
Abstract
In the second year of life, the brain undergoes rapid maturation, allowing young children to progress from relying mainly on their caregiver for comfort during distress to acquiring cognitive, motor, and emotional skills necessary for self-regulation of distress. This longitudinal, naturalistic observational study examined developmental patterns in pain-related distress responding during routine immunizations across the second year of life via cardiac and behavioural measures of pain-related distress. Respiratory Sinus Arrhythmia (RSA) and Face, Legs, Activity, Crying, and Consolability (FLACC) scores were collected at 4 epochs (Baseline, Needle, 1 min post-needle, and 2 min post-needle) during toddlers’ 12-, 18-, and 24-month vaccination visits (N = 223). No significant developmental changes in RSA were found. FLACC was most variable at 12 months. FLACC responding to pain significantly diminished with age such that toddler’s reactivity decreased, and regulatory rate exhibited a notable increase from 12 to 18 months. In 18- and 24-month-olds, pain behaviours returned to baseline levels by the third minute after vaccination, whereas in 12-month-olds, they remained elevated. These findings suggest that the second year of life marks a period of substantial development in distress regulation that mainly occurs between 12 and 18 months. With increasing age, toddlers’ initial response to an acute pain stimulus decreases while their capacity for regulation increases.
Similar content being viewed by others

Introduction
Distress regulation supports adaptability to various stressors such as acute pain1. Toddlerhood marks a critical stage in distress regulation, underpinned by synergistic and exponential development between the biological, social and psychological processes involved in emotional development2,3,4,5,6,7. In particular, the second year of life is a pivotal stage of development in which toddlers’ attachments to their caregivers shape their responses to stressors2,4,5,32,33. Thus, the second year of life is an important time to study the development of pain-related distress regulation.
Routine vaccinations in early childhood offer a unique opportunity to examine pain-related distress regulation in an ecologically valid setting. Cardiac and behavioural responses are commonly used as indices of toddler pain8,9. Respiratory Sinus Arrythmia (RSA) is a common cardiac indicator of pain-related distress and reflects heart rate variability synced with respiration rate, reflecting the parasympathetic nervous system activity10. Previous research has suggested that RSA activity during distress-inducing situations, such as pain, is influenced by an individual’s regulation abilities through top-down control processes11. Further, although cross-sectional studies have found that RSA reactivity (i.e., initial response to distress) is lower in older age groups12,13, no studies have conducted a longitudinal examination of RSA reactivity and regulation (i.e., recovery to pre-distress levels) during an acutely painful procedure across the second year of life. In addition to cardiac responding, pain behaviours have also been shown to provide a valid and reliable operationalization of distress. Multi-behavioural measures (facial expressions, body movements, and crying behaviours) have been used in young child pain contexts and shown to be sensitive to development over time and across different epochs of an acute pain paradigm (i.e. prior to pain stimulus, immediate reaction to pain stimulus, regulation of pain-related distress post-pain stimulus14,6).
Previous work has highlighted the predictive within-measure, concurrent between-measures, and predictive cross-lagged associations between toddler cardiac (heart rate and RSA) and behavioural responses during routine vaccinations15. Building on this work, the current study conducted an analysis of developmental trends in pain-related RSA and behavioural patterns separately over the second year of life. Employing both cross-sectional and predictive longitudinal analyses, this study investigated pain-related distress regulation throughout the second year of life to elucidate distinct developmental patterns. Thus, the following research questions were addressed:
-
1.
What are the mean differences in pain-related distress responses (RSA, pain behaviour) across the routine vaccination appointments (from the baseline epoch to the third minute post-needle epoch) within 12-, 18-, and 24-month old toddlers?
-
2.
How do pain-related distress response slopes (i.e. rates of change in RSA or pain behaviour over the appointment; reflecting within-appointment pain-related distress regulation) differ between 12-, 18-, and 24-month old toddlers?
We hypothesized that there would be substantial variability across epochs of the vaccination appointment within and between age groups, with younger toddlers showing greater reactivity and older toddlers demonstrating quicker recovery to baseline levels.
Methods
This research protocol was approved by the York University Research Ethics Board (ethics approval ID: 2024 −193) and all the methods were carried out in accordance with relevant guidelines and regulations.
Participants
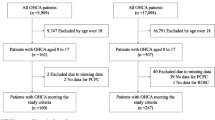
Participants consisted of healthy toddlers from a large-scale convenience sample as part of the cohort-sequential OUCH Cardio Cohort study, which has been previously examined in studies exploring emotion regulation and the dynamic interplay between autonomic and behavioral regulation3,7. Parent-toddler dyads were observed at one or more routine vaccination appointments when the child was 12, 18, and/or 24 months of age. Some toddlers were assessed at multiple time points, while others participated in only one or two. While our goal was to track toddlers’ development at each time point, attrition and scheduling challenges were the primary factors contributing to missing data, especially due to restrictions and limitations imposed by the COVID-19 pandemic. Participants were included in the analyses if they had at least one non-missing data point across time points. All parents/legal guardians provided informed consent. The full sample included 223 toddlers, 46% of whom were female. See Table 1 for a summary of participant sample size at each visit and Table 2 for demographic data of the total sample.
Procedure
Caregivers were recruited through two pediatric clinics providing early childhood vaccinations in Toronto, Ontario, Canada. Once caregivers provided written consent, they completed a demographic questionnaire prior to the vaccinations.
At 12, 18, and 24 months of age, toddlers received an average of 1.88, 1.66, 1.25 needles, respectively. All toddlers were held by a caregiver as per standard practice at the clinic and were videotaped throughout the vaccination.
Data from our behavioural and RSA outcomes of interest were collected at four 30-second epochs from prior to first needle to 3 min after the last needle, specifically: (1) “Baseline” (60–29 s prior to the first needle), (2) “Needle” (0–29 s after the last needle), (3) “Post1” (60–89 s post-needle), and (4) “Post2” (i.e., 120–149 s post-needle). By averaging responses over 30-second epochs, 1 min apart, we obtained a representative sampling of the dynamic nature of responding across a typical vaccination appointment during the second year of life.
Measures
Demographic data
A short questionnaire was completed by caregivers and included questions related to toddler age, sex, relation to toddler, caregiver education, self-reported culture, and acculturation to North American culture.
Pain-related cardiac responses
MindWare ambulatory monitors were used to collect cardiac data at a 500 Hz sampling rate. Electrocardiography (ECG) data was collected via three electrodes and was coded using MindWare HRV 3.1.5. Respiratory Sinus Arrythmia (RSA) was calculated in 30-second epochs using ECG data spectral analysis. To ensure RSA was within the bounds of young children’s natural respiration rate, 0.24 to 1.04 Hz frequency bands were used16. Intraclass correlation coefficients (ICCs) were computed by double-coding 20% of the sample to ensure high reliability of coders; ICCs ranged from 0.95 to 0.99.
Pain-related behaviour responses
The Face, Legs, Activity, Cry, Consolability (FLACC) scale17 is a well-validated measure used to code levels of behavioural distress through examination of five distinct behaviours: facial expression, leg movement, level of activity, crying, and consolability. Each of the five behaviours was scored on a scale from 0 to 2 (consolability is reverse-scored) during 15-second epochs with higher scores indicating greater distress. FLACC scores at each epoch are the sum of the five behavioural scores; thus, FLACC composite scores can range from 0 to 10 at each epoch. For the purposes of this study, and to maintain consistency with the time epochs of the RSA measure, FLACC scores were averaged across two 15-second epochs. To ensure high reliability, 20% of the sample was double-coded and ICCs ranged from 0.90 to 0.94.
Data analysis plan
We used multilevel modeling (MLM18) to describe toddler pain-related distress reactivity and regulation across their second year of life. MLM is an appropriate statistical analysis method for repeated measures due to the nested nature of the data within individuals and its capacity to incorporate participants with missing data, which is often unavoidable in longitudinal studies. We used Restricted Maximum Likelihood (REML) in our MLM analyses for several reasons. REML provides more accurate variance estimates than traditional Maximum Likelihood (ML), especially when sample sizes are smaller or data are unbalanced19,20. Since our smallest cluster (i.e., the number of participants with baseline RSA at 24 months) was 40, REML was optimal due to better variance estimates. Based on previous research, a minimum sample size of 30 individuals at level-2 is sufficient to yield reliable MLM estimates when using REML and the Kenward-Roger method, which was applied in our study21. REML also handles missing data more effectively under the assumption of missing at random (MAR), which is important for our longitudinal design where some participant dropout is expected19,20,21.
To evaluate this assumption, Little’s test of missing completely at random [MCAR22; using the12- and 18-month timepoints was non-significant (p =.095), indicating no evidence to reject the MCAR assumption. Missingness at the 24-month timepoint, where missing data were more extensive, was assessed in relation to demographic variables using logistic regression. None of the demographic variables significantly predicted missingness, supporting the MAR assumption.
MLM also provides robust significance testing by accounting for individual variability and random effects, ensuring more reliable conclusions about the effects of epoch and age group on RSA and FLACC5. We estimated the epoch effect in pain responding (i.e., Baseline to Needle, Needle to Post1, Post1 to Post2, and Baseline to Post2) within each age group and the differences in the epoch effect across age groups (i.e., comparing slope estimates).
Predictors of the MLM model included age and epoch, with random slopes for epoch, while controlling for child biological sex, caregiver education, acculturation, and total number of needles received. For research question 1, we assessed changes in RSA across epochs within each age group by using mixed-effects linear models (MLM). For research question 2, we examined age by epoch interactions to assess the differences in the epoch effect across age groups.
R statistical software (Version 4.3.3; https://www.r-project.org/) was used for all analyses with the lme4 package for model estimations23,24.
Results
Research question 1: mean differences between epochs at each age
This analysis compared pain-related distress RSA and behaviour separately across epochs for each age group. We estimated separate MLMs for RSA and behaviour to examine differences in mean RSA or behaviours across epochs within each age group.
Cardiac analyses
Descriptively, the RSA means followed a similar trend across epochs within each age group. Immediately after the needle, mean RSA increased, followed by a decrease, and then rose again (see Fig. 1). See Table 3 for the means and standard deviations of RSA across age groups and epochs.

Pain-related distress RSA across the second year of life. Each panel corresponds to different ages: 12 m = 12 months; 18 m = 18 months; 24 m = 24 months. The points represent the FLACC means at each epoch with the error bars representing one standard error of the mean.
See Table 4 for the pain-related RSA pairwise mean differences between epochs within each age group. Within the 12-month group, there was a significant change in mean RSA from Needle to Post1 (B = 0.72, p <.001). Within the 18-month group, there was a significant change in mean RSA from Needle to Post1 (B = 0.56, p =.02). Within the 24-month group, mean RSA did not significantly change across epochs. Across all age groups, mean RSA did not signficantly differ between Post1 and Post2 and between Baseline and Post2. Across age groups, the largest change in RSA was from Needle to Post1.
Behavioural analyses
Descriptively, the pain-related behaviour means followed a similar trend across epochs within each age group. Immediately after the needle, mean pain-related behaviour increased then decreased (see Fig. 2). See Table 5 for the means and standard deviations of pain-related behaviour across age groups and epochs.

Pain-related distress behaviour across the second year of life. Each panel corresponds to different ages: 12 m = 12 months; 18 m = 18 months; 24 m = 24 months. The points represent the FLACC means at each epoch with the error bars representing one standard error of the mean.
See Table 6 for the pairwise mean differences between epochs within each age group. Within the 12 m group, mean FLACC scores significantly increased by approximately 5 points from Baseline to Needle, decreased by approximately 2 points from Needle to Post1 and from Post1 to Post2. FLACC scores at 12-months also significantly differed between Baseline and Post2 by approximately 1 point, with higher Post2 scores. Within the 18 m group, there was an increase in mean FLACC scores from Baseline to Needle by approximately 3 points, a decrease from Needle to Post1 by approximately 2 points, and a decrease from Post1 to Post2 by approximately 1 point. Within the 24 m group, mean FLACC scores significantly increased from Baseline to Needle by approximately 4 points and significantly decreased from Needle to Post1 by approximately 3 points.
Research question 2: age differences in mean slope differences
This analysis examined how mean changes in pain-related RSA and behaviours varied across age groups. To do so, we tested age by epoch interactions for RSA and pain behaviours separately.
Cardiac analyses
There were no significant age by epoch interactions in RSA outcome (see Table 7 for slope difference estimates).
Behavioural analyses
There were several significant age by epoch interactions for the FLACC outcome (see Table 8 for slope difference estimates). Specifically, the increase in pain-related distress behaviours from Baseline to Needle was significantly greater at 12 months than at 18 months and 24-months with a 2- and 1-point difference in FLACC score changes, respectively. At 18-months, there was a significantly smaller decrease from Post1 to Post2 compared to 12-months with approximately a 1-point difference in FLACC score changes. In addition, the difference bewteen Baseline and Post2 was significantly smaller at 18 months than at 12 months with approximately a 1-point difference in FLACC score changes.
Discussion
The first two years of life is a critical period in which myelination, an index of structural brain maturity, is most pronounced and parallels notable development in the emerging ability to self-regulate from distress25. This study is the first to examine changes in cardiac and behavioural responses during a highly distressing situation at three ages across the second year of life: 12, 18, and 24 months. In line with previous literature, we hypothesized that recovery from a vaccine needle poke would reflect lessening reactivity and quicker regulation at older ages, consistent with what is known about brain development in early life3,26. Overall, supporting our hypotheses, there was greater reactivity from 30-seconds prior to the application of the acute stressor (i.e., needle) to 3 min after the acute stressor with the youngest group. Generally, 12-month olds demonstrated a higher initial response to the stressor and less recovery post-stressor. This pattern was more pronounced with behaviour than with cardiac responding, as we discuss below.
At each age, RSA followed a similar descriptive pattern—it intially increased at needle, decreased after the needle, and then increased to pre-needle levels by the third minute post-needle. In our study, RSA withdrawal is demonstrated at one minute post-needle, suggesting a slightly delayed expected response in toddlers’ cardiac pain-related distress responding. While RSA has typically followed a withdrawal pattern at the time of peak distress27, interval lengths used for RSA has been varied in the literature28. The pattern of responding could be reflective of ‘orienting bradycardia’ at the immediate time of the needle, a response pattern commonly observed across species faced with a novel situation29. Specifically, the initial temporary increase in RSA could reflect the toddlers’ attentional shift to the novel or uncertain situation, which is then followed immediately by vagal withdrawal after the needle pierces the skin that may reflect the pain perception and subsequent top-down regulatory process.
Across ages, the largest mean difference occurred between Needle and the Post1 epoch, in which RSA drops the most from its previous epoch. RSA responding throughout the vaccination appointment showed the most variable mean differences at 12-months compared to 18- and 24-months, with the largest mean differences occurring in the first two epoch changes (Baseline to Needle and Needle to Post1). When the analysis moved from mean differences between epochs at each age to comparing the RSA mean differences across the ages, there were no significant differences in RSA change between ages. Put together, these results indicate that despite the varying mean differences in RSA in our cross-sectional analyses at each age, the longitidunal analyses demonstrated that the absolute differences between epochs were not significantly different across the age groups.
While acknowledged as a physiological index of regulation, the stability of RSA in toddlers has been questioned as RSA reactivity continues to develop into adolescence30,15. Further, according to the Polyvagal Theory10, RSA responding can be considered a peripheral measure of emotion regulation because of its non-specific nature. Therefore, RSA variability may not only reflect individual differences in regulatory capacities but also variations in emotional reactivity and regulation processes. These findings highlight the complexity of RSA as a physiological index of pain regulation and its intricate associations with physiological and emotional regulation.
The most pronounced differences in pain-related distress behaviours during the vaccination appointment at each age occurred between Baseline to Needle. Specifically, 12-month-olds exhibited a 5-point increase, while 18- and 24-month-olds exhibited increases of 3 and 4 points, respecitvely. Toddlers in the 12-month group showed the slowest recovery, with a 1-point difference that remained between their pre-needle and third minute post-needle pain-related distress behaviours. Conversely, pain-related distress behaviours recovered to pre-needle levels by the third minute at 18-months and by the second minute at 24-months, suggesting better developed regulatory capacities with increasing age.
When the analysis moved from mean differences in pain-related distress behaviours between epochs at each age to comparing the differences across different ages, there were several significant changes between ages in line with our cross-sectional findings. Specifically, 18- and 24-month-olds showed smaller increases in behavioural pain-related distress from Baseline to Needle compared to 12-month olds. Additionally, 12-month-olds showed a greater increase in pain-related distress behaviours from Post1 to Post2 compared to 18-month olds, reflecting the developmental differences in regulatory needs. At 18 months, the difference in mean pain behaviour from Baseline to Post2 was significantly smaller than that observed in the 12-month-old group, which still exhibited a significant difference. Put together, our behavioural pain-related distress findings demonstrate a clear developmental progression in regulatory abilities: at 12 months, Baseline levels are not yet reached by Post2; by 18 months, Baseline levels are reached by Post2. These findings illustrate that the rate of recovery increases in older toddlers and suggest that toddlers become better able to regulate their pain experience as their brain develops and they gain regulatory skills throughout toddlerhood. In addition to these developmental changes, increased familiarity with the vaccination context across timepoints may contribute to shifts in response patterns, as reduced novelty and improved anticipatory coping could influence regulation. These results support our hypothesis about less reactivity and increased regulation of behavioural pain-related distress as age increases. Overall, our study suggests that the onset of behavioral expressions of pain occurs more rapidly than autonomic responding in toddlers, reflecting the complex physiological processing involved in autonomic regulation, which may create a buffering period for cardiac responses to catch up to behavioral expressions of pain.
Although this study provides valuable insights into developmental trends in acute pain responding across the second year of life, the sample consisted of toddlers from higher socioeconomic backgrounds, as reflected by caregivers’ education levels. Thus, generalizability of the study is limited because socioeconomic disadvantage is associated with altered brain development and, consequently, altered regulatory abilities31.
As would be expected in a longitudinal study on vaccination pain, vaccines administered differed across ages and sites. However, all were adminsitered via the same mode and are thought to be a painful stimulus. Relatedly, our baseline measure was collected at the end of a pediatric check-up appointment, in which the toddler was handled by the doctor (measurement, weighing, etc.) in a strange environment. Thus, we may not be capturing a true cardiac baseline, which may impact the observed patterns of cardiac responding, albeit consistently across participants.
Another limitation in this study included our diminishing sample size with each age group, particularly the 24-month-old group. Due to the COVID-19 pandemic, recruitment was ulitmately halted, resulting in a much smaller sample size in the 24-month group. Future studies may seek to describe variability in responding by identifying groups with similar patterns across epochs, as was done in Waxman et al.15. Waxman and colleagues15 described distinct classes of responding based on concurrent and predictive relations of cardiac and behavioural measures of pain using the same 12- and 18-month old toddlers in this study and similar epochs throughout the vaccination context. This finding was not surprising given the influence of children’s social context in their pain experience (e.g., attachment) as well as other more proximal factors (e.g., temperament). Thus, future studies may seek to identify distinct pain-related distress-responding groups and observe those groups across development to learn about specific developmental trends and the influence of various factors in pain-related distress responding. Moreover, future research should aim to comprehensively assess pain-related distress using multiple modes of measurements, as they offer unique insights and may capture distinct facets of distress that develop at different timescales.
In summary, we uncovered important nuances in understanding in the development of cardiac and behavioural responses to noxious stimuli over the second year of life. RSA responding demonstrated unique patterns across the vaccination context within each age group. However, there were no significant age-related differences in RSA responding. In contrast, our behavioural indicators of pain-related distress revealed distinct age-related reactivity and regulation patterns over the appointment. In addition to significant changes in pain-related distress across the vaccination appointment, we also found that older toddlers regulated the quickest, commensurate with their rapidly developing brain. Evidence suggests a developmental shift in pain regulation sometime between 12 and 18 months of age.
Data availability
The data used for the current study are available from the corresponding author upon reasonable request.
References
Kopp, C. B. Regulation of distress and negative emotions: A developmental view. Dev. Psychol. 25 (3), 343–354. https://doi.org/10.1037/0012-1649.25.3.343 (1989).
Ainsworth, M. D. S. Patterns of Attachment: A Psychological Study of the Strange Situation (Lawrence Erlbaum Associates, 1978).
Gennis, H. G. et al. Understanding the concurrent and predictive relations between child-led emotion regulation behaviors and pain during vaccination in toddlerhood. Pain 164(6), 1291–1302 (2023).
Horton, R. E., Riddell, R. P., Flora, D., Moran, G. & Pederson, D. Distress regulation in infancy: attachment and temperament in the context of acute pain. J. Dev. Behav. Pediatr. 36 (1), 35–44 (2015).
Perry, N. B., Calkins, S. D., Hollenstein, T., & Cole, P. M. A biopsychosocial perspective on the development of emotion regulation across childhood. In: Emotion Regulation. (1st ed.) 3–30. (Routledge, 2018).
Pillai Riddell, R., Racine, N., Craig, K. D. & Campbell, L. Psychological theories and biopsychosocial models in paediatric pain. Oxf. Textbook Pediatr. Pain (1st ed.) 85–94 (2013).
Sroufe, L. A. & Hoffman, M. L. The growth of self-regulation. In: Emotional Development: the Organization of Emotional Life in the Early Years. Cambridge Studies in Social and Emotional Development. 214–234. (Cambridge University Press, 1996).
Campbell-Yeo, M., Eriksson, M. & Benoit, B. Assessment and management of pain in preterm infants: A practice update. Child 9 (2), 244 (2022).
Hatfield, L. A. & Ely, E. A. Measurement of acute pain in infants: A review of behavioral and physiological variables. Biol. Res. Nurs. 17 (1), 100–111 (2015).
Porges, S. W. The polyvagal perspective. Biol. Psychol. 74 (2), 116–143 (2007).
Shader, T. M. et al. Quantifying respiratory sinus arrhythmia: effects of misspecifying breathing frequencies across development. Dev. Psychopathol. 30 (1), 351–366 (2018).
Alkon, A. et al. Developmental and contextual influences on autonomic reactivity in young children. Dev. Psychobiol. 42 (1), 64–78 (2003).
El-Sheikh, M. Stability of respiratory sinus arrhythmia in children and young adolescents: A longitudinal examination. Dev. Psychobiol. 46 (1), 66–74 (2005).
Gennis, H. G. et al. Child distress expression and regulation behaviors: A systematic review and Meta-Analysis. Child 9 (2), 174 (2022).
Waxman, J. A. et al. An examination of the reciprocal and concurrent relations between behavioral and cardiac indicators of acute pain in toddlerhood. Pain 161 (7), 1518–1531 (2020).
Huffman, L. C. et al. Infant temperament and cardiac vagal tone: assessments at twelve weeks of age. Child Dev. 69 (3), 624–635 (1998).
Merkel, S. I., Voepel-Lewis, T., Shayevitz, J. R. & Malviya, S. The FLACC: a behavioral scale for scoring postoperative pain in young children. Pediatr. Nurs. 23 (3), 293–297 (1997).
Bryk, A. S. & Raudenbush, S. W. Hierarchical Linear Models: Applications and Data Analysis Methods (Sage Publications, Inc, 1992).
McNeish, D. M. & Stapleton, L. M. The effect of small sample size on two-level model estimates: A review and illustration. Educational Psychol. Rev. 28, 295–314 (2016).
Peugh, J. L. A practical guide to multilevel modeling. J. Sch. Psychol. 48 (1), 85–112 (2010).
Snijders, T. A. & Bosker, R. Multilevel analysis: An introduction to basic and advanced multilevel modeling.
Little, R. J. A. A test of missing completely at random for multivariate data with missing values. J. Am. Stat. Association [Internet]. 83 (404), 1198–1202 (1988).
Bates, D., Maechler, M., Bolker, B. & Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 67 (1), 1–48 (2015).
R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. (2023). https://www.R-project.org/
Dubois, J. et al. The early development of brain white matter: A review of imaging studies in fetuses, newborns and infants. Neuroscience 276, 48–71 (2014).
Johnson, M. H. Functional brain development in humans. Nat. Rev. Neurosci. 2 (7), 475–483 (2001).
Oberlander, T. F., Grunau, R. E., Fitzgerald, C. & Whitfield, M. F. Does parenchymal brain injury affect biobehavioral pain responses in very low birth weight infants at 32 weeks’ postconceptional age? Pediatrics 110 (3), 570–576 (2002).
Cong, X., Ludington-Hoe, S. M., McCain, G. & Fu, P. Kangaroo care modifies preterm infant heart rate variability in response to heel stick pain: pilot study. Early Hum. Dev. 85 (9), 561–567 (2009).
Sokolov, E. N. & Cacioppo, J. T. Orienting and defense reflexes: vector coding the cardiac response. In Attention and Orienting. Apr 15 (2–22). (Psychology Press, 2013).
Dollar, J. M. et al. Developmental patterns of respiratory sinus arrhythmia from toddlerhood to adolescence. Dev. Psychol. 56 (4), 783–794 (2020).
Noble, K. G. et al. Family income, parental education and brain structure in children and adolescents. Nat. Neurosci. 18 (5), 773–778 (2015).
Pillai Riddell, R. et al. The relationship between caregiver sensitivity and infant pain behaviors across the first year of life. Pain 152 (12), 2819–2826 (2011).
Pillai Riddell, R., Jasim, S. & Hamwi, L. Out of the mouth of babes: a lot about pain has nothing to do with pain. Pain 163 (S1), S117–S125 (2022).
Author information
Authors and Affiliations
Contributions
S.J.: conceptualization, investigation, analysis, writing—main manuscript text. D.B.F.: analysis support, writing – review and edits. D.F., E.W., D.S., and H.G.: recruitment, reviewed manuscript. R.P.R.: conceptualization, investigation, supervision, writing—review and edits.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jasim, S., Flora, D.B., Flanders, D. et al. Cardiac and behavioural trends in toddler pain distress responses across early development. Sci Rep 15, 22015 (2025). https://doi.org/10.1038/s41598-025-05421-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-05421-2
