
Abstract
We investigated the differences in binocular vision function and visual fatigue between school-aged children with myopic anisometropia and those with myopic isometropia. It also examined the correlation between myopic anisometropia and binocular vision parameters. One hundred school-aged (ages 6–13 years) children (43 boys and 57 girls) were divided into two groups: the myopic anisometropia group (interocular spherical equivalent difference ≥ 1.50 and < 4.00 D) and the myopic isometropia group as control group (interocular spherical equivalent difference < 1.00 D). Binocular vision parameters related to accommodation were analyzed, including accommodative amplitude, flexibility, relative accommodation, and convergence flexibility. Differences in visual fatigue scores between groups were also evaluated. Patients with myopic anisometropia show significant binocular visual dysfunction, including reduced accommodation amplitude, accommodative facility, and vergence facility, with a compensatory increase in positive relative accommodation. Although negative relative accommodation was similar between groups, anisometropic patients had more severe visual fatigue (higher ASQ-11 scores). In myopic patients without anisometropia, visual fatigue was mildly negatively correlated with accommodative facility. Clinically, binocular accommodation and vergence function should be carefully assessed in myopic patients, especially those with anisometropia, and visual fatigue interventions should include training of accommodative and vergence facility to enhance visual quality.
Similar content being viewed by others
Introduction
Anisometropia refers to a significant difference in refractive power between the two eyes in one or more main meridians, with an interocular spherical equivalent difference of 1.50 D or more1. Various factors, including genetics, gender, age, environmental factors, education level, and ethnicity, can influence the development of anisometropia2. Anisometropia exceeding 2.50 D disrupts binocular fusion, impairing the brain’s ability to integrate disparate retinal images into a coherent stereoscopic perception. This breakdown in binocularity manifests clinically as diplopia, visual fatigue, and dyslexia-related symptoms, significantly compromising patients’ quality of life and cognitive performance3,4. The pathophysiology involves a hierarchical cascade of neural adaptations: once the interocular spherical equivalent difference surpasses fusion thresholds (spherical difference ≥ 1.50D or cylindrical ≥ 1.00D), a consequential retinal image disparity exceeding 5% triggers synaptic plasticity-mediated suppression of the defocused eye’s input5,6,7. If left untreated, prolonged suppression of the weaker eye can lead to anisometropic amblyopia, with approximately one-third of cases progressing to strabismus due to irreversible reorganization of binocular integration pathways.
Zhuang et al. previously grouped myopic anisometropia in 8–15 year old children by degree of anisometropia to analyze the accommodative and binocular visual function8. This clinical study was more descriptive, but did not delve into the relationship between anisometropia and visual fatigue. In recent years, the prevalence of myopia among school-aged children in China has increased sharply, with an earlier onset and faster progression9,10. Therefore, in this study, we focused on school-age (6–13 years old) children with minimal age variation and rapid myopia progression. We not only confirm the impact of anisometropia on binocular visual dysfunction but also establish a clear correlation between binocular vision parameters and visual fatigue. By translating these theoretical findings into clinical practice, our study provides new guidance for individualized management of anisometropia-related asthenopia. Specifically, the strong association between convergence flexibility and visual fatigue suggests that targeted vision therapy and optical interventions may help alleviate symptoms, offering a more precise and symptom-driven approach to managing anisometropia in children.
Results
Population
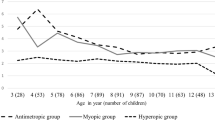
A total of 100 eligible participants were enrolled, of whom 50 participants were in the myopic anisometropia group, the mean age was 10.4 ± 1.8years. 50 participants were in the myopic isometropia group (the control group), the mean age was 9.4 ± 2.0years. No significant difference was found in age or sex among the two groups (Respectively, P = 0.062, P = 0.725). And the cylinder values were generally low in both groups. In the anisometropia group, the median cylinder was − 0.50 D for the right eye and − 0.50 D for the left eye. In the control group, the median cylinder was − 0.25 D for the right eye and − 0.50 D for the left eye. The low astigmatism in both groups were unlikely to have significantly influence on our findings regarding binocular vision function and visual fatigue. However, significant differences were found in spherical equivalent refraction (P = 0.026). The demographics of the participants in the two groups are detailed in (Table 1).
Comparison of the accommodation-related binocular function parameters between groups
The accommodative amplitude (AMP), accommodative facility (AF), and convergence facility (CF) of the myopic anisometropia group were significantly lower than those of the control group. There was no significant difference in negative relative accommodation (NRA) between the two groups (see Table 2).
Comparison of the results of the ASQ-11 between the two groups
The ASQ-11 score in the anisometropia group was significantly higher than that in the control group (see Table 2).
Correlation analysis of visual fatigue parameters and accommodation-related binocular visual function parameters
Coefficients were calculated for the two groups, and the results showed that the scores of the ASQ-11 in both groups were negatively correlated with the convergence flexibility to a medium to high degree (P < 0.001). ASQ-11 scores in both the myopic anisometropia group and the control group were significantly negatively correlated with convergence facility (see Table 3).
Discussion
Previous studies have consistently reported that anisometropia can disrupt binocular vision by impairing fusion, stereopsis, and vergence function. Research by Horwood and Riddell highlighted that anisometropia, particularly in myopic patients, is associated with reduced accommodative accuracy and vergence stability11. Similarly, Chen et al. found that myopic anisometropia contributes to decreased accommodative amplitude and facility, reinforcing the notion that accommodative control is compromised in these individuals12. Our study extends these findings by demonstrating that myopic anisometropia can not only reduce accommodative facility but also negatively affect convergence flexibility, which has been less frequently examined in prior research. This underscores the broader impact of myopic anisometropia on dynamic binocular vision function beyond what has been previously documented. Sheedy et al. established that symptoms of asthenopia are frequently associated with vergence instability and reduced accommodative function13. Zhuang et al. primarily focused on accommodative and binocular vision function in children with myopic anisometropia but did not explore its relationship with visual fatigue. Our study provides new insights by revealing that visual fatigue scores are significantly correlated with convergence flexibility in the myopic anisometropia group (P < 0.001), highlighting a specific mechanistic relationship that has not been emphasized in earlier studies.
In this study, we observed and compared parameters related to binocular vision function in myopic school-age children with and without anisometropia and found differences between groups, indicating that anisometropia impairs binocular vision function. Positive relative accommodation reflects the eye’s ability to mobilize and adjust during near vision, while negative relative accommodation reflects the eye’s ability to relax. In this study, participants in the myopic anisometropia group showed decreased accommodative amplitude and positive relative accommodation, potentially due to the fact that the myopic eye with higher refraction at near view used less or no accommodation to see clearly because of the closer near point, and at distance, the eye with lower power was used to see the distance. A small positive relative accommodation indicates insufficient, non-durable accommodation. The accommodative facility responds to the speed at which the eye switches focus between near and far objects. Reduced accommodative facility the eye’s diminished ability to swiftly adjust focus between different distances-can lead to blurred vision at both near and far ranges, difficulty maintaining clear vision, and may contribute to the progression of myopia. Individuals with reduced accommodative facility often experience delays when shifting focus between near and distant objects, resulting in transient blurred vision and challenges in sustaining clear vision. Logan et al. found that myopic children exhibited slower accommodative responses compared to their emmetropic peers, indicating a lag in the eye’s focusing mechanism14. These findings underscore the importance of assessing and managing accommodative function, particularly in individuals at risk for or experiencing myopia, to maintain visual clarity and potentially mitigate progression of myopia. Moreover, while accommodative facility has been previously linked to visual fatigue in general populations15, our study establishes this correlation specifically in the control group, suggesting that the interplay between accommodation and fatigue may differ between individuals with and without anisometropia.
Reduced accommodative facility requires a buffering period to switch focus, resulting in blurred vision for both near and distant objects, difficulty maintaining clear vision, and an increased risk of myopia progression. To avoid binocular fusion difficulty, a monocular viewing strategy develops, where the eye with higher refractive error is used for near vision, and the eye with lower refractive error is used for distance vision. This reduces visual fatigue symptoms but results in loss of normal binocular single vision. We found that the incidence of binocular vision dysfunction in patients with myopic anisometropia was higher than the control group. These dysfunctions manifest as reduced accommodation amplitude, diminished accommodative facility, and decreased convergence facility.
The anisometropic group showed less accommodative facility and convergence facility compared to the control group. In addition, in-depth analysis of the results of the visual function examination revealed that the lack of accommodative facility in the myopic anisometropia group mostly manifested as difficulty in passing through the negative lens, which could be diagnosed as insufficient accommodation combined with a decrease in binocular accommodative amplitude. When accommodation is insufficient, the eye cannot focus images behind the retina onto the retina itself, creating a state of hyperopic defocus that leads to choroidal thinning and axial lengthening, accelerating myopia progression.
In this clinical observation, the total score of the visual fatigue scale in the myopic anisometropia group was higher than that in the control group, and the total score of the visual fatigue scale in both groups was highly negatively correlated with convergence flexibility. Within a certain range (< 5%), central fusion can compensate for disparities to achieve binocular single vision. However, if the difference exceeds compensatory ability, it leads to difficulties in binocular fusion. This results in different accommodative demands for the eyes while viewing, requiring constant accommodation and coordination of the ocular muscles. Prolonged tension in these muscles can induce symptoms of visual fatigue, such as eye soreness and pain, impacting the patient’s daily life and learning.
Visual discomfort constitutes a neurophysiological dysregulation syndrome in which suboptimal visual stimuli induce 3 clinical manifestations: (1) sensory-perceptual abnormalities (photophobia, blurred vision, contrast sensitivity fluctuations), (2) ocular surface dysfunction (tear film instability, accommodative spasm), and (3) neurogenic symptoms (frontal cephalgia, visual motion intolerance). Pathophysiologically, this stems from disrupted accommodative-vergence integration, trigeminovascular activation, and cortical hyperexcitability, with symptom severity correlating with exposure to triggering factors including prolonged near-work (> 45 min), high spatial frequency patterns (> 3 cycles/degree), or aberrant illumination (≤ 100 lx or ≥ 1000 lx). Visual quality is a comprehensive evaluation of optical performance, integrating both subjective perception and objective measurements of optical clarity (visual acuity, contrast sensitivity), focusing dynamics (depth of focus, accommodation accuracy), and neural processing efficiency (glare sensitivity, aberration tolerance). High visual quality means sharp, clear, and comfortable vision across different lighting and focusing conditions, while poor visual quality may result from optical imperfections, higher-order aberrations, or ocular pathology. Patients with myopic anisometropia need optometrists to develop personalized refractive correction. Reasonable optical correction can ameliorate visual discomfort and improve visual quality; it can also reduce the imbalance of accommodative function between the two eyes16. The principle of orthokeratological refractive correction is based on nocturnal wearing of a lens with a reverse geometric design to apply precise pressure to the central area of the cornea, while raising the curvature of the cornea in the middle, and thereby temporarily reshaping it17. The process is reversible, and the cornea gradually returns to its original state after stopping wearing of the lens, so the effect needs to be maintained at night (the correction amount is about 0.50D ~ 6.00D). Its optical advantage is that the orthokeratology lens does not need to be worn during the day, and the peripheral defocus design may have the effect of controlling the myopia (evidence level I). The orthokeratology lens accurately regulates the corneal shape of both eyes through an inverse geometric design, and achieves personalized shaping for anisometropia (spherical lens difference ≥ 1.50D), effectively avoiding the burden of image fusion caused by the unequal frame image (> 5%). It acts directly on the optical region of the cornea, eliminating prism effects and aberrations caused by lens thickness differences, significantly improving visual quality and reducing visual fatigue. The fluid mechanics of tears ensures that the correction force is evenly distributed and the correction balance of both eyes is maintained. Peripheral defocus design simultaneously delays ocular axis growth, controls anisometropia progression, and promotes the reconstruction of binocular fusion function by stabilizing naked eye vision, especially in children; it significantly reduces the risk of monocular suppression, and realizes the dual benefits of optical correction and visual function improvement. A longitudinal study showed that the rate of myopia progression in each eye of children with myopic anisometropia was higher than that of the control group18. Therefore, for children with myopic anisometropia, orthokeratology is an ideal refractive correction method19,20,21,22; it can provide children with good unaided visual acuity and effectively control myopia progression, axial elongation, and anisometropia development16,19,23. Furthermore, it can prevent binocular vision dysfunction and visual fatigue24.
The eye’s accommodative function is crucial to maintain normal vision and visual function and is a prerequisite for clear, comfortable, and long-lasting visual quality25. For school-age children with myopic anisometropia, personalized accommodative function training (training improves accommodative lag using Flipper), VR training reshapes visual neural circuits through dichoptic stimulation; 3D vision training enhances stereopsis via disparity tasks. Previous studies have shown that insufficient accommodation, or low accommodative facility not conducive to myopia prevention and control26.
The strong correlation between visual fatigue and convergence flexibility suggests that specific vision therapy protocols focusing on vergence flexibility may be beneficial for patients with myopic anisometropia. Additionally, given the heightened risk of binocular dysfunction, optometrists should consider early correction strategies and possibly enhanced accommodative or vergence training to mitigate long-term visual discomfort.
Most cases of anisometropia are influenced by acquired developmental factors of refractive error, including bad eye behavior habits such as incorrect eye habits and reading postures, which deepen refractive error and increase anisometropia27,28,29. Therefore, for refractive correction of school-age patients with myopic anisometropia, it is necessary to consider the comfort of wearing glasses and the effect of myopia prevention and control; doing a good job in science education to cultivate good eye behavior habits is also very important.
In this clinical observation, the binocular vision function of school-age children with myopic anisometropia was innovatively examined, and differences were found between myopic school-age children with anisometropia and those without anisometropia in accommodative function–related parameters, such as accommodative amplitude, accommodative facility, positive relative accommodation, and convergence flexibility, where levels were lower in children with anisometropia compared with those without (control group). Therefore, in the diagnosis and treatment of myopia prevention and control, it is recommended that patients with myopic anisometropia complete the visual fatigue questionnaire to enhance their cognition of visual fatigue. Moreover, doctors should diagnose patients’ fatigue and intervene early to reduce the distress caused by visual fatigue in life and study. This will provide new ideas for clinical diagnosis and treatment.
Despite strengths, this clinical observation had several limitations. Firstly, the number of participants was small, and patients with high myopic anisometropia were lacking. Secondly, horizontal fusion range, accommodation convergence/accommodation(AC/A) and stereoscopic vision were not measured. Thirdly, because of the limited precision of detection equipment for flexibility of accommodation and selection of gradient and vision standard, the inspection distance was 2.22 times the accommodation near point, and the total inversion lens was 30% of the accommodation amplitude. We will expand the sample size, refine binocular visual function test items, and improve the precision of visual function testing equipment in future work.
Methods
Inclusion and exclusion criteria
Inclusion criteria
Participants were enrolled if they had binocular corrected visual acuity of 1.0 or above and were aged 6–13 years.
-
(a)
Myopic anisometropia group: Both eyes were myopic (compound myopic anisometropia) or one eye was emmetropic and one eye was myopic (simple myopic anisometropia), with an equivalent spherical diopter >-0.25 DS, and 1.00 DS ≤ the difference in the equivalent spherical power of both eyes < 2.50 DS.
-
(b)
Myopic isometropia group(control group): This group had binocular myopia or one eye with emmetropia and one eye with myopia, with an equivalent spherical diopter > -0.25 DS, and interocular difference < 1.00 DS.
-
(c)
Myopia progresses rapidly, with an annual increase of ≥ 0.75diopters.
Exclusion criteria
Participants with ocular surface diseases, strabismus, amblyopia, nystagmus; a history of previous eye trauma; or ophthalmic surgery, as determined through inquiry into clinical symptoms, slit-lamp examination and direct ophthalmoscopy, were excluded. Those who could not cooperate with the examination were also excluded.
Participants
Before the implementation of the study, the experimenter introduced the purpose, content and all possible consequences of the study to the participants and their parents in detail, and obtained signed informed consent of each subject and their parents. This study was conducted as a sub-analysis of the broader Shenzhen Science and Technology Program project.This study complies with the Declaration of Helsinki and was approved by the Ethics Committee of Shenzhen People’s Hospital. This part of the study has completed clinical trial registration.
School-aged children (6–13 years old) undergoing medical optometry in the Department of Ophthalmology of Shenzhen People’s Hospital from August 2023 to August 2024 were included in this study. After applying the inclusion and exclusion criteria, 100 cases with 200 eyes were enrolled. Using equivalent spherical power (spherical power + 1/2 cylindrical power), participants were divided into a myopic anisometropia group and a control group. The myopic anisometropia group included 50 cases with 100 eyes, of which 23 were boys and 27 were girls, with an average age of 10.4 ± 1.9 years. The control group included 50 cases with 100 eyes, of which 20 were boys and 30 were girls, with an average age of 9.4 ± 2.0years.
All enrolled participants underwent retinoscopy under cycloplegia to determine refraction. According to the participant’s refraction results, the corresponding prescription was attached to the automatic phoropter. Visual function examination items included accommodation amplitude (AMP), positive/negative relative accommodation (PRA/NRA), accommodative facility (AF), and convergence facility (CF).
Our study utilized Tropicamide and Phenylephrine eye drops (specification: 5 mg tropicamide and 5 mg deoxyadrenaline per ml) as the cycloplegic agent. Participants were placed in a supine position, and eye drops were dropped into the conjunctival sac of their lower eyelid, with 1 drop in each eye. The administration was repeated 3 times, 5 min apart. The lacrimal sac area was pressed continuously for 2 min after each administration to reduce the risk of systemic absorption. The effect of mydriasis was evaluated 30 min after the final dose. When the pupil diameter was ≥ 6 mm and the light reflex was absent, refractive examination could be performed. Residual accommodation after mydriasis (about 1.00D) may affect accommodative facility tests (such as Flipper tests). Therefore, the evaluation of binocular vision function (e.g. stereoscopic vision, fusion range) was performed 24 h after mydriasis to ensure data accuracy.
Accommodative amplitude (AMP)
The amplitude of accommodation is the difference in refractive power between the distant and near points of fixation, also known as the maximum accommodative force. Based on refractive correction, the modified proximity method was used to measure each eye separately. With one eye occluded, the other was tested using a phoropter. The participant read the smallest line on a near visual acuity chart at 40 cm. The chart was moved closer until letters appeared blurred. The closest distance before blurring was recorded. If the distance was less than 8 cm, a negative lens was added in front of the tested eye, in -0.25D increments, until letters became blurred. The power of the negative lens was recorded, and the accommodative amplitude calculated as 12.50 D plus the added lens power. Each eye was measured three times, and the average value recorded.
Positive/negative relative accommodation (PRA/NRA)
Near vision (40 cm) charts on the automatic phoropter were used, with full correction of the eyes. The participant was required to fixate on the 20/30 target, and the positive lens was gradually added in front of the participant’s eyes in + 0.25 D increments until the target began to appear persistently blurred. The maximum positive lens added before blurring occurred was recorded as the NRA value. The PRA measurement process was similar to the NRA measurement process after completion of accommodative response measurement. Again, it was ensured the patient’s visual target was clear, and the negative lens was gradually increased in front of the patient’s eyes, each time by −0.25 D, until fixation of the optometric target became persistently blurred. The increased negative power was then recorded, representing the PRA value.
Accommodative facility (AF)
Based on refractive correction, participants were instructed to fixate on a 20/30 target at 40 cm. Monocular examination was followed by bilateral examination. For monocular examination, one eye was occluded while the other was tested using a ± 2.00D flipper. Participants were asked to focus on the target as clearly and quickly as possible. Timing began when the flipper was first flipped, and each time the participant reported the target became clear, the flipper was immediately reversed. This process was repeated until two accommodative stimuli had been completed. The number of cycles completed in 1 min was recorded as cycles per minute (cpm). Binocular examination was performed in a binocular fixation state, and the measurement and recording method was the same as the monocular method. Results were recorded as: (1) 0 cpm if the participant could not maintain a clear visual target, indicating difficulty with both positive and negative lenses; (2) 0 cpm if the participant could not maintain a clear visual target at + 2.00 D, indicating difficulty with positive lenses; and (3) 0 cpm if the participant could not maintain a clear visual target at -2.00 D, indicating difficulty with negative lenses.
Convergence facility (CF)
After each participant donned fully corrected glasses, they were instructed to focus on a single 20/30 target at 40 cm. In front of either eye, a 3△BI/12△BO prism reversal paddle was placed, and the participant was required to concentrate and transform a blurred or overlapping target into a clear single target as quickly as possible. In this study, participants signaled the researchers when the target became clear, and the prism was immediately replaced. This process was repeated, and the number of cycles completed within 1 min was recorded (with each completed flip of two prisms counting as one cycle).
Ocular examination
The corneal reflection and occlusion methods were used to check for ocular position examination and squint.
Eye fatigue questionnaire
All participants completed the Census version of the Asthenopia Scale Questionnaire (ASQ-11). The questionnaire includes 11 symptom items, categorized into two dimensions: dimension A (ocular symptom dimension, five items) and dimension B (visual function and systemic symptom dimension, six items). According to the severity of symptoms, each item is awarded 0, 1, 2, 3, or 4 points, corresponding to responses of “None”, “Mild”, “Moderate”, “Relatively severe”, and “Severe”. The total possible score of the questionnaire is 44 points.
Statistical methods
Statistical analyses were performed using SPSS (Statistical Package for the Social Sciences) 24.0. Frequency (rate) was used to describe categorical variables, while mean ± standard deviation was used for numerical variables obeying the normal distribution. The median (with minimum and maximum values) was used for numerical variables that did not obey the normal distribution. The chi-square test compared categorical variables, while the t-test compared numerical variables obeying a normal distribution. Finally, the Wilcoxon rank-sum test compared numerical variables that did not obey a normal distribution. Correlation of normal data was evaluated using the Pearson correlation coefficient, while the Spearman correlation coefficient was used for skewed data.The accommodation-related binocular visual function parameters in both groups did not follow a normal distribution; therefore, the non-parametric Wilcoxon rank sum was performed. The asthenopia scale questionnaire ASQ-11 scores of the two groups also did not follow a normal distribution so the Wilcoxon rank sum test was conducted. Since the visual fatigue parameters and accommodative binocular visual function parameters did not follow a normal distribution, the correlation between these parameters was evaluated by calculating the Spearman correlation coefficient.
Data availability
The original contributions presented in the study are included in the article.
References
Zhong, Y., Zeng, L. & Chen, Z. Ocular anatomical and functional characteristics in anisometropic Chinese children. Optom. Vis. Sci. 98, 476–482 (2021).
Hu, Y. Y. et al. Prevalence and associations of anisometropia in children. Investig. Ophthalmol. Vis. Sci. 57, 979–988 (2016).
Wang, S. Two-dimensional, highresolution peripheral refraction in adults with is myopia and anisomyopia. Investig. Ophthalmol. Vis. Sci. 61, 16–22 (2020).
Krarup, T. G., Nisted, I., Christensen, U. & Kiilgaard, J. F. and M. la Cour. The tolerance of anisometropia. Acta Ophthalmologica. 98, 418–426 (2020).
Liu, M. J. Guan yue-han,Guo Ya-Nan, et al, A study on the relationship between refractive components and stereopsis in chiIdren with anisometropia. Chin. J. Strabismus Pediat. Ophthalmol. 30, 22–25 (2022).
OStadimoghaddam, H. et al. The prevalence of anisometropia in population base study. Strabismus 20, 152–157 (2012).
Smith, E. L. H. & Lf Arumugam B,etal.Observations on the relationship between anisometropia. Amblyopia Strabismus Vis. Res. 134, 26–42 (2017).
Zhuang, C. C., Zhang, L., Pan, S. S., Wang, Y. N. & Guo, J. X. Accommodation and binocular vision in children with myopic anisometropia. J. Ophthalmol. 1, 1–6 (2024).
Wong, C. W., Tsai, A. & Jonas, J. B. Digital screen time during the COVID-19 pandemic: risk for a further myopia boom? Am. J. Ophthalmol. 223, 333–337 (2021).
Yin, H. et al. Rates of myopia development in young Chinese schoolchildren during the outbreak of COVID-19. JAMA Ophthalmol. 139, 1115–1121 (2021).
Horwood, A. M. & Riddell, P. M. Evidence that convergence rather than accommodation controls intermittent distance Exotropia. Acta Ophthalmol. 90, 109–117 (2012).
Chen, Y. et al. Accommodation is unrelated to myopia progression in Chinese myopic children. Sci. Rep. 21, 10 (2020).
Sheedy, J. E. et al. Is all asthenopia the same? Optom. Vis. Sci. 80, 732–739 (2003).
Logan, N. S. et al. IMI accommodation and binocular vision in myopia development and progression. Invest. Ophthalmol. Vis. Sci. 62, 213–218 (2021).
Song, Y. Accommodation and binocular vision changes after wearing orthokeratology lens in 8-to14-year-old myopic children. Graefes Arch. Clin. Exp. Ophthalmol. 259, 2035–2045 (2021).
Lee, J. Y., Seo, J. Y. & Baek, S. U. The effects of glasses for anisometropia on stereopsis. Am. J. Ophthalmol. 156, 1261–1266 (2013).
Radhakrishnan, H. & Allen PM,Calver, R. I. Peripheral refractive changes associated with myopia progression. Invest. Ophthalmol. Vis. Sci. 54, 1573–1581 (2013).
Lee, T. T. & Cho, P. Relative peripheral refraction in children: twelve-month changes in eyes with different ametropias. Ophthalmic Physiol. Opt. 33, 283–293 (2013).
Song, Y. et al. Accommodation and binocular vision changes after wearing orthokeratology lens in 8-to14-year-old myopic children. Graefes Arch. Clin. Exp. Ophthalmol. 259, 2035–2045 (2021).
Lee, S. H., Kim, M., Kim, H. & Park, C. Y. Visual fatigue induced by watching virtual reality device and the efect of anisometropia. Ergonomics 64, 1522–1531 (2021).
Shen, J. & Cui, H. How ptosis affects the visual quality: an overview of visual quality impairments and contributing factors in ptotic eyes. Int. Ophthalmol. 45, 88–92 (2025).
Nie, L. L., Ma, X. & Pei, Y. Subjective and objective changes in visual quality after implantable collamer lens implantation for myopia. Front. Med. 7, 12–17 (2025).
Altoaimi, B. H., Kollbaum, P., Meyer, D. & Bradley, A. Experimental investigation of accommodation in eyes fit with multifocal contact lenses using a clinical auto-refractor. Ophthalmic Physiol. Opt. 38, 152–163 (2018).
Ana, F. & Pereira-da-Mota Jéssica Costa, Ana Amorim-de-Sousa. The impact of overnight orthokeratology on accommodative response in myopic subjects. J. Clin. Med. 9, 3687–3693 (2020).
Ma, M. M. L. et al. Effect of vision therapy on accommodative lag in myopic children: A randomized clinical trial. Optom. Vis. Sci. 96, 17–26 (2019).
Satou, T. et al. Diferences in the stimulus accommodative convergence/accommodation ratio using various techniques and accommodative stimuli.Strabismus26, 53–61 (2018).
Berntsen, D. A., Mutti, D. O. & Zadnik, K. Study of theories about myopia progression (STAMP) design and baseline data. Optom. Vis. Sci. 87, 823–832 (2010).
Lee, J. Y., Seo, J. Y. & Baek, S. U. The efects of glasses for anisometropia on stereopsis. Am. J. Ophthalmol. 156, 1261–1266 (2013).
Golebiowski, B. et al. Smartphone use and efects on tear film, blinking and binocular vision. Curr. Eye Res. 45, 428–434 (2020).
Funding
This study was supported by Shenzhen Science and Technology Program (No. JCYJ20220818102603007).
Author information
Authors and Affiliations
Contributions
Yingpin Cao and Ming-ming Yang designed the study and revised the manuscript. Yingpin Cao and Jiajia Ye wrote and revised the manuscript. Aiqin Nie performed the analysis and wrote the manuscript. Dan Sun revised the manuscript. All the authors reviewed the results and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent for publication
All the authors approved the manuscript for publication.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cao, Y., Ye, J., Nie, A. et al. Correlation between binocular vision function and visual fatigue in school-age children with myopic anisometropia. Sci Rep 15, 17473 (2025). https://doi.org/10.1038/s41598-025-01309-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-01309-3
Keywords
This article is cited by
-
Evaluation of binocular vision parameters as screening indicators for asthenopia
Graefe's Archive for Clinical and Experimental Ophthalmology (2025)
