
Abstract
Evidence on paramedics’ task load is limited despite the growth of prehospital emergency medical services (EMS). This study aims to investigate the association between the clinical complexity of prehospital EMS patients and paramedics’ (EMT-P’s) perceived task load during their most recent call. In this nationwide cross-sectional study, a total of 430 paramedics attending 10 out of the 13 training groups of the “2023 Refresher Training Program for EMT-Ps” in Taiwan were asked to complete an anonymous online survey. The survey included the Chinese version of the NASA Task Load Index (NASA-TLX), which generated a global TLX score ranging from 0 to 100. The clinical complexity of the most recent call was also assessed and divided into three groups based on whether the services provided during the call involved procedures that could be performed by EMT-1, EMT-2, or EMT-P personnel. We built multivariable linear regression models to account for confounders such as paramedics’ demographics, job tenure, and details of their most recent EMS dispatch (e.g., patient information, procedures performed, and call duration.). Among the 242 (56.3%) respondents, EMT-P and/or cardiopulmonary resuscitation calls were significantly associated with a 14.04-point (95% CI: 5.01–23.07) increase in the global TLX score when compared with EMT-1 missions after adjusting for confounders. These findings were consistent across the subdimensions of NASA-TLX, specifically, mental demand and frustration. Additionally, every additional year of a patient’s age was correlated with a 0.14-point increase in paramedics’ perceived global TLX (95% CI: 0.02–0.25) after model adjustment. Handling EMS cases that require advanced clinical skills and treating older patients is associated with increased paramedics’ perceived task load. Our findings highlight the need to improve prehospital EMS workforce management in aging countries like Taiwan.
Similar content being viewed by others
Introduction
In line with the UN Sustainable Development Goals (SDGs), it is crucial to establish resilient emergency medical services (EMS) systems to effectively manage health crises, natural disasters, extreme weather events, and infectious disease outbreaks1. Within the EMS workforce, emergency medical technicians (EMTs/advanced EMTs) and paramedics (EMT-P) play a critical role in providing urgent and life-saving prehospital medical care to acute and critically ill patients2.
While these dedicated workers ensure the health and safety of communities, they themselves are at risk of experiencing psychological distress, including post-traumatic stress disorder (PTSD)3,4, fatigue/compassion fatigue5, work-related burnout6, and even suicidal thoughts7. In addition, the mental stress faced by EMS workers may be compounded by the physical demands and time-sensitive tasks they must perform8,9. Therefore, it is crucial to assess the perceived task load of EMS personnel in order to understand the mechanism of their psychological distress.
There is limited evidence on the task load of prehospital EMTs and paramedics. A pioneering study in Germany utilized the NASA Task Load Index (NASA-TLX) to assess the task load of EMT-P during prehospital emergency medicine and non-emergency care transfers8. The study found that more than 17% of prehospital emergency missions resulted in a high task load (i.e., global NASA-TLX score > 80/100), with factors such as injury severity, performance of invasive procedures, and instances of aggression identified as contributing factors8.
The evidence regarding the task load of German EMT-Ps, where the Franco-German model was adopted and emergency care was mainly provided by emergency physicians, may not be applicable to EMT-Ps in countries that follow the Anglo-American EMS system10, such as the US and Taiwan11. Although the EMS system has been evolving globally, in the Anglo-American model, EMS typically involves cooperation with public safety organizations like police and fire departments, with EMT and paramedic personnel providing rescue services. Taking Taiwan as an example, the EMS system includes three levels of personnel responsible for pre-hospital procedures: EMT-1, EMT-2, and EMT-P. Despite varying training requirements for different life-saving skills, personnel at all levels are responsible for not only EMS but also rescue operations, firefighting, and managing both emergency and non-emergency pre-hospital transfers11.
To our knowledge, no previous research has addressed the task load of EMT-Ps in countries following the Anglo-American model. Therefore, we conducted this study to investigate the level and associated factors of EMT-P’s task load in Taiwan to address this knowledge gap.
Materials and methods
Study design and setting
This national cross-sectional study was part of the “2023 Refresher Training Program for EMT-Ps,” conducted from June 26, 2023, to September 27, 2023, in Nantou County, Taiwan. The program consisted of 13 consecutive training groups, with each group participating in a three-day training program that included “Airway Management,” “Principles of Spinal and Limb Trauma Management,” “Safety for EMTs in Violent Situations,” “Types and Management of Bleeding and Shock,” and “Pre-hospital Trauma Life Support.” EMT-Ps in Taiwan must undertake 24 h of refresher training each year, with at least 96 h every three years12. Therefore, EMT-Ps needing refresher credits traveled from all over the country to attend the “2023 Refresher Training Program for EMT-Ps.” A board-certified occupational physician (F-YL), who lectured for 10 out of the 13 groups on the topic of EMS workers’ safety and health, provided the attendees with a QR code to an online anonymous survey that included the Mandarin version of the National Aeronautics and Space Administration Task Load Index (NASA-TLX) questionnaire (Additional file 1). The REDCap platform was used to construct the online survey13. EMT-Ps were invited to scan the QR code and voluntarily fill out the anonymous survey during course breaks. F-YL informed the EMT-Ps about the study before sharing the QR code. Since the survey was anonymous, EMT-Ps were advised that their voluntary completion of the survey would be considered as giving consent to participate in the study.
Due to the nature of the anonymous survey study, the Institutional Review Board (IRB) of National Yang Ming Chiao Tung University Hospital approved this study as an exempt protocol and waived the need for obtaining informed consent (No. 2024E001). All methods were performed in accordance with the Declaration of Helsinki. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines14 (Additional file 2).
Study participants
The target population was EMT-Ps in Taiwan. There was a total of 2,114 EMT-Ps nationwide in 202315. Study participants were recruited using convenient sampling, comprising 10 out of the 13 training groups of EMT-Ps that participated in the “2023 Refresher Training Program for EMT-Ps.” Of these, 430 attended one of these 10 training groups. The lecturer (F-Y L) selected the 10 groups based on his schedule, and the attendees’ group assignment was determined solely by their work shifts, independent of their preferences or interests.
Mandarin NASA-TLX questionnaire
We used the NASA-TLX to assess the task load of EMT-Ps. To minimize recall bias, we focused on the task load related to their most recent response to an EMS call. This questionnaire is a subjective, multidimensional tool that evaluates perceived task load to assess the effectiveness of a task, system, or team, among other performance metrics16. Developed by NASA’s Ames Research Center, it is widely used to assess task load across various occupations17.
The NASA-TLX consists of two parts: six subjective subscales (i.e., mental demand, physical demand, temporal demand, performance, effort, and frustration), with each ranging from 0 to 10016. The other part involves pairwise comparisons of these subscales based on perceived importance, generating individual weights to calculate global TLX scores16. The global TLX score is the weighted sum of all subscales, ranging from 0 to 100. A higher TLX score indicates a higher perceived task load.
Although the questionnaire is available in various languages16, a traditional Chinese version was unavailable. Thus, we referenced a Chinese version of the NASA-TLX from an unpublished master’s thesis, with two graduate students majoring in health and welfare policy performing the initial translation. This was followed by critical reviews from a board-certified occupational physician (F-YL) and a health economist (Y-WT) to ensure accuracy, readability, and applicability within the EMT-P population in Taiwan. The translated questionnaire (Additional file 1) achieved acceptable internal consistency (Cronbach’s alpha: 0.76) among our study population. We used the digital version in our study because there were no significant differences between paper-based and digital NASA-TLX results18.
Mission complexity
Mission complexity was determined by the tasks carried out during EMS calls and classified into three categories: EMT-1, EMT-2, and EMT-P and/or cardiopulmonary resuscitation (CPR) missions, based on the types of treatments EMT personnel of different levels can perform according to Taiwan’s regulations for EMTs. Higher-level EMTs can perform more complex emergency procedures (summarized in Additional file 3)12. Although EMT-1 can perform basic CPR, we categorized EMT-P and CPR missions together due to their complexity and high pressure.
Task load
The primary outcome was the global TLX (range: 0-100) and raw TLX (RTLX) scores (range: 0-600)17. Previous literature suggests that RTLX may be more19 or equally20 sensitive than the global TLX. The secondary outcomes were the six subscales of NASA-TLX instead of the global TLX score. All outcomes were continuous variables.
Other covariates
The questionnaire also included sociodemographic variables (e.g., sex, age, job tenure, and daily/weekly frequency responding to EMS calls) and variables related to the most recent call (e.g., patient’s sex, patient’s gender, number of procedures provided, total time of the call, and the date of the call). Sex was a binary variable: male and female. Job tenure was classified into two groups based on the median: less than or equal to ten years and greater than ten years. The total time of the call is defined as the time from when EMTs go out on duty to when they return to the fire agency. The date of the call was divided into four categories, as indicated in the questionnaire: yesterday, two to three days ago, four to five days ago, and more than one week ago. An option for “six days ago” was omitted because recalling an event from that specific timeframe could be challenging and might result in misclassification. Other covariates were continuous variables.
Statistical analysis
The literature varies in describing the statistical measures of NASA-TLX values; thus, we reported their medians with interquartile ranges (IQR) for better comparison with previous data.
Descriptive statistics tested independence between the three mission complexity groups. Fisher’s exact test was used for categorical variables due to the small sample size in some categories, and the Kruskal-Wallis test was used for continuous variables due to the non-normality of most continuous variables.
Multivariable linear regression models estimated the associations between mission complexity and task load to control potential confounding bias. Coefficients and 95% confidence intervals (CI) were calculated.
All P values presented were two-tailed; a P value < 0.05 was considered statistically significant. Data analyses were conducted using the SAS (version 9.4; SAS Institute, Inc., Cary, NC, USA) and R software (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria).
Results
Characteristics of study participant
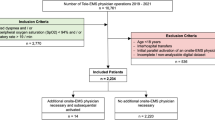
Among the 430 EMT-Ps who participated in the refresher training program, 281 consented to join the study and answered the online survey (response rate: 65.3%), with 60 (21.4%), 158 (56.2%), 61 (21.7%), and 2 (0.7%) of them from the Northern, Southern, Central Taiwan, and offshore islands, respectively. We conducted a complete-case analysis, excluding 39 EMT-Ps with missing values, resulting in a total of 242 EMT-Ps (56.2%) for data analysis (Fig. 1). The excluded respondents tended to be older (median: 42.0 vs. 38.0 years old, P < 0.01) and have more seniority in their job (87.2% vs. 68.2% job tenure > 10 years, P = 0.02).

Flow diagram of the study population selection.
Table 1 showed the characteristics of study participants. Overall, most (94.2%) of the participants were male, with a median age of 38.0 years (IQR = 8.0). Regarding the latest EMS mission complexity, 203 were classified as EMT-1 missions, 19 as EMT-2, and 20 as EMT-P and/or CPR missions. Men were more likely to report their most recent call as an EMT-1 mission. In addition, 68.6% of the patients they treated in their most recent call were male, with a median age of 60.0 years (IQR = 20.0). The EMT-P and/or CPR missions involved the greatest number of procedures performed, compared with the EMT-1 and EMT-2 missions (median [IQR] for the EMT-1, EMT-2, and EMT-P and/or CPR missions: 2 [2], 4 [3], and 7 [2], respectively, P < 0.05) (Table 1).
NASA TLX
Table 2 displayed the median TLX scores in different mission complexity groups. Overall, EMT-P and/or CPR missions were perceived to have the highest task load in terms of global TLX, RTLX, and all TLX subdimensions, except for the performance score (Table 2).
Association between mission complexity and task load
After adjusting for the participants’ sex, age, job tenure, daily/weekly frequency responding to EMS calls, and the factors related to their most recent mission (i.e., patient’s sex, patient’s age, number of provided procedures, total time of the call, and date of the call), the multiple regression results (Table 3) showed that compared to EMT-1 missions, EMT-P and/or CPR missions were significantly associated with a 14.04-point (95% CI: 5.01–23.07) increase in the global TLX score and a 73.09-point (95% CI: 22.45-123.74) increase in the RTLX score. Positive but insignificant relationships were found between EMT-2 missions and global TLX (β = 3.91, 95% CI: -4.08-11.90) and RTLX (β = 25.33, 95% CI: -19.47-70.13). In addition, during a call, EMT-Ps perceived 0.14 points higher global TLX and 0.74 points higher RTLX for every one-year increase in patient’s age (95% CI: 0.02–0.25 and 0.09–1.38, respectively) (Table 3).
Regarding the six subdimensions, EMT-P and/or CPR missions significantly increased the mental demand (β = 14.96, 95% CI: 1.47–28.44), effort (β = 15.59, 95% CI: 2.03–29.15), and frustration scores (β = 16.18, 95% CI: 3.00-29.36). EMT-2 missions were associated with an increased effort score (β = 13.47, 95% CI: 1.48–25.46). Additionally, a greater number of procedures provided during the call was associated with a higher score for RTLX (β = 6.83, 95% CI: 0.32–13.35), mental demand (β = 1.80, 95% CI: 0.06–3.53), physical demand (β = 2.05, 95% CI: 0.37–3.74), and effort (β = 1.77, 95% CI: 0.02–3.51). Those calls that took a longer time to complete were associated with higher scores for perceived RTLX (β = 21.45, 95% CI: 2.06–40.84) and temporal demand (β = 8.18, 95% CI: 3.15–13.22) (Table 3).
Discussion
This study, to our knowledge, is the first of its kind in an Asian country as well as in countries following the Anglo-American EMS model, builds on a series of studies conducted in Germany8,9, to provide insights into the task load of EMT-Ps in Taiwan.
We found that the task load of Taiwanese EMT-Ps correlates primarily with mission complexity. The task load for EMT-1 missions closely matches previous research in pre-hospital emergency medicine in Germany (median: 43.0, IQR: 21.3 vs. median: 41.0, IQR: 33.25)8. Moreover, the burden of complex emergency missions on EMT-Ps is compounded by the daily responses to EMS calls, time devoted per call, and the number of procedures provided during a call. The first two factors reflect the quantitative cumulation of the task load, while the number of procedures indicates the complexity of the emergency missions. Performing more procedures significantly increases the mental, physical, temporal, and effort-related task load. These findings highlight critical issues within the current Taiwan EMS infrastructure, particularly concerning human resource capacity and management.
Another novel finding from this study is that EMT-Ps perceived a higher task load when responding to EMS calls for older patients. As Taiwan and other developed countries enter an era with a larger elderly population, previous research has indicated that the number of EMS calls for seniors has been increasing over the past few decades and is expected to continue rising in the coming years21. Our study adds to this evidence by showing that treating an older patient is linked to a higher perceived task load compared to treating a younger patient. This suggests that the impact of the aging population on the EMS system may be more concerning than previously thought, as not only the quantity but also the quality of care for older patients will increase EMS workers’ task load. As a result, proactive strategies such as improved EMS workforce management are urgently needed to establish and sustain a resilient EMS system for aging countries like Taiwan.
In the present study, we observed a difference in gender distribution regarding calls involving varying levels of mission complexity. However, it was not possible to perform further analysis due to the small sample size of female respondents. In fact, in countries that follow the Anglo-American model, such as the US and Taiwan, EMS is primarily provided by fire departments, where male personnel are predominant. The gender distribution in our study aligns with findings from other research on US first responders22. Nonetheless, although evidence regarding EMS workers is limited, research in other fields indicates that gender differences in perceived task load exist. For example, a study on training for interventional radiology maneuvers found significant differences in perceived stress levels, self-evaluation skills, and catheter handling between untrained male and female participants23. Therefore, future large-scale studies with a greater representation of female participants are necessary to better understand gender-related differences in perceived stress and task load for EMS missions.
This study has several strengths. Firstly, we used the NASA-TLX, a widely used and validated tool, to measure the task load of EMT-Ps. Secondly, the survey was anonymous, allowing participants to provide honest answers without concerns, thereby ensuring measurement precision and accuracy and minimizing information bias. Thirdly, we constructed multiple linear regression models to account for potential confounders, thus preventing confounding bias. Finally, the study population consisted of EMT-Ps from various cities in Taiwan, including Northern, Southern, Central Taiwan, and offshore islands. Although only 0.7% of the participants were from the offshore islands, this percentage reflects Taiwan’s population distribution24. Therefore, the findings of the study may be generalizable to a larger population in Taiwan.
However, there are also some limitations. First, the use of cross-sectional surveys makes it challenging to establish a causal relationship. Second, respondents who were excluded due to incomplete data tended to have more seniority in age and job. If more experienced EMT-Ps report less task load in complex missions, our study might have overestimated the associations. Third, by asking EMT-Ps to recall their most recent response to an EMS call and related details, we may have introduced misclassification or measurement error, especially if they ran multiple calls a day and the latest workday was several days ago. Additionally, the translated NASA-TLX has not yet been validated within the Taiwanese EMS population, which could lead to information bias. However, any misclassification should be non-differentially distributed across the participants in the different mission complexity groups, leading to an underestimation of our findings. Forth, there is a possibility of the healthy worker effect, meaning those who experienced too much task load and burned out due to complex EMS missions may have left their position as an EMT-P and been unable to attend the refresher program, thereby underestimating our results. Furthermore, there may be unmeasured confounding factors associated with both mission complexity and perceived task load, such as the communication between EMS workers, the patient, and the patient’s family. However, our effect size was large enough and unlikely to be explained away by the unmeasured confounding. Finally, while a 65% response rate is considered acceptable in the literature25, the 35% non-response rate may affect the representativeness of the target population. Additionally, the distribution of respondents in the EMT-1, EMT-2, and EMT-P missions varied substantially across groups, affecting the representativeness of the findings, especially for missions with smaller sample sizes.
Conclusion
EMT-Ps experience a significant task load when handling more complex emergency missions that require advanced clinical skills. Moreover, treating older patients can further increase an EMT-P’s task load. Further large-scale longitudinal studies are needed to establish the causal relationship and explore factors that contribute to increased task load, particularly in countries with Anglo-American EMS models and aging populations, such as Taiwan.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Coates, A., Fuad, A. O., Hodgson, A. & Bourgeault, I. L. Health workforce strategies in response to major health events: A rapid scoping review with lessons learned for the response to the COVID-19 pandemic. Hum. Resour. Health 19(1), 154 (2021).
Jam, M. B., Aminizadeh, M., Akbari-Shahrestanaki, Y. & Khankeh, H. R. Evaluating the disaster preparedness of emergency medical services (EMS) facilities: A cross-sectional investigation in Iran. BMC Emerg. Med. 24(1) (2024).
Liao, D. et al. Emergency medical service personnel’ post-traumatic stress disorder and psychological detachment: The mediating role of presenteeism. Front. Public Health 11, 1030456 (2023).
Austin, C. L., Pathak, M. & Thompson, S. Secondary traumatic stress and resilience among EMS. J. Paramed. Pract. 10(6), 240–247 (2018).
Renkiewicz, G. K. & Hubble, M. W. Secondary traumatic stress in emergency services systems (STRESS) project: Quantifying and predicting compassion fatigue in emergency medical services personnel. Prehosp. Emerg. Care 26(5), 652–663 (2022).
El Mahalli, M. N. A. L. Burnout and coping methods among emergency medical services professionals. J. Multidiscip. Healthc. 13, 271–279 (2020).
Vigil, N. H. et al. Death by suicide-the EMS profession compared to the general public. Prehosp. Emerg. Care 23(3), 340–345 (2019).
Prottengeier, J. et al. Single mission workload and influencing factors in German prehospital emergency medicine—a nationwide prospective survey of 1361emergency missions. Scand. J. Trauma Resusc. Emerg. Med. 27(1), 75 (2019).
Keunecke, J. G. et al. Workload and influencing factors in non-emergency medical transfers: A multiple linear regression analysis of a cross-sectional questionnaire study. BMC Health Serv. Res. 19(1), 812 (2019).
Al-Shaqsi, S. Models of international emergency medical service (EMS) systems. Oman Med. J. 25(4), 320–323 (2010).
Huan, T. L. et al. Emergency medical services in Taiwan: Past, present, and future. J. Acute Med. 13(3), 91–103 (2023).
Laws and Regulations Database of The Republic of China (Taiwan). Regulations for Emergency Medical Technicians administration. Ministry of Health and Welfare. https://law.moj.gov.tw/LawClass/LawAll.aspx?pcode=L0020141&kw=%e6%95%91%e8%ad%b7%e6%8a%80%e8%a1%93%e5%93%a1. Accessed 25 Apr 2025.
Harvey, L. REDCap: Web-based software for all types of data storage and collection. Spinal Cord 56(7), 625 (2018).
Members of the STROBE Initiative. STROBE Checklists. https://www.strobe-statement.org/checklists/. Accessed 25 Apr 2025.
National Fire Agency, Ministry of the Interior. Emergency Medical Technician Personnel Statistics. https://www.nfa.gov.tw/cht/index.php?code=list&flag=detail&ids=21&article_id=15477. Accessed 25 Apr 2025 (2023).
Rubio, S., Díaz, E., Martín, J. & Puente, J. M. Evaluation of subjective mental workload: A comparison of SWAT, NASA-TLX, and workload profile methods. Appl. Psychol. 53(1), 61–86 (2004).
Hart, S. G. Nasa-Task Load Index (NASA-TLX); 20 years later. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting Vol. 50, 904–908 (2006).
Trujillo, A. C. & Langley Research Center. Evaluation of Electronic Formats of the NASA Task Load Index. National Aeronautics and Space Administration, Langley Research Center (2011).
Hendy, K. C., Hamilton, K. M. & Landry, L. N. Measuring subjective workload: When is one scale better than many? Hum. Factors 35(4), 579–601 (1993).
Byers, J. C., Bittner, A. C. & Hill, S. G. Traditional and Raw task load index (TLX) correlations: Are paired comparisons necessary? Adv. Ind. Ergon. Saf. 1, 481–485 (1989).
Lowthian, J. A. et al. The challenges of population ageing: Accelerating demand for emergency ambulance services by older patients, 1995–2015. Med. J. Aust. 194(11), 574–578 (2011).
Murray, M. et al. Heat-Related illness in California firefighters, 2001–2020. Am. J. Ind. Med. 68(2), 184–193 (2025).
Reder, S. R. et al. Gender differences in self-assessed performance and stress level during training of basic interventional radiology maneuvers. Eur. Radiol. 34(1), 308–317 (2024).
Department of Household Registration. Ministry of the Interior. Statistics. https://www.ris.gov.tw/app/portal/346. Accessed 25 Apr 2025.
Bennett, C. et al. Reporting guidelines for survey research: An analysis of published guidance and reporting practices. PLoS Med. 8(8), e1001069 (2011).
Acknowledgements
We are thankful to the Taiwan Association of EMS Physicians for their support in reaching the study population and gathering data.
Author information
Authors and Affiliations
Contributions
Y.-W.H., C.-H.C., H.-J.Y., C.-Y.H., Y.-W.T., and F.-Y.L. formulated the study question and research design. C.-H.L. and F.-Y.L. acquired the data. Y.-W.H., C.-H.C., H.-J.Y., C.-Y.H., Y.-W.T., and F.-Y.L. performed data analyses and drafted the manuscript. Y.-W.H., C.-H.C., H.-J.Y., C.-Y.H., Y.-H.M., C.-H.L., Y.-W.T., S.N.K., and F.-Y.L. read, contributed to the interpretation of data, critical revision of the manuscript, and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Ethics committee approval: Due to the nature of the anonymous survey study, the Institutional Review Board (IRB) of National Yang Ming Chiao Tung University Hospital approved this study as an exempt protocol and waived the need for obtaining informed consent (No. 2024E001).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
He, YW., Chueh, CH., Yu, HJ. et al. Association between prehospital medical service complexity and perceived task load of emergency calls among paramedics in Taiwan: a nationwide survey study. Sci Rep 15, 18201 (2025). https://doi.org/10.1038/s41598-025-03002-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-03002-x
