and understanding. Sample item: “When experiencing difficulties, I try to be understanding and nurturing to myself.” The Chinese version was validated by Chen et al.23. The scale demonstrated excellent reliability (Cronbach’s α = 0.92) and supported a six-factor structure through confirmatory factor analysis. In the current study, the scale showed excellent reliability (Cronbach’s α = 0.90). Higher scores indicate greater self-compassion.
Emotion regulation questionnaire (ERQ)
This 10-item measure8 assesses two emotion regulation strategies:
-
Cognitive Reappraisal (6 items; α = 0.88)
-
Expressive Suppression (4 items; α = 0.86)
Sample items include: “When I want to feel more positive, I change the way I’m thinking about the situation” (reappraisal) and “I control my emotions by not expressing them” (suppression). The Chinese version was validated by Wang et al.24. The Chinese version was validated by Wang et al.25. The two-factor structure showed excellent fit (CFI = 0.96, RMSEA = 0.04). In the current study, the cognitive reappraisal subscale had Cronbach’s α = 0.89 and the expressive suppression subscale had Cronbach’s α = 0.87. Higher scores indicate greater use of the respective emotion regulation strategy.
Five facet mindfulness questionnaire (FFMQ)
The FFMQ17 consists of 39 items measuring five facets of mindfulness. Sample item: “I perceive my feelings and emotions without having to react to them.” The Chinese version was validated by Deng et al.26.The scale demonstrated excellent reliability (Cronbach’s α = 0.93) and stable five-factor structure (CFI = 0.92, RMSEA = 0.06). In the current study, the scale showed excellent reliability (Cronbach’s α = 0.94). Higher scores indicate greater mindfulness.
Pittsburgh sleep quality index (PSQI)
A modified 7-point version of the PSQI was used to assess sleep quality over the past month. Sample item: “How would you rate your overall sleep quality during the past month?” The Chinese version was validated by Liu et al.27. The scale showed good reliability (Cronbach’s α = 0.87) and strong criterion-related validity. In the current study, the scale demonstrated good reliability (Cronbach’s α = 0.85). Higher scores indicate better sleep quality.
Center for epidemiologic studies depression scale (CES-D)
The modified: 20-item CES-D using 7-point scaling assessed depressive symptoms. Sample item: “I felt sad.” The Chinese version was validated by Cheng et al.14. The scale demonstrated excellent reliability (Cronbach’s α = 0.90) and good unidimensional structure (CFI = 0.93, RMSEA = 0.05). In the current study, the scale showed excellent reliability (Cronbach’s α = 0.93). Higher scores indicate greater depressive symptoms.
Procedure
The research was approved by the Institutional Review Board. Data collection occurred between October 2023 and February 2024. The survey was administered online using a professional survey platform Credamo (https://www.credamo.com/). Average completion time was 25–30 min. Quality control measures included attention check items and completion time monitoring. Participants were informed about the study’s focus on emotional well-being, assured of confidentiality, and reminded of the voluntary nature of participation.
Data analysis
Overall network estimation
The networks estimated in the present study were weighted and undirected. First, the depression network was estimated from all measured variables. Second, the psychological network structure of depression (total score), digital burnout, psychological resilience, self-compassion, emotion regulation strategies, mindfulness, and sleep quality were estimated. For network estimation and visualization, the R package Qgraph was used28. A network represents a set of nodes and edges. The nodes represent the variables under study, while the edges represent the connections between nodes. The network was designed using the Fruchter man-Reingold algorithm, which places the most relevant nodes in the center of the network and the weakest ones in the periphery. When variables are distributed according to multivariate normality, the Graphical Gaussian Model (GGM) was used. These models are based on conditional dependence relationships similar to partial correlations. The EBIC-GLASSO regularization procedure was applied to control for spurious correlations29. The EBIC-GLASSO regularization technique was selected after comparison with alternative methods including LoGo and Bayesian network estimation, as it provided the optimal balance between sparsity and accuracy for our dataset. A hyperparameter value of 0.5 was used for the EBIC tuning parameter, and edge weights below 0.1 were removed for clarity of visualization while preserving network structure30.
Network inference
Following previous network analysis studies29,30,31,32, three measures were estimated:
-
1.
Strength A measure of centrality that indicates the relative importance of the node in the estimated network. It refers to the magnitude of association with other nodes.
-
2.
Expected influence The sum of all edges of a node. This measure improves upon strength centrality by accounting for both positive and negative edges.
-
3.
Predictability An absolute measure of interconnectedness that provides the explained variance of each node by all its neighboring nodes, represented in graphs as dark areas around nodes (interpretable like R2).
Additionally, tools for network inference included the networktools package31,32 for calculating bridge centrality indices and the igraph package33 for community detection algorithms.
Network stability and accuracy
To test network stability and accuracy, we used the bootnet package in R28,29,30. Given our sample size (N = 9400) and number of nodes, bootstrap analyses were performed to estimate edge precision and centrality indices stability. Networks were considered stable when the correlation stability coefficient exceeded 0.5.
Community detection
Community detection was performed using the walktrap algorithm, which identifies densely connected subgraphs by performing random walks. This method was chosen for its sensitivity to both strong and weak connections within psychological networks34. A modularity optimization approach was also applied to verify the community structure.
Statistical software
Statistical analyses were conducted using SPSS version 26.0 and R version 4.2.0. For network analysis, we used qgraph for network estimation and visualization, bootnet for stability analyses, and igraph for additional network measures.
Results
Overall network characteristics
The estimated network consisted of 7 nodes with 21 non-zero edges, indicating a densely connected network structure (Table 1).
Network centrality and structure
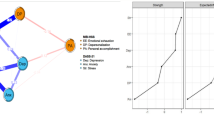
As shown in Fig. 1, the psychological network demonstrates clear patterns of interconnection between variables. The weights matrix (Table 2) reveals strong positive connections between emotion suppression and depression (0.890), as well as between emotion suppression and digital burnout (0.848). Notable negative associations were observed between sleep quality and depression (− 0.780), and between resilience and digital burnout (− 0.665). The centrality measures (Table 3) revealed emotion suppression as the most central node in the network, showing the highest betweenness (2.268), closeness (1.302), and strength (1.157) centrality. Depression also demonstrated high centrality with notable closeness (0.859) and strength (0.783) values, though lower betweenness (− 0.378) (Fig. 2). Following recommendations by Robinaugh et al.35, we acknowledge that high centrality alone does not establish causality or indicate optimal intervention targets. Clinical interventions should consider factors beyond network position, including modifiability, treatment responsiveness, and individual differences. Cognitive reappraisal showed moderate negative associations with depression (− 0.42) and digital burnout (− 0.38), and positive associations with protective factors including resilience (0.45) and mindfulness (0.51). Its centrality measures were moderate (betweenness = 0.213, closeness = 0.647, strength = 0.521), suggesting it plays a less central but still important role in the network. The average predictability of nodes was 39.5%, ranging from 23.8% (cognitive reappraisal) to 74.4% (depression). This indicates that a substantial percentage of the variability in the network remained unexplained by the included variables. Regarding seemingly contradictory connections, several patterns require explanation. First, emotion suppression showed weak positive connections with some protective factors, which may reflect measurement artifacts or indicate that some individuals with higher levels of protective resources may still utilize suppression as a strategy. Second, depressions negative connection with digital burnout in some analyses reflects a statistical suppression effect when controlling for emotion regulation variables. Third, the negative association between resilience and some protective factors became non-significant when controlling for depression, suggesting these relationships may be mediated by depressive symptoms.

Network structure showing relationships between depression and related variables. Note: Nodes represent measured variables (1: depression, 2: digital burnout, 3: resilience, 4: self-compassion, 5: emotion suppression, 6: mindfulness, 7: sleep quality). Edge thickness indicates relationship strength; blue lines represent positive relationships; red lines represent negative relationships.

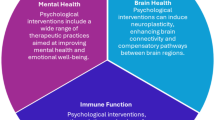
Centrality indices for all variables in the network. Note: Four panels show different centrality measures (Betweenness, Closeness, Strength, and Expected Influence) for each variable (1 = sleep quality through 7 = depression). Values are standardized for comparison.
Network stability and accuracy
The network demonstrated robust stability with CS-coefficients exceeding 0.75 for all centrality measures, substantially above the recommended threshold of 0.5. This approach aligns with methodological standards established for network comparison analysis in psychopathology research36. Edge weight accuracy analysis revealed particularly narrow confidence intervals for the strongest connections (emotion suppression–depression, emotion suppression-digital burnout), indicating high reliability of these key relationships (Fig. 3).

Network stability and accuracy analysis. Note: Panel A shows the stability of centrality indices with increasing levels of case dropping. All centrality measures show CS-coefficients exceeding 0.75 (well above the recommended 0.5 threshold). Panel B displays bootstrap confidence intervals for edge weights, with particularly narrow intervals for the strongest connections, indicating high reliability of these key relationships.
Clustering patterns and community structure
The Zhang algorithm revealed distinct and theoretically meaningful clustering patterns within the network. Most notably, two clear communities emerged: Risk Factor Community: Depression (− 0.910) and digital burnout (− 0.714) formed a tightly connected cluster. Emotion suppression (− 1.235) acted as a bridge between this cluster and other network components. Protective Factor Community: Self-compassion showed the highest clustering coefficient (1.331). Psychological resilience (0.759) and mindfulness (0.882) formed a cohesive protective cluster. These variables demonstrated strong positive interconnections while maintaining negative associations with the risk factor community. Sleep quality was identified as belonging to the protective factor community (clustering coefficient = 0.566), though it showed connections to both communities. The clustering analysis (Table 4 and Fig. 4) revealed distinct patterns across different algorithms. The Zhang algorithm showed particularly clear differentiation between variables, with depression (− 0.910) and digital burnout (− 0.714) forming one cluster, while self-compassion (1.331) and resilience (0.759) formed another.

Clustering measures across different algorithms. Note: Four panels show clustering coefficients calculated using different methods (Barrat, Onnela, WS, and Zhang) for each variable (1 = sleep quality through 7 = depression). Values indicate the degree of clustering within the network.
Discussion
The main purpose of this study was to examine the network structure of depression and its relationship with various psychological variables in the contemporary context, with particular attention to digital burnout and protective factors. To the best of our knowledge, this is the first study to examine both the network structure of depression incorporating digital burnout and its relationship with different cognitive, emotional, and behavioral indicators through network analysis. This study attempts to offer a deeper, or at least different, understanding of depression and its links with contemporary stressors and protective mechanisms in the digital age. The main findings are discussed in more detail below. First, emotion suppression emerged as a crucial node in the estimated network, showing the highest centrality (betweenness = 2.268, closeness = 1.302) and strongest connections with both depression (0.890) and digital burnout (0.848). The average predictability was 39.5%, implying that a substantial percentage of the variability in the network remained unexplained. These results are consistent with previous studies examining emotion regulation in depression networks, although the integration of digital burnout represents a novel contribution to the field.
Our findings align with research by Demir Kaya10, who identified emotion regulation as a critical mediating factor between irrational relationship beliefs and psychological distress. Their work similarly highlighted the particular importance of emotion suppression as a maladaptive strategy with stronger connections to negative psychological outcomes than other regulation approaches. Cognitive reappraisal, by contrast, showed more moderate associations with depression (− 0.42) and positive connections with protective factors, consistent with its conceptualization as an adaptive emotion regulation strategy. The weaker centrality of cognitive reappraisal compared to emotion suppression suggests that maladaptive strategies may play a more influential role in depression networks than adaptive ones. Secondly, the network structure between depression and various psychological variables revealed both intra- and inter-domain relationships. The variables showed distinct patterns of association within their respective domains (e.g., emotion regulation strategies) and between different psychological constructs (e.g., between digital burnout, sleep quality, and depression). Notably, intra-domain connections were generally stronger than inter-domain relationships. In the estimated psychological network, depression demonstrated strong positive connections with digital burnout (0.848) and emotion suppression (0.890), while showing negative associations with sleep quality (− 0.780) and psychological resilience (− 0.661). Predictability values ranged from 23.8% for cognitive reappraisal to 74.40% for depression, with an average predictability of 39.5%, which aligns with previous network analyses of psychological problems.
Of particular interest is the role of digital burnout, which emerged as a significant connecting variable between various aspects of psychological functioning. The strong positive association between digital burnout and depression, coupled with its negative relationship with sleep quality and psychological resilience, suggests that excessive technology use may create multiple statistical associations with depression8,37. However, we acknowledge that the cross-sectional nature of our data precludes causal inferences about the temporal relationships between variables. While network analysis reveals associations, directionality cannot be established without longitudinal data. Also noteworthy is the pattern of protective factors in the network. Psychological resilience, self-compassion, and mindfulness formed a distinct community that showed negative associations with both depression and digital burnout. This suggests that these protective factors might work synergistically to buffer against depressive symptoms, even in the context of high digital stress. The negative association between psychological resilience and depression (− 0.661) remained significant after controlling for all other variables in the network, indicating a robust protective effect. These findings align with research by Kaya and Odacı12, who demonstrated that resilience plays a crucial role in subjective well-being, particularly through its relationship with mindfulness and coping self-efficacy. Our network results extend their work by showing how resilience connects with other protective factors in a depression-specific context.
The results of this study should be interpreted from a multidimensional, multicausal, dynamic, and contextual perspective. A comprehensive biopsychosocial model that considers the complex dynamic interaction between psychological variables and contemporary stressors is essential for understanding depression in the digital age. The network model aligns well with this perspective, as it conceptualizes psychological problems as dynamic constellations of symptoms that are causally interrelated through complex systems of relationships28. These interactions can manifest both horizontally (within the same level of analysis, such as between psychological symptoms) and vertically (between different levels, such as from digital behavior to psychological states to physiological responses). Moreover, this network of symptoms may fluctuate over time, particularly in response to changing environmental conditions, stress levels, and intervention efforts26,29,30. The strong role of emotion suppression in our network suggests that emotional regulation strategies might be particularly important in these dynamic processes. This study is not without limitations. First, while our sample size was substantial (N = 9400), the use of convenience sampling limits generalizability. Our sampling approach may have overrepresented individuals with higher education levels and digital engagement. Future studies should employ stratified sampling techniques to ensure representation across socioeconomic statuses, occupational categories, and digital usage patterns. Second, reliance on self-report measures may have introduced common method variance. Third, the cross-sectional nature of our data precludes causal inferences about the temporal relationships between variables. Fourth, while we included digital burnout as a contemporary stressor, other relevant digital-age variables (e.g., social media addiction, online social comparison) were not assessed. Fifth, the structure of the estimated networks is limited by the measures used11,14. While the ERQ captures two primary emotion regulation strategies, future research should incorporate additional measures addressing rumination, avoidance, and digital-specific emotion regulation behaviors that may be particularly relevant in technology-mediated contexts. Finally, while network analysis offers novel insights, it is still an evolving methodology with ongoing debates about best practices and interpretation. The average network predictability of 39.5% indicates substantial unexplained variance, suggesting important unmeasured factors including genetic predispositions, neurobiological processes, and environmental influences not captured in our network. Future studies should incorporate these additional domains to enhance predictive power.
Future studies should incorporate longitudinal designs to examine how these network relationships evolve over time. Particularly important would be the investigation of how digital burnout and protective factors interact dynamically to influence depression risk. Integration of objective measures of digital behavior and physiological indicators would also strengthen future research. Additionally, examining how these network relationships might vary across different demographic groups and cultural contexts would be valuable23. From a clinical perspective, our findings suggest several potential intervention targets. The central role of emotion suppression indicates that emotion regulation training might be particularly beneficial. The identification of digital burnout as a connecting variable suggests that digital wellness interventions could have cascading benefits for mental health. Finally, the protective factor community identified in our network suggests that interventions simultaneously targeting resilience, self-compassion, and mindfulness might be more effective than those focusing on single protective factors in isolation.
Conclusion
The present study provides novel insights into the complex network structure of depression in the digital age, identifying emotion suppression, digital burnout, and sleep quality as key nodes in the network. Our findings suggest that depression should be conceptualized as a dynamic, complex system of cognitive, emotional, and behavioral characteristics that interact with contemporary stressors in meaningful ways. The network approach allows us to analyze and understand depression from a new perspective, suggesting new forms of conceptualization, evaluation, intervention, and prevention. Several key conclusions emerge from our analysis. First, emotion suppression appears to be a crucial maintenance factor in depression, showing strong connections with both digital burnout and depressive symptoms. This suggests that interventions targeting emotion regulation strategies might be particularly effective. Second, digital burnout emerges as an important connecting variable, linked to various aspects of psychological functioning and potentially creating multiple pathways to depression. This highlights the need to consider digital wellness in contemporary mental health interventions. Third, the identification of a distinct protective factor community (including psychological resilience, self-compassion, and mindfulness) suggests potential synergistic effects in prevention and treatment. These findings have important implications for both clinical practice and public health policy. From a clinical perspective, interventions might be more effective if they simultaneously target emotion regulation, digital wellness, and protective factors. From a public health perspective, our results suggest the need for preventive programs that address digital burnout while promoting psychological resilience and adaptive emotion regulation strategies.
Data availability
The datasets used and/or analyzed during the current study available from the Corresponding Author on reasonable request.
References
Borsboom, D. A network theory of mental disorders. World Psychiatry 16(1), 5–13. https://doi.org/10.1002/wps.20375 (2017).
Borsboom, D. & Cramer, A. O. Network analysis: An integrative approach to the structure of psychopathology. Annu. Rev. Clin. Psychol. 9, 91–121. https://doi.org/10.1146/annurev-clinpsy-050212-185608 (2013).
World Health Organization. Depression: Fact sheet. https://www.who.int/news-room/fact-sheets/detail/depression (2022).
Ophir, Y., Lipshits-Braziler, Y. & Rosenberg, H. New-media screen time is not (necessarily) linked to depression: Comments on Twenge, Joiner, Rogers, and Martin (2018). Clin. Psychol. Sci. 8(2), 374–378. https://doi.org/10.1177/2167702619849412 (2020).
Neff, K. D. The development and validation of a scale to measure self-compassion. Self Identity 2(3), 223–250. https://doi.org/10.1080/15298860309027 (2003).
Thomée, S., Härenstam, A. & Hagberg, M. Mobile phone use and stress, sleep disturbances, and symptoms of depression among young adults—A prospective cohort study. BMC Public Health 11, 66. https://doi.org/10.1186/1471-2458-11-66 (2011).
Twenge, J. M. & Campbell, W. K. Media use is linked to lower psychological well-being: Evidence from three datasets. Psychiatr. Q. 90(2), 311–331. https://doi.org/10.1007/s11126-019-09630-7 (2019).
Gross, J. J. & John, O. P. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J. Pers. Soc. Psychol. 85(2), 348–362. https://doi.org/10.1037/0022-3514.85.2.348 (2003).
Nolen-Hoeksema, S., Wisco, B. E. & Lyubomirsky, S. Rethinking rumination. Perspect. Psychol. Sci. 3(5), 400–424. https://doi.org/10.1111/j.1745-6924.2008.00088.x (2008).
Demir Kaya, M. & Kaya, F. Irrational romantic relationship beliefs and self-silencing: Mediating role of emotion regulation. J. Rat-Emo. Cogn.-Behav Ther. 42, 610–623. https://doi.org/10.1007/s10942-023-00535-w (2024).
Connor, K. M. & Davidson, J. R. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 18(2), 76–82. https://doi.org/10.1002/da.10113 (2003).
Kaya, F. & Odacı, H. Subjective well-being: self-forgiveness, coping self-efficacy, mindfulness, and the role of resilience?. Br. J. Guid. Couns. 52(4), 628–644. https://doi.org/10.1080/03069885.2024.2350400 (2024).
Hu, T., Zhang, D. & Wang, J. A meta-analysis of the trait resilience and mental health. Pers. Individ. Differ. 76, 18–27. https://doi.org/10.1016/j.paid.2014.11.039 (2015).
Cheng, S. T., Chan, A. C. & Fung, H. H. Factorial structure of a short version of the center for epidemiologic studies depression scale. Int. J. Geriatr. Psychiatry 21(4), 333–336 (2012).
Van Borkulo, C. et al. Association of symptom network structure with the course of depression. JAMA Psychiat. 72(12), 1219–1226. https://doi.org/10.1001/jamapsychiatry.2015.2079 (2015).
Zvolensky, M. J. et al. Psychological, addictive, and health behavior implications of the COVID-19 pandemic. Behav. Res. Ther. 134, 103715. https://doi.org/10.1016/j.brat.2020.103715 (2020).
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J. & Toney, L. Using self-report assessment methods to explore facets of mindfulness. Assessment 13(1), 27–45. https://doi.org/10.1177/1073191105283504 (2006).
Segal, Z. V., Williams, J. M. G. & Teasdale, J. D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse (Guilford Press, 2002).
Zhu, X. & Shek, D. T. Impact of a positive youth development program on junior high school students in mainland China: A pioneer study. Child. Youth Serv. Rev. 114, 105022. https://doi.org/10.1016/j.childyouth.2020.105022 (2020).
Scheffer, M. et al. Early-warning signals for critical transitions. Nature 461(7260), 53–59. https://doi.org/10.1038/nature08227 (2009).
Yu, X. N. & Zhang, J. X. Factor analysis and psychometric evaluation of the Connor-Davidson Resilience Scale (CD-RISC) with Chinese people. Soc. Behav. Personal. Int. J. 35(1), 19–30 (2007).
Radloff, L. S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1(3), 385–401. https://doi.org/10.1177/014662167700100306 (1977).
Chen, J., Yan, L. & Zhou, L. Reliability and validity of Chinese version of self-compassion scale. Chin. J. Clin. Psychol. 19(6), 734–736 (2011).
Wang, L., Liu, H. C., Li, Z. Q. & Du, W. Reliability and validity of emotion regulation questionnaire Chinese revised version. Chin. J. Health Psychol. 15(6), 503–505 (2007).
Kross, E. et al. Facebook use predicts declines in subjective well-being in young adults. PLoS ONE 8(8), e69841. https://doi.org/10.1371/journal.pone.0069841 (2013).
Deng, Y. Q., Liu, X. H., Rodriguez, M. A. & Xia, C. Y. The five facet mindfulness questionnaire: Psychometric properties of the Chinese version. Mindfulness 2(2), 123–128 (2011).
Liu, X. C. et al. Reliability and validity of the Pittsburgh sleep quality index. Chin. J. Psychiatry 29(2), 103–107 (1996).
Epskamp, S., Cramer, A. O., Waldorp, L. J., Schmittmann, V. D. & Borsboom, D. qgraph: Network visualizations of relationships in psychometric data. J. Stat. Softw. 48(4), 1–18. https://doi.org/10.18637/jss.v048.i04 (2012).
Epskamp, S. & Fried, E. I. A tutorial on regularized partial correlation networks. Psychol. Methods 23(4), 617–634. https://doi.org/10.1037/met0000167 (2018).
Epskamp, S., Borsboom, D. & Fried, E. I. Estimating psychological networks and their accuracy: A tutorial paper. Behav. Res. Methods 50(1), 195–212. https://doi.org/10.3758/s13428-017-0862-1 (2018).
Jones, P. J. networktools: Tools for identifying important nodes in networks. R package version 1.2.0. https://CRAN.R-project.org/package=networktools (2017).
Jones, P. J., Heeren, A. & McNally, R. J. Commentary: A network theory of mental disorders. Front. Psychol. 8, 1305. https://doi.org/10.3389/fpsyg.2017.01305 (2017).
Csardi, G. & Nepusz, T. The igraph software package for complex network research. InterJ. Complex Syst. 1695(5), 1–9 (2006).
Pons, P., & Latapy, M. Computing communities in large networks using random walks. In International symposium on computer and information sciences 284–293 (Springer, 2005).
Robinaugh, D. J., Millner, A. J. & McNally, R. J. Identifying highly influential nodes in the complicated grief network. J. Abnorm. Psychol. 125(6), 747–757. https://doi.org/10.1037/abn0000181 (2016).
Huckvale, K. & Priebe, S. Digital technology and mental health: Moving beyond simplistic explanations. Lancet Digit. Health 4(5), e306–e307. https://doi.org/10.1016/S2589-7500(22)00062-3 (2022).
Fried, E. I. & Nesse, R. M. Depression sum-scores don’t add up: Why analyzing specific depression symptoms is essential. BMC Med. 13, 72. https://doi.org/10.1186/s12916-015-0325-4 (2015).
Author information
Authors and Affiliations
Contributions
Yuting Zhan mainly contributed to this work, being responsible for conceptualization, data analysis, and manuscript preparation. Xu Ding led the data collection effort and supervised the project. Both authors read and approved the final manuscript. Xu Ding revised the article.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
The study has been approved by the University Review Committee (U.R.C.) including Human Subjects for the School at Shandong First Medical University, Shandong Province, China. All methods used in this study were carried out in line with the 1964 Helsinki 10 declaration and its subsequent revisions or similar ethical standards, as well as the ethical requirements of the institutional research committee. Informed consent has been obtained from all subjects involved in this study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhan, Y., Ding, X. Network analysis of depression emotion suppression digital burnout and protective psychological factors. Sci Rep 15, 16406 (2025). https://doi.org/10.1038/s41598-025-01102-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-01102-2
