
Abstract
Passing as non-autistic (PAN) is the phenomenon by which an autistic person does not present as autistic in certain contexts. Despite a proliferation of research on the construct on PAN, no study has yet examined the neurocognitive processes implicated in PAN. This study examined two well-characterized event-related potentials (ERPs) often associated with autism - the N170 and the Late Positive Potential (LPP) - in response to faces as putative mechanisms of PAN. Participants were 44 community-recruited youth (Mage = 13.36, Nmale = 30) who completed a facial emotion recognition task during EEG recording. PAN was operationalized using best practices (moderation) for calculating the discrepancy between community informant (parent and teacher) and clinician-reported autism symptoms. Results reveal a substantial proportion (approximately 44%) of the community-recruited adolescent sample met criteria for PAN. This status was associated with faster N170 latency to faces, and attenuated LPP amplitude to facial emotions, particularly subtle facial emotions. Findings suggest autistic adolescents who PAN may have more efficient automatic process of, and reduced reactivity to, social stimuli. This study provides the first direct test of a potential neurocognitive mechanism of PAN, supporting emotion regulation-mediated PAN models.
Similar content being viewed by others

Introduction
While autism is historically defined by pervasive difficulties with social interaction1, recent research has highlighted that contextual variability in social interaction may be the norm—rather than the exception—for autistic youth2,3,4. Most notably, substantial literature has emerged validating the phenomenon of passing as non-autistic (PAN5), in which autistic individuals present such that others do not identify them as autistic in some settings6,7,8,9,10. While considerable empirical work has begun to unpack what the impact of PAN may be on autistic individuals, most efforts to identify the mechanisms underlying PAN have remained either anecdotal or theoretical to date6. Consensus has begun to emerge, though, that those who PAN may respond to social stimuli in a fundamentally different way than autistic (and non-autistic) individuals who do not PAN11. A better understanding of what specific aspects of response to social stimuli may characterize those who PAN is crucial for both understanding and phenomenology of the experience of PAN, efforts to address the consequences of doing so repeatedly over time, and the development of interventions to reduce situations in which PAN occurs more generally. Thus, research is needed to identify specific social neurocognitive predictors of PAN in autistic youth.
PAN in autism
Many definitions have emerged regarding the PAN phenomenon5. However, the most straightforward index implicates variation in autism features by context2,3: the presentation of clear autism features in one (e.g., clinical) context with the clear absence of detection of such features in another (e.g., social) context. This definition benefits from a lack of prima facie confounding by intentionality, self-perception, or an individual’s belief about the value of PAN - it is purely descriptive in nature. Previous research, including a comprehensive review of the relevant literature to date, has proposed PAN to function as an umbrella construct encompassing camouflage, masking, compensation, and other terms encompassing multiple phenomena that have the same end result of autistic presentation varying by social context5.
This definition of PAN is generative regarding underlying mechanisms: how does an unambiguously autistic youth present as non-autistic among their peers? Several theories have been proposed, including the use of compensatory cognitive strategies12, increased emotion regulation13, and strengths in other specific domains14. However, for any of these strategies to work, they rely on upstream differences in neural mechanisms implicated in processing social information. Without such differences (whether intentional or not, perceptual or cognitive), adjustment of behavior in response to social context would not be possible. While well-established social and general learning models suggest the presence of such mechanisms for adjustment of behavior across context15little is known about how they operate in practice.
Neural indices of social processing in autism
Face processing is the most well-studied domain of social information processing16,17,18,19, with event-related potential (ERP) indices of electroencephalogram (EEG) activity being especially promising and practical in the study of autism20,21. The N170 is the most well studied ERP in autism, representing an early, negative-going deflection that is considered an obligatory perceptual marker thought to differentiate faces from non-face stimuli17,21. Differences in the N170 are thought to reflect slowed automatic responses to faces among autistic individuals, yielding difficulties keeping up with the rapid-fire pace of the social world22.
Recent work suggests later affective processing differences may discretely relate to how autistic individuals process the social world. A distinction must be made between the processing of emotional stimuli and the processing of facial stimuli, both of which are utilized in the processing of emotionally salient faces, but which are thought to be indexed by different ERPs. Indeed, the Late Positive Potential (LPP) is a sustained positive ERP deflection beginning ~ 300 ms after stimulus onset, which increases in response to emotionally evocative stimuli23. The LPP represents a region in the post-stimulus time course that has been implicated in machine-learning models as differentiating the EEG response of autistic vs. non-autistic individuals24. Differences in the LPP have been identified in autism, with some studies finding attenuated LPPs25, but others finding larger LPPs to faces dependent on the emotional face (subtle vs. overt) intensity26.
Autism-related differences in N170 implicate different neurocognitive social response processes than in the LPP: slowed automatic processing of facial stimuli vs. reduced (or enhanced) affective (arousal) processing of them. Crucially, efforts to identify consistent differences in these ERPs associated with autism have not come to fruition, even under highly controlled conditions27. While one source of inconsistency may lie in the stimuli (e.g., overt vs. subtle emotions), contextual variability in autism feature presentation is common2 and implicates another possibility: variation in ERP response may relate to differences in the context of measurement (e.g., clinicians vs. parents vs. teachers). Moreover, given that such variability is often exhibited within-person, it may be that analytically combining individuals who present with more autistic features in one context but not another (e.g., clinic vs. classroom) and those who do not (e.g., same presentation across context) obscures important effects that better map the autistic phenotype. Nevertheless, no research has yet examined if these relationships between these ERPs and autism features are context specific. Crucially, this very approach (i.e., examining discrepancies between informants in their view of the same individual regarding the same construct across different contexts) has successfully and reliably been used to detect valid context-specific information in other (non-autistic) populations (e.g., disruptive behavior, social anxiety)28,29,30.
The present study
While there has been much conjecture regarding differences in how those who PAN experience the social world7,10,31,32, no research has yet examined the neurocognitive processes that may be implicated in PAN. This study examined well-characterized ERP responses to faces as trait-level factors in relation to PAN among adolescents, operationalizing PAN as the discrepancy between presentation of autistic features in familiar public and private settings (i.e., home and classroom, measured by the Social Responsiveness Scale- second edition (teacher and parent report SRS-2)33 versus clinical setting, measured by the Autism Diagnostic Observation Schedule—second edition (ADOS-2)34. We hypothesized that (1) participants would present according to each of the dimensions of relationship between SRS (parent report and teacher report) and ADOS-2. That is, both convergence (e.g., high SRS-2 with high ADOS-2) and discrepancy (e.g., high SRS-2 with low ADOS-2) would be evident in the sample. We then hypothesized that (2) the N170 & LPP ERPs would relate to autism traits. Replicating known relations among these factors, we expected these relations would be stronger in the presence of subtler facial emotion stimuli. Finally, we hypothesized that (3) this relationship would vary as a function of PAN. That is, the discrepancy between public (teacher report SRS-2) and clinical (ADOS-2), and the discrepancy between private (parent report SRS-2) and clinical (ADOS-2) presentation of autistic features, would relate to the face-responsive ERPs (N170 and LPP) above and beyond univariate relationships, and that this effect would be driven by those who PAN (low familiar [public and private], high clinical presentation of autistic features).
Results
The autistic group had significantly higher ADOS-2 and parent report SRS-2 scores, and marginally higher teacher report SRS-2 scores, compared to the non-autistic group (Table 1).
Autistic presentation across dimensions of familiar and clinical settings
Participants varied across dimensions such that there was a substantial proportion of participants in both agreement groups and both discrepancy groups. This was evident using both parent report and teacher report SRS-2 (see Fig. 1). In the overall sample, group membership was not unevenly distributed when examining the parent report SRS-2 (χ2(1, N = 44) = 0.13, p =.72) or the teacher report SRS-2 (χ2(1, N = 44) = 1.02, p =.31) in association with the ADOS-2.

Scatterplot of SRS-2 and ADOS-2 by autism diagnostic group placement. ADOS-2 = Autism Diagnostic Observation Schedule, 2nd edition; SRS-2 = Social Responsiveness Scale, 2nd edition. Quadrants are determined using the recommended clinical cutoffs for each measure (ADOS-2 CS = 4; SRS-2 = 76). Groupings (autistic vs. non-autistic) are determined by combination of ADOS-2, SCQ, and diagnostic history, or ADI-R score when ADOS-2 and SCQ cutoffs were exceeded in absence of diagnostic history. Jitter applied to the graphs for readability, all scores are whole numbers. A Within the subset of participants placed in the non-autistic group (n = 27), n = 16 (59%) had convergent low scores on the ADOS-2 and SRS-2 Teacher, n = 2 (7%) had low ADOS-2 but high SRS-2 Teacher scores (DISC), n = 7 (26%) had high ADOS-2 but low SRS-2 Teacher scores (PAN), and n = 2 (7%) participants had convergent high scores. Within the subset of participants placed in the autistic group (n = 17), n = 13 (76%) had high ADOS-2 but low SRS-2 Teacher scores (PAN), and n = 4 (24%) participants had convergent high scores. B SRS-2 Parent and ADOS-2: Within the subset of participants placed in the non-autistic group (n = 27), n = 14 (52%) had convergent low scores on the ADOS-2 and SRS-2 Parent, n = 4 (15%) had low ADOS-2 but high SRS-2 Parent scores (DISC), n = 9 (33%) had high ADOS-2 but low SRS-2 Parent scores (PAN). Within the subset of participants placed in the autistic group (n = 17), n = 10 (59%) had high ADOS-2 with low SRS-2 Parent scores (PAN), and n = 7 (41%) participants had convergent high scores.
Within the subset of non-autistic participants (n = 27), group membership was not unevenly distributed when examining the parent report SRS-2 (χ2(1, N = 27) = 2.35, p =0.13) or the teacher report SRS-2 (χ2(1, N = 27) = 0.59, p =0.44) in association with the ADOS-2.
Since all participants in the autistic subset (n = 17) scored above the indicated cutoff on the ADOS-2, χ2statistics examining group distribution by parent report and teacher report SRS-2 scores and ADOS-2 comparison scores could not be computed. Still, these participants varied regarding whether their high ADOS-2 comparison scores were in agreement with or discrepant with (i.e., PAN) parent report or teacher report SRS-2 scores.
Face-responsive ERPs (N170 & LPP) in relation to autism features
ADOS-2 comparison scores were marginally negatively correlated with P7 N170 latency response to all faces (r = −0.261, p =0.088) but no other relationships were found with the N170 (Fig. 2; Table 2).

Grand average waveforms of the A N170 and B LPP by autism diagnostic group. LPP = Late Positive Potential. The N170 was extracted from the left (P7 electrode) and the right (P8 electrode) hemisphere. The Late Positive Potential (LPP) was the average of central electrodes (Cp1, Cp2, Cz).
ADOS-2 was negatively correlated with LPP overall (r = −0.483, p <0.001), as well as for both subtle (r = −0.490, p <0.001) and overt (r = −0.412, p =0.005) intensity faces. Additionally, teacher report SRS was negatively correlated with LPP overall (r = −0.377, p =0.012), as well as with LPP to overt faces (r = −0.393, p =0.008), and LPP to subtle faces (r = −0.301, p =0.047). Parent report SRS was marginally negatively correlated with LPP overall (r = −0.266, p =0.081), as well as with LPP to overt (r = −0.261, p =0.087), but not subtle faces (r = −0.232, p =0.130).
Relation between face-responsive ERPs and PAN
An interaction was found between ADOS-2 and teacher report SRS-2 scores in predicting N170 latency (P7 - left lateralized) in response to all faces (B = 0.27, p =0.04; See Table 3). For those with low and moderate teacher report SRS-2 scores, higher ADOS-2 comparison scores were related to faster N170 responses; this was not the case for those with high teacher report SRS-2 scores (Fig. 3). In other words, those who PAN exhibited significantly faster N170 latencies than non-autistic, as well as autistic, but not PAN, peers. This effect was not present at differing levels of facial emotion intensity (both p >0.09).

Probing of the interaction between SRS-2 Teacher T-Scores and ADOS-2 Comparison Scores in predicting the N170 to faces. ADOS-2 = Autism Diagnostic Observation Schedule, 2nd edition; SRS-2 = Social Responsiveness Scale, 2nd edition. The ADOS-2 Score predicted N170 latency at low (β= −7.38, p =0.0073) and moderate (β = −3.71, p =0.032), but not high levels (β = 1.48, p =0.597) of SRS-2 Total T-Score. Data are stratified for visualization and interpretation purposes, consistent with standard moderation analysis techniques. However, moderation analyses were conducted on continuously-distributed moderator variables.
Further, a marginal interaction was found between ADOS-2 and teacher report SRS-2 scores in predicting LPP to overall faces (B = 0.0292, p =0.0595). Specifically, for participants with low (B = − 0.986, p =0.002) and medium (B = − 0.592, p =0.004) teacher report SRS-2 scores, ADOS-2 predicted LPP amplitude; this effect was not present for participants with high teacher report SRS-2 scores (B = − 0.034, p =0.917). When probing based on facial emotion intensity, this effect was present in predicting LPP amplitude to subtle (B = 0.036, p =0.024) but not overt (B = 0.023; p =0.214) facial expressions. Specifically, for participants with low and moderate teacher report SRS-2 scores, ADOS-2 predicted attenuated LPP amplitudes to subtle faces (Fig. 4): low teacher report SRS-2 and high ADOS-2 (i.e., individuals who PAN) related to smaller LPP amplitudes.
Finally, no interactions were found between ADOS-2 and parent report SRS-2 in predicting N170 latency in response to all faces (B = −0.02; p =0.88), nor when broken down into subtle and overt (all p >0.73). There were also no interactions for LPP amplitude in response to subtle faces (B = 0.02; p =0.18), nor overall/overt faces (all p >0.14).

Probing of the interaction between SRS-2 Teacher T-Score and ADOS-2 Comparison Score in predicting the LPP to subtle emotional faces. LPP = Late Positive Potential; ADOS-2 = Autism Diagnostic Observation Schedule, 2nd edition; SRS-2 = Social Responsiveness Scale, 2nd edition. The ADOS-2 Score predicted LPP amplitude at low (β = −1.15, p <0.001) and moderate (β = −0.67, p =0.0013), but not high levels (β = 0.0059, p = 0.99) of SRS-2 Total T-Score. Data are stratified for visualization and interpretation purposes, consistent with standard moderation analysis techniques. However, moderation analyses were conducted on continuously-distributed moderator variables.
Discussion
This was the first study to explore possible neural indices of PAN. We found that there was a wide array of presentations along the ADOS-2 and SRS-2 distributions. The examined neural indices, N170 latency and LPP amplitude, were compared to autism traits measured by both ADOS-2 and SRS-2. N170 was not correlated with either, but LPP was correlated with ADOS-2 and teacher report SRS-2. We also examined the relationship between these neural indices and the relationship between ADOS-2 and SRS-2 (teacher report and parent report). We found that, among participants with a low teacher report SRS-2, ADOS-2 successfully predicted N170 latency for all faces, and LPP amplitude for subtle faces such that higher ADOS-2 comparison scores correlated with faster N170 and smaller LPP.
Distribution of autistic presentation across settings
It was hypothesized that participants would present with a wide range of agreement and discrepancy in autistic presentation across settings. The individuals represented in this sample illustrate the dynamic nature of autistic presentation—not just between individuals, but within an individual’s own experiences. The variation by context and informant reveals important insight into the ways we measure and conceptualize autistic traits, as previously the field has favored a more static view of presentation. This context-dependent presentation is increasingly viewed as a defining phenotype within autism2, and in future research can be used to further explain variation within a group. Accounting for this variation in recruitment, possibly by strategically utilizing multiple sources (based on those that are thought to be most likely to provide opportunities for detecting youth who do versus do not PAN), may also open doors for a more representative sample of participants who may have previously been excluded if they PAN in certain contexts.
The informant discrepancy highlighted by these findings suggests that many autistic children may be at risk of being overlooked. School is one of the main opportunities for children to be referred for assessment35, and often testimonials from teachers and academic records play a large part in assessment and accommodations36,37. If other sources of referral are not available or are inadequate, autistic children who PAN in classroom settings are at a disadvantage for identification and referral.
This variation also highlights and reaffirms the importance of diversified sampling approaches. Autism research often exclusively samples from clinical settings or utilizes prior clinical diagnosis for inclusion, which may leave out many who PAN5. Different sampling sources, such as the community-based approach utilized in this study, may help capture individuals who have been historically excluded. This helps to better define the contours of the autistic phenotype as we continue to explore the rich diversity of autistic experience and presentation.
ERP indices of autistic presentation
It was hypothesized that N170 latency and LPP amplitude would relate to autism traits. N170 was not correlated to autism traits, highlighting an inconsistency of the N170 relationship with autism in the literature38. While it may be a biomarker21, it is likely not a diagnostic biomarker, but rather a stratifying one27. While we did not find strong correlations between N170 and autism traits, LPP was correlated with autism traits as measured by the ADOS-2 and teacher report SRS-2, and marginally correlated with parent report SRS-2. These findings indicate LPP as a point of interest when teasing apart differences in autistic vs. non-autistic neurocognitive processing of social interaction39.
It is worth noting that LPP did not correlate with N170. Due to the related nature of these neural indices, this was important to consider in order to rule out the possibility that differences in LPP were simply extensions of earlier differences in N170. The lack of correlation between the two indicates that, within the context of this study, the two may measure discrete processes - automatic processing for N170 and affective processing for LPP—without the influence of the other.
ERP indices of PAN
It was hypothesized that the relationship between the ERPs of interest and autism traits would vary as a function of PAN. The relation of N170 latency and LPP amplitude to PAN provides a novel window into understanding how those who PAN process their social world. In terms of N170, youth who PAN showed faster latencies than all other groups. Indeed, among youths with low teacher report SRS-2 scores, higher ADOS-2 comparison scores related to faster N170 latencies. This finding runs counter to the literature indicating slowed N170 as an index of autistic-like face processing38. There are a few possible implications of this. First, it may be that past findings recruited autistic samples that do not PAN; many of these studies involve rigorously-characterized samples of autistic youth, which would exclude those with the subtler social presentation of the PAN group. Second, the N170 becomes faster over the course of adolescence as behavioral indices of face perception improve16; it may be, then, that there is a greater acceleration among a subgroup of autistic youth, and this group then develops the ability to PAN. Conversely, behavioral differences may instead be upstream: perhaps those autistic youth who PAN engage differentially with social stimuli in their environment, leading to an acceleration of N170 across development—creating a bifurcation in what was previously a monolithic group. Future research should consider these possibilities.
Similarly, youth who PAN showed attenuated LPP in response to subtle, but not overt, faces. For youth with low teacher report SRS-2 scores, higher ADOS-2 related to smaller LPP amplitudes in response to subtle facial expression. This converges with some prior literature showing that LPP response to social stimuli is smaller in autistic individuals25. While older interpretations suggest that LPP indexes subjective emotional significance of stimuli40, more recent research implicates LPP in the processing of stimuli that cause high arousal and reactivity, regardless of subjective significance41. These findings, then, could point to a lower emotional reactivity in response to subtle facial stimuli in youth who PAN42.
Looking at both the faster N170 and attenuated LPP in the PAN group, there are a few potential explanations. First, autistic adolescents who PAN may simply have more practice quickly processing social stimuli and subsequently regulating their emotions to fit in. Based on the reduced LPP response specifically to subtle stimuli, it is possible that these individuals have learned over time to suppress overt reactions to ambiguous peer responses that may cause uncertainty, whereas overt stimuli by nature may be easier to rapidly interpret and therefore not require the same suppression. Another possibility, as noted above, is that these adolescents have developed faster automatic processing of social stimuli, making it easier to keep up with non-autistic peers, and lower arousal in response to subtle social stimuli, therefore not engaging in disruptive or socially inappropriate behavior that would normally indicate the presence of autism to a teacher. Overall, future research should consider each of these components, as well as related socially linked ERPs, in examining the neural correlates of PAN.
One last possible explanation is that these results relate to alexithymia, which is a trait common in autistic individuals43 that makes it difficult to experience, identify, or describe emotions and inner feelings44,45. Indeed, this difficulty with emotion processing is often (incorrectly) cited as a core feature of autism46,47. These results highlight the possibility that the experience of PAN may present a variation in the experience of alexithymia in autistic youth. For instance, autistic individuals who PAN may experience less alexithymia than those who do not. Future research should explore variations in alexithymia in association with various operationalizations of PAN to explore this possibility. Notably, the LPP has previously been associated with alexithymia when elicited during primed emotion regulation tasks48. While these tasks differ substantially from the ones used here (wherein no reappraisal or regulation instructions were given), these previous findings nonetheless further the intriguing possibility that alexithymia is implicated in the relationship between LPP and PAN. Future research should directly address this possibility, with the aim of disambiguating the interplay between the PAN, the LPP, and alexithymia, including the role emotion regulation may play in representing and/or mediating these relationships.
Clinical implications
These findings highlight the presence and unique presentation of autistic adolescents who are otherwise not likely to be identified. One key question that arises is the degree to which the group identified here (PAN) overlaps with other established definitions of groups with less pronounced public presentation of autistic features. For instance, the field has long identified the presence of a broader autism phenotype (BAP)49, those who were previously diagnosed but lose that diagnosis by adolescence50,51, masking and camouflaging as defined in ways that may differ from PAN as described here7,31,52, and ESSENSE53,54. It remains an open question whether these groups represent the same individuals as one another (as well as the PAN group identified here), and, if not, which features may distinguish them. It is imperative for future research to continue to explore the parameters of these groups developmentally, clinically, and socially to better understand their overlap within—and beyond—the autism spectrum.
As noted, our results indicate that the N170 is not reliably slower in all autistic individuals. This suggests the possibility that the N170 may be at least in part indexing important (perhaps developmentally or contextually mediated) information about in vivo social presentation of autistic features, rather than “core” autism features per se. This also implicates the inverse possibility: that examining presumably non-autistic samples of youth may reveal variations in N170 latency that relate to otherwise unidentified or non-impairing features of autism that distribute across non-autistic populations55.
Overall, these findings highlight the urgency of better understanding the neurocognitive mechanisms underlying PAN. Indeed, the varying features and parameters of PAN (e.g., intentionality, effectiveness, emotional burden, response to stigma)5 each implicate discrete potential mechanisms that bear future study. Thus, as the field continues to refine and specify methods for measuring PAN11, it is crucial to consider these implications and examine them empirically.
Limitations
This study was subject to several limitations. First, the sample size was fairly small, which could limit the generalizability of the findings to the broader autism community. However, it is notable that this is the first known study which sought to identify PAN youth in this way. Indeed, usual screening procedures (i.e., an individual exceeds cutoffs on a questionnaire such as the SRS-2 to then be eligible for receiving a more thorough assessment such as the ADOS-2), would explicitly exclude the participants we identified as PAN here. Thus, despite being a small initial sample, the presence of this group at all (representing > 50% of those who ended up presenting with high ADOS-2 comparison scores) underlines the importance of future efforts to identify and characterize this novel group. Second, the study focused exclusively on ERPs elicited by facial stimuli. This restricts understanding of neural responses to broader categories of stimuli and limits the application of the findings to real-world scenarios involving non-facial social stimuli. Additionally, although the use of LPP and N170 components in this study was informed by prior literature, a more comprehensive understanding of the underlying neural processes cannot be determined without analyzing additional ERPs. Next, reliance on current gold-standard autism diagnostic measures may have yielded unusually high specificity in diagnostic threshold determination, thereby excluding some individuals who may meet clinical diagnostic criteria and yet still PAN in familiar contexts. Additionally, due to the correlation between the SRS-2 and other behavioral measures56, it is possible that the PAN group may represent those with autism but fewer visible co-occurring behavioral concerns, rather than purely those who present as non-autistic in public. Indeed, other behavioral features (e.g., co-occurring internalizing or externalizing symptoms) were not examined, which could provide a more thorough understanding of this unique population. These limitations should be considered when interpreting the results of this study.
Future directions
Future work should continue to probe the neurocognitive processes underlying PAN, as well as how adolescents who PAN differ from their peers. This work is important as the field continues to expand our understanding of PAN, which may help identify these individuals sooner and aid in attempts to develop and provide targeted support where appropriate. Identifying these individuals is imperative, as it will allow for a more accurate understanding of the diverse ways autism can present. This may also promote inclusion and acceptance by challenging stereotypes and stigma. Additionally, identifying these individuals in childhood and adolescence will aid in connecting them to resources that may improve their quality of life. This is especially true for autistic girls and children of color, who may be more likely to PAN and are disproportionately affected by inaccessibility of care5.
Future work should also investigate how different operationalizations of PAN affect which individuals are captured. Finally, future work should consider the effectiveness of existing supports and interventions within this group, as well as whether these individuals require the same types of support within the same domains as their more classically-presenting autistic peers. Thus, future work should investigate potential unique struggles and long-term outcomes of those who PAN, especially in social, academic, occupational, and mental health domains.
Methods
Participants
Participants included 44 adolescents aged 11–17 years recruited from the greater Long Island area (Mage = 13.36 years; rangeage = 11.24–17.62 years; SDage = 1.82; Nautistic = 17; Nmale = 30; Table 1). Exclusion criteria included a measured IQ < 70, the presence of a significant medical or cognitive impairment that would interfere with study participation, a known developmental disability other than autism that would interfere with study participation, a verbal ability incompatible with administration of the ADOS-234 Module 3 or 4, and/or if the adolescent or their parent were non-English speaking.
Procedures
All methods and protocols were carried out in accordance with relevant guidelines and regulations and were approved by the Stony Brook University Institutional Review Board. Informed consent was obtained from all subjects and/or legal guardians.
Recruitment
Participants represent a community sample recruited from local school districts, family-oriented events, autism-focused organizations, and community mental-health agencies in the Long Island area. To facilitate the collection of teacher reported data, study personnel met with the superintendent of each participant’s school district and secured a research agreement. This agreement provided study personnel district-level permission to contact teachers and request that they consider study participation. Only teachers nominated by participating parents in districts with an active research agreement were recruited for study participation. Informed consent was obtained from all parents and teachers and all adolescents assented to study procedures. Study procedures were approved by the University’s Institutional Review Board and conform to Common Rule standards.
Diagnostic group placement
Administration of the Kaufman Brief Intelligence Test, 2nd Edition (KBIT-2)57 confirmed an IQ > 70 for each participant. Phone screening procedures were used to assess the presence of all other exclusionary criteria. Autistic group inclusion criteria were: high sensitivity cutoffs (see below; used due to the community-recruited sampling approach) on the ADOS-234 and Social Communication Questionnaire (SCQ)58, and a parent reported prior or current diagnosis of autism. If adolescents met cutoff criteria, but their parents did not report a prior or current autism diagnosis, the Autism Diagnostic Interview-Revised (ADI-R)59 was administered by a research-reliable staff member; in this case, adolescents meeting a total score of ≥ 16 on the ADI-R were also placed into the autistic group. Participants who did not meet either of the criteria outlined above were placed into the non-autistic group.
Data collection
Following the determination of study eligibility and group placement, adolescents attended an additional study visit during which they completed the Diagnostic Analyses of Nonverbal Accuracy-2 (DANVA-2)60, a facial emotion recognition task, while undergoing simultaneous EEG recording18,26,61. Parents accompanied their adolescent to each study visit and completed a developmental history questionnaire reporting their child’s demographic characteristics, developmental history, and diagnostic history as well as the SRS-2. Parents also provided study personnel with contact information for a teacher who had substantial day-to-day interaction with the child and was best able to report on their child’s social interactions with peers in the school. Once a teacher was identified, study personnel confirmed that an active research agreement was in place with the district and reached out to the teacher via email to schedule a school-site visit. Teachers then completed the teacher-report version of the SRS-2. Families who elected to receive a report on their child’s results were given a comprehensive report.
Measures
ADOS-2
The ADOS-234 is a standardized, observational measure that involves presses to elicit social, verbal, imaginative, and physical (e.g., gesture) responses. In the current study, ADOS-2 Module 3 and Module 4 were used since these modules incorporate conversations, therefore are appropriate for verbally fluent children and adolescents, and the specific module was selected based on developmental level (i.e., whether it would be appropriate to play with make believe toys). Trained, research-reliable clinicians administered and scored the ADOS-2. Each ADOS-2 module yields a Module-specific diagnostic algorithm score (revised algorithm utilized for Module 4)62. In the present study, an algorithm score of six or greater was used as a “high sensitivity” inclusion cutoff. Separately, normed “comparison scores” (CS) were derived so that traits may be compared across language and developmental levels62,63; the CS was used for all continuous analyses.
KBIT-2
The KBIT-257 is a brief intelligence measure for individuals ranging from 4 to 90 years old. It includes a non-verbal, verbal, and overall composite IQ score.
SCQ
The SCQ58 includes 40 yes/no questions completed by a parent or caregiver of a child over 4 years of age with a mental age of at least 2 years old. A total score ≥ 11 was used as a “high sensitivity” inclusion cutoff.
SRS-2
Caregivers and teachers completed the SRS-2, a 65-item tool that assesses both the presence and severity of features associated with autism33. In addition to identifying levels of social functioning within the autism spectrum, the SRS-2 can also be used to differentiate between autism and other disorders with accompanying social deficits, making it a favorable tool for differential diagnosis64,65,66. SRS-2 T-Scores per parent report and teacher report are used in the current analysis.
DANVA-2
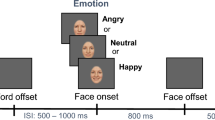
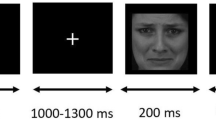
The Diagnostic Analyses of Nonverbal Accuracy-2 (DANVA-2) is a standardized measure of emotion recognition, which includes facial emotion recognition, and was completed by participants during EEG recording18,26,60. It has been widely-used in autistic populations67. Stimuli for the DANVA-2 facial emotion recognition task include a total of 48 naturalistic color photos, which is comprised of females (24) and males (24). These photos are of the head and torso and show facial emotion expressions either overtly (high intensity; 24) or subtly (low intensity; 24). The facial emotion expressions include happy (12), sad (12), angry (12), and fearful (12); in addition, one subtest is adults above the age of 18 years (24) and the other subtest is children ages 6 to 12 years (24). The emotional valence and intensity was based on consensus rating from students, ranging from third grade to college level, with at least 80% of coders in agreement60. The photos were digitized images superimposed on a black background and displayed on a computer screen at a visual angle of 22.5° (width)×15.5° (height). The face occupied about 4.75° (width)×6° (height) of the visual angle. The face was presented on the computer screen for at least 1000 ms and at most 3000 ms. Participants were instructed to identify the emotion presented on the screen (happy, fearful, sad or angry) using a button box. This behavioral response elicited trial advancement, a blank-screen inter-trial interval was presented for 1000 ms, after each response. If a participant did not respond within the 3000 ms time window, the picture of the face disappeared from the computer screen, and the response options (i.e., text) remained on the screen until the participant responded26.
EEG acquisition and processing
EEG data were collected while participants completed the DANVA-2, using a 32-channel BrainVision actiCAP (Brian Products). All trials were included in ERP analyses, regardless of emotion identification accuracy. Channels are arranged in the international standard 10/20 system with Ag/AgCl active electrodes and an actiCHamp amplifier. Four facial electrodes were placed to collect electrooculogram (EOG) response approximately one centimeter below the right eye, above the right eye, to the left of the left eye, and to the right of the right eye. SuperVisc electrolyte gel was applied to each electrode to reduce signal impedance to ≤ 10 kΩ. Data were recorded continuously using BrainVision Recorder software at a 500 Hz sampling rate. BrainVision Analyzer 2.1 was used for offline data reduction. Data were re-referenced to an average reference of all the channels then filtered using a Butterworth filter, with a low cutoff of 0.1 Hz and a high cutoff of 30 Hz. Ocular correction using the Gratton and Coles algorithm68 and semi-automatic artifact rejection were completed on epochs ranging from 200 ms before and 1000 ms after stimulus onset, when the face appeared on the screen. For automatic artifact rejection, the program identified artifacts based on the following criteria: voltage step of greater than 50 µV/ms, a difference of values in intervals of more than 175 µV with an interval length of 400 ms, and activity in intervals of 100 ms lower than 0.5 µV. In the manual phase of artifact rejection, program-identified artifacts were approved or rejected by a trained research assistant and each epoch was visually inspected for additional artifacts, such as drift. Data were baseline corrected against − 200 to 0 ms before stimulus onset. The N170 peak amplitude (i.e., mean value around the peak +/- 25 ms) was extracted from 160 to 270 ms at P7 and P8 electrodes, consistent with prior work showing the N170 occurs at occipitotemporal sites69. The LPP mean amplitude was extracted from 500 to 1000 ms from the average of Cz, Cp1, and Cp2 electrodes, consistent with prior work showing the LPP occurs at midline centroparietal sites70.
The autistic and non-autistic group did not differ significantly in the number of trials retained overall, in the overt emotional face condition, nor in the subtle emotional face condition (all ps ≥ 0.308). Early components, such as the N170, stabilize as early as 10 trials71 and the LPP signal stabilizes at 10 trials72, thus the threshold for inclusion in the final analyses was at least 10 usable trials in each condition. After removing participants without an SRS-2-Teacher score, 62 participants remained. Of these participants, 16 were removed as they had no ERP data, one was removed due to excess noise, and one was removed due to insufficient trials, yielding our final N = 44 for this project. For LPP (i.e., the average at Cz, Cp1, & Cp2 electrodes), an average of 46.9 trials (SD = 1.85) were included in the analyses across all faces with an average of 23.3 trials (SD = 1.11) for the overt condition and an average of 23.5 trials (SD = 0.921) for the subtle condition. For the N170 (i.e., the average at P7 & P8 electrodes) an average of 47.0 trials (SD = 1.42) were included in the analyses across faces with an average of 23.4 trials (SD = 0.884) for the overt condition and an average of 23.6 trials (SD = 0.759) for the subtle condition.
Data analytic plan
To examine hypothesis 1, that participants would present with both convergence and discrepancy profiles across SRS-2 and ADOS-2, we examined the visual distribution of the relationship between ADOS-2 and parent report SRS-2 scores, and between ADOS-2 and teacher report SRS-2 scores. Additionally, participants were binned into four groups: high SRS-2/high ADOS-2 (agreement), low SRS-2/low ADOS-2 (agreement), high SRS-2/low ADOS-2 (discrepant, informant social concerns [DISC]), low SRS-2/high ADOS-2 (PAN). χ2 tests were used to compare distributions across convergence and discrepancy group membership.
To examine hypothesis 2, that N170 latencies and LPP amplitudes would relate to autism traits, we examined correlations between each of these ERPs and SRS-2 (parent and teacher report) and ADOS-2 comparison scores across the whole sample. Specifically, we looked at the correlation with these ERPs in response to all faces, as well as in response to overt and subtle faces, specifically.
Finally, to examine hypothesis 3, whether this relationship varies as a function of PAN, we analyzed the discrepancy between SRS-2 (parent and teacher report) and ADOS-2 comparison scores in relation to these ERP components. To operationalize PAN, we used moderated regression, which, in contrast to traditional difference score methodologies, is unconfounded by source variance and allows for estimates of the true relationship between informant discrepancies and variables of interest73,74. Thus, the discrepancy between SRS-2 T-Scores and ADOS-2 comparison scores were calculated using interaction terms, centering each predictor variable75, predicting each given ERP component (N170 latency, LPP amplitude; overall, as well as to subtle and overt faces); these models were run twice, once for parent report SRS-2 and once for teacher report SRS-2. In these models, if the parent or teacher reported little to no autism traits despite the ADOS-2 revealing clear symptomatology, the child would be considered to be PAN in the given setting (home or classroom), despite likely being autistic according to clinical criteria for an autism diagnosis.
Data availability
Data associated with the underlying project are publicly available via the National Institute of Mental Health Data Archive here: https://nda.nih.gov/edit_collection.html? id=2421. For specific questions or data requests, please contact Dr. Matthew Lerner (ml3823@drexel.edu).
References
Hobson, R. P. The coherence of autism. Autism 18, 6–16 (2014).
Kang, E., Lerner, M. D. & Gadow, K. D. The importance of Parent-Teacher informant discrepancy in characterizing autistic youth: A replication latent profile analysis. J. Clin. Child. Adolesc. Psychol. 52, 108–118 (2023).
Lerner, M. D., De Los Reyes, A., Drabick, D. A. G., Gerber, A. H. & Gadow, K. D. Informant discrepancy defines discrete, clinically useful autism spectrum disorder subgroups. J. Child. Psychol. Psychiatry. 58, 829–839 (2017).
Piergies, A. M., Hirota, T., Monden, R. & Zheng, S. Subgrouping school-aged children on the autism spectrum based on co-occurring psychiatric symptoms. Res. Autism Spectr. Disord. 95, 101983 (2022).
Libsack, E. J. et al. A systematic review of passing as Non-autistic in autism spectrum disorder. Clin. Child. Fam Psychol. Rev. 24, 783–812 (2021).
Ai, W., Cunningham, W. A. & Lai, M. C. Reconsidering autistic ‘camouflaging’ as transactional impression management. Trends Cogn. Sci. (2022).
Cook, J., Hull, L., Crane, L. & Mandy, W. Camouflaging in autism: A systematic review. Clin. Psychol. Rev. 89, 102080 (2021).
Hull, L. et al. Putting on my best normal: social camouflaging in adults with autism spectrum conditions. J. Autism Dev. Disord. 47, 2519–2534 (2017).
Lai, M. C. et al. Quantifying and exploring camouflaging in men and women with autism. Autism 21, 690–702 (2017).
Mandy, W. Social Camouflaging in Autism: Is It time To Lose the Mask? Autism vol. 23, 1879–1881 (SAGE Publications, Sage UK, 2019).
Williams, Z. J. & Commentary The construct validity of ‘camouflaging’in autism: psychometric considerations and recommendations for future research-reflection on Lai et al.(2020). J. Child. Psychol. Psychiatry. 63, 118–121 (2022).
Livingston, L. A., Shah, P., Milner, V. & Happé, F. Quantifying compensatory strategies in adults with and without diagnosed autism. Mol. Autism. 11, 15 (2020).
McQuaid, G. A., Sadowski, L. Y., Lee, N. R. & Wallace, G. Perceived stress and emotion regulation mediate associations between camouflaging and internalizing symptomatology among autistic adults. (2022).
Corbett, B. A. et al. Camouflaging in autism: examining sex-based and compensatory models in social cognition and communication. Autism Res. 14, 127–142 (2021).
Crick, N. R. & Dodge, K. A. A review and reformulation of social information-processing mechanisms in children’s social adjustment. Psychol. Bull. 115, 74–101 (1994).
Batty, M., Meaux, E., Wittemeyer, K., Rogé, B. & Taylor, M. J. Early processing of emotional faces in children with autism: an event-related potential study. J. Exp. Child. Psychol. 109, 430–444 (2011).
Kang, E., Clarkson, T., Keifer, C. M., Rosen, T. E. & Lerner, M. D. Discrete electrocortical predictors of anxiety and anxiety-related treatment response in youth with autism spectrum disorder. Biol. Psychol. 146, 107710 (2019).
Lerner, M. D., McPartland, J. C. & Morris, J. P. Multimodal emotion processing in autism spectrum disorders: an event-related potential study. Dev. Cogn. Neurosci. 3, 11–21 (2013).
McPartland, J. C. et al. Looking back at the next 40 years of ASD neuroscience research. J. Autism Dev. Disord. 51, 4333–4353 (2021).
Webb, S. J. et al. Guidelines and best practices for electrophysiological data collection, analysis and reporting in autism. J. Autism Dev. Disord. 45, 425–443 (2015).
Webb, S. J. et al. The autism biomarkers consortium for clinical trials: initial evaluation of a battery of candidate EEG biomarkers. Am. J. Psychiatry. 180, 41–49 (2023).
Mendelson, J. L., Gates, J. A. & Lerner, M. D. Friendship in school-age boys with autism spectrum disorders: A meta-analytic summary and developmental, process-based model. Psychol. Bull. 142, 601–622 (2016).
Hajcak, G. & Foti, D. Significance?… significance! Empirical, methodological, and theoretical connections between the late positive potential and P300 as neural responses to stimulus significance: an integrative review. Psychophysiology 57, e13570 (2020).
Torres, J. M. M. et al. Facial emotions are accurately encoded in the neural signal of those with autism spectrum disorder: A deep learning approach. Biol. Psychiatry Cogn. Neurosci. Neuroimaging. 7, 688–695 (2022).
Benning, S. D. et al. Late positive potential ERP responses to social and nonsocial stimuli in youth with autism spectrum disorder. J. Autism Dev. Disord. 46, 3068–3077 (2016).
Keifer, C. M., Hauschild, K. M., Nelson, B. D., Hajcak, G. & Lerner, M. D. Differences in the late positive potential and P300 to emotional faces in individuals with autism spectrum disorder. J. Autism Dev. Disord. 49, 5009–5022 (2019).
Lerner, M. D. & Day, T. C. Beyond the landmarks: where to next with biomarkers of autism?? Am. J. Psychiatry. 180, 5–7 (2023). (Am Psychiatric Assoc.
De Los Reyes, A., Henry, D. B., Tolan, P. H. & Wakschlag, L. S. Linking informant discrepancies to observed variations in young children’s disruptive behavior. J. Abnorm. Child. Psychol. 37, 637–652 (2009).
De Los Reyes, A. et al. The operations triad model and youth mental health assessments: catalyzing a paradigm shift in measurement validation. J Clin. Child. Adolesc. Psychol. (2023).
Makol, B. A. et al. Integrating multiple informants’ reports: how conceptual and measurement models May address Long-Standing problems in clinical Decision-Making. Clin. Psychol. Sci. 8, 953–970 (2020).
Fombonne, E. Camouflage and autism. J. Child Psychol. Psychiatry. 61, 735–738 (2020). (Wiley Online Library.
Hull, L. et al. Is social camouflaging associated with anxiety and depression in autistic adults? Mol. Autism. 12, 13 (2021).
Constantino, J. N. & Gruber, C. P. Social Responsiveness Scale Second Edition (SRS-2): Manual (Western Psychological Services (WPS), 2012).
Lord, C. et al. Autism diagnostic observation schedule–2nd edition (ADOS-2). Los Angel CA West. Psychol. Corp. 284 (2012).
Ming, X. et al. Access to specialty care in autism spectrum disorders-a pilot study of referral source. BMC Health Serv. Res. 11, 99 (2011).
Filipek, P. A. et al. The screening and diagnosis of autistic spectrum disorders. J. Autism Dev. Disord. 29, 439–484 (1999).
Joshi, G. et al. Examining the clinical correlates of autism spectrum disorder in youth by ascertainment source. J. Autism Dev. Disord. 44, 2117–2126 (2014).
Kang, E. et al. Atypicality of the N170 event-related potential in autism spectrum disorder: A meta- analysis. Biol. Psychiatry Cogn. Neurosci. Neuroimaging. 3, 657–666 (2018).
Clarkson, T., Keifer, C., Lerner, M., Nelson, B. & Jarcho, J. T54. Youth with ASD symptoms have reduced LPP as learn about unpredictable peers during social interactions. Biol. Psychiatry. 85, S149–S150 (2019).
Lang, P. J. & Bradley, M. M. Emotion and the motivational brain. Biol. Psychol. 84, 437–450 (2010).
Schupp, H. T. & Kirmse, U. M. Case-by‐case: emotional stimulus significance and the modulation of the EPN and LPP. Psychophysiology 58, e13766 (2021).
Wiese, A. D., Lim, S. L., Filion, D. L. & Kang, S. S. Intolerance of uncertainty and neural measures of anticipation and reactivity for affective stimuli. Int. J. Psychophysiol. 183, 138–147 (2023).
Kinnaird, E., Stewart, C. & Tchanturia, K. Investigating alexithymia in autism: A systematic review and meta-analysis. Eur. Psychiatry. 55, 80–89 (2019).
Cook, R., Brewer, R., Shah, P. & Bird, G. Alexithymia, not autism, predicts poor recognition of emotional facial expressions. Psychol. Sci. 24, 723–732 (2013).
Shah, P., Hall, R., Catmur, C. & Bird, G. Alexithymia, not autism, is associated with impaired interoception. Cortex 81, 215–220 (2016).
Bird, G. & Cook, R. Mixed emotions: the contribution of alexithymia to the emotional symptoms of autism. Transl Psychiatry. 3, e285–e285 (2013).
Gerber, A. H., Girard, J. M., Scott, S. B. & Lerner, M. D. Alexithymia – Not autism – is associated with frequency of social interactions in adults. Behav. Res. Ther. 123, 103477 (2019).
Walker, S., O’Connor, D. B. & Schaefer, A. Brain potentials to emotional pictures are modulated by alexithymia during emotion regulation. Cogn. Affect. Behav. Neurosci. 11, 463–475 (2011).
Bailey, A., Palferman, S., Heavey, L., Le Couteur, A. & Autism The phenotype in relatives. J. Autism Dev. Disord. 28, 369–392 (1998).
Eigsti, I. M., Fein, D. & Larson, C. Editorial perspective: another look at ‘optimal outcome’in autism spectrum disorder. J. Child Psychol. Psychiatry. 64, 332–334 (2023). (Wiley Online Library.
Fein, D. et al. Optimal outcome in individuals with a history of autism. J. Child. Psychol. Psychiatry. 54, 195–205 (2013).
Miller, D., Rees, J. & Pearson, A. Masking is life: experiences of masking in autistic and nonautistic adults. Autism Adulthood. 3, 330–338 (2021).
Fernell, E. & Gillberg, C. Autism under the umbrella of ESSENCE. Front. Psychiatry. 14, 1002228 (2023).
Gillberg, C. The ESSENCE in child psychiatry: early symptomatic syndromes eliciting neurodevelopmental clinical examinations. Res. Dev. Disabil. 31, 1543–1551 (2010).
Kim, H. et al. Quantifying the optimal structure of the autism phenotype: A comprehensive comparison of dimensional, categorical, and hybrid models. J. Am. Acad. Child. Adolesc. Psychiatry. 58, 876–886 (2019). e2.
Hus, V., Bishop, S., Gotham, K., Huerta, M. & Lord, C. Factors influencing scores on the social responsiveness scale. J. Child. Psychol. Psychiatry. 54, 216–224 (2013).
Kaufman, A. S. Kaufman brief intelligence test—second edition (KBIT-2). Circ Pines MN Am. Guid Serv (2004).
Rutter, M., Bailey, A. & Lord, C. S. C. Q. Soc Commun. Quest Torrance CA West. Psychol. Serv. (2003).
Rutter, M., Le Couteur, A. & Lord, C. A. D. I. R. Autism Diagn. Interview Revis. Man. Los Angel West. Psychol. Serv. (2003).
Nowicki, S. J. Manual for the diagnostic analysis of nonverbal accuracy (DANVA). Unpubl. Manuscr. Dept psychol. Emory univ. Atlanta GA Nowicki SJ carton J1993 meas. Emot. Intensity facial Expr. J. Soc. Psychol. 133, 749–750 (2004).
Keifer, C. M., Mikami, A. Y., Morris, J. P., Libsack, E. J. & Lerner, M. D. Prediction of social behavior in autism spectrum disorders: explicit versus implicit social cognition. Autism 24, 1758–1772 (2020).
Hus, V. & Lord, C. The autism diagnostic observation schedule, module 4: revised algorithm and standardized severity scores. J. Autism Dev. Disord. 44, 1996–2012 (2014).
Gotham, K., Pickles, A. & Lord, C. Standardizing ADOS scores for a measure of severity in autism spectrum disorders. J. Autism Dev. Disord. 39, 693–705 (2009).
Constantino, J. N., Frazier, T. W. & Commentary The observed association between autistic severity measured by the social responsiveness scale (SRS) and general psychopathology–a response to. J. Child. Psychol. Psychiatry. 54, 695 (2013).
Frazier, T. W. et al. Confirmatory factor analytic structure and measurement invariance of quantitative autistic traits measured by the social responsiveness scale-2. Autism 18, 31–44 (2014).
Norris, M. & Lecavalier, L. Screening accuracy of level 2 autism spectrum disorder rating scales: A review of selected instruments. Autism 14, 263–284 (2010).
Booth, A. J., Rodgers, J. D., Volker, M. A., Lopata, C. & Thomeer, M. L. Psychometric characteristics of the DANVA-2 in high-functioning children with ASD. J. Autism Dev. Disord. 49, 4147–4158 (2019).
Gratton, G., Coles, M. G. & Donchin, E. A new method for off-line removal of ocular artifact. Electroencephalogr. Clin. Neurophysiol. 55, (1983).
Eimer, M. The face-sensitivity of the N170 component. Front. Hum. Neurosci. 5 (2011).
Hajcak, G., Weinberg, A., MacNamara, A. & Foti, D. ERPs and the study of emotion. In The Oxford Handbook of event-related Potential Components 441–472 (Oxford University Press, 2012).
Huffmeijer, R., Bakermans-Kranenburg, M. J., Alink, L. R. A. & van IJzendoorn, M. H. Reliability of event-related potentials: the influence of number of trials and electrodes. Physiol. Behav. 130, 13–22 (2014).
Moran, T. P., Jendrusina, A. A. & Moser, J. S. The psychometric properties of the late positive potential during emotion processing and regulation. Brain Res. 1516 (2013).
De Los Reyes, A., Tyrell, F., Watts, A. & Asmundson, G. Conceptual, methodological, and measurement factors that disqualify use of measurement invariance techniques to detect informant discrepancies in youth mental health assessments. Front. Psychol. 13 (2022).
Laird, R. D. & De Los Reyes, A. Testing informant discrepancies as predictors of early adolescent psychopathology: why difference scores cannot tell you what you want to know and how polynomial regression May. J. Abnorm. Child. Psychol. 41 (2013).
Laird, R. D. Analytical Challenges of Testing Hypotheses of Agreement and Discrepancy (Comment on Campione-Barr, 2020).
Acknowledgements
This work was supported by the National Institute of Mental Health (NIMH #1R01MH110585).
Author information
Authors and Affiliations
Contributions
ML, AH, TD, and IM contributed to the conceptualization and refining of research ideas. ML, KH, and TD contributed to the acquisition of the data. ML, AH, JR, KH, and TD contributed to the analysis and interpretations of data. ML, AH, JR, JG, KH, and TD contributed to the drafting and revising of the manuscript for important intellectual content. ML, AH, JR, and TD contributed to the creation of tables and figures. ML contributed to the creation of the research design and selection of measures. All authors contributed to manuscript revision, read and approved the submitted version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Houck, A.P., Richards, J.K., Day, T.C. et al. Automatic and affective processing of faces as mechanisms of passing as non-autistic in adolescence. Sci Rep 15, 22850 (2025). https://doi.org/10.1038/s41598-025-04801-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-04801-y
