
Abstract
The presence of a known labor companion was shown to improve childbirth satisfaction. However, a companion’s anxiety might affect the satisfaction of laboring women. Therefore, this study aimed to evaluate the relationship between the anxiety of labor companions and childbirth satisfaction among laboring women. This cross-sectional study was conducted on primiparous women who gave birth with a relative as a labor companion in a hospital in Sabzevar, Iran, between December 2020 and November 2021. The demographic checklist and Mackey Childbirth Satisfaction Rating Scale were filled out for laboring women, and the Spielberg Trait Anxiety (STAI) was filled out for companions. One-hundred fifty-seven laboring women (mean age 25.76 (SD = 4.99) years and their companions (mean age 40.54 (SD = 10.67 years) were analyzed. Moderate and severe anxiety were found in 98 (62.4%) and 21 (13.4%) participants, respectively. Favorable childbirth satisfaction was reported by 64 (40.7%) laboring women. No significant relationship was observed between the companion’s anxiety score and laboring women’s childbirth satisfaction (r=-0.117, p = 0.145), even after adjusting for confounders (partial r=-0.092, p = 0.276). The findings of this study revealed no significant relationship between companion anxiety and childbirth satisfaction in laboring women in hospital settings.
Similar content being viewed by others
Introduction
Childbirth is a wonderful and special experience for women. It can also be potentially traumatic, as it is one of the most painful events that a woman endures1. Across time and cultures, support of childbearing women has been an old concept in which a family member, friend, relative, community member, community health worker, doula, or healthcare professional accompanies the woman during childbirth2.
The World Health Organization (WHO) advises childbirth support by a companion to enhance prenatal outcomes and childbirth satisfaction3. Supporting childbirth by a labor companion, who can be any person chosen by a woman from the pregnant woman’s social network, is effective as the companion can provide continuous support regarding advice, information, and comfort during labor and childbirth4,5.
Labor companions can provide emotional and psychological support, reduce pain and anxiety, and improve childbirth outcomes6. Previous evidence showed that labor support can benefit childbirth in terms of reducing the length of labor, increasing the vaginal delivery rate, reducing labor pain and anxiety, as well as increasing labor satisfaction7,8.
In Iran, following the implementation of the Iranian Health System Transformation Plan to promote normal vaginal childbirth, maternity services were allowed to employ labor companions during labor9. This reform resulted in a reduction in the rate of cesarean section and promoted positive childbirth experiences10. Accordingly, a study that compared the rate of vaginal delivery before and after the Iranian Health System Transformation Plan reported the ratio of vaginal deliveries to all deliveries in 2013 and 2014 was 57.4% and 61.4%, respectively11.
However, the clinical experiences of the authors show some labor companions may fail to provide support to laboring women due to a lack of readiness for labor support or their stress and anxiety. Also, the conditions of labor companions have been noticed in recent studies. A qualitative study indicated that companions are emotionally involved in birth12. In a previous survey of 50 Indian birth companions, the level of anxiety was moderate among the majority of the companions (88%), and the level of maternal satisfaction was moderate in the majority of the mothers. The authors hypothesized that companion anxiety could be reduced by providing education before participation in the birth process13. A study showed that applying an empowerment educational program promoted childbirth satisfaction, reduced labor duration, and cesarean section compared to those with no education program14. Midwives could be good sources of information for companions. In a stepped wedge cluster randomized trial on 475 participants, midwife-provided empowerment resulted in improved maternal coping and satisfaction; however, the study did not evaluate the level of anxiety among the companions15. A meta-analysis published in 2024 reported a lack of comprehensive analysis of the optimal characteristics of labor companions in the existing literature16. This systematic review noted the emotional condition of the labor companion and reported that training labor companions should include a psychological component and highlight empathy as one of the most important characteristics of a labor companion16.
Regarding the important role of labor companions’ emotional condition, this study evaluated the relationship between labor companions’ anxiety and labor satisfaction among laboring women.
Methods
Study design
A cross-sectional design was employed from December 4, 2020 to November 23, 2021. The Vice Chancellor of Research and Technology, Gonabad University of Medical Sciences, approved the study protocol. All methods were performed under the relevant guidelines and regulations. This report was based on the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cross-sectional studies14.
Setting and participants
This study was conducted at Shahid Mobini Hospital in Sabzevar, located in the North-East of Iran. The participants were laboring woman women and their labor companions. The inclusion criteria were being primiparous, having an age range of 18 and 35 years, having singleton-term uncomplicated pregnancy with a head presentation, being planned for vaginal delivery, and being accompanied by a relative during labor. The exclusion criteria were fetal distress, the occurrence of any complications during labor, and the application of cesarean section.
Sample size and sampling
The required sample size was calculated using the following formula for correlation estimation, considering an alpha error rate of 0.05, a test power of 0.80, and a small effect size of 0.217.
The sample size was determined to be 153 individuals, which was increased to 170, with a potential attrition rate of 10%.
The convenience sampling method was used to recruit the participants, considering inclusion and exclusion criteria.
Study instruments
-
a.
Demographic checklist
The demographic checklist included information about the personal characteristics of the laboring woman and her labor companion, including age, level of education, employment status, monthly household income, time of the onset of labor pain, pain relief method during labor, neonatal birth weight, satisfaction level with pregnancy, husband’s support, and marital relationship satisfaction. This checklist was developed using the updated textbook and existing literature. The face and content validity of the demographic checklist was assessed and approved by an expert panel consisting of eight university lecturers and two medical doctors.
-
b.
The Mackey Childbirth Satisfaction Rating Scale
This scale is a 34-item questionnaire that evaluates postpartum women’s satisfaction with childbirth. It comprises six subscales, including self-satisfaction (9 items), partner (2 items), newborn baby (3 items), midwife (9 items), doctors (8 items), and an overall childbirth assessment (3 items). These questions are answered using a 5-point Likert scale from 1 (extremely dissatisfied) to 5 (extremely satisfied). The overall score can range between 34 and 17018. The reliability of the Persian version of the instrument was approved in a previous study Cronbach’s alpha = 0.78 and intraclass correlation coefficient [ICC] = 0.98)19. In the present study, the Cronbach’s alpha was 0.903.
-
c.
Spielberger Trait Anxiety Inventory (STAI)
Spielberger et al. developed the STAI in 1970 to measure trait-state anxiety20. This questionnaire includes separate self-assessment scales to measure both state and trait anxiety. State anxiety has been defined as a “transitory emotional response involving unpleasant feelings of tension and apprehensive thoughts.“19. In the current study, the state scale was used to evaluate the anxiety at present. The state scale consists of 20 items rated using a 4-point Likert scale ranging from 1 (Not at all) to 4 (Very much). Higher scores indicate greater anxiety. The reliability and validity of the Persian version of STAI has been confirmed in the Iranian population(Cronbach’s alpha = 0.79)21. In the present study, the Cronbach’s alpha was 0.936.
Data collection
After receiving comprehensive information, eligible laboring women and their labor companions were invited to participate in the study. The participants signed written informed consent and filled out the demographic questionnaire. Then, the Spielberger State Anxiety Inventory was completed by labor companions. Laboring women completed the Mackey Childbirth Satisfaction Rating Scale 2–4 h after childbirth.
Statistical analysis
The statistical package for social sciences (SPSS) version 16.0 (SPSS, Chicago, IL, USA) and the STATA version 12.0 were used to analyze the data. Mean (standard deviation [SD]) and frequency (percentage) were used to present descriptive statistics for continuous and categorical variables, respectively. The Kolmogorov–Smirnov (K–S) test was employed to assess the normality of the continuous variables. The Pearson correlation coefficient was used to evaluate the relationship between the anxiety score of the labor companion during labor and childbirth satisfaction in primiparous women. Univariate linear regression models were performed to identify confounders, and variables with p < 0.25 were identified as possible confounders. Then, a multiple linear regression model was performed to adjust for the confounders. The effect size was determined using partial r and was interpreted based on Cohen’s cut-offs (small = 0.10, medium = 0.30, large = 0.50)22. Post-hoc power analysis was conducted to evaluate the study’s sensitivity to detect the observed effect size, using the G.Power 3.1.9.4 software with the actual sample size and the observed correlation coefficient. The linear regression assumptions, including normality, homoscedasticity of variance, and error independence, were evaluated using the K–S test on residuals, a scatter plot of the standardized residuals vs. standardized predicted values, and a residual time series plot, respectively. The statistical significance level was set at p < 0.05.
Results
Characteristics of the participants
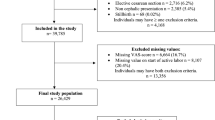
From 234 laboring women and their companions, 157 primiparous women were eligible for the study, and their data were analyzed. The mean age of the laboring women was 25.76 (SD = 4.99) years (ranging from 18 to 35 years). The mean gestational age at the time of labor was 39.31 weeks (SD = 1.0), with a range from 37.0 to 42.0 weeks. The median duration of the first stage of labor was 220.0 min (Interquartile Range [IQR]: 135.0 to 300.0 min), while the median duration of the second stage of labor was 50.0 min (IQR: 25.0 to 90.0 min). As shown in Table 1, most women had university-level education (40.8%), were housewives (81.5%), and reported moderate-to-high knowledge about natural childbirth (89.8%). Notably, 68.2% did not desire the current pregnancy, and 45.2% expressed high or very high fear of natural childbirth. Over half (54.1%) had participated in childbirth preparation classes, and 55.4% strongly believed in their usefulness, while 12.8% found them minimally helpful. 68.2% reported using of reliable information sources about childbirth. 61.8% of the cases utilized analgesic methods during their childbirth. For the majority of laboring women, midwives served as the primary birth assistants (58.6%), followed by obstetricians at 31.2%.
The mean age of the labor companions was 40.54 (SD = 10.67) years (ranging from 24 to 67 years). Table 2 reveals that almost half of the companions (49.7%) had only completed elementary or secondary education, while only 20.4% held a university degree. The majority (69.4%) were housewives. 40.8% were mothers, and 28.7% were sisters of laboring women. A significant of them (71.3%) reported having experience with natural childbirth. Knowledge about natural childbirth was rated as high or very high by 51.6%, but 15.9% had only minimal knowledge. In terms of fear levels regarding natural childbirth, 43.9% reported little to no fear levels, while 31.2% had high or very high fear levels. 74.5% reported using of reliable information sources about childbirth.
The anxiety of labor companions
The mean anxiety score among labor companions during labor was 39.3 (SD = 12.0). Anxiety levels were moderate in 98 participants (62.4%; 95% CI: 54.3–70.0%) and severe in 21 participants (13.4%; 95% CI: 8.4–19.7%). The univariate analyses revealed no significant differences in anxiety levels among labor companions based on factors such as education, occupation, relationship to the laboring woman, pregnancy history, sources of information about childbirth, participation in childbirth classes, knowledge of natural childbirth, and fear of natural childbirth (p > 0.05 for all). However, companions who lacked experience with natural childbirth exhibited a nearly significant trend toward higher anxiety levels (p = 0.052).
Childbirth satisfaction
The mean childbirth satisfaction score in the laboring women was 56.1 (SD = 8.8). The satisfaction level was slight in 93 participants (59.3%; 95% CI: 51.1–67.0%) and favorable in 64 participants (40.7%; 95% CI: 33.0–48.9%) participants. The results of univariate analyses revealed that higher knowledge about natural childbirth was significantly associated with greater childbirth satisfaction (p = 0.032). Additionally, the type of childbirth assistant (midwife, obstetrician, etc.) showed a significant relationship with satisfaction scores (p = 0.029). However, no other variables—including education level, occupation, wanted pregnancy, source types of information about natural childbirth, fear level, participation in childbirth classes, belief in their usefulness, or use of analgesia—demonstrated a statistically significant association (p > 0.05 for all).
Correlation between the anxiety of labor companion and childbirth satisfaction
The unadjusted Pearson correlation coefficient between the anxiety of labor companions and childbirth satisfaction in laboring women was − 0.117 (P = 0.145).
Chat.
Multivariate linear regression was conducted to assess the relationship between the anxiety levels of labor companions and childbirth satisfaction among laboring women. This analysis controlled for confounding variables that had a p-value of less than 0.25 in simple linear regression, including maternal education, partner education, education level of labor companions, fear levels of labor companions, type of childbirth assistant, and the duration of both the first and second stages of labor, as well as the anxiety levels of the labor companions. The total variance of anxiety explained by the independent variables in the model was 8.6% (F (10,145) = 2.46, p = 0.009, adjusted R-squared = 0.086). A negative non-significant relationship was found between the anxiety of labor companions during labor and childbirth satisfaction in laboring women (partial r=-0.092, P = 0.276). Moreover, there was no association between childbirth satisfaction in laboring women and other variables in the regression model (Table 3).
Post-hoc power analysis.
A post-hoc power analysis indicated that the study had only 30.9% power to detect the observed effect size (two-tailed Pearson correlation, α = 0.05, N = 157), which is significantly below the conventional threshold of 80%. This suggests that the study had limited sensitivity to identify relationships of this magnitude.
Discussion
This study was conducted to evaluate the relationship between labor companions’ anxiety levels and childbirth satisfaction in primiparous women. The findings showed no significant relationship between labor companion anxiety and childbirth satisfaction in laboring women, even after adjusting for confounders.
To the best of our knowledge, no study has evaluated the effect of labor companies’ anxiety during labor on childbirth satisfaction. However, a previous study examined the impact of an empowering program for labor companion women on childbirth satisfaction. This program included stages, signs, and symptoms of labor, physical and comfort measures, emotional support, and instrumental support.
The findings showed that empowering labor companions improved childbirth satisfaction14. This study did not directly assess the relationship between labor companions’ anxiety during labor and childbirth satisfaction. Still, maybe labor companion education in the intervention group had positive effects on reducing their anxiety and increased satisfaction with the childbirth experience of laboring women in this group. In other words, Although the interventions used in this study did not include anxiety management for the labor companion, empowerment might have indirectly reduced the stress and anxiety level of the companion.
The reasons for the lack of association between labor companion anxiety level and childbirth satisfaction in this study might be as follows: (1) the level of stress in the majority of the labor companion was low to moderate, which could not be high enough to affect maternal satisfaction, (2) the presence of professional midwives and physicians in the hospital setting could have reassured women and their companions in terms of safe delivery and the emotional support provided by the companion improved childbirth satisfaction23,24, (3) the presence of professional midwives has resulted in the management of labor problems that might have been evolved due to maternal anxiety25, (4) the inclusion of uncomplicated pregnancies in this study was not challenging, and thus the companion anxiety could not affect the labor procedure.
This study indicated that most laboring women were satisfied with childbirth. It was previously shown that a known labor companion could improve childbirth satisfaction in laboring women26,27. In a systematic review and meta-analysis, having a labor companion was associated with a 2.66 times increase in childbirth satisfaction28. In another systematic review, the choice of a female relative labor companion improved childbirth satisfaction29. In line with the mentioned systematic review, a cross-sectional study on 320 postpartum women reported the presence of a labor companion was the only nonpharmacological intervention that improved maternal satisfaction in terms of emotional support30. These findings led to the hypothesis that childbirth satisfaction might be affected if the labor companion has emotional distress. This hypothesis was approved in previous studies on caregivers in emergency and non-emergency department patients. A review of the literature indicated that caregiver stress, anxiety, and depression affect patient outcomes in terms of patient physical and mental health as well as quality of life31. A study on 30 stroke patients and their caregivers reported that the emotional state of caregivers was associated with that of the patients16.
Companion anxiety level showed marginal associations with childbirth satisfaction (p = 0.078). Though these did not reach conventional significance thresholds, they align with existing literature suggesting psychosocial and physiological factors may collectively influence birth experiences8,27,28. These variables may function as moderators in larger samples or interact with unmeasured factors like coping strategies. Future studies with enhanced power should explore these relationships.
Our post-hoc power analysis indicated a limited statistical power of 30.9% to detect the observed small correlation (r = -0.117). Additionally, the regression analysis yielded a modest adjusted R² of 8.6%, suggesting that only a small portion of the variance in childbirth satisfaction was accounted for by the included variables. This limited explanatory power may have been influenced by several factors: the study focused on a homogeneous population of healthy primiparous women, which could have restricted variability in outcomes, and while key demographic and clinical factors were controlled for, other potentially significant variables-such as the quality of interpersonal interactions during labor and specific support behaviors-were not measured. Therefore, these results should be regarded as preliminary and warrant further investigation through studies with larger sample sizes to ensure adequate power.
The strength of this study was evaluating the anxiety level of the labor companion instead of the laboring women to evaluate the effect of mental state in the important emotional support of the laboring women during delivery on their childbirth satisfaction level. However, this study had limitations, including the convenience sampling method, which might have included pregnant women confident in their delivery outcome. Another limitation of the study was the low rate of severe anxiety in labor companions, which might have affected the statistical findings. Therefore, it is recommended that further studies evaluate the anxiety of labor companions on childbirth satisfaction using stratified random sampling to include a comparable number of labor companions with different levels of anxiety. This study only reported the lack of association between the anxiety level of labor companions and childbirth satisfaction in laboring women, and the findings do not rule out the possible effect of companion mental state on the mental state of the laboring women.
Conclusion
The findings of this study showed that in uncomplicated pregnancies, the anxiety level of labor companions was not significantly associated with childbirth satisfaction in laboring women. However, the lack of association may reflect low-severity anxiety in most labor companions (only 13.4% with severe anxiety). A study focusing on high-anxiety companions might yield different results. Training labor companions to manage their anxiety may still be beneficial even though the current study showed no significant association between the anxiety of labor companions and childbirth satisfaction of laboring women.
Data availability
The datasets generated and analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
References
Sun, X. F. X. et al. Psychological birth trauma: A concept analysis. Front Psychol. 13(13), 1065612. https://doi.org/10.3389/fpsyg.2022 (2023).
Organization. WH. Why having a companion during labour and childbirth may be better for you. World Health Organization. 2019:Available at: https://www.who.int/news/item/19-03-2019-why-having-a-companion-during-labour-and-childbirth-may-be-better-for-you. [site accesse: May 2,24].
Li, J. & Jin, Y. Labor companionship in midwifery context: A concept analysis. Nurs. Midwifery Stud. 13(2), 92–99 (2024).
Hunie Asratie, M. M. A. H. & Abuhay, M. Labor companionship in labor and delivery at Debremarkos town public health facilities: magnitude and associated factors. Int. J. Womens Health. 13, 815–827. https://doi.org/10.2147/IJWH.S327753 (2021).
Kabakian-Khasholian T PA. Companion of choice at birth: factors affecting implementation. . BMC Pregnancy Childbirth. 2017;17(1265. 0.1186/s12884-017-1447-9.).
Doba, Y. S. B. G. et al. Birth attendants’ attitudes and practice of companionship during facility-based childbirth and associated factors in the West Shoa Zone, central Ethiopia: A mixed method design. SAGE Open Med. 11, 20503121231168284. (2023).
Hoga, L. A. K., Gouveia, L. M. R., Higashi, A. B. & de Souza, Z.-R. The experience and role of a companion during normal labor and childbirth: a systematic review of qualitative evidence. JBI Evid. Synth. 11(12), 121–156 (2013).
Dahl, C.M.G.-T.J. & Premkumar, A. Birth behind bars: The need for labor support in the incarcerated population. Obstet. Gynecol. 136(5), 1036–1039 (2020).
Lamyian, M.J.-A.K., Alijanpoor, M., Hoorsan, R., Daneshfar, Z. & Rasoulzadeh, M. Health transformation plan in birth departments in Iranian hospitals: A rapid review. J. Iran. Inst. Health Sci. Res. 20(4), 439–449. https://doi.org/10.52547/payesh.20.4.439 (2021).
Toosi, Z. S. E., Zamanian, L. & Fallahinia, G. Implementation of the Health System Reform Plan in Two Contexts of “Promoting Vaginal Delivery and Reducing Out-of-Pocket Payment of Hospitalized Patients” in Hospitals Affiliated to Hamadan University of Medical Sciences. Hakim J. 21(3), 173–179 (2018).
Sarbaz, M., Mousavi Baigi, S. F., Manouchehri Monazah, F., Dayani, N. & Kimiafar, K. The trend of normal vaginal delivery and cesarean sections before and after implementing the health system transformation plan based on ICD-10 in the northeast of Iran: A cross-sectional study. Health Sci. Rep. 6(3), e1131 (2023).
Wanyenze, E. W., Byamugisha, J. K., Tumwesigye, N. M., Muwanguzi, P. A. & Nalwadda, G. K. A qualitative exploratory interview study on birth companion support actions for women during childbirth. BMC Pregnancy Childbirth. 22(1), 63 (2022).
Wanyenze, E. W., Nalwadda, G. K., Byamugisha, J. K., Muwanguzi, P. A. & Tumwesigye, N. M. Effect of midwife-provided orientation of birth companions on maternal anxiety and coping during labor: A Stepped wedge cluster randomized control trial in Eastern Uganda. Int. J. Environ. Res. Public Health 20(2), 1549 (2023).
Jisha, C., Piliai, S. G. & Ashalatha, P. Effect of empowered female labour companion on anxiety, birth outcome, and maternal satisfaction among primiparturients. Manipal J. Nurs. Health Sci. 7(1), 47–53 (2021).
Wanyenze, E. W., Nalwadda, G. K., Byamugisha, J. K., Muwanguzi, P. A. & Tumwesigye, N. M. Effect of midwife-provided orientation of birth companions on maternal anxiety and coping during labor: A stepped wedge cluster randomized control trial in Eastern Uganda. Int. J. Environ. Res. Public Health 20(2), 1549 (2023).
Maggio, M. G. et al. Understanding the family burden and caregiver role in stroke rehabilitation: insights from a retrospective study. Neurol. Sci. 45(11), 5347–5353 (2024).
Martin, E. L. & Martinez, D. A. The effect size in scientific publication. Educación XX1. 26(1), 9–17 (2023).
Lopes, F. J. N., Nakamura, M. U. & Nomura, R. M. Y. Psychometric properties of the Mackey Childbirth Satisfaction Rating Scale cross-culturally adapted to Brazilian Portuguese. J. Matern. Fetal Neonatal. Med. 34(13), 2173–2179. https://doi.org/10.1080/14767058.2019.1660763 (2021).
Moudi, Z. & Tavousi, M. Evaluation of Mackey childbirth satisfaction rating scale in Iran: what are the psychometric properties. Nurs. Midwifery stud. https://doi.org/10.17795/nmsjournal29952 (2016).
Spielberger, C.D.G.-R.F., Martinez-Urrutia, A., Natalicio, L. F. & Natalicio, D. S. The state-trait anxiety inventory. Interam. J. Psychol. 5(34), 145–158 (1971).
Abdoli, N. et al. Reliability and validity of Persian version of state-trait anxiety inventory among high school students. East Asian Arch. Psychiatry 30(2), 44–47 (2020).
Cohen, J. Statistical power analysis for the behavioral sciences (Routledge, 2013).
Capogna, G., Camorcia, M. & Stirparo, S. Expectant fathers’ experience during labor with or without epidural analgesia. Int. J. Obstet. Anesth. 16(2), 110–115 (2007).
Evans, K., Pallotti, P., Spiby, H., Evans, C. & Eldridge, J. J. B. Supporting birth companions for women in labor, the views and experiences of birth companions, women and midwives: A mixed methods systematic review. Birth 50(4), 689–710 (2023).
Liu, Y. et al. Women’s experience and satisfaction with midwife-led maternity care: a cross-sectional survey in China. BMC Pregnancy Childbirth 21, 1–10 (2021).
Younes, R. E., Mohamad Eid, S., Shalaby, N. S. & Heeba, M. Supportive care provided by companion during childbirth and it’s effect on labor progress and maternal satisfaction. Port Said Sci. J. Nurs. 7(3), 218–243 (2020).
Handelzalts, J. E., Levy, S., Ayers, S., Krissi, H. & Peled, Y. J. Two are better than one? The impact of lay birth companions on childbirth experiences and PTSD. Arch. Women’s Mental Health 25(4), 797–805 (2022).
Kassa, B. G., Beyene, F. Y. & Demilew, B. C. J. Maternal satisfaction with emergency obstetric and newborn care services in Ethiopia and the associated factors: A systematic review and meta-analysis. Womens Health. 19, 17455057231183854 (2023).
Nguyen, H. H. & Heelan-Fancher, L. Female relatives as Lay Doulas and birth outcomes: A systematic review. J. Perinat. Educ. 31(2), 111–123 (2022).
Sena, M. M., Barros, M. A. R., Holanda, S. M., Aquino, P. D. S. & Cardoso, A. Factors associated with puerperal women’s perception of the support received from their companions during labor and delivery. Int. J. Gynecol. Obstetr. 161(2), 517–524 (2023).
Broxson, J. & Feliciano, L. J. P. C. M. Understanding the impacts of caregiver stress. Prof. Case Manag 25(4), 213–219 (2020).
Acknowledgements
The authors would like to thank the Vice Chancellor of Research and Technology of Gonabad University of Medical Sciences for providing financial support for the study.
Funding
The study was financially supported by Gonabad University of Medical Sciences (Grant number 256).
Author information
Authors and Affiliations
Contributions
Study concept and design: N.B, A.N, F.M., and N. B.Data gathering: S.K and A.D Analysis and interpretation of data: F.M, N.B, A.N, and S.DDrafting of the manuscript: F.M, N.B, A.N, and S.D Critical revision of the manuscript for important intellectual content: All of the authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Gonabad University of Medical Sciences (Code: IR.GMU.REC.1397.052). All participants were briefed about the study’s aims and gave written informed consent before entering the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Nasirzadeh, A., Mohammadzadeh, F., Kazeminia, S. et al. Relationship between the anxiety of labor companion and labor satisfaction among laboring women. Sci Rep 15, 19424 (2025). https://doi.org/10.1038/s41598-025-04754-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-04754-2
