
Abstract
With the aging population, the majority of patients in acute care hospitals in high-income countries are older adults. To identify the factors associated with pressure ulcers among patients aged ≥ 75 years in an acute care hospital,we conducted a retrospective study using individual-level secondary data obtained from patient medical and nursing records. The study population was patients aged ≥ 75 years who were admitted to the hospital between March 2016 and February 2021. We fitted multivariable logistic regression models. A total of 15,258 were included in the analysis, and 513 (3.4%) patients were with pressure ulcers. The factors associated with pressure ulcers were Body Mass Index (adjusted OR = 0.96, 95% CI: 0.93–0.98); albumin level (0.51, 0.42–0.63); cardiovascular disease (2.10, 1.57–2.82); infection (1.91, 1.07–3.42); bedridden (1.85, 1.01–3.39); using bed when moving (0.45, 0.25–0.84); fecal or urine incontinence (2.44, 1.46–4.06); admission to the emergency medicine (1.71, 1.06–2.74); length of stay (1.02, 1.01–1.02); and tube feeding (2.02, 1.44–2.82). Low nutritional status, low activity levels, incontinence, cardiovascular disease, infection, admission to the emergency medicine, and more extended hospital stay were significantly associated with pressure ulcers. Therefore, nurses in acute care should carefully monitor the patients aged ≥ 75 years with these factors.
Similar content being viewed by others
Introduction
With the aging population, the majority of patients in acute care hospitals in high-income countries are older adults. For instance, in US and Canada, older adults (aged ≥ 65 years) account for approximately 30% of all patients receiving a surgical intervention and nearly half of all acute inpatients1. In Japan, adults aged 65 years and older and those aged 75 years and older accounted for 73.3% and 53.1% of all hospital admissions, and the proportion of older adults of all acute inpatients is also on the rise2. When older adults are hospitalized for acute care, they are at a higher risk for postoperative complications, readmission, delirium, and pressure ulcers3,4,5,6,7,8.
In particular, the risk of pressure ulcers (also known as pressure injuries, bedsores, pressure sores, or decubitus ulcers) is increased among older inpatients9,10,11,12,13,14. Furthermore, pressure ulcers can cause more harm than the presenting clinical conditions15,16,17,18. Pressure ulcers are sections of tissue that sustain irreversible ischemic damage from an external force that reduces or blocks blood flow to the soft tissues between the bones and the surface layer of the skin for a certain period of time19. Pressure ulcer development is associated with multiple factors, including age, patient activity and mobility, skin moisture, and perceived cognition20. Age is one of the important associated factors with pressure ulcers, suggesting that the risk of pressure ulcers increases with older age9,10. However, little is known about the factors for pressure ulcers among inpatients of the old and oldest-old (those aged ≥ 75 years) in acute care, which has increased rapidly in recent years21,22.
Since the risk of pressure ulcers is a potential determinant of care resource use, it should inform service provision planning and resource allocation; however, there are major barriers to the identification of this risk among older patients admitted to acute care hospitals. While there are tools available to measure the risk of pressure ulcers20,23,24,25,26, most tools are difficult to use and time-consuming to assess for pressure ulcers in acute care hospitals27,28,29. Therefore, there is a need for an automated system for identifying older patients at high risk for pressure ulcers using existing medical record data27,30. However, a dearth of evidence remains regarding what data from regular inpatient medical records are associated with pressure ulcers.
Among older adults aged ≥ 75 years in chronic care hospitals, nursing homes, and home care, previous studiers shows that incontinence, bedridden, or receiving tube feeding were more likely to have pressure ulcers31,32,33,34,35. However, little is known about the factors for pressure ulcers among inpatients aged ≥ 75 years in acute care. Therefore, we aimed to identify factors associated with pressure ulcers among patients of the old and oldest-old (those aged ≥ 75 years) in an acute care hospital using data from regular inpatient medical records.
Methods
Study design
This retrospective study was designed using individual-level secondary data obtained from patient medical and nursing records provided by the University of Osaka Hospital in Japan. This university hospital currently staffs 1,145 nurses and is committed to providing quality healthcare and training outstanding nurses. In 2019, the number of inpatients was 336,410, with an average hospital stay of 14.4 days36.
Participants
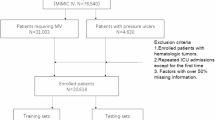
The study population was patients who were admitted to the university hospital between March 2016 and February 2021. The criteria for inclusion into the study were: (1) age 75 years or older, (2) admission to the university hospital, and (3) hospitalized between March 2016 and February 2021. Patients with missing data were excluded from the analysis.
Data collection
Data were collected using electronic medical records of the University of Osaka Hospital in Japan. We obtained individual-level secondary data between March 2016 and February 2021. We identified potentially relevant variables as previous studies, and the following variables were extracted from the electronic medical records: age9,10,14,37,38,39,40; sex14,28,39,41,42,43; body mass index [BMI]44,45; primary diagnosis (i.e., cancer, cardiovascular disease, diabetes mellitus, infection, other)10,31,38,42,46; Japan Coma Scale (i.e., level 0 [no problem], level 1 [delirium, confusion, senselessness], level 2 [stupor, lethargy, hypersomnia, somnolence, drowsiness], level 3 [deep coma, coma, semi-coma])28,48; albumin40,41,49; total protein44; hemoglobin37,49; activity level (i.e., unrestricted activity, walking to toilets, sitting up in bed, bedridden)50, transferring (i.e., walking, cane or rollator, wheelchair, bed)28,40; toileting (i.e., toilet use, use of portable toilet, fecal or urine incontinence)39,49; and history of smoking (yes or no)51,52. As for the hospital environment and treatment, the following variables were extracted: type of admission (unscheduled admission or scheduled admission)53; hospital ward (i.e., surgery, internal medicine, sensory, skin, and motor function, emergency medicine, other)28,39; length of stay [LOS]39,40,42,46,49,50,54,55; surgical treatment during stay (yes or no)14; bed rest as a treatment during stay (yes vs. no)14,56,57; use of feeding tube during stay (yes or no)38,39; parenteral nutrition during stay (yes or no)38,39; and respirator use during stay (yes or no)32,43.
Data analysis
Using ‘pressure ulcer’ (bivariate) as the dependent variable, we fitted multivariable logistic regression models to determine the factors associated with pressure ulcers among patients of the old and oldest-old (those aged ≥ 75 years) in an acute care hospital. All odds ratios (ORs) were calculated with regard to the identified potentially relevant variables: basic patient information, primary diseases, coma levels, nutritional status, activity levels, transferring, toileting, smoking, types of admission, hospital wards, length of stay, surgical treatment, bed rest as a treatment, use of feeding tube, parental nutrition, and respirator use. All potentially relevant variables were included in the models unless there was strong evidence of collinearity, as reflected by a variance inflation factor greater than 10. List-wise deletion was used to address missing values. All reported model p values were considered significant at p < 0.05. All analyses were performed using Stata 16 (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC, https://www.stata.com/stata16/).
Validity and reliability
In the sensitivity analysis, we restricted the patients of the LOS ≤ 3 days, excluding short-term hospitalizations that are less likely to be related to pressure ulcers49. Moreover, we restricted the patients with BMI > 30, excluding obese, because BMI and the likelihood of having pressure ulcers have a U-shaped relationship39,58.
Ethical consideration
Ethical considerations were in accordance with the Japanese epidemiological guidelines for secondary data analysis. Ethical approval for the study was obtained from the institutional review board at the University of Osaka Hospital in Japan (approval number: 20569). The study used de-identified data (fully anonymized prior to receipt of the data); therefore, the need for obtaining written informed consent was waived by the Institutional Review Board of the University of Osaka Hospital, Japan.
Results
Patient characteristics
Of the 23,210 patients identified, 15,258 met the inclusion criteria and were included in the analysis. Total blood protein was the most frequently missing variable, absent in 3,352 patients (14.4%), followed by albumin, which was missing in 2,581 patients (11.1%). Among the 15,258 patients analyzed, 7,989 (52.4%) were male. The median age was 79 years (interquartile range [IQR]: 77–83), and the mean body mass index (BMI) was 21.9 (standard deviation [SD]: 3.5). A total of 4,609 patients (30.2%) had cancer, and 3,563 (23.4%) had cardiovascular disease (Table 1). Regarding the hospital environment, 597 (2.3%) were admitted to the ward of emergency medicine, and the median LOS was 12 (6–22) days. The proportions of patients with and without pressure ulcers were 3.4% and 96.6%, respectively.
Among the 513 (3.4%) patients with pressure ulcers, the mean BMI was 20.7 (3.6), 190 (37.0%) had cardiovascular diseases, 106 (20.7%) had cancers, 27 (5.3%) had infections, 107 (20.8%) were unresponsiveness or coma, the mean albumin was 3.3 (0.7), 219 (42.7%) were bedridden, and 241 (27.0%) were fecal or urine incontinence. In addition, 104 (20.3%) were admitted to the ward of emergency medicine, the median LOS was 23 (11–42) days, and 153 (29.8%) required respirators.
Among the 14745 (96.6%) patients without pressure ulcers, the mean BMI was 21.9 (3.5), 4503 (30.5%) had cancers, 3373 (22.9%) had cardiovascular diseases, 201 (1.4%) had infections, 517 (3.5%) were unresponsiveness or coma, and the mean albumin was 3.8 (0.5), 2816 (19.1%) were bedridden, and 3113 (21.1%) were fecal or urine incontinence. Furthermore, 104 (20.3%) were admitted to the ward of emergency medicine, the median LOS was 23 (11–42) days, and 153 (29.8%) required respirators.
Logistic regression analysis
Regarding the multilevel logistic regression analysis, the factors associated with pressure ulcers were BMI (adjusted OR = 0.96, 95% CI: 0.93–0.98); cardiovascular disease (2.10, 1.57–2.82); infection (1.91, 1.07–3.42); Japan Come Scale level 1 (1.58, 1.01–2.48); albumin level (0.51, 0.42–0.63); walking to toilets (1.52, 1.02–2.27), bedridden (1.85, 1.01–3.39); using bed when moving (0.45, 0.25–0.84); fecal or urine incontinence (2.44, 1.46–4.06); admission to the emergency medicine (1.71, 1.06–2.74); LOS (1.02, 1.01–1.02); and tube feeding (2.02, 1.44–2.82). A summary of all factors considered and their corresponding p values in the multivariable logistic regression are shown in Table 2. We found that low BMI, cardiovascular disease, infection, Japan Come Scale level 1, a low albumin level, walking to the toilet, being bedridden, using a bed when moving, fecal or urinary incontinence, emergency ward admission, LOS, and tube feeding were significantly associated with pressure ulcers.
Results of sensitivity analyses
First, we restricted patients of LOS ≤ 3 days, excluding 993 (6.5%) patients for the multilevel logistic regression analysis. The sensitivity analysis among patients of LOS ≤3 days showed that the factors significantly associated with pressure ulcers were BMI (0.95, 0.93–0.98); cardiovascular disease (2.17, 1.60–2.92); infection (2.11, 1.16–3.82); albumin level (0.52, 0.42–0.64); walking to toilets (1.61, 1.07–2.41); bedridden (2.15, 1.13–4.07); use a bed when moving (0.44, 0.24–0.83); fecal or urine incontinence (2.31, 1.37–3.92); admission to the emergency medicine (1.71, 1.05–2.79); LOS (1.02, 1.01–1.02); and tube feeding (1.90, 1.34–2.68).
Second, we restricted patients with BMI > 30, excluding 258 (1.7%) patients for the multilevel logistic regression analysis. The sensitivity analysis among patients with BMI > 30 showed that the factors significantly associated with pressure ulcers were BMI (0.96, 0.93–0.99); cardiovascular disease (2.12, 1.58–2.84); infection (1.87, 1.04–3.37); albumin level (0.51, 0.42–0.63); walking to toilets (1.54, 1.03–2.31); bedridden (1.90, 1.03–3.51); use a bed when moving (0.44, 0.24–0.81); fecal or urine incontinence (2.47, 1.48–4.13); admission to the emergency medicine (1.72, 1.07–2.78); LOS (1.02, 1.01–1.02); and tube feeding (2.01, 1.43–2.81).
Discussion
We conducted multivariable logistic regression analyses to identify the factors associated with pressure ulcers among patients aged ≥ 75 years in an acute care hospital using data from regular inpatient medical records. We found that low BMI, cardiovascular disease, infection, Japan Come Scale level 1, a low albumin level, walking to toilets, bedridden, using bed when moving, fecal or urine incontinence, admission to the emergency medicine, LOS, and tube feeding were significantly associated with pressure ulcers.
We found that patients aged ≥ 75 years in acute care who were admitted to the ward of emergency medicine, with a longer hospital stay, cardiovascular diseases, or infections were more likely to have pressure ulcers as well as among all adult patients receiving acute care46,48,49,50,59. Notably, the odds of having pressure ulcers were nearly twice as high among patients with cardiovascular diseases or infections compared to those with cancer. These findings were consistent with prior studies reporting an increased risk of pressure ulcers in patients with cardiovascular disease60,61. Specifically, individuals with left main or triple-vessel coronary lesions exhibit higher susceptibility to pressure ulcers60. Patients undergoing cardiac surgery were also considered had high-risk, with contributing factors such as prolonged operative time, intraoperative hypothermia, vascular pathology, and postoperative use of vasoconstrictive agents, all of which may impair skin and soft tissue perfusion, increasing pressure ulcer risk61. These results underscore the need for careful pressure ulcer monitoring in acute care settings for patients with cardiovascular diseases, infections, prolonged hospitalization, or emergency admissions, regardless of age.
Patients aged ≥ 75 years in acute care who were incontinence, bedridden, or receiving tube feeding were more likely to have pressure ulcers, which are in line with previous evidence in chronic care hospitals, nursing homes, and home care31,32,33,34,35. In this study, the odds of having pressure ulcers was 2.44 in incontinence as without incontinence. Incontinence, bedridden, and tube feeding are important factors associated with pressure ulcers among older adults aged ≥ 75 years, regardless of where they receive care. These findings indicate that healthcare providers and caregivers of older adults aged ≥ 75 years should pay sufficient attention to pressure ulcers when the older adults are incontinence, bedridden, or receiving tube feeding.
Patients who had low BMI or a low albumin level were more likely to have pressure ulcers among patients aged ≥ 75 years in acute care. In particular, the odds of having a pressure ulcer decreased by about half when albumin levels increased by one. These findings are consistent with those of previous studies that showed that patients with malnutrition and underweight were more likely to develop pressure ulcers41,43, which suggests that assessments of albumin level and BMI are essential to identify patients with pressure ulcers even in the patients aged ≥ 75 years. This study has limitations as well as strengths. First, owing to the observational study design and analysis of secondary data, no data on several potential confounders, including skin status, were obtained20,62,63. However, the aim of this study was to identify factors associated with pressure ulcers using data from existing inpatient electronic medical records. The data obtained from inpatient electronic medical records were beneficial in elucidating the factors associated with pressure ulcers in older inpatients. Second, because this study was conducted on patients admitted to a single university hospital, it is uncertain how our findings may apply to patients in other acute care hospitals and other countries. Further studies should be conducted on patients in a wide variety of acute care hospitals and examine the generalizability of these findings. Third, acute care hospitals in Japan have a nurse dedicated to the management of pressure ulcers, who assists nurses in the wards with pressure ulcer care. Moreover, all patients were assessed for pressure ulcers and received preventive measures, which may have influenced the results. However, to the best of our knowledge, this is the first study to investigate the factors associated with pressure ulcers among inpatients aged ≥ 75 years in an acute care hospital using data from inpatient electronic medical records.
Conclusions
We examined the factors associated with pressure ulcers among patients aged ≥ 75 years in an acute care hospital using data from regular inpatient medical records. Low BMI, cardiovascular disease, infection, Japan Come Scale level 1, a low albumin level, walking to toilets, bedridden, using bed when moving, fecal or urine incontinence, admission to the emergency medicine, length of hospital stay, and tube feeding were significantly associated with pressure ulcers among inpatients aged ≥ 75 years in acute care. Therefore, patients aged ≥ 75 year with these factors associated with pressure ulcers should be carefully monitored by nurses in acute care.
Data availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request and with permission from the University of Osaka Hospital in Japan.
Change history
26 August 2025
A Correction to this paper has been published: https://doi.org/10.1038/s41598-025-17041-x
Abbreviations
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- IQR:
-
Interquartile range
- LOS:
-
Length of stay
- OR:
-
Odds ratio
- SD:
-
Standard deviation
References
Khadaroo, R. G. et al. Clinical effectiveness of the elder-friendly approaches to the surgical environment initiative in emergency general surgery. JAMA Surg. 155(4), e196021 (2020).
Japan MoHLaWo. Overview of patient surveys. 2017. https://www.mhlw.go.jp/toukei/saikin/hw/kanja/17/index.html (2017).
Ho, V. P., Schiltz, N. K., Reimer, A. P., Madigan, E. A. & Koroukian, S. M. High-risk comorbidity combinations in older patients undergoing emergency general surgery. J. Am. Geriatr. Soc. 67(3), 503–510 (2019).
Saravana-Bawan, B. et al. Incidence and predictors of postoperative delirium in the older acute care surgery population: a prospective study. Can. J. Surg. 62(1), 33–38 (2019).
Hasemann, W. et al. A before and after study of a nurse led comprehensive delirium management programme (DemDel) for older acute care inpatients with cognitive impairment. Int. J. Nurs. Stud. 53, 27–38 (2016).
Shin, J., Han, S. H., Choi, J., Kim, Y. S. & Lee, J. Importance of geriatric syndrome screening within 48 hours of hospitalization for identifying readmission risk: A retrospective study in an acute-care hospital. Ann. Geriatr. Med. Res. 24(2), 83–90 (2020).
McElhinny, M. L. & Hooper, C. Reducing hospital-acquired heel ulcer rates in an acute care facility: an evaluation of a nurse-driven performance improvement project. J. Wound Ostomy Cont. Nurs. 35(1), 79–83 (2008).
Aygör, H. E. et al. Features of pressure ulcers in hospitalized older adults. Adv. Skin. Wound Care. 27(3), 122–126 (2014).
Perneger, T. V. et al. Screening for pressure ulcer risk in an acute care hospital: development of a brief bedside scale. J. Clin. Epidemiol. 55(5), 498–504 (2002).
Slowikowski, G. C. & Funk, M. Factors associated with pressure ulcers in patients in a surgical intensive care unit. J. Wound Ostomy Cont. Nurs. 37(6), 619–626 (2010).
Jaul, E., Barron, J., Rosenzweig, J. P. & Menczel, J. An overview of co-morbidities and the development of pressure ulcers among older adults. BMC Geriatr. 18(1), 305 (2018).
Li, Z., Lin, F., Thalib, L. & Chaboyer, W. Global prevalence and incidence of pressure injuries in hospitalised adult patients: A systematic review and meta-analysis. Int. J. Nurs. Stud. 105, 103546 (2020).
Lindgren, M., Unosson, M., Fredrikson, M. & Ek, A. C. Immobility–a major risk factor for development of pressure ulcers among adult hospitalized patients: a prospective study. Scand. J. Caring Sci. 18(1), 57–64 (2004).
Perneger, T. V., Héliot, C., Raë, A. C., Borst, F. & Gaspoz, J. M. Hospital-acquired pressure ulcers: risk factors and use of preventive devices. Arch. Intern. Med. 158(17), 1940–1945 (1998).
Khor, H. M. et al. Determinants of mortality among older adults with pressure ulcers. Arch. Gerontol. Geriatr. 59(3), 536–541 (2014).
Manzano, F. et al. Hospital-acquired pressure ulcers and risk of hospital mortality in intensive care patients on mechanical ventilation. J. Eval Clin. Pract. 20(4), 362–368 (2014).
Bauer, K., Rock, K., Nazzal, M., Jones, O. & Qu, W. Pressure ulcers in the united States’ inpatient population from 2008 to 2012: results of a retrospective nationwide study. Ostomy Wound Manage. 62(11), 30–38 (2016).
Gorecki, C. et al. Impact of pressure ulcers on quality of life in older patients: a systematic review. J. Am. Geriatr. Soc. 57(7), 1175–1183 (2009).
Hasegawa, M. et al. Wound, pressure ulcer and burn guidelines – 1: guidelines for wounds in general, second edition. J. Dermatol. 47(8), 807–833 (2020).
Tschannen, D. & Anderson, C. The pressure injury predictive model: A framework for hospital-acquired pressure injuries. J. Clin. Nurs. 29(7–8), 1398–1421 (2020).
Wann-Hansson, C., Hagell, P. & Willman, A. Risk factors and prevention among patients with hospital-acquired and pre-existing pressure ulcers in an acute care hospital. J. Clin. Nurs. 17(13), 1718–1727 (2008).
Jenkins, M. L. & O’Neal, E. Pressure ulcer prevalence and incidence in acute care. Adv. Skin. Wound Care. 23(12), 556–559 (2010).
Defloor, T. & Grypdonck, M. F. Validation of pressure ulcer risk assessment scales: a critique. J. Adv. Nurs. 48(6), 613–621 (2004).
Moore, Z. E. & Patton, D. Risk assessment tools for the prevention of pressure ulcers. Cochrane Database Syst. Rev. 1(1), Cd006471 (2019).
Moore, Z. E. & Cowman, S. Risk assessment tools for the prevention of pressure ulcers. Cochrane Database Syst. Rev.(2), Cd006471 (2014).
Pancorbo-Hidalgo, P. L., Garcia-Fernandez, F. P., Lopez-Medina, I. M. & Alvarez-Nieto, C. Risk assessment scales for pressure ulcer prevention: a systematic review. J. Adv. Nurs. 54(1), 94–110 (2006).
Jin, Y., Kim, H., Jin, T. & Lee, S. M. Automated fall and pressure injury risk assessment systems: nurses’ experiences, perspectives, and lessons learned. Comput. Inf. Nurs. 39(6), 321–328 (2021).
Nakagami, G. et al. Supervised machine learning-based prediction for in-hospital pressure injury development using electronic health records: A retrospective observational cohort study in a university hospital in Japan. Int. J. Nurs. Stud. 119, 103932 (2021).
Norton, D. M. R. & Exton-Smith, A. N. An Investigation of Geriatric Nursing Problems in Hospital. 2nd ed. (Churchill Living Stone, 1975).
Ibrahim, K. et al. Can routine clinical data identify older patients at risk of poor healthcare outcomes on admission to hospital? BMC Res. Notes. 10(1), 384 (2017).
Cox, J. & Roche, S. Vasopressors and development of pressure ulcers in adult critical care patients. Am. J. Crit. Care. 24(6), 501–510 (2015).
Brandeis, G. H., Ooi, W. L., Hossain, M., Morris, J. N. & Lipsitz, L. A. A longitudinal study of risk factors associated with the formation of pressure ulcers in nursing homes. J. Am. Geriatr. Soc. 42(4), 388–393 (1994).
Ooi, W. L., Morris, J. N., Brandeis, G. H., Hossain, M. & Lipsitz, L. A. Nursing home characteristics and the development of pressure sores and disruptive behaviour. Age Ageing. 28(1), 45–52 (1999).
Reed, R. L., Hepburn, K., Adelson, R., Center, B. & McKnight, P. Low serum albumin levels, confusion, and fecal incontinence: are these risk factors for pressure ulcers in mobility-impaired hospitalized adults? Gerontology 49(4), 255–259 (2003).
Berlowitz, D. R. & Wilking, S. V. Risk factors for pressure sores. A comparison of cross-sectional and cohort-derived data. J. Am. Geriatr. Soc. 37(11), 1043–1050 (1989).
Hospital, O. U. Osaka University Hospital Outline 2021. https://www.hosp.med.osaka-u.ac.jp/2021_outline_all.pdf (2021).
Haleem, S., Heinert, G. & Parker, M. J. Pressure sores and hip fractures. Injury 39(2), 219–223 (2008).
Artico, M. et al. Prevalence, incidence and associated factors of pressure injuries in hospices: A multicentre prospective longitudinal study. Int. J. Nurs. Stud. 111, 103760 (2020).
Kayser, S. A., VanGilder, C. A. & Lachenbruch, C. Predictors of superficial and severe hospital-acquired pressure injuries: A cross-sectional study using the international pressure ulcer prevalence™ survey. Int. J. Nurs. Stud. 89, 46–52 (2019).
Raju, D., Su, X., Patrician, P. A., Loan, L. A. & McCarthy, M. S. Exploring factors associated with pressure ulcers: a data mining approach. Int. J. Nurs. Stud. 52(1), 102–111 (2015).
Ülker Efteli, E. & Yapucu Günes, Ü. A prospective, descriptive study of risk factors related to pressure ulcer development among patients in intensive care units. Ostomy Wound Manage. 59(7), 22–27 (2013).
Cremasco, M. F., Wenzel, F., Zanei, S. S. & Whitaker, I. Y. Pressure ulcers in the intensive care unit: the relationship between nursing workload, illness severity and pressure ulcer risk. J. Clin. Nurs. 22(15–16), 2183–2191 (2013).
O’Brien, D. D., Shanks, A. M., Talsma, A., Brenner, P. S. & Ramachandran, S. K. Intraoperative risk factors associated with postoperative pressure ulcers in critically ill patients: a retrospective observational study. Crit. Care Med. 42(1), 40–47 (2014).
Jaul, E. & Calderon-Margalit, R. Systemic factors and mortality in elderly patients with pressure ulcers. Int. Wound J. 12(3), 254–259 (2015).
Shahin, E. S. et al. The relationship between malnutrition parameters and pressure ulcers in hospitals and nursing homes. Nutrition 26(9), 886–889 (2010).
Yepes, D., Molina, F., León, W. & Pérez, E. Incidence and risk factors associated with the presence of pressure ulcers in critically ill patients. Med. Intensiva. 33(6), 276–281 (2009).
Frankel, H., Sperry, J. & Kaplan, L. Risk factors for pressure ulcer development in a best practice surgical intensive care unit. Am. Surg. 73(12), 1215–1217 (2007).
Boyle, M. & Green, M. Pressure sores in intensive care: defining their incidence and associated factors and assessing the utility of two pressure sore risk assessment tools. Aust Crit. Care. 14(1), 24–30 (2001).
Theaker, C., Mannan, M., Ives, N. & Soni, N. Risk factors for pressure sores in the critically ill. Anaesthesia 55(3), 221–224 (2000).
Sayar, S. et al. Incidence of pressure ulcers in intensive care unit patients at risk according to the waterlow scale and factors influencing the development of pressure ulcers. J. Clin. Nurs. 18(5), 765–774 (2009).
Suriadi, S. H., Sugama, J., Thigpen, B. & Subuh, M. Development of a new risk assessment scale for predicting pressure ulcers in an intensive care unit. Nurs. Crit. Care. 13(1), 34–43 (2008).
Sanada, H. et al. Risk factors in the development of pressure ulcers in an intensive care unit in Pontianak, Indonesia. Int. Wound J. 4(3), 208–215 (2007).
Kaitani, T., Tokunaga, K., Matsui, N. & Sanada, H. Risk factors related to the development of pressure ulcers in the critical care setting. J. Clin. Nurs. 19(3–4), 414–421 (2010).
Fife, C. et al. Incidence of pressure ulcers in a neurologic intensive care unit. Crit. Care Med. 29(2), 283–290 (2001).
Tayyib, N., Coyer, F. & Lewis, P. Saudi Arabian adult intensive care unit pressure ulcer incidence and risk factors: a prospective cohort study. Int. Wound J. 13(5), 912–919 (2016).
Moore, Z. E., van Etten, M. T. & Dumville, J. C. Bed rest for pressure ulcer healing in wheelchair users. Cochrane Database Syst. Rev. 10(10), Cd011999 (2016).
Thomas, D. R. Prevention and treatment of pressure ulcers. J. Am. Med. Dir. Assoc. 7(1), 46–59 (2006).
Cai, S., Rahman, M. & Intrator, O. Obesity and pressure ulcers among nursing home residents. Med. Care. 51(6), 478–486 (2013).
Eachempati, S. R., Hydo, L. J. & Barie, P. S. Factors influencing the development of decubitus ulcers in critically ill surgical patients. Crit. Care Med. 29(9), 1678–1682 (2001).
Wang, Y. et al. Predictive value of pressure ulcer risk for obstructive coronary artery disease. Nurs. Open. 8(4), 1848–1855 (2021).
Lee, H. J. et al. Risk factors for heel pressure injury in cardiovascular intensive care unit patients. Int. Wound J. 19(5), 1158–1164 (2022).
Coleman, S. et al. A new pressure ulcer conceptual framework. J. Adv. Nurs. 70(10), 2222–2234 (2014).
Alderden, J., Rondinelli, J., Pepper, G., Cummins, M. & Whitney, J. Risk factors for pressure injuries among critical care patients: A systematic review. Int. J. Nurs. Stud. 71, 97–114 (2017).
Acknowledgements
We thank staff members at the Division of Nursing and Department of Medical Informatics, the University of Osaka Hospital in Japan, for assisting with collecting data from electronic medical records.
Author information
Authors and Affiliations
Contributions
All authors contributed substantially to the conception and design; ST, KA, KK, RN, YN, TM, SM and TT collected data; SI drafted the article; SI performed the statistical analysis; SI, SY, RY, ST, KA, KK, TT and YM interpreted the data; all authors critically revised the article for important intellectual content; and all authors made meaningful contributions to the final submitted manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical considerations were in accordance with the Japanese epidemiological guidelines for secondary data analysis. Ethical approval for the study was obtained from the institutional review board at Osaka University Hospital in Japan (approval number: 20569). The study used de-identified data (fully anonymized prior to receipt of the data); therefore, participant consent was exempted by the Institutional Review Board of Osaka University Hospital, Japan.
Competing interests
SI, KK, and MK: Department of Genome Informatics is an endowment department, supported with an unrestricted grant from NEC Corporation. All other authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained errors in the Results section, where three instances of the ‘median LOS days’ in parenthesis were mistakenly stated as reference citations due to a technical error in Production. Full information regarding the corrections made can be found in the correction for this Article.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Itoh, S., Yokota, S., Yotsu, R.R. et al. Factors associated with pressure ulcers among middle-old and oldest-old inpatients in an acute care hospital. Sci Rep 15, 23538 (2025). https://doi.org/10.1038/s41598-025-03937-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-03937-1
