
Abstract
High low-density lipoprotein cholesterol are a significant risk factor for ischemic stroke. This study aims to analyze the burden of disease and temporal trends of ischemic stroke attributable to high LDL-C (IS-hLDL-C) in China, thereby providing a scientific basis for the development of effective prevention and intervention strategies. This study extracted the age-standardized mortality rates (ASMRs) and age-standardized disability-adjusted life years rates (ASDRs) of IS-hLDL-C from the global burden of disease (GBD) 2021. Stratified analysis was performed by gender and age groups. Joinpoint regression models were used to calculate average annual percentage changes (AAPC) to assess trends in IS-hLDL-C burden between 1990 and 2021. Age-period-cohort (APC) model to estimate the independent effects of age, period, and cohort on IS-hLDL-C burden. In 2021, the total number of IS-hLDL-C deaths in China was 300,052 (95% UI 92,515–527,456), and disability-adjusted life years (DALYs) was 6,850,565 (95% UI 2,313,203 − 11,418,167). From 1990 to 2021, ASMRs changed from 18.23 (95% CI 5.52–33.43) to 15.93 (95% CI 4.83–28.08), and the AAPC was −0.47 (95% CI −0.83 to −0.10). The ASDRs decreased from 385.65 (95% CI 129.83 to 647.51) in 1990 to 335.59 (95% CI 112.75 to 566.25) in 2021, with an AAPC of −0.49 (95% CI −0.83 to −0.10). Sex-stratified analysis showed that male had greater ASMRs and ASDRs than female. Age-stratified analysis showed that the burden was greatest among the elderly. In the age-period-cohort analysis, the age effect of IS-hLDL-C showed a continuous increasing trend during the study period. The period effect generally showed a positive trend during the study period. From 1990 to 2021, while the ASMRs and ASDRs related to IS-hLDL-C have decreased in China, the absolute numbers of deaths and DALYs remain substantial. The burden of IS-hLDL-C disease is disproportionately higher among male and the elderly. Given large population and the ongoing trend of population aging, it is essential to consider various lipid-lowering strategies in the future to allocate healthcare resources effectively and reduce the disease burden associated with IS-hLDL-C.
Similar content being viewed by others

Introduction
Stroke is the second leading cause of death and disability globally and ranks among the top three causes of death in China1,2. In 2019, stroke was responsible for approximately 6.55 million deaths and 143 million disability-adjusted life years (DALYs) worldwide1. In China, stroke caused 3.94 million deaths and was the leading cause of DALYs, totaling 40.55 million3. Ischemic stroke (IS) accounts for about 85% of all strokes. It is characterized by blockage or severe stenosis of cerebral blood vessels, which leads to reduced cerebral blood flow or insufficient oxygen supply to the brain, resulting in necrosis of brain tissue within the affected cerebral blood supply area1. Despite significant advancements in prevention, diagnosis, and treatment, the burden of ischemic stroke remains substantial. From 1990 to 2019, the number of deaths attributed to IS in China increased by 226.5%3.
Ischemic stroke is highly preventable, with 90% of the stroke burden attributable to modifiable risk factors4. These factors primarily include high low-density lipoprotein cholesterol (hLDL-C), high systolic blood pressure, high fasting plasma glucose, and high body mass index5,6. Rapid economic development in China has led to significant changes in dietary patterns, lifestyle habits, and work environments, contributing to hyperlipidemia as a major public health concern7,8. Since 1990, approximately 610,000 IS deaths worldwide have been attributed to hLDL-C, accounting for 22.4% of all IS deaths9. Concurrently, the number of IS deaths attributed to hLDL-C has risen by 47.8%9. High LDL-C not only heightens the risk of IS but also adversely affects the prognosis of IS patients. For instance, a large prospective cohort study conducted in China revealed that IS patients with average LDL-C levels < 1.80 mmol/L exhibited a 50% lower risk of recurrent stroke compared to those with LDL-C levels ≥ 1.80 mmol/L10. The pathological mechanism by which LDL-C increases the risk of IS primarily involves its deposition on the vascular walls, promoting the formation of atherosclerotic plaques, inducing inflammatory responses, leading to vascular stenosis or occlusion, and increasing the risk of thrombosis, ultimately resulting in ischemia and damage to brain tissue11,12,13,14. However, research on the disease burden of ischemic stroke attributed to high LDL-C (IS-hLDL-C) in the Chinese population remains lacking.
Global burden of disease (GBD) study 2021 provides comprehensive estimates of IS disease burden from 1990 to 2021 and provides a framework for assessing risk factors15. Although previous studies have investigated the disease burden of ischemic stroke in China, most have relied on GBD 2019 data and exhibited methodological limitations in analytical approaches. In this study, we utilized data from the GBD 2021 Results Tool to calculate the average annual percentage change (AAPC), thereby delineating temporal trends in the burden of IS-hLDL-C in China from 1990 to 2021. Our analyses further incorporated stratified evaluations by gender and age groups. These methodological advancements not only provide a more precise assessment of the current burden but also uncover emerging epidemiological patterns and potential targets for public health interventions, addressing critical gaps in prior research.
Methods
Data resource
The global burden of disease (GBD) study is a comprehensive global initiative led by the Institute for health metrics and evaluation (IHME) at the University of Washington. Its primary objective is to quantify health losses across various regions and over time, with the aim of enhancing health systems and addressing health disparities1,15. The GBD 2021 report encompasses aggregated estimates of exposure levels, relative health risks, and attributable disease burdens for 88 risk factors across 204 countries and territories worldwide16,17). We obtained data on ischemic stroke DALYs number, deaths number and age-standardized rates (ASRs) attributable to hLDL-C in China from 1990 to 2021 using the GBD 2021 results tool (https://ghdx.healthdata.org/)18. The University of Washington Institutional Review Board waived the informed consent requirement for the acquisition of GBD data. The study adhered to the Guidelines for Accurate and Transparent Health Evaluation Reporting (GATHER)19.
Definitions
According to the diagnostic standards established by the World Health Organization, IS is defined as a condition in which the arteries supplying blood to the brain are constricted or blocked, resulting in the infarction of local brain tissue, spinal cord, or retina, and consequently causing neurological dysfunction20,21. This vasculopathy is typically attributed to atherosclerosis, thrombosis, or other vascular diseases, and in severe cases, it can lead to permanent brain damage. In the GBD 2021, the diagnostic codes for IS are categorized as G45–G46.8, I63–I63.9, I65–I66.9, I67.2–I67.848, and I69.3–I69.421.
Statistical analysis
In this study, we employed Joinpoint regression analysis to investigate the temporal trend changes of IS-hLDL-C in China and to calculate the average annual percentage change (AAPC) along with its 95% uncertainty interval (UI). Joinpoint regression analysis is a statistical technique designed to identify points of trend change in time series data22,23. Its fundamental principle is based on piecewise linear regression, which posits that the trend (slope) of the data varies before and after specific time points22,23. The objective of Joinpoint analysis is to pinpoint the exact moments when these slopes shift, referred to as the “ joinpoints ”. The determination of “ joinpoints ” requires data preparation and configuration, including specifying the dependent variable, independent variable, and grouping methods. Subsequently, by defining the minimum and maximum number of “ joinpoints ” and employing the Grid Search Method, all possible Joinpoint locations are evaluated. Furthermore, the significance of the Joinpoints is assessed using methods such as the Bayesian Information Criterion (BIC), thereby determining the statistical significance of trend changes22,23,24. Prior to conducting the Joinpoint regression analysis, we meticulously cleaned and preprocessed the data to ensure its integrity and accuracy. Subsequently, we utilized Joinpoint software to fit the data, enabling the identification of trend change points and the calculation of the statistical significance of each change point. We set a significance level of 0.05 to ascertain the presence of joinpoints. Through this analysis, we were able to determine whether IS-hLDL-C mortality trends in China were increasing, decreasing, or stable, as well as to identify the specific time points at which these trends shifted. The results of this analysis will provide crucial insights for evaluating the effectiveness of public health strategies in managing IS-hLDL-C over recent decades and will offer a scientific foundation for future prevention and treatment strategies. Joinpoint analysis is also instrumental in elucidating the magnitude of trend changes across different time periods, which is crucial for comprehending the dynamic effects of IS-hLDL-C on the health of the Chinese population. A positive AAPC value signifies an upward trend, while a negative value denotes a downward trend; a value of zero indicates no significant change25. The 95% confidence interval (CI) provides a range within which the true AAPC value is expected to fall with 95% probability. This interval accounts for sampling variability and uncertainty inherent in model estimates. When P < 0.05, the AAPC is deemed statistically significant, suggesting that the observed changes are unlikely to have occurred by chance25.
The age-period-cohort (APC) model is primarily utilized to elucidate the three principal effects that influence temporal trends in diseases: age effects, period effects, and cohort effects25,26. A significant challenge associated with the APC model is the complete collinearity among age, period, and cohort variables. To address the collinearity issue among age, period, and cohort variables in the APC model, we employed the intrinsic estimator (IE) method, which is a widely used approach to disentangle the independent effects of age, period, and cohort. The IE method imposes a unique constraint that minimizes the influence of arbitrary constraints on the estimation of age, period, and cohort effects24,27. This method was chosen because it provides a robust and unbiased estimation of the effects, particularly in the context of disease burden studies where the temporal trends are of primary interest. Researchers have devised a range of methods to address this parameter identification issue, including both theory-driven and method-driven parameter identification strategies28,29. These approaches aim to estimate model parameters through diverse statistical techniques and theoretical frameworks, thereby enhancing our understanding and prediction of social changes and health trends. All analyses were performed using R, version 4.4.1 and Joinpoint software.
Result
Burden of ischemic stroke attributable to high low-density lipoprotein cholesterol in China
Table 1 presents the disease burden of IS-hLDL-C in China for 1990 and 2021. Specifically, the number of deaths related to IS-hLDL-C in 2021 was 300,052 (95% UI 92,515–527,456), representing a remarkable increase of 161.8% compared to 1990 (Fig. 1A). The age-standardized mortaliry rates (ASMRs) experienced a slight decrease, from 18.23 per 100,000 people (95% UI 5.52–33.43) in 1990 to 15.93 per 100,000 people (95% UI 4.83–28.08) in 2021 (Fig. 1C). In 2021, the total number of DALYs was 6,850,565 (95% UI 2,313,203 − 11,418,167), with an age-standardized DALYs rates (ASDRs) of 335.59 cases per 100,000 individuals (95% UI 112.75–566.25) (Fig. 1B, D).

Burden of IS-hLDL-C in China from 1990 to 2021. (A) Deaths cases; (B) DALYs cases; (C) Age-standardized mortaliry rates (ASMRs); (D) Age-standardized DALYs rates (ASDRs).
From 1990 to 2021, although the number of deaths and DALYs of IS-hLDL-C showed an upward trend, its age-standardized rate gradually decreased (Fig. 1, Table S1, Table 2). Both ASMRs and ASDRs of IS-hLDL-C decreased during the study period, with annual average percent change (AAPC) of −0.47 (95% CI −0.83 to −0.10) and −0.49 (95% CI −0.83 to −0.10), respectively. Further analysis showed that between 1990 and 1999, the ASMRs remained stable (AAPC: 0.05; 95% CI −0.11 to 0.22) (Fig. 2). However, from 2000 to 2009, there was a downward trend (AAPC: −0.73; 95% CI −1.92 to 0.46). Entering 2010 to 2021, the downward trend is more significant (AAPC: −1.49; 95% CI −1.71 to −1.26). Across the entire 1990 to 2021, the AAPC p-values from 2010 to 2021 are statistically significantly different. Through Joinpoint regression analysis, significant change points in ASMRs in 1998, 2004, 2007 and 2010 were determined (Fig. 2). Likewise, ASDRs also showed a similar downward trend with significant changes observed in the same years. These findings suggest that China has made progress over time in reducing the disease burden of IS-hLDL-C.

Joinpoint regression analysis for ASMRs and ASDRs from 1990 to 2021. ASMRs age-standardized mortaliry rates, ASDRs age-standardized DALYs rates.
Temporal trend in the burden of ischemic stroke attributable to high low-density lipoprotein cholesterol by sex in China
As illustrated in Table 1; Fig. 3A, from 1990 to 2021, the number of deaths due to IS-hLDL-C in male consistently exceeded that in female. In 2021, the number of IS-hLDL-C deaths among male was 170,524 (95% UI 55,095–298,988), whereas the number of female was 129,528 (95% UI 39,343−233,383). Throughout this period, DALYs cases continued to rise for both genders. In 2021, the male DALYs totaled 3,947,467 (95% UI 1,379,348–6,623,022), while female DALYs amounted to 2,903,098 (95% UI 984,544–4,925,899). Additionally, in 2021, the ASMRs for male was 20.96 cases per 10,000 people (95% UI 6.72–37.13), compared to 12.36 cases per 10,000 people for female (95% UI 3.73–22.43) (Fig. 3B). Regarding DALYs, the age-standardized rates (ASRs) in 2021 was 416.3 cases per 100,000 for male (95% UI 143.15–703.34) and 268.95 cases for female (95% UI 91.45–455.85).

Burden of IS-hLDL-C by sex pattern in China from 1990 to 2021. (A) Deaths cases; (B) DALYs cases.
The ASMRs of IS-hLDL-C exhibited a declining trend in both males and females from 1990 to 2021. The AAPC for males was −0.05 (95% CI −0.37 to 0.26), while the AAPC for females was −0.84 (95% CI −1.19 to −0.48). Specifically, during the period from 1990 to 1999, ASMRs for male demonstrated an increasing trend, with an AAPC of 0.30 (95% CI 0.19 to 0.41; p < 0.001), whereas ASMRs for female indicated a decreasing trend with an AAPC of −0.17 (95% CI −0.43 to 0.08). During the 2000 to 2009 period, the increasing trend was more pronounced among males, with an AAPC of 0.14 (95% CI −1.13 to 1.44; p < 0.001), while the decreasing trend was also more pronounced for females, with an AAPC of -1.48 (95% CI −2.68 to −0.28). From 2010 to 2021, a significant decline in ASMRs was observed for males, with an AAPC of -1.43 (95% CI −1.56 to −1.30; p < 0.001), and a similar significant decline was noted for females, with an AAPC of −1.63 (95% CI −2.08 to −1.18; p < 0.001). Joinpoint regression analysis revealed significant change points in ASMRs for males in 1999, 2004, 2007, and 2010, while significant change points for females occurred in 1997, 2004, 2007, and 2015. In terms of ASDRs, males showed a decreasing trend with an AAPC of -0.15 (95% CI −0.38 to 0.08), whereas females demonstrated a statistically significant decreasing trend with an AAPC of −0.81 (95% CI −1.03 to −0.60; p < 0.001).
The burden of ischemic stroke attributable to high low-density lipoprotein cholesterol across different age groups in China
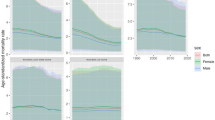
Figure 4 illustrates the burden of deaths and DALYs attributable to IS-hLDL-C across different age groups in China in 1990 and 2021. The data indicate a notable upward trend in disease burden with advancing age, particularly among individuals aged 70 and older. Compared to 1990, there were substantial increases in both ASMRs and ASDRs across all age groups by 2021. However, this upward trend is not mirrored in the ASMRs and ASDRs. Specifically, the IS-hLDL-C mortality rate for each age group under 80 years in 2021 has decreased relative to 1990, while the mortality rate for the elderly group aged 80 and above has risen. Similarly, the ASDRs of IS-hLDL-C for the under-80 age group were lower in 2021 compared to 1990, while the rates for those over 80 surpassed the levels observed in 1990. Figure 5 further depicts the contribution of total deaths and DALYs caused by IS-hLDL-C within each age groups in China from 1990 to 2021. Both the number of deaths and DALYs associated with IS-hLDL-C increased with advancing age. Notably, there were few significant fluctuations in the disease burden of IS-hLDL-C among individuals under 64 years from 1990 to 2021. In contrast, the elderly population aged 65 years and above constitutes the majority of deaths and DALYs caused by IS-hLDL-C, underscoring the critical role of the elderly demographic in the overall disease burden associated with IS-hLDL-C.

Burden of IS-hLDL-C in China by age group in 1990 and 2021. (A) Deaths cases; (B) Age-standardized mortality rates; (C) DALYs cases; (D) Age-standardized DALYs rates.

The contribution of each age group to total deaths and DALYs of IS-hLDL-C between 1990 and 2021 in China.
Age, period and cohort effects on deaths
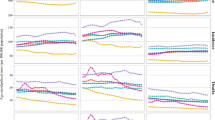
The longitudinal age curves of mortality attributable to IS-hLDL-C in China are depicted in (Fig. 6). All mortality rates associated with IS-hLDL-C exhibited a significant increase with age, and the rate of increase accelerated as age advanced. Notably, we observed that the substantial rise in IS-hLDL-C mortality commenced in the 65–69 age group. The cohort relative risk (RR) indicates a gradual decline in mortality for individuals born after 1952 (RR < 1). Between 1990 and 2021, the Period RR for IS-hLDL-C demonstrated a decreasing trend, with an RR of 1 recorded in 2005. Figure 6 presents the analysis results of local drifts and net drift, where the horizontal solid line represents the net drift, and the curved solid line represents the local drift. The net drift value reflects the estimated annual percentage change in the ASMRs of IS-hLDL-C, adjusted based on the APC model. The local drift values characterize the annual percentage change trends across different age groups. In this study, the net drift value is below 0, indicating an overall declining trend in the ASMRs of IS-hLDL-C. Furthermore, the results reveal that the local drift curve of IS-hLDL-C exhibits a U-shaped distribution and intersects with the net drift line at two points, suggesting an increasing mortality proportion in both younger age groups (30 to 40 years) and older age groups (60 to 70 years).

Age, period and cohort effects on mortality rates of IS-hLDL-C in China during 1990–2021.
Discussion
This study comprehensively analyzes the long-term disease burden of IS-hLDL-C in China from 1990 to 2021. Our findings indicate that the number of deaths and DALYs attributable to IS-hLDL-C has increased over the past 32 years; however, ASMRs and ASDRs have shown a gradual decline. Notably, male exhibit higher ASMRs and ASDRs for IS-hLDL-C compared to female. The decline in disease burden was most pronounced among female, while it remained stable for male. It is important to highlight that the disease burden rises sharply with advancing age, particularly after 70 years. In light of the increasingly complex landscape of chronic disease management, effective IS prevention and control of LDL-C are imperative. To mitigate the burden of stroke, it is essential to develop more comprehensive policies for IS prevention, which should include promoting low-fat diets and healthy lifestyles, enhancing healthcare services for demographics, and increasing awareness, treatment, and management of hyperlipidemia among Chinese adults.
Elevated levels of LDL-C are widely recognized as a risk factor for atherosclerosis, a key pathological process leading to ischemic stroke30. After LDL-C enters the arterial intima, it is oxidized and modified to form oxidized low-density lipoprotein (Ox-LDL), which activates endothelial cells and monocytes and promotes the occurrence of inflammatory reactions31. A Mendelian randomization study indicated that among patients with atherosclerosis-related stroke, a one standard deviation increase in LDL-C significantly heightened the risk of stroke by 28%32. A study found a U-shaped association between LDL-C levels and all-cause mortality during the acute phase of IS, with the lowest risk of death corresponding to an LDL-C level of 2.67 mmol/L. This U-shaped relationship was consistent across subgroups and was particularly significant in patients aged ≥ 65 years and in female33. Notably, maintaining appropriate LDL-C levels appears essential for mitigating stroke severity34. In China, atherosclerosis is the primary cause of ischemic stroke, accounting for over 45% of all ischemic stroke cases35. Our study demonstrates that while the number of deaths attributable to IS-hLDL-C showed a marked cases increase from 1990 to 2021, the ASMRs exhibited a declining trend. This trend in ASMRs may be attributed to China’s rapid demographic aging over recent decades and the remarkable advancements in medical technology, which have collectively contributed to lowering ASMRs2,17. As a result of health education on IS, there has been a significant increase in public awareness of IS. This increased awareness promotes positive lifestyle changes that help prevent and control further disease progression, which in turn effectively reduces the morbidity and mortality of IS36,37). Meanwhile, the widespread use of lipid-lowering drugs such as statins has played an important role in controlling the level of LDL-C, which has significantly reduced the occurrence and progression of atherosclerosis38. In addition, the rational use of antiplatelet and anticoagulant drugs has also played a positive role in reducing the risk of stroke, which may be one of the key factors contributing to the decline in ASMRs36.
Gender-stratified analyses revealed that from 1990 to 2021, the ASMRs and ASDRs associated with IS-hLDL-C were consistently higher in males than in females. This disparity can be attributed to various factors, including lifestyle, physiological differences, and disparities in health awareness. Among premenopausal women, relatively higher levels of estrogen secretion may inhibit the progression of atherosclerosis and exert protective effects on vascular endothelium39,40). Research indicates that estrogen plays a role in regulating the release of nitric oxide (NO), promoting vasodilation and enhancing blood flow, thereby providing protective effects on brain tissue39. A study involving 134 postmenopausal women demonstrated that estrogen treatment significantly enhances the ability of blood vessels to dilate, thereby improving vascular function and promoting cerebral blood flow41. Additionally, women generally exhibit higher health awareness, whereas men are more likely to engage in unhealthy lifestyle habits, such as smoking and excessive alcohol consumption. Nicotine from tobacco is known to induce vascular endothelial dysfunction, heighten inflammatory responses within the blood vessel walls, and facilitate the progression of atherosclerosis42,43). Therefore, it is imperative for male to focus on improving their health behaviors to mitigate the risk of IS-hLDL-C. Recognizing the sex-specific of stroke risk factors is essential for the development of more effective and targeted prevention strategies.
Age-specific analyses revealed a rapid increase in ASMRs and ASDRs with advancing age. The number of IS-hLDL-C deaths and DALYs further escalated with the growing aging population. This observation aligns with the global trend of an increasing disease burden among the elderly as the population ages21. Contributing factors may include physiological changes, diminished vascular elasticity, the accumulation of chronic diseases, and lifestyle prevalent in older adults38. Our study revealed minimal significant fluctuations in the number of IS-hLDL-C related deaths from 1990 to 2021 among individuals younger than 64 years, suggesting success in preventive efforts and early interventions within this age group. The elderly population, specifically those aged 65 years and older, represents the majority of deaths and DALYs attributable to IS-hLDL-C, underscoring the critical role of this age group in the overall disease burden. Recommended strategies may include enhancing health management for older adults, increasing awareness regarding stroke prevention and early recognition, and improving healthcare services tailored for the elderly.
The local drift curve results indicate that the percentage change in ASMRs exhibits a ‘U-shaped’ trend. The cohort effect primarily reflects the interplay between an individual’s early experiences and their social environment, with different birth cohorts often facing varying exposures to risk factors. In China the risk of IS-hLDL-C initially increases and subsequently decreases across successive birth cohorts, particularly after 1952. This phenomenon is largely attributed to the unstable social environment, such as war and famine, as well as poor living conditions, which may lead to a higher risk of IS-hLDL-C in early birth cohorts44. The period effect primarily reflects the impact of external factors such as advancements in diagnostic and treatment technologies, as well as lifestyle changes, on the disease. The findings of this study reveal that the risk of IS-hLDL-C declined to varying degrees from 1990 to 2021. On the one hand, over time, the expansion of healthcare insurance coverage played a role. On the other hand, advances in medical technologies, including the use of statins and improved public awareness of stroke, may have positively influenced the reduction in the risk of IS-hLDL-C45.
This study is based on the Global Burden of Disease Study 2021, an international, large-scale epidemiological research project. GBD 2021 provides detailed and standardized disease burden data that encompasses multiple countries and regions, thereby ensuring the representativeness and reliability of the research findings. However, this study has several limitations. Although the data quality of GBD 2021 is high and representative, there may still be certain biases and omissions during the data collection process. China has a vast territory, and there are significant differences in health care accessibility and medical infrastructure in different regions. For example, economically developed regions may have more comprehensive medical resources and higher IS-hLDL-C screening rates, while economically developed regions may have insufficient diagnosis or missing data. Additionally, fluctuations in the disease burden of IS-hLDL-C may be influenced by various external factors, including socioeconomic conditions, advancements in medical technology, and changes in health policies. These factors may introduce data biases to some extent, complicating the analysis of temporal trends. For the management of IS-hLDL-C, primary prevention should emphasize lifestyle modifications including a healthy diet, increased physical activity, smoking cessation, and alcohol restriction to reduce LDL-C levels. In high-risk populations, statin therapy may be initiated and combined with other lipid-lowering agents based on individual risk profiles. Secondary prevention in stroke survivors requires intensive lipid-lowering strategies targeting LDL-C < 1.4 mmol/L, utilizing high-intensity statins combined with PCSK9 inhibitors to mitigate recurrence risk46. This stratified approach balances overtreatment in low-risk populations with precision interventions for high-risk patients, thereby facilitating the translation of evidence-based medicine into clinical practice.
Conclusion
In conclusion, while ASMRs and ASDRs associated with IS-hLDL-C have decreased in China from 1990 to 2021, the absolute number of deaths and DALYs remains significant. The burden of IS-hLDL-C is greater in males than females, and the ASMRs increases with age among the senior population. Given the large population base and the ongoing trend of an aging population, it is essential to consider various lipid-lowering strategies and the rational allocation of healthcare resources in the future to effectively reduce the disease burden of IS.
Data availability
All data used from GHDx platform (https://vizhub.healthdata.org/gbd-results/).
References
Global Burden. Of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the global burden of disease study 2019. Lancet 396, 1204–1222. https://doi.org/10.1016/s0140-6736(20)30925-9 (2020).
Wu, S. et al. Stroke in china: advances and challenges in epidemiology, prevention, and management. Lancet Neurol. 18 (4), 394–405. https://doi.org/10.1016/s1474-4422(18)30500-3 (2019).
Ma, Q. et al. Temporal trend and attributable risk factors of stroke burden in china, 1990–2019: an analysis for the global burden of disease study 2019. Lancet Public. Health. 6 (12), e897–e906. https://doi.org/10.1016/s2468-2667(21)00228-0 (2021).
Zhang, R. et al. Global burden of ischemic stroke in young adults in 204 countries and territories. Neurology 100 (4), e422–e34 https://doi.org/10.1212/wnl.0000000000201467 (2023).
Tang, L., Xie, L. & Liu, Y. Temporal trends of ischemic stroke attributable to high fasting plasma glucose in China from the global burden of disease study 2019. Front. Endocrinol. (Lausanne) 15 https://doi.org/10.3389/fendo.2024.1408691 (2024).
Harshfield, E. L., Georgakis, M. K., Malik, R. & Dichgans, M. and H. S. Markus. Modifiable lifestyle factors and risk of stroke: A mendelian randomization analysis. Stroke 52, (3), 931 – 936 https://doi.org/10.1161/strokeaha.120.031710 (2021).
Du, S. F., Wang, H. J., Zhang, B. & Zhai, F. Y. and B. M. Popkin. China in the period of transition from scarcity and extensive undernutrition to emerging nutrition-related non-communicable diseases. Obes Rev. 15 (1), 8–15 https://doi.org/10.1111/obr.12122 (2014).
Popkin, B. M. Synthesis and Implications: China’s nutrition Transition in the context of changes across other low- and middle-income countries. Obes Rev. 15 (1), 60 – 76 https://doi.org/10.1111/obr.12120 (2014).
Zhang, J. et al. Global, regional and national burden of ischemic stroke attributed to high low-density lipoprotein cholesterol, 1990–2019: a decomposition analysis and age-period-cohort analysis. J Cereb Blood Flow Metab. 44 (4), 527 – 41 https://doi.org/10.1177/0271678x231211448 (2024).
Lau, K. K. et al. Low-Density lipoprotein cholesterol and risk of recurrent vascular events in Chinese patients with ischemic stroke with and without significant atherosclerosis. J. Am. Heart Assoc. 10, 16. https://doi.org/10.1161/jaha.121.021855 (2021).
Borén, J. et al. Low-Density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: A consensus statement from the European atherosclerosis society consensus panel. Eur. Heart J. 41 (24), 2313–2330. https://doi.org/10.1093/eurheartj/ehz962 (2020).
Ruuth, M. et al. Susceptibility of Low-Density lipoprotein particles to aggregate depends on particle lipidome, is modifiable, and associates with future cardiovascular deaths. Eur. Heart J. 39, 27. https://doi.org/10.1093/eurheartj/ehy319 (2018).
Michos, E. D., McEvoy, J. W. & Blumenthal, R. S. Lipid management for the prevention of atherosclerotic cardiovascular disease. N Engl. J. Med. 381 (16), 1557–1567. https://doi.org/10.1056/NEJMra1806939 (2019).
Chen, Z. et al. Effects of individual and integrated cumulative burden of blood pressure, glucose, low-density lipoprotein cholesterol, and C-reactive protein on cardiovascular risk. Eur. J. Prev. Cardiol. 29 (1), 127–135. https://doi.org/10.1093/eurjpc/zwaa052 (2022).
Global burden and strength of evidence for 88 risk factors in 204countries and 811 subnational locations, 1990–2021: A systematic analysis for the global burden of disease study 2021. Lancet 403 (10440), 2162–2203 https://doi.org/10.1016/s0140-6736(24)00933-4 (2024).
Fan, J. et al. Global burden, risk factor analysis, and prediction study of ischemic stroke, 1990–2030. Neurology 101 (2), e137–e50. https://doi.org/10.1212/wnl.0000000000207387 (2023).
Li, X. Y. et al. Global, regional, and national burden of ischemic stroke, 1990–2021: An analysis of data from the global burden of disease study 2021. EClinicalMedicine 75, 102758 https://doi.org/10.1016/j.eclinm.2024.102758 (2024).
Fertility, G. A. S. S. Mortality, healthy life expectancy (Hale), and population estimates in 204 countries and territories, 1950–2019: A comprehensive demographic analysis for the global burden of disease study 2019. Lancet 396 (10258), 1160 – 203 https://doi.org/10.1016/s0140-6736(20)30977-6 (2020).
Stevens, G. A. et al. Guidelines for accurate and transparent health estimates reporting: the gather statement. Lancet 388, 10062. https://doi.org/10.1016/s0140-6736(16)30388-9 (2016).
Global, R., National Burden of Stroke and Its, Risk & Factors 1990–2019: A systematic analysis for the global burden of disease study 2019. Lancet Neurol. 20 (10), 795–820. https://doi.org/10.1016/s1474-4422(21)00252-0 (2021).
Deng, Z., Li, H. & Wang, J. Temporal trends of the burden of ischemic stroke attributable to high Low-Density lipoprotein cholesterol in China from 1999 to 2019. BMC Public. Health. 24 (1), 3003. https://doi.org/10.1186/s12889-024-20461-5 (2024).
Liu, F. et al. and J. Yu. Age-period-cohort analysis of long-term trends in ischemic stroke mortality in China caused by specific risk factors from 1990 to 2019. Neuroepidemiology 58 (3), 182 – 98 https://doi.org/10.1159/000536014 (2024).
Gao, Y., Liu, K. & Fang, S. Changing patterns of stroke and subtypes attributable to high systolic blood pressure in China from 1990 to 2019. Stroke 55 (1), 59–68 https://doi.org/10.1161/strokeaha.123.044505 (2024).
Guo, M., Xu, J. & Du, J. Trends in cervical cancer mortality in China from 1989 to 2018: an age-period-cohort study and joinpoint analysis. BMC Public. Health. 21 (1), 1329. https://doi.org/10.1186/s12889-021-11401-8 (2021).
Zhang, Y. et al. Long-Term trends in the burden of inflammatory bowel disease in China over three decades: A joinpoint regression and Age-Period-Cohort analysis based on Gbd 2019. Front. Public. Health. 10, 994619. https://doi.org/10.3389/fpubh.2022.994619 (2022).
Gao, Y. & Liu, X. Secular trends in the incidence of and mortality due to alzheimer’s disease and other forms of dementia in China from 1990 to 2019: an Age-Period-Cohort study and joinpoint analysis. Front. Aging Neurosci. 13, 709156. https://doi.org/10.3389/fnagi.2021.709156 (2021).
Woo, P. P., Thach, T. Q., Choy, S. T., McGhee, S. M. & Leung, G. M. Modelling the impact of Population-Based cytologic screening on cervical Cancer incidence and mortality in Hong kong: an Age–Period–Cohort approach. Br. J. Cancer. 93 (9), 1077–1083. https://doi.org/10.1038/sj.bjc.6602805 (2005).
Ocaña-Riola, R., Mayoral-Cortés, J. M. & Sánchez-Cantalejo, C. Analysis of Age-Period-Cohort effects on overall mortality in Andalusia (Southern Spain). Public. Health. 127 (10), 922–929. https://doi.org/10.1016/j.puhe.2013.04.032 (2013).
Hwang, J. H. & Park, S. W. Gender differential secular trend in lifetime smoking prevalence among adolescents: an Age-Period-Cohort analysis. BMC Public. Health. 19 (1), 1374. https://doi.org/10.1186/s12889-019-7735-8 (2019).
Yuan, S., Tang, B., Zheng, J. & Larsson, S. C. Circulating lipoprotein lipids, apolipoproteins and ischemic stroke. Ann. Neurol. 88 (6), 1229–1236. https://doi.org/10.1002/ana.25916 (2020).
Jiang, H. et al. Mechanisms of oxidized Ldl-Mediated endothelial dysfunction and its consequences for the development of atherosclerosis. Front. Cardiovasc. Med. 9, 925923. https://doi.org/10.3389/fcvm.2022.925923 (2022).
Hindy, G. et al. Role of blood lipids in the development of ischemic stroke and its subtypes: A Mendelian randomization study. Stroke 49 (4), 820–827 https://doi.org/10.1161/strokeaha.117.019653 (2018).
Chen, Z. M. et al. U-shaped association between low-density lipoprotein cholesterol levels and risk of all-cause mortality mediated by post-stroke infection in acute ischemic stroke. Sci. Bull. (Beijing). 68 (12), 1327–1335. https://doi.org/10.1016/j.scib.2023.05.028 (2023).
Chen, Z. M. et al. Beyond low-density lipoprotein cholesterol levels: impact of prior Statin treatment on ischemic stroke outcomes. Innov. (Camb). 5 (6), 100713. https://doi.org/10.1016/j.xinn.2024.100713 (2024).
Wang, Y. et al. Stroke care quality in China: Substantial improvement, and a huge challenge and opportunity. Int. J. Stroke 12 (3), 229 – 35 https://doi.org/10.1177/1747493017694392 (2017).
Li, Z., Jiang, Y., Li, H., Xian, Y. & Wang, Y. China’s response rising stroke burd. Bmj 364, l879 https://doi.org/10.1136/bmj.l879 (2019).
Ge, R. et al. Global, regional, and national temporal trends of diet-related ischemic stroke mortality and disability from 1990 to 2019. Int. J. Stroke 19 (6), 665 – 75 https://doi.org/10.1177/17474930241237932 (2024).
Ovbiagele, B. & Nguyen-Huynh, M. N. Stroke epidemiology: Advancing our understanding of disease mechanism and therapy. Neurotherapeutics 8 (3), 319 – 29 https://doi.org/10.1007/s13311-011-0053-1 (2011).
Miller, V. M. & Mulvagh, S. L. Sex steroids and endothelial function: Translating basic science to clinical practice. Trends Pharmacol. Sci. 28 (6), 263 – 70 https://doi.org/10.1016/j.tips.2007.04.004 (2007).
Bots, S. H., Peters, S. A. E. & Woodward, M. Sex differences in coronary heart disease and stroke mortality: A global assessment of the effect of ageing between 1980 and 2010. BMJ Glob Health. 2 (2), e000298. https://doi.org/10.1136/bmjgh-2017-000298 (2017).
Vitale, C. et al. Time since menopause influences the acute and chronic effect of estrogens on endothelial function. Arterioscler. Thromb. Vasc Biol. 28 (2), 348–352. https://doi.org/10.1161/atvbaha.107.158634 (2008).
Kelly, T. N. et al. Cigarette Smok. Risk Stroke Chin. Adult Popul. Stroke 39 (6), 1688–1693 https://doi.org/10.1161/strokeaha.107.505305 (2008).
Lv, J. et al. Adherence to healthy lifestyle and cardiovascular diseases in the Chinese population. J. Am. Coll. Cardiol. 69 (9), 1116–1125. https://doi.org/10.1016/j.jacc.2016.11.076 (2017).
Osmond, C., Kajantie, E., Forsén, T. J., Eriksson, J. G. & Barker, D. J. Infant growth and stroke in adult life: The Helsinki birth cohort study. Stroke 38 (2), 264 – 70 https://doi.org/10.1161/01.Str.0000254471.72186.03 (2007).
Wang, W. et al. Prevalence, incidence, and mortality of stroke in China: Results from a nationwide population-based survey of 480 687 adults. Circulation 135 (8), 759 – 71 https://doi.org/10.1161/circulationaha.116.025250 (2017).
Chinese guidelines on prevention and treatment of dyslipidemia in adults. Zhonghua Xin Xue Guan Bing Za Zhi 35 (5), 390–419 (2007).
Acknowledgements
We extend our gratitude to the contributors of the Global Burden of Diseases, Injuries, and Risk Factors Study 2021 for their invaluable work. We also express our sincere appreciation to the Institute for Health Metrics and Evaluation (IHME) for making the GBD data available for this research. The study funders did not participate in the design of the study, data collection, analysis, interpretation, or report writing.
Funding
The author(s) declare that financial support was received for the research, authorship, and publication of this article. YK.L were funded by the “Joint Fund for Science and Technology Innovation of Fujian (No. 2023Y9288).”
Author information
Authors and Affiliations
Contributions
Hua Xue: Drafting/revision of the manuscript for content, including medical writing for content; Major role in the acquisition of data; Analysis or interpretation of data Yuqi Zeng: Drafting/revision of the manuscript for content, including medical writing for content Xinyang Zou: Drafting/revision of the manuscript for content, including medical writing for content Yanhong Jiang: Drafting/revision of the manuscript for content, including medical writing for content.Wenhui Fan: Drafting/revision of the manuscript for content, including medical writing for content Yongkun Li: Drafting/revision of the manuscript for content, including medical writing for content; Major role in the acquisition of data; Analysis or interpretation of data.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xue, H., Zeng, Y., Zou, X. et al. Burden of ischemic stroke attributable to high low-density lipoprotein cholesterol in China from the global burden of disease study 2021. Sci Rep 15, 20037 (2025). https://doi.org/10.1038/s41598-025-04677-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-04677-y
