
Abstract
Children with multiple disabilities have developmental issues in psychological domains. Adaptive yoga tailored to individual abilities promises positive results on children with special needs. This study applies multiple baseline single-case experimental design (SCED) to establish functional relationship between yoga and psychological health of children with autism spectrum disorder (ASD) and intellectual disability (ID). A multiple baseline SCED (AB1B2), with phases (A) baseline without intervention, (B1) intervention in the institute with a yoga teacher and caregiver, and (B2) intervention at home with the caregiver. The experiment was replicated across six children aged 7–12 years with mild ASD and ID. The study assessed the impact of a 180-day adaptive yoga intervention on twelve parameters across cognitive, behavioural, and emotional domains. Assessments were administered using the Indian Scale for Assessment of Autism (ISAA) and Behavioural Assessment Scales for Indian Children with Mental Retardation (BASIC-MR) tools. The study involved caregivers, yoga teacher, and clinical psychologists. The visual analysis established the functional effect of yoga intervention. The effectiveness of impact was supplemented by percentages of non-overlapping pairs and Cohen’s d shows moderate to significant impact among all the participants in at least three instances across psychological domains. The experiment establishes both internal and external validity.
Trial registration CTRI/2021/08/035389; DoR: 04/08/2021.
Similar content being viewed by others



Introduction
Children with multiple disabilities, particularly those diagnosed with autism spectrum disorder (ASD) and with intellectual disability (ID), represent a uniquely vulnerable population facing profound challenges in various aspects of psychological health. These children often struggle with cognitive delays, behavioural issues, and emotional dysregulation, which can significantly impede their ability to engage in daily activities, form social connections, and to reach developmental milestones.
In a recent study, parents of children with both intellectual and developmental disabilities (IDD) and with ASD reported greater psychological distress compared to those with IDD alone. Specifically, symptoms of hyperactivity, emotional difficulties and conduct problems in children with ASD were significant contributors to this distress1.
The study indicates that conditions like ASD and with ID exhibit significantly more symptomatology, including anxiety, mania, schizophrenia, stereotypies/tics, self-injurious behaviour, eating disorders, sexual disorders, and impulse control2. These conditions are also associated with a greater negative impact on family financial and employment burdens3.Without the necessary services and supports, preferably starting in the earliest years of life, these conditions can result in significant and lifelong impairments4.
Compounding difficulties of children with developmental disorders often require specialized care beyond standard interventions. Traditional therapeutic interventions, such as behavioural therapy, occupational therapy, speech therapy, and medication are beneficial in meeting the respective functional objectives. The complexity of managing co-occurring conditions like ASD and with ID intensifies these challenges. This study is an attempt to supplement the existing therapies with yoga intervention to see if there are any improvement in psychological areas like cognitive, behavioural, and emotional domains.
Yoga, an ancient mind-body practice, has increasingly been recognized for its potential therapeutic benefits across various populations. Yoga based interventions on normal preschool children shows significant improvement in their motor abilities like balance, strength, and flexibility5,6. In few other studies yoga interventions like asana (postures), pranayama (breath regulation), dharana (concentration), dhyana (meditation) appears to be an effective modality for helping normal children to cope with the stress, anxiety and improvement in self-regulation and emotional regulation7,8. Among children with ASD with interventions like IYAT (Integrated Approach to Yoga Therapy) and movement based yoga has shown significant improvement in their motor skills, while few study involving mindfulness based practices such as MBSR (Mindfulness Based Stress Reduction), MBPBS (Mindfulness Based Positive Behaviour Support) shows improvement in behavioural skills among adults with ID9,10,11,12. However, the body of research is still nascent on yoga interventions for multiple disabilities having combination of more than one developmental disorder, often marked by methodological limitations and non-scientific case studies.
Yoga intervention for children with ASD and ID necessitates modification in yoga teaching methodology customized to the individual level and capacity. The yoga course plan is designed based on the fundamental principles of yoga as rooted in classical text of Patanjali Yogasutra (PYS). The aphorism, sukham sthiram asanam (PYS, Chap. 2, Verse 46) means quality of asana (practice) should meet the criteria of sukham (comfort) and sthiram (stability) of the practitioner. Another aphorism, tasya bhumisu viniyoga (PYS, Chap. 3, Verse 6) means the practice is always unique and specific to the individuals’ capacity and comfort. A common misconception among people around yoga is to attain only certain form classically. This might lead to compromising sukham and sthiram. All the tools of yoga like asana (physical postures or form), pranayama (breath regulation), and dhyana (meditation) were designed to serve certain functional benefits. This purpose can also be achieved through adaptations. Another important reason for practicing asana variations is to encourage attentiveness. The design of a right course plan serves this purpose, yet that is personalised, meets the criteria of function over form and safe, while maintaining the sukham and sthiram for a practitioner. A course plan also evolves as the practitioner establishes themselves in the practice gradually. Yoga practices performed with coordination of movement and breath with awareness offers a pathway to better sensory integration and subsequently improve psychological areas such as cognitive, behavioural, and emotional domains13.
The participation of caregiver in the session along with yoga teacher is an important dimension. This helps the participants to build a psychologically safe environment. The caregiver also helps in patterning the movements along with the yoga teacher. The design also involves extended intervention in home setting without yoga teacher, where the participant continues the practice along with the caregiver during follow-up phase and later.
Children with special needs require personalized intervention. Every child has unique needs and capacity. A traditional group design and aggregate analysis like RCT may not be appropriate for the study of intervention impact on psychological areas. A Single Case Experimental Design (SCED) empirically establishes both internal and external validity even with smaller sample size where the participant serves as their own control. The data generated by continuous assessments across phases contribute to establish the significance of the impact. The baseline phase compared to intervention phases shows the functional relationship14,15. The SCED established functional relationships between the intervention (or independent variable) and the outcomes observed in autistic children or youth16. The significance of impact can be established by replication of study across participants, psychological domains, and settings.
This study was first of its kind to apply yoga intervention on children with multiple disabilities on their psychological skills. The study was a multi-stakeholder study with involvement of experts from field of multiple disabilities, clinical psychology, and yoga. The genesis of this experiment was a joint effort to test and see any possibilities of benefit that can be derived from yoga for children with special needs with multiple developmental disorders. From clinical psychology experts’ point of view, the scope of the study was kept simple, limited to the children having ASD and with ID, with mild level of severity and assess the impact on psychological areas using standardized tools - ISAA and BASIC(MR) across sub-domains that do not conflict cross functionally, i.e., cognitive, behavioural and emotional. From yoga experts’ point of view, the scope was to design an adaptive yoga module and an intuitive teaching methodology that suits the capacity of individual participants with such conditions, keeping the foundational principles of yoga intact and simplifying the practice to the level of participants and their caregivers, to ensure continuity of practice in post research context. The anticipated indicators of improvement in cognitive domain were for the participants to be able to follow basic yoga instructions, under behavioural domain were to have reduced hyper activity, cooperate to complete daily practice and under emotional domain the indicators were improvement in demonstrating certain level of expression and regulation of emotions. We wanted to make this study as a robust experiment, empirically establishing any outcome as it comes. Thus, used SECD with continuous assessments to generate adequate data to support our outcome. Both psychological assessments and yoga intervention happened in parallel and the respective observations were blinded from each other till the experiment was over. The empirical significance and the subjective observations to these psychological domains are provided in this article.
This research work aims to prove existence of a functional relationship and efficacy of tailored made yoga intervention for children with ASD and with ID on improving their psychological health in cognitive, behavioural, and emotional domains by employing a rigorous scientific framework, a well-crafted adaptive course plan and teaching methodology. The purpose is also to involve caregivers that ensures continuity of the practice if there are carry forward benefits in home condition.
Method
Participants
Six children participated along with their caregivers (mothers), recruited from NIEPMD—National Institute for Empowerment of Persons with Multiple Disabilities (Divyangjan), Chennai, Tamil Nadu, India, Under Department of Empowerment of Persons with Disabilities (Divyangjan), Ministry of Social Justice & Empowerment, Govt. of India. The participants are residents and day boarders availing therapeutic services from the institute. Two of the participants attend special model school run by the institute and four attend other schools outside the institute admitted based on special status. The mothers with limited educational background could communicate only in vernacular (Tamil) language and children could follow their mothers. For children, two were non-verbal and other four however verbal, had minimal communication. Mostly caregivers understood them better and helped bridging the communication gaps during the intervention.
The two participants from the institute were introduced to basic yoga postures as part of school curricula in form of a group practice and not formally as a regular therapeutic one-to-one intervention. Other four participants had no prior exposure to yoga. The common therapeutic services like occupational therapy, speech therapy, behavioural therapy and special education were attended time to time by all the participants in the institute.
All the participants are certified by the institute under Department of Empowerment of Persons with Disability (DEPD) gazette guidelines for multiple disability certification on ASD and with ID. As per the guidelines, INCLEN Diagnostic tool for Autism Spectrum Disorder (INDT-ASD) is used by the institute for ASD diagnosis followed by Indian Scale for Assessment of Autism (ISAA) to assess the severity of the condition. The Binet-Kamat Test of Intelligence (BKT) and Malins Intelligence Scale for Indian Children (MISIC) are used to confirm the ID diagnosis and Vineland Social Maturity Scale (VSMS) tool is used assess the severity of the diagnosis.
The inclusion criteria for the study included children those were certified by the institution as multiple disabled having ASD and with ID, chronological age between 7 and 12 years having mild severity level and the caregiver agreed to participate throughout the study. Children having other disabilities, beyond the age criteria, having moderate, severe to profound conditions in ASD and ID were excluded. Demographic details are represented in Table 1. Prior to the participation the informed consent was obtained from parents and/or legal guardians.
The six assessors recruited were practicing clinical psychologists facilitated by the institute. One assessor was mapped to one participant. The trained yoga teacher was the researcher of this study to execute the intervention.
Design
A multiple baseline single case experimental design (AB1B2) was implemented for this study. Each participant went through three phases: (A) baseline phase without intervention, (B1) intervention phase in institute setting with yoga teacher and caregiver, and (B2) intervention phase in home setting with only caregiver. Continuous assessments were planned and administered for each participant at a frequency of every two weeks. The start of the intervention was stratified based on completion of four months of without any yoga practice and completion of associated baseline assessments for respective participants from the time of recruitment. This was planned to establish the existence of the problem related to the variables of interest before start of the intervention. Six months of intervention along with yoga interventionist and caregiver in institute setting followed by three months of yoga along with caregiver alone in home setting was planned. The duration of each intervention phase was decided based on number of intervention sessions as per the plan and that covers at least five counts of assessments for observable data representation for a phase analysis15. The multiple baselines were compared for each replication across six participants, twelve parameters distributed under three psychological domains and two settings. Replication added strength for external validity17. There was limited scope of randomization in this study. The continuous assessment outcomes were blinded for the interventionist and parents, also the assessors were blinded to the intervention procedure throughout the study. The study was conducted and reported as per the Single-Case Reporting Guidelines In Behavioural Interventions (SCRIBE) 2016 Statement18.
The study was approved by Research Committee (RC) of the institution where the study was executed, Doctoral Committee (DC) and Institutional Ethics Committee (IEC) of affiliated University. This is to confirm that all the methods were performed in accordance with the relevant guidelines and regulations as per the Declaration of Helsinki. The study adhered to the approved protocol and consent process.
Intervention procedure
A caregiver orientation workshop was conducted before commencing the intervention to explain the purpose of study and the importance of their role during the intervention. The participants continued their respective regular therapies throughout the study. There were no conditional restrictions on other therapies along with yoga intervention. This also met the purpose of SCED where respective participants served as their own control and only change was additional yoga intervention to assess the impact.
The yoga sessions were administered for the participants as one-to-one intervention along with yoga teacher and caregiver. The intervention sessions started in institute setting along with yoga teacher and caregiver for 120 days, followed by 60 days in home setting along with only caregiver. Each intervention session duration was between 45 to 60 minutes administered every working day of the week excluding weekends and holidays. Before moving from institute setting to home setting, the ownership of intervention was handed over to the caregiver with documented course plan for continuity and smooth execution. A sample documented plan can be referenced in Appendix B.
During home setting phase, six sessions (once in a fortnight) over this period were conducted by the yoga teacher to re-establish the continuity and correct the course plan as applicable. The total days of intervention were adjusted to the planned number of days to compensate any longer absences (more than a week) against medical emergencies. Figure 1 represents the flow.

Recruitment flowchart.
Course plan
A well-crafted course plan designed that was personalized, prioritized function over form, and was safe based on the fundamental principles of yoga as rooted in the scripture of Patanjali Yogasutra13. (1) Personalized – The practice was designed specific to the individual’s capacity and comfort. The course plan was further modified to suite the physical and mental condition of the participant on a particular day. (2) Function over form – A well-structured yet flexible course plan was designed with appropriate sequences towards fulfilling the function rather than emphasis to achieve the form. (3) Transition of planes were carefully crafted keeping it smooth and in sequence for example from seated to standing to supine to prone to kneeling to seated. (4) For all asanas (physical postures) adequate counter postures were given. (5) Adequate rests were incorporated between asanas integrated with counting or chanting to sustain the participant’s attention. Refer to a sample course plan in Appendix A.
In the initial phase, the sessions were simplified, preparatory, and executed depending on the interest and comfort of the participant on that day. Once the relationship was established (between the yoga teacher and the participant), the nuances were understood by the yoga teacher, the sessions were modified incrementally as per the course plan.
Teaching methodology
The fundamentals of yoga—movement, breath and awareness were achieved by incorporating following adaptation techniques in teaching.
Movement (1) The objective is to get into and come out of the posture with comfort. This sequence was simplified and broken into smaller steps. (2) Adaptations were seasoned by repetition. The approach was iterative and incremental, subject to the readiness of participant for next stage. (3) asana forms were established using patterning wherever applicable with support of caregiver. For example, in dvipada pitham (bridge pose), the hip movements were patterned by support of caregiver lifting the back of the participant.
Breath The breath was influenced in two ways. (1) Our body naturally inhales on expansion and exhales on contraction. Appropriate sequencing by alternating movements helped to achieve the right breathing. (2) Chanting happens on exhalation. Thus, chanting of any syllable of participants’ choice was used in exhalation leading to an implicit inhalation. Length of the chant was moderated as per the participant’s capacity.
Awareness Awareness was brought by maintaining the attention of the participants throughout the session. (1) Every session started by re-establishing a positive connect between yoga teacher, the participant, and the caregiver. (2) The sessions were then executed with continuous engagement in form of movements integrated with limited voice modulated short instructions, counting, chanting, demonstration, and patterning that was suitable for the participant for that session. (3) Every day the teacher assessed the readiness and responsiveness of the participants and accordingly customised the session to bring the best to meet the session objective. (4) The yoga teacher demonstrated and practiced along with the participants throughout the session for ease of imitation.
The visual cues (parallel demonstration), auditory cues (limited voice modulated short instructions), support (caregiver patterning), simple plan integrating movements with chanting or counting; all combined throughout the session helped in making the session mindful and accessible.
Assessments
Indian Scale for Assessment of Autism (ISAA) and Behavioural Assessment Scales for Indian Children with Mental Retardation (BASIC-MR) instruments were used to assess the desired cognitive, behavioural, and emotional parameters objectively.
ISAA is an objective assessment tool for persons with autism which uses observation, clinical evaluation of behaviour, testing by interaction with the subject and information supplemented by parents or caretakers. The ISAA questionnaire is divided under six domains: social relationship and reciprocity, emotional responsiveness, language and communication, behaviour pattern, sensory aspects, and cognitive component. These are further quantified by providing percentages to indicate the frequency, degree and intensity of behavioural characteristics that are observed. Lower the percentage indicates lesser problem and higher the score indicates severity. ISAA is a standardized, reliable, and valid tool for diagnosis and assessment of severity in autism among children19.
BASIC-MR is designed to elicit systematic information on the current level of behaviour in school going children with development disorders. It is developed in two parts. Part-A helps to assess the current level of skills behaviours in the child. Part-B helps to assess the current level of problem behaviours in the child. Part-A consists of seven domains: motor, activity of daily living (ADL), language, reading-writing, number-time, domestic-social, and prevocational-money. Part-B consists of ten domains: violent and destructive behaviour, temper tantrums, misbehaviour with others, self-injurious behaviours, repetitive behaviours, odd behaviours, hyperactive behaviours, rebellious behaviours, antisocial behaviours, and fears. For both Part-A and Part-B each of the respective domains of interest can be consumed independently. The scores for each domain are calculated and converted into a percentage. For Part-A a higher score indicates better skill behaviours, while for Part-B a lower score indicates fewer behaviour problems20.
Twelve domains as variables of interest were picked from ISAA and BASIC-MR (A&B) that was administered to generate percentage scores. The aggregate score of the child on each domain expressed as the raw score. This was converted into percentage for each domain by dividing the obtained raw score by maximum score for that domain and multiplied by 100. The percentage scores across phases were compared against the expected outcome of increasing or decreasing measure as prescribed in the tool. Table 2 describes the assessment parameters of interest, description of problems assessed in each domain, and expected outcome.
The study was conducted over three phases. The assessments were administered by assessors to collect cognitive, behavioural, and emotional data desired for the study every two weeks as per the plan. Total twenty-six (26) assessments were administered throughout the study with first eight during baseline phase (without intervention), followed by twelve during intervention phase in institute setting followed by six during intervention phase in home settings. The assessors were blinded to the intervention modifications. The yoga interventionist and caregivers were blinded to the assessment scores during the intervention phases. After all the assessments were completed and completion of intervention phases, the scores were revealed and consolidated for analysis.
Data analysis–collection, visual and empirical analysis
Overall, 1836 data points generated out of 153 assessments for six participants. The data points were aggregated and analysed for each participant, for each parameter within and across phases. A visual analysis tool was developed using MS Excel to consume the data collected and generate respective participant-parameter wise time sequence line graphs for visualization. Figure 2 represents the sample distribution of 26 data points representing the percentage score on ‘Odd Behaviour’ across three phases for Participant#1. Percentage scores of observable parameters are depicted along the ordinate axis, and the abscissa represents the baseline (B1-B8), intervention institute setting (II1-II12), and intervention home setting (IH1-IH6) assessments.
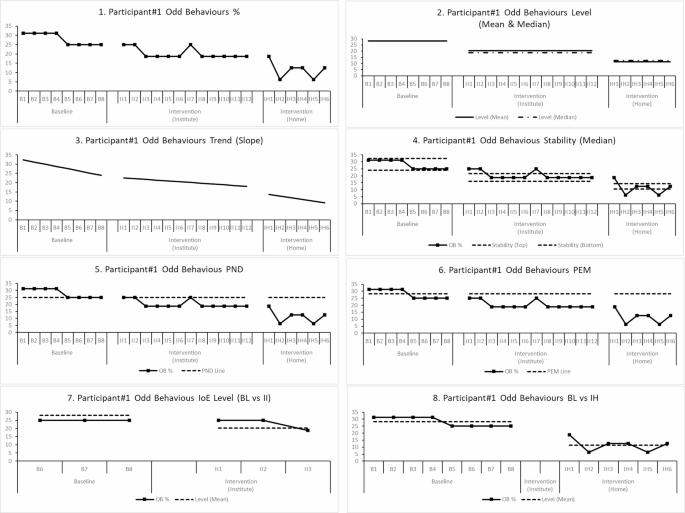
Sample graphs generated for visual analysis for Participant#1 for “odd behaviours” parameter. Description of graphs in order (1) Overall 26 data points across baseline, intervention(institute), intervention(home). (2) Levels represented by Mean and Median Lines. (3) Phase wise trend line. (4) Stability of data between Median range of (+/-) 15%. (5) The Percentage of Non-overlapping data (PND) using min (or max) baseline data point. (6) Percentage of data exceeding median line (PEM). (7) Immediacy of effect comparing last three data points of baseline against first three data points of intervention phase. (8) The level mean comparison between baseline phase and intervention in home setting.
Visual analysis was used to determine the functional relationship between the intervention and observable parameters. A change in percentage score indicates the change in functional behaviour as observed during assessment. If the change is visible to be significant, consistent during visual analysis and aligned to the desired direction, was a clear indication of functional improvement. The visual analysis was further supplemented with quantitative analysis for evaluating the magnitude of impact using multiple non-overlapping indices for effect size and the statistical effect size was calculated using Cohen’s d between baseline to intervention (institute settings) and baseline to intervention (home settings) respectively.
The visual analysis involved evaluating level, trend, and stability of data for within phase analysis. Further the immediacy-of-effect, consistency of data patterns, and non-overlap of data was compared between baseline and respective intervention phases. When the changes (and/or variability) in level, are in the desired direction, are immediate, perceptible, and maintained over time, it is concluded that the changes in behaviour across phases is a result of the intervention and are indicative of functional improvement. This analysis was repeated for all 12 parameters for each participant and across all participants. At least three such demonstration of an intervention effect during visual analysis was necessary for establishing a functional relationship14.
Level, trend, and stability of the data within each phase was evaluated. Mean and median of percentage scores was used to report the level. An increasing or decreasing trend was observed. Within phase stability was evaluated.
by calculating the percentage of data points within 15% of the phase median. The stability criteria are satisfied if about 85% (80-90%) of the data in a phase fall within a 15% range of the median of all data points for that phase.
Between the phase analysis included observing shift in level, change in stability of data distribution, immediacy of effect, and non-overlap of data between phase. The immediacy of effect is observed by change in level, trend or variability comparing the last three data points of baseline compared with first three data points of intervention phase. Immediacy of effect is not considered between baseline and second intervention phase in home settings.
Non overlapping indices were used to calculate the magnitude of effect and quantify the proportion of measurements in the intervention phase not overlapping with the baseline measurements. Non-overlapping of All Pairs (NAP), Percentage of Non-overlapping Data (PND), Percentage of Data Exceeding the Median (PEM) were used to quantify the magnitude of effect to supplement the visual analysis21. This paper depicts the NAP as a parameter to show the magnitude effect. The significance associated with the magnitude of effect was classified as greater than 0.90 are indicative of significant impact, 0.89 to 0.70 represent moderately significant and 0.69 to 0.50 are less significant and score less than 0.50 are considered insignificant21.
The Cohen’s d was used to generate the effect size between baseline and intervention phases (first and second) respectively15. A score greater than 0.80 was considered significant, 0.79 to 0.50 represents moderately significant, 0.49 to 0.20 represent less significant and less than 0.2 is considered insignificant. The polarity of the Cohen’s d represented the alignment to the expected result, negative for decreased effect and positive for increased effect22.
Results
Preliminary analyses
The visual analysis of all baseline data across participants establishes the existence of the problem associated with the parameter as per the definition in Table 2. Quantifying the same, the minimum baseline mean (or median) > 10% is considered as problem for parameters where expected outcome is to decrease. The maximum baseline mean (or median) < 50% is considered as problem for parameters where expected outcome is to increase.
For Participant#1 and Participant#2, “self-injurious behaviour” and for Participant#3 “hyperactivity and inattention”, “repetitive behaviour” and “temper tantrums” were not the observable problems during baseline phase and thus excluded from further analysis. Supplementing data points to visual analysis within phase of level (mean), trend (slope) and stability is represented in Tables 3, 4 and 5 for cognitive, behavioural, and emotional domains respectively.
Overall, all the participants recorded more than 90% of the attendance during the intervention phase (institute settings). Participant#6 dropped during the last phase of intervention in home settings resulted in only three recorded observations, the between phase comparison for baseline (BL) vs intervention home (IH) results are not conclusive for this participant.
Primary outcomes
The visual analysis done between the phases from baseline to intervention phase (institute setting) and baseline to intervention phase (home setting), establishes the functional dependency between yoga intervention and psychological skills. This is visible in at least one or more of the parameters under cognitive, behavioural, and emotional domains respectively across all the six participants. More than three instances of change in level, immediacy of effect and sustenance of change in measure is observed for each of the participants across all the observable parameters. The data supplementing this observation is represented in Tables 3, 4 and 5 depicting the level (mean), trend (slope) and stability (consistency of data around median) for cognitive, behavioural, and emotional domains respectively. The sample immediacy of effect can be observed from graphical analysis as shown in Fig. 2.
The visual analysis for respective participants has shown the following significant changes in functional behaviours. Under cognitive domain for ‘language’ skills Participant#1 and Participant#6 shown significant improvement. For ‘reading-writing’ skills only Participant#1 shown significant improvement. For rest of the cognitive parameters none of the participants have shown a visible improvement. For Participant#6 cognitive domain reflected opposite effect. Under behavioural domain for ‘behaviour patterns’ Participant#2 and Participant#3 demonstrated significant decrease in expected behaviour changes. All the five participants shown significant reduction in ‘hyperactivity-inattention’ behaviour with Participant#3 not having the problem at first place. Except Participant#5 all other participants have shown reduction in ‘repetitive behaviour’. Under emotional domain, Participant#1, Particpant#2 and Participant#6 have shown significant improvement in ‘emotional responsiveness’, while Participant#4 and Participant#5 have shown opposite effect. ‘Violent and destructive behaviour’ of Participant#6 have shown significant reduction. Participant#1, Participant#2, and Participant#6 have shown significant reduction in ‘temper-tantrums’. The ‘self-injurious behaviour’ has significantly dropped for Participant#4 and Participant#6. The ‘odd behaviour’ of Participant#6 was significantly reduced (Tables 6, 7, 8).
The visual analysis is supplemented by the effect size calculation using non-overlap indices PND, PEM, NAP. This data is depicted in Tables 6 and 7 for respective domains and aggregated interpretation of NAP is depicted in Table 9. For this paper, the effect size calculation measure of NAP between baseline vs. intervention phase (institute settings) and baseline vs. intervention phase (home settings) is used for depiction of impact. NAP shows moderately significant to significant outcome for Participant#1, #2, #3, #4 and #6 for at least one parameter across cognitive, behavioural, and emotional domains respectively. For participant#5 it shows less significant impact.
The statistical effect size calculated using Cohen’s d between baseline vs. intervention phase (institute settings) and baseline vs. intervention phase (home settings) shows the outcome is positive and significant for at least one parameter across cognitive, behavioural, and emotional domains for Participant#1, #2, #3 and #6. For Participant#4 the results are significant only in cognitive domain and in other domains it is insignificant. For Participant#5 the outcome is insignificant across domains. The supporting data is depicted in Table 8 for respective domains and aggregated interpretation of the same is presented in Table 10.
Comparing the statistical effect along the functional changes in participants shows mismatch in few instances. The observable significant change in behaviour was not always resulted in equivalent Cohen’s d significance and/or NAP significance. For example, ‘hyperactivity-inattention’ was reduced significantly as behaviour for all participants, however, the magnitude of effect supplemented by Cohen’s d did not reflect as significant as it was. Similarly, a significant Cohen’s d and NAP score for a parameter did not reflect as actual behavioural improvement. For example, the ‘language’ skills show statistical significance for most of the participants however, it was only demonstrated by Participant#1 and Participant#6.
Overall outcome
The internal validity of effectiveness of adaptive yoga intervention is established based on visual analysis, the effectiveness is supplemented by non-overlap method NAP and statistical significance using Cohen’s d. The impact of intervention shows effectiveness across all cognitive, behavioural, and emotional domains; and across participant replications. This establishes external validity of the impact.
Effect size using non overlap method shows for the 122 observable parameters across baseline vs. intervention phases (institute and home settings) having 17% as less significant, 25% as moderately significant, 44% as significant and 14% as insignificant. Similarly, effect size using Cohen’s d shows 34% of data has significant effect, 8% of data shows moderately significant and 12% of data shows less significance. 33% of data shows the intervention impact is positive, however, insignificant and 12% of data shows opposite effect. Tables 9 and 10 represents the impact summary for NAP and Cohens’ d respectively.
Observed changes of clinical significance
There were changes observed by interventionist during the sessions and by caregivers beyond sessions. All the improvements were not consistent across all participants, and impact varied for participants from mild to moderate to significant and at an early, middle or later stage of the intervention. Few indicators and observations with examples are as follows.
Cognitive All the participants’ quality of participation and cooperation to follow the practice like, imitating the postures, following the instructions and reduced dependency on caregiver for patterning improved over time. Except Participant#2 and #5, all other participants towards end started to practice independently along with yoga interventionist in presence of caregiver as an observer. Participant#2 and Participant#4 were able to repeat the instructions at home for other family members as feedback shared by their respective caregivers.
Behavioural Repetitive behaviour for Participant#1 and Participant#6 were reduced. For example, Participant#1 used to pinch people around him that got reduced and Participant#6 used to be aggressive and hit people at times, got moderately reduced. Hyper-activity reduced gradually among all the participants. Fiddling during rest or practice reduced over time for all. Later stages they were more stable and calmer during the sessions. Participant#2 and Participant#4 could able to chant comfortably for even 5–10 min without distraction towards the end of the intervention. As shared by the caregiver, Participant#4 even continued chanting during his day-to-day activities while taking bath, and sometimes even during sleep.
Emotional Participant#6 used to demonstrate aggression which reduced over time during sessions. Also, the caregiver testified the participant had reduced temper tantrums at home.
Discussions
To the best of our knowledge, this is the first study to design and develop an integrated yoga module within a single-case experimental design to evaluate its effectiveness on the psychological health of children with multiple disabilities, specifically those having ASD and with ID, using a long-term intervention, and multi-time point approach. A distinctive feature of this study is the inclusion of caregivers and psychologists who are emotionally involved with the children and can assess them more effectively.
Considering the current condition of ASD and with ID, each child was unique and had respective ways to adapt with a stranger. Involving caregivers and being present in each of the sessions helped significantly to establish the initial connect before start of the intervention making the child feel secured and comfortable. Every day 5–10 min of the session was consumed to understand the readiness of the participant based on cues, like smile when greeted, energy level before the session, hyper activity level etc. The time it took to establish the first connect varied from participant to participant and gradually they got used to the instructor. A flexible, simplified approach made all the difference to establishing the comfort and safety of the participant. As we progress with time the participants start experiencing the comfort and safety and get along cooperating with the teacher. The duration may vary for individual participant. So, based on the readiness for each session only that portions they were comfortable were covered. The use of yoga components like movement, chanting, rest were customised to a day keeping function over form. There were few days, where depending on their readiness sessions were also cancelled as required.
The strength of the study lies in its methodological rigor, enhanced by the single-case, multiple-baseline design, and the objective assessments of psychological parameters. The long-term intervention allows for detailed insights into individual responses and trajectories of change over time. As a single-case experimental design (SCED), this study addresses the need for individualized interventions, which are crucial for mitigating the influence of time-varying social and psychological factors, and thus cannot rely on group statistical inferences. Generalizing group estimates to individuals can be, at best, ineffective and, at worst, potentially harmful23.
The participants continued with their other regular therapies served as a control environment. This adaptive yoga intervention was only additional change for the participants, strengthens the hypothesis of functional improvement of the behaviours in psychological domains. The possibility of a cross functional effects among interventions was kept out of scope for this study.
The qualitative feedback as observed and shared by the caregivers (mothers) were subjective and experiential. Few caregivers found the yoga intervention made a lot of difference in reducing hyper activity, improved quality of sleep, and eye contact during the intervention. One of the participants had shown significant improvement in verbal skills. Even post intervention the mothers were in touch with the interventionist sharing feedback over long term. Few repetitive behaviours in participants while reduced significantly during and post intervention, however, observed to be reversed due to discontinuity in practice later. The caregiver’s involvement and dedication as one of the predictors was not taken into consideration for this study, would be an interesting dimension to research in future.
There was no clear evidence for attendance of practice in home settings. Thus, the results obtained in home settings could be a carry forward effect from institute intervention or due to continued practice. This was inconclusive. There is a scope to consider the factor of change from one setting to another setting and validate the effect in future. The comparative data between institute and home settings using Cohen’s d can be referenced in Appendix C.
This study now establishes the change in functional behaviour across cognitive, behavioural, and emotional domains for children with ASD and with ID along with empirical evidence. This study now is subject to further research by replications across increased number of participants, on other psychological parameters, geographical conditions, varied severity levels with similar combinations of multiple disability, longitudinal study etc. In future, cross functional effectiveness of other therapies practiced along with yoga intervention as a complementary therapy can be researched.
Conclusion
This is a single case experimental design to study the impact of adaptive yoga intervention on the children with multiple disabilities with ASD and ID. The result suggests that a long term, consistent one-to-one adaptive yoga intervention can effectively improve the cognitive, behavioural, and emotional conditions of children having ASD and with ID. The results are observed to be satisfactory and shows mild to moderate change in each of the psychological areas for all six participants. This study establishes the potential of yoga interventions in the field of multiple disabilities. The study will unlock the perspectives of caregivers, assessing the feasibility and acceptability of yoga practices in the context of their daily routines and overall care strategies.
Data availability
The aggregate summary and analysis outcome of data are included in this published article.
References
Wolstencroft, J. et al. Mental health impact of autism on families of children with intellectual and developmental disabilities of genetic origin. JCPP Adv. 3, (2023).
Cervantes, P. E. & Matson, J. L. Comorbid symptomology in adults with autism spectrum disorder and intellectual disability. J. Autism Dev. Disord. 45, 3961–3970 (2015).
Saunders, B. S. et al. Financial and employment impact of intellectual disability on families of children with autism. Fam Syst. Health. 33, 36–45 (2015).
Okoye, C. et al. Early diagnosis of autism spectrum disorder: A review and analysis of the risks and benefits. Cureus https://doi.org/10.7759/cureus.43226 (2023).
Aleksić Veljković, A., Katanić, B. & Masanovic, B. Effects of a 12-Weeks yoga intervention on motor and cognitive abilities of preschool children. Front. Pediatr. 9, (2021).
Valentini, N., Folleto, J. & Pereira, K. R. G. The effects of yoga practice in school physical education on children’s motor abilities and social behavior. Int. J. Yoga. 9, 156 (2016).
Nanthakumar, C. The benefits of yoga in children. J. Integr. Med. 16, 14–19 (2018).
Rashedi, R. N., Rowe, S. E., Thompson, R. A., Solari, E. J. & Schonert-Reichl, K. A. A yoga intervention for young children: Self-Regulation and emotion regulation. J. Child. Fam Stud. 30, 2028–2041 (2021).
Radhakrishna, S., Nagarathna, R. & Nagendra, H. Integrated approach to yoga therapy and autism spectrum disorders. J. Ayurveda Integr. Med. 1, 120 (2010).
Reina, A. et al. Yoga for functional fitness in adults with intellectual and developmental disabilities. Int. J. Yoga. 13, 156 (2020).
Shanker, S. & Pradhan, B. Effect of yoga on the motor proficiency of children with autism spectrum disorder and the feasibility of its inclusion in special school environments. Adapted Phys. Activity Q. 39, 247–267 (2022).
Singh, N. N. & Hwang, Y. S. Mindfulness-based programs and practices for people with intellectual and developmental disability. Curr. Opin. Psychiatry. 33, 86–91 (2020).
Desikachar, T. K. V. The Heart of Yoga (Simon and Schuster, 1999).
Kratochwill, T. R. & Levin, J. R. Single-case Intervention Research (American Psychological Association (APA), 2014).
Lobo, M. A., Moeyaert, M., Baraldi Cunha, A. & Babik, I. Single-Case design, analysis, and quality assessment for intervention research. J. Neurol. Phys. Ther. 41, 187–197 (2017).
Kazdin, A. E. Single-case Research Designs (Oxford University Press, 2011).
Bentley, K. H., Kleiman, E. M., Elliott, G., Huffman, J. C. & Nock, M. K. Real-time monitoring technology in single-case experimental design research: opportunities and challenges. Behav. Res. Ther. 117, 87–96 (2019).
Tate, R. L. et al. The Single-Case reporting guideline in behavioural interventions (SCRIBE) 2016 statement. J. Clin. Epidemiol. 73, 142–152 (2016).
Chakraborty, S., Thomas, P., Bhatia, T., Nimgaonkar, V. L. & Deshpande, S. N. Assessment of severity of autism using the Indian scale for assessment of autism. Indian J. Psychol. Med. 37, 169–174 (2015).
Peshawaria, R. & Venkatesan, S. Behavioral Assessment Scales for Indian Children with Mental Retardation (Basic-MR). (1992).
Lenz, A. S. Calculating effect size in Single-Case research. Meas. Evaluation Couns. Dev. 46, 64–73 (2013).
Richman, D. M., Barnard-Brak, L. & Watkins, L. Interpreting treatment effect size from single case experimental design data: a preliminary analysis of differential effects of treatments designed to increase or decrease behaviour. J. Intellect. Disabil. Res. 66, 743–755 (2022).
Fisher, A. J., Medaglia, J. D. & Jeronimus, B. F. Lack of group-to-individual generalizability is a threat to human subjects research. Proceedings of the National Academy of Sciences 115, (2018).
Acknowledgements
I thank the Department of Clinical Psychology, NIEPMD(D), Chennai, India in supporting this research by helping with identifying participants, assessors, and providing space to conduct the study. I thank the participants, caregivers, assessors, department staff, head of the department and the institute. My sincere thanks for the support by Mr. Sumit Bose who provided technical support, ran the analyses, was the scribe and assisted in writing the paper.
Funding
No funds, grants, or other support was received.
Author information
Authors and Affiliations
Contributions
J.M. designed and executed the study, performed data analyses, and wrote the paper. S.M. & K.S. were involved in planning, guiding the study, reviewing the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of interest
Authors and co-authors have no conflict of interest in publishing this work.
Ethical approval
The study was approved by Research Committee (RC) of the National Institute for Empowerment of Persons with Multiple Disabilities (Divyangjan) (NIEPMD), Doctoral Committee (DC) and Institutional Ethics Committee (IEC) of Swami Vivekananda Yoga Anusandhana Samsthana (Deemed to-be University), Bengaluru, India. The study adhered to the approved protocol and consent process.
Informed consent
Informed consent was obtained from parents and/or legal guardians.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Maggu, J., Mohanty, S. & Sundaravadivel, K. Adaptive yoga for psychological health of children having autism spectrum disorder and with intellectual disability: single case experimental design. Sci Rep 15, 18360 (2025). https://doi.org/10.1038/s41598-025-02368-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-02368-2
