
Abstract
Minimally invasive endodontic treatment has been an important topic of discussion in recent years, particularly in endodontics. This randomized prospective clinical trial aimed to assess outcomes after at least 2 years following two distinct root canal treatment (RCT) protocols: (1) conventional treatment protocol (CP) and (2) minimally invasive protocol (MP), with a focus on the amount of root canal preparation. 175 mature permanent teeth were randomly assigned to one of two groups. The CP group was treated using ProTaper Gold systems and the continuous wave condensation technique, while the MP group underwent treatment with TruNatomy, ultrasonic-associated irrigation, calcium hydroxide (Ca[OH]₂), and a sealer-based obturation technique. The patients were recalled after a minimum of 2 years, and the outcome was dichotomized into success or failure according to strict and loose criteria, respectively. The results were analyzed statistically through chi-squared, Fisher’s exact tests or t-tests, followed by multivariable logistic regression analysis. A total of 125 teeth were analyzed, with a recall rate of 67.4% and an average follow-up period of 36 months (24–46 months). The overall success rates were 84.8% for loose criteria (CP 91.9%, MP 77.8%) and 80.8% for strict criteria (CP 88.7%, MP 71.4%), with statistically significant differences observed between the groups (p = 0.027 and p = 0.016, respectively). The MP group and the presence of sinus tract were associated with a greater risk of failure under both loose and strict criteria. Within the constraints of this protocol—which combined minimal preparation with supplemental disinfection techniques—the MP group exhibited significantly lower success rates than the CP group. While MP may offer benefits in structural preservation, clinicians should carefully weigh these advantages against the potential compromise in treatment outcomes. Trial registration: CRIS, KCT0005351. Registered on 25 August 2020.
Similar content being viewed by others

Introduction
The concept of minimally invasive treatment in dentistry is based on scientific evidence and widely applied in the treatment of dental caries1. This approach prioritizes preserving the structural integrity of original tissues, reducing patient harm, and enhancing the immune system’s natural self-healing ability to combat disease2. In endodontics, this paradigm has influenced access cavity preparation, prompting investigations into the effects of various designs on subsequent endodontic procedures3.
Preserving dentin in the coronal third of the root during instrumentation has also been identified as a key concern in minimally invasive endodontics. Small taper preparation of the coronal third of the root canal may reduce fracture risk in the cervical part of the tooth3,4. Additionally, Pinto et al.5 demonstrated that excessive apical enlargement significantly increased microcrack formation and apical transportation. Consequently, manufacturers have developed instruments with a low taper. The TruNatomy Rotary System (TN, Dentsply Sirona, Ballaigues, Switzerland) features a unique nickel-titanium (Ni-Ti) wire with a fluted diameter reaching up to 0.8 mm that preserves radicular dentin during mechanical preparation6,7. Although small taper preparation preserves coronal dentin effectively, concerns exist that reduced instrumentation may compromise root canal cleanliness8,9, and restrict plugger penetration to the apical third, potentially compromising the effectiveness of warm compaction techniques10.
However, it is important to note that minimal preparation alone may not guarantee optimal root canal debridement. Laboratory studies focusing solely on canal taper and preparation extent, such as those by Augusto et al.13 and Lima et al.14, demonstrated that reducing taper alone (0.03 vs. 0.05) did not improve canal shaping ability, fracture resistance, or dentin removal, and in some cases increased the percentage of untouched canal areas. These findings suggest that taper reduction should be carefully balanced with other disinfection strategies to ensure effective endodontic treatment outcomes.
To address potential inadequate root canal disinfection with minimally invasive instrumentation11,12, additional disinfection procedures may be necessary, such as ultrasonic-associated irrigation (UI) combined with medicament placement within the root canal system13,14. Although the application of calcium hydroxide did not show a clear benefit when assessed by culture techniques15, several clinical studies have shown that it improves the microbiological status of the root canal system16,17. Similarly, while one randomized clinical trial found no significant influence of UI on endodontic outcome18, a systematic review found that UI exhibited superior antimicrobial efficacy compared to conventional irrigation19. Furthermore, given the challenges of achieving adequate plugger penetration in minimally instrumented canals, the sealer-based obturation (SBO) technique with, a newly developed calcium silicate-based bioceramic sealer, may serve as a more practical alternative. A recent systematic review showed that SBO yielded results comparable to those of other materials20.
Despite these advances in minimally invasive endodontic techniques and materials, significant gaps in clinical outcomes research remain. While a few studies have examined postoperative pain associated with minimally invasive approaches21,22, no randomized clinical trials have assessed healing outcomes—the ultimate measure of endodontic success. Additionally, while previous laboratory studies13,14 have evaluated individual components such as reduced taper preparation in isolation, this clinical trial was designed to test a comprehensive protocol package. Our study protocol established a minimally invasive approach that integrates multiple modifications—minimal instrumentation with TruNatomy, supplementary disinfection using ultrasonic irrigation and calcium hydroxide medication, and sealer-based obturation—as a complete treatment strategy. This design decision was made to evaluate the clinical effectiveness of a realistic minimally invasive protocol as it would be implemented in practice, rather than isolating each component separately.
Therefore, this prospective randomized clinical trial aimed to assess healing outcomes of two distinct root canal treatment (RCT) approaches over a minimum follow-up period of 2 years: (1) the conventional treatment protocol (CP), using ProTaper Gold systems (PTG, Dentsply Sirona) and continuous wave condensation technique (CWC), and (2) the minimally invasive treatment protocol (MP) utilizing TN and SBO.
Materials and methods
This clinical trial received approval from the Institutional Review Board of Yonsei University Dental Hospital (no. 2-2020-0003) and was registered with the Clinical Research Information Service (CRIS, no. KCT0005351: 25/08/2020). All methods were performed in accordance with the relevant guidelines and regulations, including the Declaration of Helsinki and the CONSORT 2010 guidelines. It followed the Preferred Reporting Items for Randomized Trials in Endodontics (PRIRATE) guidelines23. Between April 2020 and March 2021, we methodically recruited healthy individuals aged 18–82 for this study. Each participant provided written consent after receiving comprehensive information detailing the objectives and procedures of the study.
Patient selection
The inclusion criteria specified healthy individuals aged 18 or older with mature permanent teeth in need of RCT. Exclusion criteria included teeth that had previously undergone treatment or initiation, periodontal pockets extending beyond the apical third of the root, recent analgesic use within 24 h before treatment, communication difficulties, and root canals that could not be negotiated within 2 mm of the radiographic apex.
Sample size determination and randomization
This clinical trial aimed to assess two main outcomes: short-term postoperative pain, previously reported in another publication22, and the long-term success rates of the protocols described in this study. Sample size determination incorporated both endpoints, with the larger of the two servings as the definitive criteria. To determine the required sample size for comparing postoperative pain between the groups, we utilized G*Power 3.1 software (Franz Faul, University of Kiel, Germany) with a 5% significance level, 80% statistical power, and an effect size of 0.5. The calculation for success rate comparisons was informed by results from a previous clinical trial investigating nonsurgical root canal treatment24. Kim et al.25 reported success rates with loose criteria as 92.3% and 94.3% used with the continuous wave condensation method with resin-based sealer and the calcium silicate sealer applied using a sealer-based obturation method, respectively. This equivalence trial was planned with a 10% equivalence limit, a 5% significance level, and 90% statistical power. Using these parameters, the calculated sample size per group was 75. To allow for a 20% dropout rate, the final estimated sample size was increased to 180 cases.
This study adhered to a thorough methodology to ensure fairness in the allocation process. Random numbers were generated by an independent assistant through the Sealed Envelope website (https://www.sealedenvelope.com/) using a 1:1 allocation ratio and random block sizes of six. The resulting allocation list was securely stored in a locked cabinet to maintain confidentiality. Access to the list was restricted to the independent assistant, who referred to it after participant inclusion but before the intervention phase. Participants were assigned an enrolment number, determining their allocation to either the CP or MP treatment groups as per the predetermined protocol.
Preoperative clinical and radiographic evaluations
Prior to treatment, all teeth were subjected to a detailed clinical and radiographic evaluation. Percussion testing and periodontal probing were performed, and the presence of any sinus tract was documented. Pulp sensibility was assessed using cold-pulp and electric-pulp tests to verify the necessity for RCT. Observing bleeding within the pulp chamber was crucial for determining pulp vitality. The absence of vital tissue within the pulp chamber indicated pulpal necrosis. Periapical radiographs were captured using extension cone paralleling devices, ensuring greater dimensional accuracy in the resulting dental X-ray images.
Treatment protocols
All procedures were carried out in a single facility by ten clinicians, including three professors and seven skilled residents from the Department of Conservative Dentistry, utilizing a dental operating microscope (OPMI pico; Carl Zeiss, Göttingen, Germany). RCT protocols strictly adhered to rubber dam isolation and were completed over two or more appointments. In the CP group, during the initial visit, an access cavity was prepared under local anesthesia (infiltration and/or block anesthesia) using high-speed burs, and the working length was determined with an electronic apex locator (DentaPort Root zx II, Morita, Irvine, USA) and confirmed by periapical radiography. Root canal shaping was performed sequentially with PTG files (S1, S2, F1, F2), finishing with PTG F2 (25/0.08) for curved canals and PTG F3 (30/0.09) for straight canals. During this process, the canals were irrigated with a 2.5% sodium hypochlorite (NaOCl) solution using a 30-gauge notched-tip needle (Sungshim Medical Co., Bucheon-si, Korea). The access cavity was temporarily sealed with a cotton pellet and restorative material (Caviton, GC Corporation, Tokyo, Japan). At the root canal filling appointment, reinstrumentation was performed using the final shaping file, followed by irrigation with the needle set 2 mm shorter than the working length, using 1 mL of 18% ethylenediamine tetraacetic acid (EDTA) solution and 3 mL of NaOCl. Properly sized gutta-percha cones (GPC) were fitted and checked via periapical radiography. The canals were soaked with NaOCl for 15 s, replacing the irrigant three times to standardize final irrigation across both groups. The canals were dried using paper points, and obturation was carried out using CWC technique. The GPC was coated with AH Plus sealer (Dentsply Sirona) and placed into the prepared canals. A heated plugger (SuperEndo Alpha 2, B & L Biotech, Ansan, Korea) was used to compact and cut the master cone, stopping 4–5 mm short of the working length. Backfilling was achieved using a thermoplastic injection system (SuperEndo Beta 2, B&L Biotech).
In the MP group, access cavity preparation, working length determination, and canal irrigation followed the same procedures as implemented in the CP group. During canal irrigation, the same 30-gauge notched-tip needle was used as in the CP group. For canal shaping, the TN system was utilized in the sequence recommended by the manufacturer: Orifice Modifier (20/0.08), Glider file (17/0.02), and Prime file (26/0.04). If the Prime file could not reach the working length easily, Small files (20/0.04) were used during canal preparation at the clinician’s discretion. The final shaping instruments were TN Prime shaping files for curved canals and Medium files (36/0.03) for straight canals. After the final instrument was used, additional disinfection procedures, such as UI and calcium hydroxide (Ca[OH]₂), were performed. Passive UI was performed using a size 15 Ni-Ti file with a 0.02 taper (Endosonic Blue, Maruchi, Wonju, Korea) positioned 2 mm short of the working length for 15 s. After drying the canals, premixed syringe-type calcium hydroxide (Ca[OH]₂) paste (Cleanical, Maruchi) was applied to the middle third of the canal, and its distribution along the canal walls was achieved with a GPC slightly smaller than the prepared canal size. The access cavity was temporarily sealed with a cotton pellet and restorative material (Caviton, GC Corporation). During the subsequent visit for root canal filling, the Ca(OH)₂ paste was removed using the final file from the previous visit, and the canals were flushed with 1 mL of EDTA followed by 3 mL of NaOCl. The fit of the GPC was verified through periapical radiography. Passive UI with NaOCl was carried out for 15 s per canal, repeated three times for uniform final irrigation. After drying the canals, a calcium silicate-based sealer (Endoseal TCS, Maruchi) was dispensed into the middle third of the canal with a 24-gauge needle tip. Matching-taper gutta-percha cones (DiaDent, Cheongjusi, Korea) were inserted up to the working length, and the GPC was sealed at the orifice level using a heated plugger. Vertical compaction of the GPC was performed with an Obtura S-Kondenser (Obtura Spartan, Earth City, MO, USA).
Outcome variables
Preoperative and postoperative pain assessment
At their initial visits, prior to recieving local anesthesia, patients were instructed to rate their preoperative pain levels on a 0–10 numerical rating scale (NRS). To assist with scoring, a modified Wong-Baker FACES scale was also provided. Patients were also contacted via phone one day after root canal filling and requested to report their pain scores.
Quality of root-filling
The quality of root canal fillings was assessed based on three criteria: sealer extrusion, root canal filling voids, and root canal filling level. Periapical radiographs taken immediately after the root canal filling procedure were independently reviewed by two blinded and calibrated examiners (S. K. and M. S.). Both sealer extrusion and root canal filling voids were classified as either present or absent. In multirooted teeth, the presence of sealer extrusion or voids in at least one root was categorized as “present.” The root canal filling level was also evaluated. Any discrepancies between the examiners regarding sealer extrusion, filling voids, or filling level were resolved through discussion to reach a final agreement.
Healing outcomes
Patients underwent annual recall appointments, which included clinical and radiographic evaluations of the treated teeth. The presence of caries or marginal leakage associated with coronal restorations was assessed by clinical inspection and periapical radiography. Only patients who completed at least 24 months of follow-up were included in the healing outcome analysis. Two blinded, independent, and calibrated examiners (S. K., M. S.) independently evaluated the preoperative and recall periapical radiographs for the periapical index (PAI)26,27. The PAI scores were as follows:
-
PAI 1:
Normal periapical structure.
-
PAI 2:
Bone structural changes indicating but not pathognomonic for apical periodontitis.
-
PAI 3:
Bone structural changes with mineral loss in apical periodontitis.
-
PAI 4:
Well-defined apical radiolucency.
-
PAI 5:
Radiolucency with the radiative expansion of bone structural changes.
For multirooted teeth, the maximum score among the roots was recorded. Clinical assessments included the evaluation of pain, swelling, the presence of sinus tract, other symptoms and overall functionality. Healing criteria were defined as a decrease in the PAI score along with the absence of clinical symptoms. According to previous research, teeth were categorized into the following three evaluation criteria based on the success or failure in analyzing the change in the PAI28.
-
1.
‘Strict’ radiographic success criteria: Asymptomatic tooth with no evidence of apical radiolucency during the follow-up assessment (Fig. 1).
-
2.
‘Loose’ radiographic success criteria: Asymptomatic tooth showing a reduction in apical radiolucency size during the follow-up assessment (Fig. 1).
-
3.
Failure: Non-functional, symptomatic teeth with no change or an increase in size of radiographic periradicular radiolucency (Fig. 2).

Representative periapical radiographs of cases in each category of success. (A) Preoperative radiograph of the first right mandibular molar tooth with a periapical lesion. (B) Postoperative radiograph after treatment with the minimally invasive protocol. (C) The 39-month follow-up radiograph shows a normal contour of the periodontal ligament, with no clinical signs and symptoms. The outcome is considered “successful” under strict criteria. (D) Preoperative radiograph of the first left mandibular molar tooth with a periapical lesion. (E) The tooth was treated with the conventional treatment protocol. (F) The 25-month follow-up radiograph shows a reduction of the former radiolucency, and the tooth was asymptomatic at the time of clinical examination. The outcome is considered ‘successful’ only under loose criteria.

Representative periapical radiographs of cases in category of failure. (A) Preoperative radiograph of the first maxillary molar tooth with a periapical lesion. (B) Postoperative radiograph after treatment with the minimally invasive protocol. (C) The 35-month follow-up radiograph still shows radiolucency around the apex of mesiobuccal root. The outcome is considered ‘failure’. (D) The preoperative radiograph of the first mandibular molar tooth with a periapical lesion. (E) The tooth was treated with the conventional treatment protocol. (F) In the 38-month follow-up radiograph, while the periapical radiolucency around the distal root has decreased, an increase in radiolucency around the mesial root can be observed. The outcome is considered ‘failure’.
Disagreements in radiographic and clinical assessments were addressed through discussion until a consensus was reached.
Statistical analysis
The t-test, Chi-square test, or Fisher’s exact test were used to analyze demographic characteristics, postoperative pain, and root canal filling quality between the two groups. Observer agreement was assessed using Cohen’s kappa test, and the healing outcomes were statistically compared through bivariate analysis, including the Chi-square test and Fisher’s exact test. Variables with a p-value of < 0.30 from the bivariate analysis were incorporated into a binary logistic regression model to identify predictors of outcomes. A stepwise method was applied to identify factors associated with the ourcome. All statistical analyses were conducted utilizing SPSS software (version 27; IBM Corp, Armonk, NY, USA).
Results
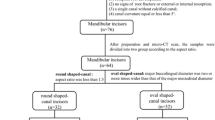
Initially, 172 participants (185 teeth) were included. Seven participants (10 teeth) were excluded because they either withdrew from the study or did not meet the inclusion criteria. After 24 months, 46 patients (49 teeth) failed to comply with the follow-up requirements, and one tooth in the MP group was extracted with no data on the periapical status (Fig. 3). Accordingly, 118 participants and 125 teeth were analyzed in the final evaluation, resulting in a recall rate of 67.4%. The average follow-up duration was 36 months (range 24–46 months), except for four cases with early failure within 2 years. All teeth analyzed in this study had permanent restorations with no evidence of marginal caries or leakage.

Flow chart of allocation of the patients (PRIRATE 2020 flowchart). CP conventional treatment protocol, MP minimally invasive treatment protocol.
For multirooted teeth, the maximum score among the roots was recorded. Healing outcomes were assessed using both strict and loose radiographic success criteria, as mentioned earlier:
-
1.
Strict criteria: Asymptomatic tooth with no apical radiolucency.
-
2.
Loose criteria: Asymptomatic tooth showing reduction in apical radiolucency size.
-
3.
Failure: Symptomatic tooth with no change or increased periradicular radiolucency.
The inter-examiner agreement for preoperative radiographic evaluation showed a Kappa score of 0.87, while the follow-up radiographic evaluation demonstrated a score of 0.79. These inter-examiner kappa values indicate ‘substantial’ to ‘almost perfect’ agreement, as defined by Landis and Koch29. The intra-examiner scores for the two evaluators, obtained from the second radiographic evaluation conducted one week later, were 0.96 and 0.95, respectively, indicating an ‘almost perfect’ level of agreement29.
The preoperative demographic characteristics were comparable between the two treatment groups, except for the presence of a sinus tract (Table 1). A total of one hundred-one teeth (80.8%) underwent RCT over two visits. The number of visits required to complete treatment did not significantly differ between the groups (p = 0.063). Postoperative pain showed identical distributions in both groups (p = 0.163). All cases achieved appropriate root canal filling levels, with the GPC located within 0–2 mm from the radiographic apex. However, sealer extrusion rates showed a significant variation between the groups (p = 0.001), while voids were similar between the groups (p = 0.833) (Table 1).
The overall success rate of the RCT was 84.8% (106/125) based on loose criteria. The CP group demonstrated a significantly higher success rate of 91.9% (57/62) compared to 77.8% (49/63) in the MP group (p = .027). Based on strict criteria, the overall success rate of the treatment was 80% (100/125). Similarly, the CP group achieved a success rate of 88.7% (55/62), which was significantly greater than the 71.4% (45/63) observed in the MP group (p = .016).
According to bivariate analysis using loose criteria, teeth without sealer extrusion had a significantly lower success rate (77.6%) compared to those with sealer extrusion (95.9%, p = .005). However, bivariate tests based on strict criteria showed that gender was a significant factor in success (p = .019). Additionally, patients without a sinus tract had a higher success rate (84%) than those with a sinus tract (57.9%) (Table 2).
Multivariable logistic regression analysis was performed based on both loose and strict criteria to exclude the possibility that these variables were associated with each other (Tables 3 and 4). After adjusting for other variables, the MP group (odds ratio [OR] = 7.59, p = .0.009) and the absence of sealer extrusion (OR = 0.09, p = .0.012), and presence of a sinus tract (OR = 7.14, p = .0.021) significantly increased the risk of failure based on the loose criteria. However, the MP group (OR = 6.75, p = .0.002), presence of a sinus tract (OR = 6.59, p = .0.007, and male participants (OR = 3.27, p = .0.022) significantly increased the risk of failure, based on strict criteria.
Discussion
This study was initiated to investigate potential differences in healing outcomes between minimally invasive endodontic treatment and conventional approaches. Given the limited research addressing clinical concerns related to irrigation and obturation in minimally prepared root canals, we established a set of protocols (MP) using Ca(OH)₂, UI, and the SBO with a calcium silicate sealer based on previous studies. To our knowledge, this is the first prospective clinical study to comparatively evaluate the long-term outcomes following MP.
Notably, the MP group exhibited significantly lower success rates compared to the CP group under both loose and strict criteria. Given that the primary etiology of pulpal and periradicular pathosis is microbiological30,31, our findings suggest that the MP employed in this study was less effective than the CP in eliminating or controlling infected tissue within the root canal system. The multiple variables between the two groups—including differences in instrument type, disinfection protocol, and obturation methods—introduced confounding factors, making it difficult to attribute the observed outcomes solely to minimal canal preparation. Given the multi-component nature of the MP protocol, which combines various modifications, the lower success rates observed in the MP group are unlikely to be solely attributable to minimal instrumentation alone, but rather may reflect the cumulative effects of multiple contributing factors.
Nevertheless, reduced dimensions of the prepared root canal system seem to be the primary factor influencing these outcomes, rather than the supplementary techniques employed. Although some clinical studies have not shown clear benefits from the UI systems or Ca(OH)₂ application15,18, numerous studies confirm their enhanced antimicrobial efficacy16,17,19,32,33. Notably, Koulogiannis et al.34 reported that the insertion depth of the ultrasonic file had minimal impact on the effectiveness of irrigation, which supports the potential for efficient cleaning even in minimally prepared canals. Moreover, a recent meta-analysis indicates that SBO with calcium silicate-based bioceramic sealers achieves outcomes comparable to other root canal filling materials and techniques in promoting the healing of apical periodontitis20. These findings collectively suggest that the reduced canal preparation dimensions in the MP group—rather than the supplementary techniques—likely account for the observed differences in success rates.
Albrecht et al.35 demonstrated that larger tapers enable irrigation needles to reach significantly closer to the apex. In clinical settings, wider tapers facilitate deeper irrigation needle penetration, allowing a greater volume of irrigant to reach the apical area. Although flexible needles are recommended for the TruNatomy system, we opted to use 30-gauge stainless steel needles in both groups. This decision was made to ensure consistency between the two treatment protocols, as flexible needles were not widely used in the clinical practice at the time and posed operational challenges in posterior teeth. Furthermore, during the course of the clinical study, we observed that these stainless-steel needles were less effective at reaching deeper portions of the root canal, particularly when the coronal third was not sufficiently enlarged. Studies have shown that PTG removes more dentin in the coronal area of mesial roots than TN 2, potentially facilitating deeper insertion of the irrigation needle in the PTG group and affecting healing outcomes. Additionally, canal taper influences the efficacy of ultrasonic irrigation (UI)36,37 and the small tapers in the MP group may have limited irrigation penetration, leading to less effective cleaning compared to the CP group.
Clinical studies have produced varied results regarding the impact of canal taper on treatment outcomes. Using strict criteria, Hoskinson, et al.38 and Ng, et al.39 found no significant differences between small (0.05) and wide (0.10) canal tapers. In contrast, under loose criteria, Smith, et al.40 reported a significantly higher success rate for “flared” preparations (wide taper) compared to “conical” preparations (narrow taper). More recently, a randomized clinical trial involving 120 patients with mandibular first molars and asymptomatic apical periodontitis revealed that canal preparations with a small taper (0.04) and less extensive apical enlargement were associated with a significantly lower success rate (57.1%) than those with a larger taper and preparation size at 1-year follow-up41. However, in the present study, as previously mentioned, it must be acknowledged that the lower success rates observed in the MP group may reflect the combined effect of multiple protocol modifications rather than minimal preparation alone. Future studies should aim to isolate individual factors—such as by combining MP instrumentation with CP irrigation—to better clarify their respective contributions to treatment outcomes.
This study employed a minimum follow-up period of 2 years, bases on evidence that most periapical lesions heal completely within this time frame28. Wu et al.42 suggested that “recall” rates lower than 50% could lead to overestimation of treatment success. In this study, the recall rate was 67.4%, which is relatively high, providing more reliable data than studies with shorter follow-up periods. Notably, patients who did not return for follow-up visits were typically asymptomatic and, during follow-up phone calls, verbally reported feeling fine and expressed a preference not to attend further visits. This suggests that the dropouts were unlikely to bias the results toward treatment failure. In fact, these dropouts may have led to an underestimation of success rates, meaning the true success rate could be higher than reported. Our overall success rates—84.8% under loose criteria and 80% under strict criteria—are consistent with those reported in a systematic review by Ng et al.28, which found success rates of 85.2% and 74.7%, respectively. However, it is important to note that this review analyzed data ranging over more than 50–60 years43. A more recent systematic review examining treatment outcomes published between 2003 and 202043 reported higher weighted pooled success rate: 92.6% for primary endodontic treatment under loose criteria (from 21 studies) and 82% under strict criteria (from 39 studies)44. While these contemporary success rates are slightly higher than our overall results, they closely resemble the outcomes achieved with our conventional protocol (CP), which demonstrated success rates of 91.9% under loose criteria and 88.7% under strict criteria.
Multivariable logistic regression analysis consistently identified the MP group and the presence of sinus tract as negative predictor of success under both loose and strict criteria, suggesting that these factors significantly influence clinical outcome. The finding that sinus tracts adversely affect periapical healing align with previous research39. Sinus tracts represent a clinical manifestation of chronic periapical disease, indicating that the host tissue’s defense mechanisms are locally overwhelmed. While the precise mechanisms underlying reduced treatment success in these conditions remain unclear, they likely relate to established, long-standing root canal infections.
Furthermore, under loose criteria, sealer extrusion was associated with an increased success rate. Sealer extrusion is more frequently observed with CWC compared to SBO25,45, and these findings were confirmed in the present study (Table 1). The association between sealer extrusion and higher success rates in this study may be attributed to the CWC technique used in the more successful CP group, which tends to produce more frequent sealer extrusion. While our multivariable logistic regression analysis attempted to control for these confounding variables, the observed association between sealer extrusion and treatment success likely reflects the overall effectiveness of the CP rather than a causal connection. Further research is necessary to determine whether sealer extrusion acts as a causal factor or correlates with the outcome.
While our analysis showed that male sex was a significant predictor of failure under strict criteria (OR = 3.27, p = 0.022), this finding warrants cautious interpretation. This gender difference was only observed under strict criteria, not loose criteria, suggesting an isolated finding rather than a true clinical pattern. Furthermore, this association has not been reported in previous endodontic outcome studies or systematic reviews46, and lacks a clear biological mechanism to support gender-based differences in periapical healing. The relatively small sample size, wide confidence intervals, and lower odds ratios compared to other factors suggest this may be an incidental finding specific to our study population rather than a clinically significant factor. Future large-scale studies with diverse patient populations are needed to determine whether this represents a genuine pattern requiring clinical consideration.
A limitation of this study is that the treatment protocol was implemented by ten clinicians with varying levels of expertise, which may have influenced the findings. However, differences in operator experience were minimized, as all clinicians, except for the professors, were senior residents with at least 2 years of experience using various Ni-Ti file systems. Although most clinicians were more familiar with PTG than TN, this experience likely minimized the impact of operator variability on treatment outcomes.
Conclusion
Within the constraints of this protocol—which combined minimal preparation with supplemental disinfection techniques—the MP group showed lower success rates than the CP group at 2-year follow-up. Further research is needed to determine whether this reflects inherent limitations of minimal preparation or interactions between protocol components. Clinicians should carefully weigh the benefits of dentin preservation against the need for effective disinfection when selecting endodontic treatment strategies.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Murdoch-Kinch, C. A. & McLean, M. E. Minimally invasive dentistry. J. Am. Dent. Assoc. 134, 87–95 (2003).
Silva, E. et al. Present status and future directions—minimal endodontic access cavities. Int. Endod J. 55 (Suppl 3), 531–587 (2022).
Yuan, K. et al. Comparative evaluation of the impact of minimally invasive preparation vs. conventional straight-line preparation on tooth biomechanics: a finite element analysis. Eur. J. Oral Sci. 124, 591–596 (2016).
Sabeti, M. et al. Impact of access cavity design and root canal taper on fracture resistance of endodontically treated teeth: an ex vivo investigation. J. Endod. 44, 1402–1406 (2018).
Pinto, J. C. et al. Effect of foraminal enlargement on microcrack formation and apical transportation: a nano-CT assessment. Sci. Rep. 13, 4881 (2023).
Peters, O. A., Arias, A. & Choi, A. Mechanical properties of a novel nickel-titanium root canal instrument: stationary and dynamic tests. J. Endod. 46, 994–1001 (2020).
Mustafa, R. et al. Evaluating in vitro performance of novel nickel-titanium rotary system (TruNatomy) based on debris extrusion and preparation time from severely curved canals. J. Endod. 47, 976–981 (2021).
Ribeiro, G., Martin, V., Rodrigues, C. & Gomes, P. Comparative evaluation of the canal shaping ability, pericervical dentin preservation, and smear layer removal of trunatomy, WaveOne gold, and protaper ultimate—an ex vivo study in human teeth. J. Endod. 49, 1733–1738 (2023).
Sarıyılmaz, Ö., Sessiz, R. & Kocaman, O. S. The impact of coronal flaring files on pericervical dentin thickness in mandibular molars. J. Endod. 50, 514–519 (2024).
Debelian, G. & Plotino, G. in Filling of Root Canals after Minimally Invasive Preparation in Minimally Invasive Approaches in Endodontic Practice 1 Edn. 109–135 (eds Plotino, G.) (Springer, 2020). https://doi.org/https://doi.org/10.1007/978-3-030-45866-9_6.
Rodrigues, R. C. V. et al. Influence of the apical Preparation size and the irrigant type on bacterial reduction in root canal-treated teeth with apical periodontitis. J. Endod. 43, 1058–1063 (2017).
Plotino, G., Özyürek, T., Grande, N. M. & Gündoğar, M. Influence of size and taper of basic root canal preparation on root canal cleanliness: a scanning electron microscopy study. Int. Endod J. 52, 343–351 (2019).
Augusto, C. M. et al. A laboratory study of the impact of ultraconservative access cavities and minimal root canal tapers on the ability to shape canals in extracted mandibular molars and their fracture resistance. Int. Endod J. 53, 1516–1529 (2020).
Lima, C. O. et al. The impact of minimally invasive root canal preparation strategies on the ability to shape root canals of mandibular molars. Int. Endod J. 53, 1680–1688 (2020).
Sathorn, C., Parashos, P. & Messer, H. Antibacterial efficacy of calcium hydroxide intracanal dressing: a systematic review and meta-analysis. Int. Endod J. 40, 2–10 (2007).
Ricucci, D., Russo, J., Rutberg, M., Burleson, J. A. & Spångberg, L. S. A prospective cohort study of endodontic treatments of 1369 root canals: results after 5 years. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 112, 825–842 (2011).
Vera, J. et al. One- versus two-visit endodontic treatment of teeth with apical periodontitis: a histobacteriologic study. J. Endod. 38, 1040–1052 (2012).
Liang, Y. H. et al. Radiographic healing after a root canal treatment performed in single-rooted teeth with and without ultrasonic activation of the irrigant: a randomized controlled trial. J. Endod. 39, 1218–1225 (2013).
Chalub, L. O. et al. Antimicrobial effectiveness of ultrasonic irrigation in root canal treatment: a systematic review of randomized clinical trials and meta-analysis. Clin. Oral Investig. 27, 1343–1361 (2023).
Sabeti, M. A., Karimpourtalebi, N., Shahravan, A. & Dianat, O. Clinical and radiographic failure of nonsurgical endodontic treatment and retreatment using single-cone technique with calcium silicate-based sealers: a systematic review and meta-analysis. J. Endod. 50, 735–746e731 (2024).
Valliappan, C. T. et al. Evaluation of postoperative pain with new heat-treated rotary and reciprocating nickel-titanium files: a randomized controlled clinical trial. J. Conserv. Dent. 26, 170–175 (2023).
Kim, D. H., Choi, Y. W., Kang, S., Shin, S. J. & Jung, I. Y. Postoperative pain of minimally invasive root canal treatment: a randomized clinical trial. Odontology. 112, 1307–1315 (2024).
Nagendrababu, V. et al. PRIRATE 2020 guidelines for reporting randomized trials in endodontics: a consensus-based development. Int. Endod J. 53, 764–773 (2020).
Flight, L. & Julious, S. A. Practical guide to sample size calculations: non-inferiority and equivalence trials. Pharm. Stat. 15, 80–89 (2016).
Kim, J. H. et al. Clinical efficacy of sealer-based obturation using calcium silicate sealers: a randomized clinical trial. J. Endod. 48, 144–151 (2022).
Orstavik, D. Time-course and risk analyses of the development and healing of chronic apical periodontitis in man. Int. Endod J. 29, 150–155 (1996).
Orstavik, D., Kerekes, K. & Eriksen, H. M. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Endod Dent. Traumatol. 2, 20–34 (1986).
Ng, Y. L., Mann, V., Rahbaran, S., Lewsey, J. & Gulabivala, K. Outcome of primary root canal treatment: systematic review of the literature—part 1. Effects of study characteristics on probability of success. Int. Endod J. 40, 921–939 (2007).
Landis, J. R. & Koch, G. G. The measurement of observer agreement for categorical data. Biometrics 33, 159–174 (1977).
Kakehashi, S., Stanley, H. R., Fitzgerald & R. J. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg. Oral Med. Oral Pathol. 20, 340–349 (1965).
Möller, A. J., Fabricius, L., Dahlén, G., Ohman, A. E. & Heyden, G. Influence on periapical tissues of Indigenous oral bacteria and necrotic pulp tissue in monkeys. Scand. J. Dent. Res. 89, 475–484 (1981).
Susila, A. & Minu, J. Activated irrigation vs. conventional non-activated irrigation in endodontics—a systematic review. Eur. Endod J. 4, 96–110 (2019).
Virdee, S. S., Seymour, D. W., Farnell, D., Bhamra, G. & Bhakta, S. Efficacy of irrigant activation techniques in removing intracanal smear layer and debris from mature permanent teeth: a systematic review and meta-analysis. Int. Endod J. 51, 605–621 (2018).
Koulogiannis, A., Walmsley, A. D., Angeli, P. & Balabani, S. Ultrasonic irrigation flows in root canals: effects of ultrasound power and file insertion depth. Sci. Rep. 14, 5368 (2024).
Albrecht, L. J., Baumgartner, J. C. & Marshall, J. G. Evaluation of apical debris removal using various sizes and tapers of profile GT files. J. Endod. 30, 425–428 (2004).
Lee, S. J., Wu, M. K. & Wesselink, P. R. The efficacy of ultrasonic irrigation to remove artificially placed dentine debris from different-sized simulated plastic root canals. Int. Endod J. 37, 607–612 (2004).
van der Sluis, L. W., Wu, M. K. & Wesselink, P. R. The efficacy of ultrasonic irrigation to remove artificially placed dentine debris from human root canals prepared using instruments of varying taper. Int. Endod J. 38, 764–768 (2005).
Hoskinson, S. E., Ng, Y. L., Hoskinson, A. E., Moles, D. R. & Gulabivala, K. A retrospective comparison of outcome of root canal treatment using two different protocols. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 93, 705–715 (2002).
Ng, Y. L., Mann, V. & Gulabivala, K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int. Endod J. 44, 583–609 (2011).
Smith, C. S., Setchell, D. J. & Harty, F. J. Factors influencing the success of conventional root canal therapy—a five-year retrospective study. Int. Endod J. 26, 321–333 (1993).
Fatima, S., Kumar, A., Andrabi, S., Mishra, S. K. & Tewari, R. K. Effect of apical third enlargement to different preparation sizes and tapers on postoperative pain and outcome of primary endodontic treatment: a prospective randomized clinical trial. J. Endod. 47, 1345–1351 (2021).
Wu, M. K., Shemesh, H. & Wesselink, P. R. Limitations of previously published systematic reviews evaluating the outcome of endodontic treatment. Int. Endod J. 42, 656–666 (2009).
Setzer, F. C. & Kim, S. Comparison of long-term survival of implants and endodontically treated teeth. J. Dent. Res. 93, 19–26 (2014).
Burns, L. E. et al. Outcomes of primary root canal therapy: an updated systematic review of longitudinal clinical studies published between 2003 and 2020. Int. Endod J. 55, 714–731 (2022).
Yu, Y. H., Kushnir, L., Kohli, M. & Karabucak, B. Comparing the incidence of postoperative pain after root canal filling with warm vertical obturation with resin-based sealer and sealer-based obturation with calcium silicate-based sealer: a prospective clinical trial. Clin. Oral Investig. 25, 5033–5042 (2021).
Ng, Y. L., Mann, V., Rahbaran, S., Lewsey, J. & Gulabivala, K. Outcome of primary root canal treatment: systematic review of the literature—part 2. Influence of clinical factors. Int. Endod J. 41, 6–31 (2008).
Acknowledgements
This work was supported by ‘Supporting Project to Evaluation New Domestic Medical Devices in Hospitals’ funded by ‘Ministry of Health and Welfare (MOHW)’ and ‘Korea Health Industry Development Institute (KHIDI)’. The authors denied any conflict of interests related to this study.
Author information
Authors and Affiliations
Contributions
Statement of Authorship Seung-Kyung Kwon: writing—original draft prepration, data curation(lead), formal analysis(supporting), investigation, visualization (lead). Minkyeong Seog: Data Curation(supporting), Formal analysis(supporting), Visualization(supporting)Dohyun Kim: Writing – Review & Editing, Formal analysis(lead), Methodology, Software, ValidationIl-Young Jung: Writing – Review & Editing, Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Validation.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical statement
This randomized clinical trial was approved by the Institutional Review Board of Yonsei University Dental Hospital (no. 2-2020-0003) and registered with the Clinical Research Information Service (CRIS, no. KCT0005351: 25/08/2020).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kwon, SK., Seog, M., Kim, D. et al. Impact of minimally invasive root canal treatment on healing outcomes in a randomized clinical trial. Sci Rep 15, 23260 (2025). https://doi.org/10.1038/s41598-025-02905-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-02905-z
