
Abstract
Idiopathic generalized epilepsy (IGE) is a complex epilepsy syndrome with various subtypes that appear normal on conventional magnetic resonance imaging (MRI). However, advanced quantitative MRI techniques have revealed subtle structural abnormalities. This study aims to identify specific cerebral regions with structural and volumetric alterations in IGE patients. A retrospective study was conducted on 38 IGE patients and 38 age and sex-matched healthy control subjects. MRI images were processed and segmented semi-automatically to extract volumes of cortical and subcortical brain regions. Statistical analysis was performed to compare volumes between IGE patients and controls. IGE patients exhibited significantly increased volumes in the precuneus (p = 0.002), and the pallidum (p < 0.001) compared to control subjects. No significant differences were observed in other regions, such as the precentral gyrus and frontal gyri. This study highlights conflicting results in the literature regarding radiologic volumetric data in IGE. While our findings imply the potential utility of incorporating volumetric analysis in the radiologic diagnosis of IGE patients to enhance targeted treatment approaches, it is important to exercise caution in interpreting these results, especially since these are primarily based on group-wise comparison. The increased volumes of the precuneus and pallidum in IGE patients suggest possible diagnostic implications. However, the extent of their clinical significance necessitates further investigation. Further research should investigate the clinical significance of these volumetric alterations and their potential role in guiding personalized treatment strategies for IGE patients.
Similar content being viewed by others

Introduction
Genetic generalized epilepsy (GGE) is characterized by the occurrence of one or more of the following generalized seizure types: absence, myoclonic, and bilateral tonic-clonic (BTC) seizures, either alone or in combination with documented generalized spike-wave discharges on EEG. It is further classified into subtypes based on the predominant seizure types, electrophysiological features, and age of seizure onset1,2. GGE includes the idiopathic generalized epilepsy (IGE) that consists of juvenile myoclonic epilepsy (JME), childhood absence epilepsy (CAE), juvenile absence epilepsy (JAE), and IGE with generalized tonic-clonic alone (IGE-GTCA)3,4.
While conventional magnetic resonance imaging (MRI) typically appears normal in patients with IGE4, advanced neuroimaging techniques have enabled the detection of subtle structural and microstructural abnormalities. Quantitative MRI techniques, such as voxel-based morphometry (VBM), diffusion imaging, and volumetric segmentation, have significantly advanced our understanding of IGE by revealing alterations in both gray and white matter that are not detectable on routine imaging. These approaches have identified abnormalities in thalamocortical and basal ganglia circuits, which are thought to play a key role in seizure generation and propagation5,6. Particularly, diffusion and functional MRI studies have revealed disrupted thalamocortical connectivity and motor system hyperactivation in patients with JME, suggesting the potential utility of structural imaging as a biomarker for seizure-related cognitive dysfunction6,7.
Recent work has also explored multimodal imaging, including diffusion tensor imaging (DTI), EEG-fMRI, and structural-functional coupling techniques, to better characterize network-level disruptions in IGE. DTI studies have revealed microstructural alterations in thalamocortical and corticospinal pathways even in patients without visible lesions on structural scans8,9,10. Functional MRI, particularly when combined with EEG, has further identified abnormal activation patterns within motor and cognitive control networks11,12. However, the interpretation of these modalities may be affected by factors such as variability in acquisition protocols, patient state during scanning, and complex preprocessing requirements.
In contrast, quantitative volumetric MRI provides a reproducible and anatomically grounded framework for assessing morphological brain changes. Prior VBM studies have highlighted structural abnormalities in cortical regions, in the frontal lobes13,14, as well as subcortical gray matter (GM) structures such as the thalamus15,16. Nonetheless, VBM results have often been inconsistent, likely due to methodological heterogeneity14,17. These inconsistencies underscore the need for precise and controlled manual segmentation approaches to enhance the reliability of morphometric findings in IGE.
Given these considerations, the objective of this study is to identify specific cerebral regions that exhibit volumetric alterations in patients with IGE. To achieve this, we will perform segmentation of a targeted set of cortical and subcortical brain regions, including those identified as potential contributors in previous studies3. Subsequently, we will analyze the segmented data to assess volumetric differences between patients with IGE and age and sex-matched healthy controls.
Materials and methods
Research design and study population
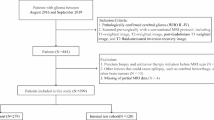
Patients identified for this study participated in an ongoing prospective trial enrolling children and adults with suspected new-onset unprovoked seizure(s). This is a centralized study conducted in association with the Lebanese Chapter of the International League against Epilepsy. Adult and pediatric neurologists from across Lebanon are referring patients (six months and older) with a suspected single unprovoked seizure or newly diagnosed epilepsy to our institution where a full clinical evaluation and extensive workup are performed. Patients with acute symptomatic seizures, those with a history of alcohol or drug abuse, children with febrile seizures, and pregnant women were excluded. For each included patient, we recorded the age at seizure onset, gender, family history of epilepsy, and the initial seizure types. A detailed history that included a thorough description of the spells was obtained from the patient, and an eyewitness, as well as a complete physical and neurological examination, were performed. All patients underwent a three-hour sleep-deprived video-EEG recording interpreted by two experienced epileptologists.
We included patients classified as having one of the IGE syndromes based on the types of seizure (BTC, absence seizures, myoclonic seizures), the presence of a generalized spike or/and polyspikes (GSPWD) and wave discharges, at a repetition rate of three Hz or more and on the EEG, age of onset and predominant seizure types. Patients who underwent a brain MRI within three months of presentation were included.
This study was approved by the Biomedical Institutional Review Board (IRB) of the American University of Beirut, which explicitly waived the requirement for written informed consent due to the retrospective nature of the study and minimal risk to participants. It was also conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and all relevant institutional and national regulations. All methods were performed in accordance with the applicable guidelines and regulations.
MRI acquisition
All patients had their MRIs performed either at the radiology department of our institution on a 3 T Philips Ingenia System (Philips Healthcare, Best, The Netherlands), or an external imaging center on a 3 T Siemens Verio System (Siemens Healthcare, Erlangen, Germany). A complete conventional MRI protocol was acquired. For the purposes of this study, we only used the 3D sagittal T1-weighted image (our institution: TR = 8.3 ms; TE = 3.8 ms; flip angle = 8°; field of view = 240 × 240 × 170 mm; spatial resolution = 1 × 0.94 × 0.94 mm3; external imaging center: TR = 1900 ms; TE = 32.48 ms; TI = 900 ms; flip angle = 9°; field of view = 512 × 512 × 150 mm; spatial resolution = 1 × 0.49 × 0.49 mm3).
Image processing
MRI images were manually checked by an experienced operator with more than fifteen years of experience (SH) for any major artifacts that could introduce errors or biases during image segmentation. Images first underwent bias-field correction using the N4-algorithm in 3DSlicer (https://www.slicer.org/), followed by a whole-brain extraction using the Brain Extraction Tool of the FMRIB Software Library (FSL5.0)18 to measure the intra-cranial volume (ICV). Volumes of subcortical GM, including the Accumbens, Amygdala, Caudate nucleus, Hippocampus, Pallidum, Putamen, and Thalamus, were then measured using FIRST which is a model-based segmentation/registration tool that uses manually segmented models18.
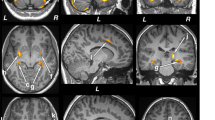
An atlas-based segmentation was also performed to extract the volumes of specific GM cortical areas, including the anterior cingulate gyrus, superior, inferior, and middle frontal gyri, precentral gyrus, precuneus, frontal medial cortex, subcallosal cortex, thalamic nucleus related to both posterior parietal lobe and temporal lobe. The Harvard-Oxford cortical structural atlas and the JHU-ICBM WM atlas were non-linearly registered to each subject’s T1 images using the Nifty-Reg software (http://cmictig.cs.ucl.ac.uk/wiki/index.php/NiftyReg). The resulting transformations were then applied to the atlas cortical GM masks. All extracted cortical and subcortical GM masks were visually checked for accuracy and manually corrected by a trained team of raters comprising an experienced neuroradiologist (R.H., 20 + years of experience) overseeing the work performed by a senior diagnostic radiology resident (S.A.F.) and two neuroradiology research students (N.A. & Z.M.). The raters were blinded for the patients’ diagnoses during the assessment of the images. Subsequently, the volumes of these masks were first extracted and then divided by the total intracranial volumes for each participant. These values, termed normalized volumes, represent the portion or percentage of the total brain volume that each specific region occupies (Fig. 1). The selection of cortical and subcortical regions of interest (ROIs) was hypothesis-driven, based on previous studies implicating these areas in the pathophysiology of IGE. Specifically, prior volumetric and connectivity research has highlighted alterations in thalamic, basal ganglia (notably the pallidum), and cortical regions including the frontal gyri and precuneus as key nodes in seizure generation and propagation networks in IGE patients3,5,6,13,19 The inclusion of these ROIs was informed by both structural and functional imaging studies that identified abnormalities in these regions across various IGE subtypes, enhancing the comparability and reproducibility of our findings. This targeted approach prioritized anatomical structures consistently implicated in previous morphometric studies and meta-analyses3,5,19.

Boxplots of normalized precuneus and pallidum volumes in IGE patients vs. healthy controls (HC). Horizontal lines represent group medians; boxes indicate interquartile ranges.
Given the variation in acquisition parameters between scanners—including spatial resolution (Philips: 1 × 0.94 × 0.94 mm³; Siemens: 1 × 0.49 × 0.49 mm³), field of view, and flip angle—all images were processed using a uniform pipeline consisting of N4 bias correction, brain extraction, and non-linear registration to a common anatomical space. This helped mitigate inter-scanner differences in tissue contrast and spatial alignment. All segmentation masks were visually reviewed and manually corrected by a team of blinded raters which helped reduce scanner-induced variability.
Statistical analysis
The mean and standard deviation volume measurements of all the normalized structures were determined for the patients with IGE and compared to those in the control group. Regions of interest (ROIs) were selected based on prior literature implicating specific cortical and subcortical structures in the pathophysiology of IGE. The difference in the means between these two groups with the 95% confidence interval for all the structures was calculated. The final analysis was performed by comparing the means of each structure using independent t-tests while applying a Bonferroni correction. A significant p-value was adjusted for multiple comparisons.
Ethical approval
The Institutional Review Board of our institution approved this study and waived the requirement to obtain informed consent, due to the retrospective nature of the study and the minimal risk for the patients.
Results
One hundred and fifteen subjects were identified from our institution’s database. Thirty-eight patients with IGE (22 males and 16 females) with a mean age of 18.1 ± 7.4 years along with 38 normal control subjects (NC, 17 males and 21 females) with a mean age of 18.7 ± 11.1 years were included in this study. In the IGE group, 15 were diagnosed as IGE with GTC alone, seven with JAE, and 16 with JME. No significant age and gender differences were observed between patients and control subjects. The demographics of the 38 patients with GGE are summarized in Table 1.

Illustration of the precuneus (posterior parietal cortex) and pallidum (basal ganglia region) anatomical locations.
The included GGE patients were newly diagnosed and were not on any anti-seizure Medications (ASM) before presentation. After diagnosis, 33 patients were started on Valproate, and 5 on Levetiracetam. Fifteen patients had begun ASM treatment before MRI acquisition, with a mean of 77.4 days (± 121 days). Given that most patients were untreated at the time of imaging, medication status was not included as a confounder in our analysis.
The total intracranial volume and the normalized volumes of the cortical gyri, specific cortical areas, and basal ganglia are stratified by IGE or control is summarized in Table 2. After correction for multiple comparisons, significant differences were found in the precuneus volume (IGE: 1.935 ± 0.237 vs. NC: 1.766 ± 0.240; p = 0.002) and the pallidum volume (IGE: 0.241 ± 0.021 vs. NC: 0.227 ± 0.018; p < 0.001) (Fig. 2).
Discussion
The use of advanced MRI techniques in the study of patients diagnosed with an IGE has been scarce, particularly with regards to regional brain segmentation and volumetric assessment. In our study, we conducted a comprehensive evaluation of numerous cerebral regions in patients with IGE, comparing them to a group of normal controls.
Our findings revealed a significant increase in the normalized volumes of the precuneus in patients with IGE compared to the control group. The precuneus is anatomically located in the postero-medial portion of the parietal lobe, anterior to the cuneus of the occipital lobe from which it is separated by the parieto-occipital fissure. It is also positioned posterior to the paracentral lobule, and superior to the sub-parietal sulcus20. It includes both unimodal and polymodal association regions and plays a crucial role in visual-spatial imagery, sensorimotor functions, and consciousness21. Precuneal epilepsy is rarely reported in the literature due to its diverse heterogeneous presentations and complex circuitry20. Previous studies have implicated the precuneus in the pathogenesis of IGE, as reduced functional connectivity has been observed in this region, as well as in the posterior cingulate gyrus19. This highlights the importance of further investigating and understanding the seizure pathophysiology in IGE patients, which differs significantly from other classic epilepsy syndromes3. The functional consequences of increased precuneus volume in IGE remain to be fully elucidated. However, given the region’s involvement in the default mode network (DMN)—which governs consciousness, introspection, and attention—alterations in its structure may reflect compensatory neuroplastic responses or disrupted synaptic pruning. These changes could influence network excitability and impair the dynamic regulation of attention and awareness during seizures6,22. The observed volumetric increase may thus represent a structural correlate of altered connectivity and dysfunctional consciousness mechanisms in IGE.
We also observed a significant increase in normalized volumes of the pallidum in patients with IGE compared to the control group. This finding contrasts with previous studies that reported reductions in the volume of the globus pallidus3,23. The discrepancies between our findings and those of other studies may be attributed to differences in sample sizes (38 IGE cases in our study compared to 14 IGE cases in the study by Du et al.23. The basal ganglia, including the globus pallidus, have been suggested to modulate the occurrence of spike-wave discharges in IGE through feedback circuits to the thalamus and cerebral cortex. It has been also suggested that abnormally increased activity in subcortical structures including the basal ganglia may play a crucial role in the motor manifestations of IGE24.
In our study, we did not find a statistically significant increase in the volume of the subcallosal cortex of patients with IGE compared to normal controls. This finding contrasts with a VBM study that reported an increase in GM volume in the right subcallosal gyrus in patients with absence epilepsy25. However, considering that reduced connectivity and function of the subcallosal gyrus have been implicated in treatment-resistant major depression26, further evaluation of this often-overlooked region may be warranted in patients with IGE.
We did not observe any statistically significant differences in the volume in the precentral gyrus, or frontal gyri between patients with IGE and normal controls3. The precentral gyrus, also known as the primary motor cortex, is responsible for executing voluntary movements on the contralateral side of the body. Previous studies investigating the function and involvement of the precentral gyrus in IGE have not yielded conclusive results, highlighting the need for further neurofunctional studies to explore the correlation between dysfunctional motor symptoms during seizures and activation of this specific brain region27.
It is important to acknowledge a few limitations to our study: the use of MRI data acquired from two different scanners with varying parameters, including field of view, spatial resolution, and flip angles, and the lack of standardized MRI protocols across imaging centers. However, this limitation was minimized through a consistent preprocessing pipeline—including bias correction and non-linear registration—and by performing visual quality control and manual correction of all segmented regions. Additionally, volumetric analysis was conducted using the same software for all included patients, after excluding non-diagnostic or sub-diagnostic evaluations. While these steps reduce potential bias, future studies may benefit from the integration of harmonization approaches or scanner-adjusted modeling. Considering that previous studies focusing on diffusion kurtosis have revealed distinct patterns of microstructural alterations in patients with IGE, particularly involving thalamo-cortical projections28, we suggest that future studies combining diffusion kurtosis and volumetric analysis may provide further insights into these findings.
Although this study did not include an a priori power calculation, a post hoc sensitivity analysis using GPower (α = 0.05, power = 0.80, two-tailed t-test) indicated that the sample size was adequate to detect medium to large effect sizes. The significant findings in the precuneus and pallidum volumes fall within this range, supporting the robustness of the observed group differences.
The observed volumetric increases in the precuneus and pallidum in IGE patients raise important considerations for clinical practice. Although our study is cross-sectional and does not directly assess clinical outcomes, previous work suggests that such structural alterations may hold predictive value. For example, increased precuneus volume has been associated with altered default mode network activity, which may influence attention and consciousness during seizures6. Similarly, basal ganglia abnormalities, particularly involving the pallidum, have been linked to motor manifestations and seizure modulation through thalamocortical loops5. These findings support the potential of regional volumetric markers as complementary tools for identifying IGE subtypes with distinct clinical or cognitive profiles. Future studies may investigate whether these morphometric features correlate with pharmaco-resistance, cognitive deficits, or long-term seizure control, thereby informing personalized treatment strategies.
Although this study did not assess cognitive or motor performance directly, previous work has linked abnormalities in the precuneus to deficits in attention, introspection, and working memory among patients with IGE6. Increased volume in this region may reflect altered neurodevelopmental pruning or compensatory reorganization in response to seizure-related network disruption29. Similarly, the pallidum is involved in the modulation of motor output and seizure propagation through basal ganglia-thalamocortical circuits30. Structural changes in this region may be associated with motor manifestations, particularly in patients experiencing GTCA5. Future studies combining volumetric analysis with neuropsychological and motor assessments could clarify the clinical impact of these findings.
In our study, the decision to consolidate the IGE subsyndromes offered several advantages such as the increase in sample size, a better statistical power to identify generalizable trends and shared morphometric patterns with potential clinical implications across IGE patients. However, it also limited our ability to isolate subsyndrome-specific characteristics. Therefore, it is important to recognize the trade-off between broader insights and the depth of subsyndrome-specific exploration within our study context.
Conclusion
The literature on radiologic volumetric data in IGE presents conflicting and inconsistent results, underscoring the need for further quantitative radiologic evaluation. Our study contributes to this body of knowledge by revealing a significant increase in the volumes of the precuneus and pallidum in patients with IGE. While qualitative MRI features have traditionally been evaluated in patients with IGE, our findings raise the question of whether adding volumetric measurements to IGE protocols could enhance targeted treatment approaches. By identifying patterns of regional cerebral cortical and subcortical volume changes that align with the clinical assessment of patients, we may improve the accuracy of IGE diagnosis. It is however important to exercise caution in interpreting these results, especially since these are primarily based on group-wise comparison.
Further research is warranted to investigate the clinical significance of these volumetric alterations and their potential role in guiding personalized treatment strategies for patients with IGE. By leveraging quantitative radiologic evaluation, we can potentially unlock new avenues for advancing the management of this complex epilepsy syndrome.
Data availability
The anonymized volumetric measurements, and segmentation masks that support the findings of this study are available from the corresponding author upon reasonable request. Due to ethical and privacy restrictions, individual raw MRI scans cannot be shared. Access to the available data may require institutional approval and the signing of a data use agreement to ensure compliance with ethical standards and data protection regulations.
References
Nordli, D. R. Jr. Idiopathic generalized epilepsies recognized by the international league against epilepsy. Epilepsia 46 (Suppl 9), 48–56. https://doi.org/10.1111/j.1528-1167.2005.00313.x (2005).
Berg, A. T. et al. Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE commission on classification and terminology, 2005–2009. Epilepsia 51, 676–685. https://doi.org/10.1111/j.1528-1167.2010.02522.x (2010).
Nuyts, S., D’Souza, W., Bowden, S. C. & Vogrin, S. J. Structural brain abnormalities in genetic generalized epilepsies: A systematic review and meta-analysis. Epilepsia 58, 2025–2037. https://doi.org/10.1111/epi.13928 (2017).
McGill, M. L. et al. Functional neuroimaging abnormalities in idiopathic generalized epilepsy. Neuroimage Clin. 6, 455–462. https://doi.org/10.1016/j.nicl.2014.10.008 (2014).
Gong, J. et al. Distinct effects of the basal ganglia and cerebellum on the thalamocortical pathway in idiopathic generalized epilepsy. Hum. Brain Mapp. 42, 3440–3449. https://doi.org/10.1002/hbm.25444 (2021).
Caciagli, L. et al. Motor hyperactivation during cognitive tasks: an endophenotype of juvenile myoclonic epilepsy. Epilepsia 61, 1438–1452. https://doi.org/10.1111/epi.16575 (2020).
O’Muircheartaigh, J. et al. Abnormal thalamocortical structural and functional connectivity in juvenile myoclonic epilepsy. Brain 135, 3635–3644. https://doi.org/10.1093/brain/aws296 (2012).
Kreilkamp, B. A. K. et al. Multi-spectral diffusion MRI mega-analysis in genetic generalized epilepsy: relation to outcomes. NeuroImage: Clin. 39, 103474. https://doi.org/10.1016/j.nicl.2023.103474 (2023).
Pei, H. et al. Functional and structural networks decoupling in generalized tonic–clonic seizures and its reorganization by drugs. Epilepsia Open. 8, 1038–1048. https://doi.org/10.1002/epi4.12781 (2023).
Lüttjohann, A. & van Luijtelaar, G. The role of thalamic nuclei in genetic generalized epilepsies. Epilepsy Res. 182, 106918. https://doi.org/10.1016/j.eplepsyres.2022.106918 (2022).
Ji, G. J. et al. A generalized epilepsy network derived from brain abnormalities and deep brain stimulation. Nat. Commun. 16, 2783. https://doi.org/10.1038/s41467-025-57392-7 (2025).
Shamshiri, E. A., Sheybani, L. & Vulliemoz, S. The role of EEG-fMRI in studying cognitive network alterations in epilepsy. Front. Neurol. 10, 1033. https://doi.org/10.3389/fneur.2019.01033 (2019).
Woermann, F. G., Free, S. L., Koepp, M. J., Sisodiya, S. M. & Duncan, J. S. Abnormal cerebral structure in juvenile myoclonic epilepsy demonstrated with voxel-based analysis of MRI. Brain 122 (Pt 11), 2101–2108. https://doi.org/10.1093/brain/122.11.2101 (1999).
Lin, K. et al. Voxel-based morphometry evaluation of patients with photosensitive juvenile myoclonic epilepsy. Epilepsy Res. 86, 138–145. https://doi.org/10.1016/j.eplepsyres.2009.05.016 (2009).
Mory, S. B., Li, L. M., Guerreiro, C. A. & Cendes, F. Thalamic dysfunction in juvenile myoclonic epilepsy: a proton MRS study. Epilepsia 44, 1402–1405. https://doi.org/10.1046/j.1528-1157.2003.67702.x (2003).
Helms, G., Ciumas, C., Kyaga, S. & Savic, I. Increased thalamus levels of glutamate and glutamine (Glx) in patients with idiopathic generalised epilepsy. J. Neurol. Neurosurg. Psychiatry. 77, 489–494. https://doi.org/10.1136/jnnp.2005.074682 (2006).
Ciumas, C. & Savic, I. Structural changes in patients with primary generalized tonic and clonic seizures. Neurology 67, 683–686. https://doi.org/10.1212/01.wnl.0000230171.23913.cf (2006).
Smith, S. M. et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 23 (Suppl 1), 208–219. https://doi.org/10.1016/j.neuroimage.2004.07.051 (2004).
Kim, J. B. et al. Altered thalamocortical functional connectivity in idiopathic generalized epilepsy. Epilepsia 55, 592–600. https://doi.org/10.1111/epi.12580 (2014).
Al-Ramadhani, R. R. et al. The precuneal cortex: anatomy and seizure semiology. Epileptic Disord. 23, 218–227. https://doi.org/10.1684/epd.2021.1257 (2021).
Cavanna, A. E. & Trimble, M. R. The precuneus: a review of its functional anatomy and behavioural correlates. Brain 129, 564–583. https://doi.org/10.1093/brain/awl004 (2006).
Blumenfeld, H. Impaired consciousness in epilepsy. Lancet Neurol. 11, 814–826. https://doi.org/10.1016/s1474-4422(12)70188-6 (2012).
Du, H. et al. Regional atrophy of the basal ganglia and thalamus in idiopathic generalized epilepsy. J. Magn. Reson. Imaging. 33, 817–821. https://doi.org/10.1002/jmri.22416 (2011).
Luo, C. et al. Resting state basal ganglia network in idiopathic generalized epilepsy. Hum. Brain Mapp. 33, 1279–1294. https://doi.org/10.1002/hbm.21286 (2012).
Bin, G. et al. Patterns of Gray matter abnormalities in idiopathic generalized epilepsy: A Meta-Analysis of Voxel-Based morphology studies. PLoS One. 12, e0169076. https://doi.org/10.1371/journal.pone.0169076 (2017).
Dunlop, B. W. et al. Functional connectivity of the Subcallosal cingulate cortex and differential outcomes to treatment with Cognitive-Behavioral therapy or antidepressant medication for major depressive disorder. Am. J. Psychiatry. 174, 533–545. https://doi.org/10.1176/appi.ajp.2016.16050518 (2017).
Jia, X. et al. Disrupted coupling between the spontaneous fluctuation and functional connectivity in idiopathic generalized epilepsy. Front. Neurol. 9, 838. https://doi.org/10.3389/fneur.2018.00838 (2018).
Lee, C. Y. et al. Diffusional kurtosis imaging reveals a distinctive pattern of microstructural alternations in idiopathic generalized epilepsy. Acta Neurol. Scand. 130, 148–155. https://doi.org/10.1111/ane.12257 (2014).
Tracy, J. I. et al. Computational support, not primacy, distinguishes compensatory memory reorganization in epilepsy. Brain Commun. 3, fcab025. https://doi.org/10.1093/braincomms/fcab025 (2021).
Brodovskaya, A., Shiono, S. & Kapur, J. Activation of the basal ganglia and indirect pathway neurons during frontal lobe seizures. Brain 144, 2074–2091. https://doi.org/10.1093/brain/awab119 (2021).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
R.H., A.B. and W.N. conceived and designed the study. S.H., S.A.F., Z.M., and N.A. performed data collection and image processing. S.H. and W.N. conducted statistical analysis. S.H., R.H., A.B. and W.N. interpreted the results. S.H. and S.A.F. drafted the main manuscript text. R.H. and W.N.supervised the study and provided critical revisions. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of interest disclosure
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hannoun, S., Abi Fadel, S., Mousawi, Z. et al. Increased volumes of the precuneus and the pallidum in idiopathic generalized epilepsy. Sci Rep 15, 32157 (2025). https://doi.org/10.1038/s41598-025-02003-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-02003-0
