
Abstract
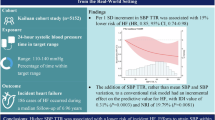
To examine the associations between the systolic blood pressure (SBP) time in target range (TTR) and carotid atherosclerosis indicators: carotid intima-media thickness (cIMT) and carotid atherosclerotic plaques (CAPs). We conducted a cross-sectional analysis of 7738 hypertensive participants from the Kailuan study who completed a health examination and carotid ultrasonography. TTR was estimated using linear interpolation method, with SBP falling within 120–140 mmHg. Participants were categorized into four groups according to quartiles of SBP-TTR. Logistic and multivariate linear regression were used to study the associations between SBP-TTR and cIMT/CAPs. Compared with the SBP-TTR < 25% group, cIMT gradually decreased in the other three groups and the cIMT decreased by 0.018 mm for every standard deviation increase in SBP-TTR. Additionally, compared to the SBP-TTR < 25% group, the incidence rates of CAPs were lower in the other three groups. Each one standard deviation increase in SBP-TTR was associated with a 10.6% decrease in the risk of CAPs (0.894 [95% CI 0.814 to 0.982]). Those associations were found independent of conventional risk factors. Our study indicates a negative correlation between SBP-TTR and carotid atherosclerosis among hypertensive individuals. Stabilizing blood pressure within normal ranges could reduce cardiovascular risks in hypertensive patients.
Similar content being viewed by others
Introduction
Hypertension stands as one of the most prevalent cardiovascular diseases globally1,2,3. As of 2019, 1.28 billion adults worldwide were diagnosed with hypertension, indicating a twofold increase over the past 30 years4. Furthermore, the Report on Cardiovascular Health and Diseases in China 20225 revealed that approximately 245 million individuals suffer from hypertension. Hypertension not only serves as the main controllable risk factor for atherosclerotic cardiovascular diseases but also prolonged elevations in blood pressure can lead to subclinical target organ damage, such as vascular structural alterations including thickening of the carotid artery intima-media and the development of left ventricular hypertrophy6. Hypertension emerges as a significant risk factor for atherosclerotic cardiovascular diseases (ASCVD). Extensive epidemiological studies and randomized controlled trials (RCTs) have confirmed that effective management of blood pressure and associated risk factors among hypertension patients can drastically mitigate the risk of ASCVD.
The common index for controlling the blood pressure of hypertension patients is achieving the standard level, which entails reducing the blood pressure to below 140/90 mmHg through various interventional measures, including the administration of antihypertensive drugs. RCTs and clinical practice often use this criterion to assess blood pressure control. However, as a fluctuating physiological process, a single blood pressure value reaching the standard threshold is insufficient to reflect sustained blood pressure control over time and does not consider blood pressure variability. In response to this limitation, Doumas et al. introduced the concept of time in target range (TTR) for blood pressure measurements in 20177,8,9. TTR represents the proportion of blood pressure readings falling within a specified range, and subsequent studies have successively confirmed its negative correlation with adverse outcomes including ASCVD10,11,12. However, there is no study reporting the association between TTR and carotid atherosclerosis. We speculate that the TTR of hypertension patients may be negatively associated with the intima-media thickness or plaque of the carotid artery. To validate our conjecture, we used the data of the Kailuan study population to analyze the association between the TTR of hypertension patients and two key indicators for carotid atherosclerosis: carotid intima-media thickness (cIMT) and carotid atherosclerotic plaques (CAPs).
Methods
Study population and design
This cross-sectional study was conducted among hypertensive participants in the Kailuan study. Briefly, the Kailuan study is a prospective cohort study that focuses on risk factors associated with cardiovascular and cerebrovascular diseases. It was conducted among both current and retired employees of the Kailuan Company in Tangshan City. Since 2006, epidemiological data from health examinations have been systematically collected every two years. The participants in this study were randomly selected from those who attended the initial physical examination in 2006. They subsequently underwent cIMT and CAPs measurements through carotid ultrasonography, which was not part of the routine follow-up schedule but instead performed at various time points between 2012 and 2018. The exposure period for calculating TTR was defined as the interval between the time of the participant’s first Kailuan health examination and the time of their first carotid ultrasound measurement. The data for cIMT and CAPs were derived from their first ultrasound measurement.
Initially, 8403 participants underwent carotid artery ultrasound measurements and were found to be hypertensive during the first physical examination in 2006–2010. Following the application of certain exclusion criteria, 665 participants were excluded from the study, comprising 395 participants with fewer than two blood pressure records and 270 participants with cardiovascular diseases at the time of carotid ultrasound measurement. Consequently, a total of 7738 participants were included in the analysis. Figure 1 shows the study-design flowchart.

The study-design flowchart.
In accordance with the Helsinki Declaration, the protocol was approved by the Ethics Committee of the Kailuan General Hospital [(2006) Approval No. 5], and all participants gave written informed consent to participate in the study. Clinical Trial number: ChiCTR-TNC-11,001,489 (retrospective registration). Trained professionals surveyed the subjects and completed a standard questionnaire that encompassed gender, age, height, weight, waist circumference, occupational status, and lifestyle habits, including sleep, smoking, drinking, physical exercise, and diet. The details of the Kailuan study have been previously documented13,14. For clarity, smoking was defined as consuming an average of at least 1 cigarette daily over the past year, and drinking was described as consuming at least 100 ml of alcohol with a 50% alcohol content per day. Laboratory examinations were conducted using the Hitachi 7600 Automatic Biochemical Analyzer (Northern Biological Institute, Beijing, China), performed by the same team following reagent instructions. Subjects fasted for a minimum of 8 h before a 5 ml venous blood sample was drawn at 7:00 am. Serum was promptly isolated and processed within 4 h, with measurements for total cholesterol (TC), triglyceride (TG), fasting blood glucose (FBG), high-sensitivity C-reactive protein (hs-CRP), Serum creatinine (Scr), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) collected. Diabetes was defined as having a history of diabetes mellitus, currently using insulin or oral hypoglycemic drugs, or FBG > 126 mg/dl. Hyperlipidemia was characterized as having a history of hyperlipidemia, TC > 220 mg/dl, TG > 150 mg/dl, or current lipid-lowering drug use. eGFR was computed using serum creatinine, sex, and age15: male: eGFR = 141 × min(Scr/к,1)а × max(Scr/к,1)−1.209 × 0.993age; Female: eGFR = 141 × min(Scr/к,1)а × max(Scr/к,1)−1.209 × 0.993age × 1.018.
Assessment of blood pressure and SBP-TTR
Blood pressure measurements were conducted between 7:00 am and 9:00 am on the day of the physical examination under the supervision of trained medical professionals. Before the measurements, subjects were required to rest in a comfortable position for at least 15 min, keeping quiet during the measurement. A calibrated desk mercury sphygmomanometer was utilized to measure the blood pressure in the right brachial artery during the follow-up period spanning from 2006 to 2012. The first Korotkoff sound was employed to define systolic blood pressure (SBP), while the fifth Korotkoff sound was used to determine diastolic blood pressure. For the 2014 follow-up and onwards, an electronic sphygmomanometer (HEM-8102 A; Omron Healthcare, Matsusaka, Japan) was employed. SBP-mean refers to the average of all SBP measurements obtained before the carotid ultrasound measurements. SBP-TTR, denoting the percentage of time that SBP falls within the target range of 120–140 mmHg based on prevailing guidelines, was estimated using linear interpolation method11,16.
Carotid artery ultrasound measurements
The examination was conducted by experienced physicians, each with over 5 years of expertise, utilizing a Philips HD-15 color ultrasonic diagnostic instrument (with a probe frequency of 5–12 MHz) following uniform calibration, while the patients were lying supine with their heads slightly inclined backward. Both long-axis and short-axis scans were used to detect the carotid arteries, encompassing the common carotid artery, internal carotid artery, and external carotid artery. The measurement of cIMT and CAPs was carried out by a pair of proficient doctors, with one performing the examination and the other recording the findings. Subsequently, the examination results underwent review by two independent operators, and any discrepancies in evaluation were resolved through consensus. cIMT is recorded as the average of the maximum values obtained from three repeated measurements on both the left and right common carotid arteries. The standardized measurement methods were applied as previously documented. In this study, cIMT was defined and measured following the Mannheim Carotid Intima-Media Thickness and Plaque Consensus (2004–2006–2011)17. CAPs were defined as local bulges protruding from the lumen of the artery by 0.5 mm or exceeding 50% of the cIMT, or when the cIMT was greater than 1.5 mm.
Statistical analysis
Continuous and normal distribution data were expressed as mean ± standard deviation (SD), while skew distribution measurement data were expressed as medians and interquartile ranges. Categorical data were expressed as counts and percentages. The participants were divided into four groups according to SBP-TTR (0% to < 25%, 25% to < 50%, 50% to < 75%, 75–100%). The comparison of means was conducted using the t-test, counts and proportions were compared using the χ2 test or the Fisher exact test. The comparison of medians was made using the Wilcoxon rank-sum test. The Logistic regression model was used to evaluate the relationship between TTR and CAPs, while multivariate linear regression model was used to estimate the relationship between TTR and cIMT. Both models were adjusted for potential confounders: model 1 was adjusted for age and sex, and model 2 was further adjusted for baseline SBP, BMI, LDL-c, HDL-c, FBG, hs-CRP, eGFR, smoking, drinking, exercising, antihypertensive drugs, glucose-lowering drugs, lipid-lowering drugs, and educational status.
To investigate the influence of different population characteristics on the association between SBP-TTR with cIMT and CAPs, this study examined the multiplicative interaction effect of one SD increase of SBP-TTR and age (< 60 years, ≥ 60 years), BMI (< 24 kg/m2, ≥ 24 kg/m2), gender and antihypertensive therapy on cIMT and CAPs through the use of odds ratios (ORs) and 95% confidence interval (CI).
To verify the robustness of the results, we conducted several sensitivity analyses. First, we added SBPmean to the fully adjusted model to determine whether the association between SBP‑TTR and outcomes was independent of average SBP. Second, we excluded participants receiving lipid‑lowering or glucose‑lowering therapy to eliminate potential pharmacological confounding. Third, we redefined the target SBP range as 110–130 mmHg and repeated the analyses. Fourth, we removed individuals with fewer than five BP measurements to assess the influence of measurement frequency. Fifth, we incorporated the duration of SBP‑TTR exposure into the fully adjusted model to account for differences in exposure periods. Sixth, we refined smoking status into three categories (current, former, and never smoker) to explore the effect of smoking behavior. Finally, we substituted the last BP measurement during the exposure period for the baseline value in a correction analysis. Statistical analysis was performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA) and Stata software version 16 (Stata Corp, College Station, TX). All p values were two-sided, with p < 0.05 considered statistically significant.
Results
Among the 7738 subjects at baseline, the mean age was 56.33 ± 10.64 years, with 6352 males (82.09%). All participants underwent multiple blood pressure measurements before carotid ultrasound examination, with a median of 4(3,4) measurements. The SBP-mean during the exposure period was 143.38 ± 14.01 mmHg, and the final SBP measured at the end of the exposure period was 146.86 ± 18.87 mmHg. The median cIMT was 0.90 (0.80, 1.00) mm. CAPs were detected in 930 patients (12.02%). Table 1 presents the baseline characteristics of participants categorized by SBP-TTR quartiles. The eGFR concentration, the proportions of current smokers, drinkers, and percentage of high school education or above increased with higher levels of SBP-TTR (p < 0.001). Conversely, there is a decreasing trend in the mean age, concentration of hs-CRP, cIMT level, CAPs detection rate, proportion of diabetes mellitus, and the prevalence of hypertension and diabetes treatment from the low-level group to the high-level group (p < 0.05).
Association between SBP-TTR with caps and cIMT
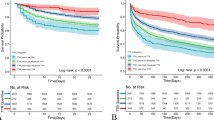
After adjusting for confounding factors in Logistic regression models, compared to the TTR < 25% group, the incidence rates of CAPs were lower in the 25% ≤ TTR < 50%, 50% ≤ TTR < 75%, and TTR ≤ 75% groups (0.824 [95% CI 0.663 to 1.020], 0.882 [95% CI 0.703 to 1.102], 0.766 [95% CI 0.588 to 0.993]). Each 1-SD increase in SBP-TTR was associated with a 10.6% decrease in the risk of CAPs (0.894 [95% CI 0.814 to 0.982]) (Table 2).
In generalized linear regression models, compared to the TTR < 25% group, the cIMT was thinner in the 25% ≤ TTR < 50%, 50% ≤ TTR < 75%, and TTR ≤ 75% groups (− 0.006 mm [95% CI − 0.033 to 0.021 mm], − 0.014 mm [95% CI − 0.042 to 0.014 mm], − 0.048 mm [95% CI − 0.078 to − 0.018 mm]). Additionally, each 1-SD increase in SBP-TTR was associated with a statistically significant decrease in cIMT by 0.018 mm (95% CI − 0.029 to − 0.006) (Table 3).
Subgroup analysis
The subgroup analysis revealed a significant age-dependent correlation between SBP-TTR and cIMT (P for interaction = 0.029). Among individuals aged < 60 years, cIMT decreased by 0.021 mm per one standard deviation increase in SBP-TTR (95% CI − 0.039 to − 0.002), whereas among those aged > 60 years, cIMT decreased by 0.007 mm (95% CI − 0.014 to 0). Besides, although not statistically significant based on the interaction test, CAPs were significantly associated with SBP-TTR in females, participants who were not receiving antihypertensive medications, individuals with a BMI < 24 kg/m2, and those aged ≥ 60 years. cIMT was statistically associated with SBP-TTR in males, participants with a BMI < 24 kg/m2, and those without antihypertensive drug intake. Detailed associations are provided in Supplementary Tables 1 and 2.
Sensitive analysis
The negative correlation between SBP-TTR and CAPs and cIMT remained statistically significant even after adjusting for the duration of the SBP-TTR exposure period, refining smoking status into three categories, excluding individuals taking antidiabetic and lipid-lowering medications, as well as those with fewer than 5 blood pressure recordings. Setting the target SBP control range at 110–130 mmHg, our findings indicated a 12.2% decrease (95% CI 0.773 to 0.994) in the odds of CAPs occurrence and a 0.022 mm decrease (95% CI − 0.036 to − 0.008 mm) in cIMT per one SD increase in SBP-TTR. However, after adjusting for SBP-mean in the model, SBP-TTR did not exhibit a significant association with either CAPs or cIMT (Supplementary Table 3).
Discussion
In this community-based cross-sectional study, we identified a notable inverse correlation between SBP-TTR and carotid atherosclerosis among hypertensive individuals. This association remained statistically significant after adjusting for traditional risk factors, including baseline SBP. Moreover, we observed that this relationship was influenced by age, sex, and BMI factors.
Our primary finding reveals a negative association between SBP-TTR and carotid atherosclerosis in hypertensive individuals. Firstly, we observed lower CAPs risk across all three groups compared to the SBP-TTR < 25% group. Specifically, the SBP-TTR 75% group exhibited a statistically significant 24% reduction in risk. Additionally, for each SD increase in SBP-TTR, the risk of CAPs decreased by 11%. Secondly, linear regression analysis demonstrated a gradual decrease in cIMT with increasing SBP-TTR. Compared to the SBP-TTR < 25% group, cIMT in the SBP-TTR 75% group decreased by 0.048 mm. For every SD increase in SBP-TTR, cIMT decreased by 0.018 mm. These associations remained after adjusting for confounding factors, including baseline SBP. These results suggest that the relationship between SBP-TTR and carotid atherosclerosis is independent of baseline SBP. Therefore, clinical attention should focus not only on achieving standard blood pressure values in hypertensive patients18,19 but also on maintaining a high proportion of time within those standards. Effective, continuous, and stable blood pressure control may offer hypertensive patients greater benefits in terms of CAPs and cIMT.
We identified an interaction between age and the relationship between SBP-TTR and cIMT. Our findings indicate a stronger correlation between SBP-TTR and cIMT in individuals aged < 60 years (P for interaction = 0.029). This could be attributed to younger individuals maintaining better vascular function early in the atherosclerotic process, thereby being more responsive to blood pressure control. Consistent with our results, data from the Women’s Health Study have shown significant age-related effects on most cardiovascular risk factors and biomarkers, with the association with ASCVD weakening as age increases20. However, we observed no age-related differences in the association between SBP-TTR and CAPs. The development of CAPs represents an advanced stage of cIMT progression, reflecting long-term pathological processes such as lipid deposition, inflammatory responses, and vascular remodeling21,22. At this stage, the benefits of blood pressure control may not significantly differ across age groups, despite potential similarities in vascular function and pathology. Moreover, our classification using a 60-year age cutoff may not sufficiently demonstrate the varying response of carotid atherosclerosis to blood pressure control across different age groups23. However, limited by population characteristics, we were unable to analyze the correlation between SBP-TTR and cIMT and CAPs in younger age groups. Future investigations should consider finer age groupings to improve result sensitivity and specificity. Furthermore, despite the absence of interaction, given that older age, male sex, and higher BMI are established risk factors for atherosclerosis, we conducted additional subgroup analyses. These revealed a stronger association between SBP-TTR and CAPs in women aged over 60 years with BMI less than 24 kg/m2, whereas the association with cIMT was more pronounced in men with BMI ≥ 24 kg/m2. Additionally, no significant interaction was observed between SBP-TTR and antihypertensive medication use. However, a stronger association between SBP-TTR and CAPs/cIMT was found among participants who were not receiving antihypertensive medications. The reasons for this disparity require further discussion, potentially linked to variations in the severity of carotid atherosclerosis across diverse populations and differences in their response to SBP-TTR.
In recent years, studies have demonstrated that intensive blood pressure-lowering strategies can provide additional benefits for hypertensive individuals24,25. Building on this, we defined a target SBP control range of 110–130 mmHg. Our findings indicate that SBP-TTR exhibits a stronger negative correlation with CAPs under strict blood pressure control. This suggests that SBP-TTR could serve as a predictor for progress in CAPs and cIMT within stringent blood pressure management. Intensive blood pressure reduction may thus delay subclinical vascular disease in hypertensive patients. Future intervention studies should explore the comparative benefits of intensive versus standard antihypertensive strategies on CAPs and cIMT to optimize clinical management for hypertensive patients. Additionally, we observed that mean SBP levels influenced the association between SBP-TTR and CAPs/cIMT. This is consistent with findings by Buckley11, indicating that adjusting for mean SBP attenuates the relationship between SBP-TTR and cardiovascular disease and chronic kidney disease risks. We speculate that this could be due to the strong collinearity between SBP-mean and SBP-TTR, as both variables reflect similar blood pressure information to some extent. Therefore, it is important to consider both SBP-mean and SBP-TTR when evaluating blood pressure control. Additionally, it is possible that, during the long-term follow-up with regular health check-ups, participants received guidance from physicians, which could have helped to control their blood pressure fluctuations. As a result, SBP-mean may have emerged as another useful predictor, diminishing the additional contribution of SBP-TTR to the outcomes. In conclusion, although SBP-TTR, as an intuitive indicator of SBP control, shows its potential value, its predictive value compared to SBP-Mean still needs further research and verification.
This study presents several significant advantages. Firstly, we identified, for the first time, the relationship between SBP-TTR, CAPs, and cIMT, filling a critical research gap and providing a foundational reference for future studies in this area. Secondly, through simultaneous evaluation of CAPs and cIMT, we provided a comprehensive assessment of atherosclerosis severity, contributing to a deeper understanding of how hypertension influences atherosclerosis mechanisms. Lastly, we adjusted for numerous covariates to minimize residual confounding, enhancing the reliability of our findings. The clinical implications of our results are significant. In the management of hypertension, maintaining a relatively stable SBP over the long term may help prevent atherosclerosis, providing a novel basis for early intervention and preventive strategies. Our study also has several limitations. Firstly, it is a cross-sectional study, which precludes the establishment of causality. Secondly, the TTR in hypertensive patients with different comorbidities may exhibit variability. Our study lacked a sufficient sample size for subgroup analysis. Thirdly, potential differences in blood pressure measurements between follow-up visits may affect the TTR calculated by linear interpolation. However, the Kailuan study followed a strict standardized protocol for blood pressure measurement designed to minimize variability during long-term follow-up. Fourth, a relatively long measurement interval (2 years) may introduce inaccuracies in TTR estimation. Therefore, future studies should consider shorter intervals, such as 24-h measurements, to further enhance the robustness of these findings. Fifth, because each participant had only a single carotid ultrasound measurement, we were unable to evaluate longitudinal changes in cIMT or CAP in relation to SBP‑TTR. Future prospective studies with serial carotid imaging are warranted to determine whether SBP‑TTR predicts progression of carotid atherosclerosis over time. Finally, the study participants were exclusively drawn from the Kailuan study cohort, necessitating validation in other populations.
In conclusion, this study demonstrates a significantly negative correlation between SBP-TTR and carotid atherosclerosis among hypertensive individuals. This association is independent of conventional risk factors such as baseline SBP and shows dependence on age, sex, BMI, and antihypertensive therapy. Effective management to stabilize blood pressure within normal ranges could reduce cardiovascular risks in hypertensive patients.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Liu, Y. et al. Influence of management of intensive weight, blood pressure, and lipids on disease severity in patients with carotid atherosclerosis. Altern. Ther. Health Med. 29, 174–179 (2023).
Xie, W. et al. Five-year change in systolic blood pressure is independently associated with carotid atherosclerosis progression: A population-based cohort study. Hypertens. Res. 37, 960–965 (2014).
Fuchs, F. D. & Whelton, P. K. High blood pressure and cardiovascular disease. Hypertension 75, 285–292 (2020).
Worldwide trends in. Hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 398, 957–980 (2021).
The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Interpretation of report on cardiovascular health and diseases in China 2022. Chin. J. Cardiovasc. Med. 28, 297–312 (2023).
Mancusi, C. et al. Carotid atherosclerosis predicts blood pressure control in patients with hypertension: The campania salute network registry. J. Am. Heart Assoc. 11, e022345 (2022).
Doumas, M. et al. Time in therapeutic range, as a determinant of all-cause mortality in patients with hypertension. J. Am. Heart Assoc. 6 (2017).
Muntner, P. et al. Trends in blood pressure control among US adults with hypertension, 1999–2000 to 2017–2018. JAMA 324, 1190–1200 (2020).
Fatani, N., Dixon, D. L., Van Tassell, B. W., Fanikos, J. & Buckley, L. F. Systolic blood pressure time in target range and cardiovascular outcomes in patients with hypertension. J. Am. Coll. Cardiol. 77, 1290–1299 (2021).
Li, S. et al. Systolic blood pressure time in target range and cognitive outcomes: Insights from the SPRINT. MIND Trial Hypertens. 80, 1628–1636 (2023).
Buckley, L. F. et al. Systolic blood pressure time in target range and major adverse kidney and cardiovascular events. Hypertension 80, 305–313 (2023).
Huang, R. et al. Time in target range for systolic blood pressure and cardiovascular outcomes in patients with heart failure with preserved ejection fraction. J. Am. Heart Assoc. 11, e022765 (2022).
Wu, S. et al. Prevalence of ideal cardiovascular health and its relationship with the 4-year cardiovascular events in a Northern Chinese industrial City. Circ. Cardiovasc. Qual. Outcomes. 5, 487–493 (2012).
Zheng, X. et al. Association between cumulative exposure to ideal cardiovascular health and arterial stiffness. Atherosclerosis 260, 56–62 (2017).
Teo, B. W. et al. GFR estimating equations in a multiethnic Asian population. Am. J. Kidney Dis. 58, 56–63 (2011).
Zhang, Y. et al. Time in target range for systolic blood pressure and glucose with cardiovascular disease and all-cause mortality risks. Hypertens. Res. 48, 256–272 (2025).
Touboul, P. J. et al. Mannheim carotid intima-media thickness and plaque consensus (2004-2006-2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc. Dis. 34, 290–296 (2012).
Nwabuo, C. C. et al. Long-term blood pressure variability in young adulthood and coronary artery calcium and carotid intima-media thickness in midlife: The CARDIA study. Hypertension 76, 404–409 (2020).
Ferreira, J. P. et al. Intima-media thickness is linearly and continuously associated with systolic blood pressure in a population-based cohort (STANISLAS cohort Study). J. Am. Heart Assoc. 5 (2016).
Dugani, S. B. et al. Association of lipid, inflammatory, and metabolic biomarkers with age at onset for incident coronary heart disease in women. JAMA Cardiol. 6, 437–447 (2021).
Cheng, H. et al. Effects of shear stress on vascular endothelial functions in atherosclerosis and potential therapeutic approaches. Biomed. Pharmacother. 158, 114198 (2023).
Pewowaruk, R. J. et al. Carotid artery stiffness mechanisms associated with cardiovascular disease events and incident hypertension: The multi-ethnic study of atherosclerosis (MESA). Hypertension 79, 659–666 (2022).
Age-stratified and. blood-pressure-stratified effects of blood-pressure-lowering pharmacotherapy for the prevention of cardiovascular disease and death: An individual participant-level data meta-analysis. Lancet 398, 1053–1064 (2021).
Xie, X. et al. Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: Updated systematic review and meta-analysis. Lancet 387, 435–443 (2016).
Dolui, S. et al. Association of intensive vs standard blood pressure control with cerebral blood flow: Secondary analysis of the SPRINT MIND randomized clinical trial. JAMA Neurol. 79, 380–389 (2022).
Acknowledgements
The authors thank all the participants of the Kailuan Study and those who contributed their information to the present study.
Funding
This study was supported by the Clinical Research Project of Health Consortium (ynlglht202402), Scientific Research Foundation of SUMHS (SSF-23-14-002), and Hebei Provincial Health and Health Commission key scientific and technological research project (20231856).
Author information
Authors and Affiliations
Contributions
Wen Li and Zhiran Liu carried out the studies, participated in collecting data, and drafted the manuscript. Jianqiu Zhao and Shuohua Chen participated in the statistical analysis. Shouling Wu, Wei Huang and Xuemei Liu helped with revising the manuscript. Yuxia Gao and Shouling Wu designed the outline of the topic and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Kailuan General Hospital [(2006) Approval No. 5]. The patients provided their written informed consent to participate in this study. We confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, W., Liu, Z., Zhao, J. et al. Association of systolic blood pressure time in target range with carotid atherosclerotic plaque and carotid intima-media thickness in hypertensive patients. Sci Rep 15, 17347 (2025). https://doi.org/10.1038/s41598-025-01217-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-01217-6
