
Abstract
Neglected Tropical Diseases (NTDs) and malaria, as tropical diseases, have long been major global public health challenges, particularly in low-income countries. Although the burden of NTDs and malaria has declined in recent years, significant health inequalities persist across regions. In the future, climate change may further exacerbate the burden of NTDs and malaria, with these burdens likely to disproportionately concentrate in low-income countries. This study aims to describe the global trends in the burden of NTDs and malaria, reveal health inequalities, and forecast future disease burdens. This study utilizes the latest data from the Global Burden of Disease Study (GBD) 2021 to assess the global trends and spatial distribution of NTDs and malaria burden from 1990 to 2021. Inequality analyses and frontier analysis were employed to evaluate disparities in disease burden and governance potential across countries, and the interactive effects between environmental risks and socio-economic factors on the burden of NTDs and malaria were explored in depth. Furthermore, the Bayes Age-Prior-Cohort model was used to forecast changes in disease burden from 2022 to 2041. From 1990 to 2021, the age-standardized DALY rate for NTDs and malaria declined from 1506.54 to 1020.27 per 100,000. Western Sub-Saharan Africa remains the most affected, contributing 51.18% of the global burden. Males have lower incidence but higher mortality rates compared to females. Despite improvements in global inequality, regional disparities persist. Environmental and socio-economic factors interact significantly, exacerbating the burden in vulnerable regions. The NTDs and malaria burden is projected to increase over the next 20 years, particularly in Middle and Low-middle Socio-Demographic Index (SDI) regions. Despite a global decline in the burden of NTDs and malaria, low-income countries, particularly in Western Sub-Saharan Africa, continue to experience significant health inequalities. Global climate change may exacerbate this burden, and these burdens will be disproportionately concentrated in tropical, poverty-stricken countries.
Similar content being viewed by others

Background
Neglected tropical diseases (NTDs) are a group of diverse diseases caused by a variety of pathogens, including viruses, bacteria, parasites, fungi, and toxins1. Over 1·6 billion people worldwide are affected by NTDs, including more than 500 million children, contributing significantly to the global health burden2. In 2012, the World Health Organization (WHO) launched its first NTDs roadmap (2012–2020), outlining a comprehensive plan to control, eliminate, and eradicate 17 NTDs3. By 2020, although substantial progress had been made in addressing NTDs, many targets remained unmet4. In response, WHO introduced a new roadmap for 2021–2030, which includes strategies for 20 diseases and disease groups5. This new roadmap shifts away from the previous single-disease control model, embracing an integrated and multi-sectoral action framework that reflects the long-term and complex nature of NTD governance.
Malaria is a deadly disease caused by parasites and transmitted through mosquito bites. Although it is preventable and treatable, its control faces significant challenges due to the high variability and adaptability of the malaria parasite6. Several studies have reported that some strains of Plasmodium have developed resistance to antimalarial drugs, particularly in Southeast Asia7,8,9. According to the World Health Organization’s World Malaria Report 2023, global malaria cases reached 249 million in 2022, an increase of 5 million compared to 2021, with an estimated 608,000 deaths10. In response, the World Health Organization updated its Global Technical Strategy for Malaria 2016–2030 in 2021, summarizing lessons from the past five years, refining strategies to address malaria’s complexity, and stressing the urgent need to focus on its control challenges11.
While NTDs and malaria are classified as distinct diseases, they share key similarities in epidemiological research. Both are closely tied to environmental factors, are endemic in tropical and subtropical regions, and are transmitted by vectors such as mosquitoes and parasites. This common transmission mechanism and ecological connection result in overlapping strategies for disease control12. Furthermore, the burden of both NTDs and malaria is particularly severe in low- and middle-income countries, especially among the most impoverished populations. As global temperatures rise, the expected burden of NTDs and malaria is likely to increase. This burden is anticipated to disproportionately impact the poorest regions, exacerbating health inequalities13.
This study utilizes the latest data from GBD 2021 to systematically analyze the temporal trends and spatial distribution of NTDs and malaria burden at global, regional, and national levels, uncovering health inequalities and evaluating governance potential at the national level. It also predicts the changes in NTDs and malaria burden over the next 20 years. The study aims to provide the latest and most comprehensive global evidence, offering targeted public health strategies and recommendations for reducing the burden of NTDs and malaria, ultimately promoting global health equity.
Methods
Data source
The data for this study were entirely sourced from the latest findings of GBD 2021. The data were downloaded from the GBD Results Tool on the Global Health Data Exchange (GHDx) platform (http://ghdx.healthdata.org/gbd-results-tool).
GBD 2021 systematically assessed the disease burden of 371 diseases and injuries, as well as 88 attributable risk factors, across 204 countries and regions from 1990 to 2021. It also classified countries and regions into five SDI categories based on the Socio-Demographic Index (SDI) levels: Low SDI (0–0·47), Low-middle SDI (0·47−0·62), Middle SDI (0·62−0·71), High-middle SDI (0·71−0·81), and High SDI (0·81−1)14. Furthermore, GBD collected a range of covariates, including socioeconomic, demographic, health system, and climate data from governments and international organizations15.
This study selected data on the incidence, mortality, and Disability-Adjusted Life Years (DALYs) related to NTDs and malaria from GBD for analysis, along with environmental covariates that may be associated with NTDs and malaria. The specific covariates are listed in Annexed table 1. All rates in GBD are expressed per 100,000 population, and this study adopts the same standard.
This study has thoroughly reviewed and agreed to the GBD data usage agreement. Since the GBD database is publicly available and this study does not involve personal privacy or sensitive information, it is exempt from ethical review.
Data inclusion and exclusion criteria
Data inclusion criteria
Diseases classified as NTDs and malaria in the GBD 2021 framework, including but not limited to dengue, malaria, lymphatic filariasis, and schistosomiasis.
Data covering the period from 1990 to 2021 across 204 countries and territories, including indicators such as incidence, mortality, and DALYs.
The SDI and environmental covariates from the GBD 2021 study that are not directly modifiable by human intervention, such as population-weighted average temperature, absolute latitude, and other natural environmental factors.
Data exclusion criteria
Diseases not classified as NTDs or malaria in the GBD 2021 framework.
Countries or territories with missing or incomplete data for key indicators during the study period.
Socioeconomic covariates from the GBD 2021 study that are directly modifiable by human intervention, excluding SDI, such as per capita disposable income and health spending indices.
Case definition
Neglected tropical diseases and malaria (NTDs and malaria)
This category estimates burden from Chagas, cutaneous and visceral leishmaniasis, cystic echinococcosis, cysticercosis, dengue, Ebola, food-borne trematodes, Guinea worm disease, leprosy, human African trypanosomiasis, malaria, lymphatic filariasis, onchocerciasis, rabies, schistosomiasis, soil-transmitted helminths, trachoma, yellow fever, Zika, and other NTDs16.
Natural Environment Index(NEI)
The NEI is a composite indicator that quantifies the impact of natural environmental factors on the burden of NTDs and malaria. It integrates key environmental variables, such as temperature, rainfall, and elevation, to account for environmental heterogeneity, ensuring fairer and more accurate comparisons of disease burden across regions.
Socio-Demographic Index(SDI)
The SDI is a geometric mean ranging between 0 and 1, calculated using three indicators: total fertility rate under the age of 25, mean years of education for those aged 15 and older, and lag-distributed income per capita. A higher SDI score indicates a higher level of social development14.
Statistical analysis
Analysis of differences in disease burden composition
Percentage stacked bar charts and absolute value bar charts were used to analyze the differences in the disease composition of the Age-Standardized DALYs Rate across different SDI regions. This analysis revealed the main sources of the burden of NTDs and malaria in each region and compared the burden levels across regions. Additionally, time series ranking charts were used to analyze the dynamic changes in the major causes of disease burden from 1990 to 2021, providing a comprehensive view of regional differences in disease distribution and their temporal trends.
Analysis of regional, age, and gender differences in distributions and trends
This study analyzed the disease burden of NTDs and malaria using multiple approaches. By calculating the Estimated Annual Percentage Change (EAPC) of the Age-Standardized Incidence Rate (ASIR), Age-Standardized Mortality Rate (ASMR), and Age-Standardized Disability-Adjusted Life Years Rate (ASDR) from 1990 to 2021, it evaluated the trends in disease burden changes across regions and different SDI levels. A population pyramid-style bar chart was constructed to reveal differences in disease burden between genders and age groups. Additionally, based on data from 204 countries and regions, global disease distribution maps and burden change rate maps were generated to comprehensively assess the disease burden and its trends across countries and regions.
Inequality analyses
The Slope Index of Inequality (SII) and Concentration Index (CI) were used to assess the absolute and relative inequalities in the burden of NTDs and malaria associated with SDI across countries17. SII is an absolute measure of health inequality, calculated through a regression model, reflecting the linear relationship between disease burden and socioeconomic status. CI is a relative measure, calculated by plotting the Lorenz curve, reflecting the distribution of disease burden in relation to socioeconomic status. The study also employed the Locally Estimated Scatterplot Smoothing (LOESS) method to reveal the non-linear trend of disease burden changes with SDI.
Additionally, annual SII and CI values from 1990 to 2021 were calculated, and their rates of change were computed to visually compare the trends in absolute and relative inequalities in the burden of NTDs and malaria over this period. This approach highlights the dynamic nature of health inequality over time.
Natural environment index construction
Considering that NTDs and malaria are strongly tied to natural environmental factors like temperature and humidity, relying solely on SDI to assess their impact falls short. To more effectively examine how environmental factors and SDI together influence NTDs and malaria, we made several essential adjustments.
Using 2021 GBD data, we gathered 15 environmental covariates—such as the proportion of coastal areas, population distributions by elevation and latitude, and population-weighted rainfall and temperature measures—with details outlined in Appendix Table 1. After organizing the data, we treated ASDR high-low groupings as the dependent variable and the environmental covariates as independent variables. We then applied Binomial Lasso regression to filter variables, tackle potential multicollinearity, and pinpoint key factors linked to NTDs and malaria ASDR. Based on the Lasso regression results, we built a Logistic regression model to evaluate the independent effects of these natural environmental factors on the disease burden. The Natural Environment Index (NEI) was derived from Logistic model as an indicator of the natural environment’s potential impact on disease burden. Next, using NEI as a predictor and ASDR groupings as the outcome, we plotted an ROC curve, calculated the AUC and cutoff value, and used the cutoff to classify countries into high- and low-NEI-risk groups, setting the stage for further analysis.
Impact of NEI, SDI, and Their Interaction on NTDs and malaria
The study further analyzed the impact of NEI and SDI on NTDs and malaria ASDR using LOESS regression and Spearman’s correlation coefficient. The Generalized Additive Model (GAM) was employed to explore the interaction between NEI and SDI. The Restricted Cubic Spline (RCS) plot was used to demonstrate the sensitivity of NTDs and malaria ASDR to SDI across different NEI regions. This approach aims to uncover the combined effects of NEI and SDI on NTDs and malaria.
Frontier analysis
Frontier Analysis utilized GBD data to generate 500 bootstrap samples and calculate the average NTDs and malaria ASDR for each SDI value. The Free Disposal Hull method was used for Data Envelopment Analysis to construct a nonlinear frontier model. Local Polynomial Regression was applied to smooth the frontier, generating a stable boundary. To minimize the impact of outliers, countries with super-efficiency were excluded. The difference between the actual ASDR and the minimum ASDR at the same SDI level was calculated to assess each country’s and region’s disease burden management levels and untapped health potential.
Considering the environmental traits of NTDs and malaria, using only SDI for frontier analysis doesn’t fully capture the true state of disease control across countries. Thus, building on the previously established NEI risk groups, we performed separate frontier analyses for each group, allowing for a more precise evaluation of disease burden performance across varying environmental conditions.
Bayes age-period-cohort (BAPC)
The BAPC model is a statistical tool used to evaluate and predict events over time. This study employs the BAPC and INLA packages in R to predict DALYs for NTDs and malaria, based on existing disease burden data from 1990 to 2021 and predicted population data for 2022 to 204118, constructing the BAPC model. The model assumes that DALYs follow a Poisson distribution, using RW1 smoothing, with the precision prior for random effects set as log(τ)∼Gamma(1,0.00001). The prediction is configured with a 5-year interval, forecasting the trend of NTDs and malaria DALYs changes from 2022 to 2041. The research process is shown in Fig. 1.

Analytical Flowchart. Map generated using the “sf” package (version 1.0.2) in R (version 4.4.1). See https://cran.r-project.org/package=sf for more information.
Results
Regional and temporal differences in disease composition
Between 1990 and 2021, the rankings of NTDs and malaria ASDR causes changed significantly. Malaria consistently ranked first, while conditions such as intestinal nematodes and leishmaniasis saw a marked decline in rankings. Conversely, diseases like schistosomiasis, dengue, cysticercosis, and other NTDs showed significant upward trends in their rankings19as shown in Fig. 2A.
An analysis of disease etiology across different SDI regions reveals that malaria dominates the disease burden in Low, Low-middle, and Middle SDI regions, accounting for over half of the burden in the Low and Low-middle SDI regions. In contrast, in High and High-middle SDI regions, the malaria burden is almost negligible, with cysticercosis, food-borne trematodiases, and other NTDs becoming the primary contributors, as shown in Fig. 2B. A stark disparity exists in absolute DALYs burden across SDI levels, with higher SDI regions showing significantly lower burdens than lower SDI regions, as shown in Fig. 2C.

shows the rankings and distribution of the composition of NTDs and malaria ASDR globally and across different SDI regions in 1990 and 2021. Panel A displays the global rankings of the causes of NTDs and malaria ASDR in 1990 and 2021; Panel B illustrates the percentage composition of the causes of NTDs and malaria ASDR in 2021 across different SDI regions; Panel C shows the absolute distribution of the causes of NTDs and malaria ASDR in 2021 across different SDI regions.
The distribution and trends of NTDs and malaria burden across regions
From 1990 to 2021, the global ASIR for NTDs and malaria showed minimal change, increasing slightly from 4235·42 per 100,000 in 1990 to 4259·54 per 100,000 in 2021 (EAPC = -0·11%, P = 0·13). However, the ASMR declined significantly, dropping from 16·29 per 100,000 to 11·80 per 100,000 (EAPC = -1·49%, P < 0·0001). Similarly, the ASDR decreased from 1506·54 per 100,000 to 1020·27 per 100,000 (EAPC = -1·66%, P < 0·0001), as shown in Fig. 3. It is worth noting that, despite declines in both ASMR and ASDR, as of 2021, NTDs and malaria still claim 2322 lives daily worldwide.

The ASIR, ASMR, and ASDR of NTDs and malaria, as well as their trends of change, in 1990 and 2021 globally, across the five SDI regions, and in the 21 GBD regions.
During this period, the ASMR and ASDR of NTDs and malaria showed a declining trend across different SDI regions. The ASIR in Low SDI and Low-middle SDI regions showed a clear decreasing trend, whereas in Middle SDI, High-middle SDI, and High SDI regions, the ASIR exhibited a significant increasing trend. Nevertheless, due to the lower baseline prevalence in high SDI regions, there remains a significant gap in the NTDs and malaria burden between low SDI and high SDI regions, As shown in Fig. 4A.
In the analysis of 21 GBD regions, the ASIR of NTDs and malaria showed a downward trend in most regions, with only Australia, Central Latin America, High-income Asia Pacific, High-income North America, and Tropical Latin America showing an upward trend. Meanwhile, ASMR and ASDR showed a declining trend in all regions except High-income North America. Notably, although ASIR, ASMR, and ASDR in African regions have generally decreased, these areas remain the most burdened globally by NTDs and malaria, with incidence rates, mortality rates, and DALY rates ranking among the highest in the world, especially in Western Sub-Saharan Africa, as shown in Fig. 3.
In the analysis of 204 countries and regions, we observed consistent trends in the distribution of ASIR, ASMR, and ASDR for NTDs and malaria, with a notable concentration in Africa, particularly in Western Sub-Saharan Africa, as shown in Fig. 4B–D. In 2021, the countries with the highest ASIR for NTDs and malaria were Liberia, Benin, Solomon Islands, Burkina Faso, Sierra Leone, Guinea, Nigeria, Central African Republic, Mozambique, and the Democratic Republic of the Congo. The countries with the highest ASMR were Burkina Faso, Sierra Leone, Niger, Liberia, Benin, Côte d’Ivoire, Cameroon, Mozambique, Nigeria, and Central African Republic. The top ten countries with the highest ASDR were Sierra Leone, Burkina Faso, Liberia, Niger, Benin, Central African Republic, Nigeria, Côte d’Ivoire, South Sudan, and Burundi, see Annexed Table 2. All of these countries, except for Solomon Islands, are located in Africa.
Additionally, based on the calculated EAPC from 1990 to 2021, the countries where the ASDR for NTDs and malaria has been increasing include Monaco (EAPC = 2·20%), Tonga (EAPC = 1·89%), Syrian Arab Republic (EAPC = 1·21%), Singapore (EAPC = 0·98%), United States of America (EAPC = 0·50%), Georgia (EAPC = 0·42%), Ukraine (EAPC = 0·18%), and Zimbabwe (EAPC = 0·12%). The countries with the fastest declines in ASDR are Bhutan (EAPC = -12·18%), Vanuatu (EAPC = -7·81%), and Timor-Leste (EAPC = -6·89%), as shown in Fig. 4E.

Illustrates the current status and trends of the NTDs and malaria burden across different SDI regions and 204 countries and regions globally. Panel A shows the trends in ASIR, ASMR, and ASDR from 1990 to 2021 across different SDI regions. Panel B shows the distribution of NTDs and malaria ASIR in 2021 across the 204 countries and regions; Panel C displays the distribution of NTDs and malaria ASMR in 2021; Panel D presents the distribution of NTDs and malaria ASDR in 2021; Panel E depicts the changes in NTDs and malaria ASDR from 1990 to 2021 across the 204 countries and regions. Map generated using the “sf” package (version 1.0.2) in R (version 4.4.1). See https://cran.r-project.org/package=sf for more information.
The distribution and trends of NTDs and malaria burden across genders and age groups
In the distribution of NTDs and malaria across different genders and age groups, we found that although women have higher incidence rates than men in almost all age groups, men experience higher mortality rates and DALY rates across all age groups. Additionally, the incidence and mortality of NTDs and malaria are predominantly concentrated in the < 5 age group, as shown in Fig. 5.

The distribution of incidence rates, mortality rates, and DALYs rates of NTDs and malaria across different sexes and age groups in 2021.
Inequality analyses
The results of the Inequality Analyses show that the SII for NTDs and malaria decreased significantly from 4625·35 in 1990 to 1053·00 in 2021 (Fig. 6A), and the inequality intercept declined from 12,079·00 to 5954·00 (Fig. 6B), indicating a substantial narrowing of the disease burden gap between the highest and lowest SDI regions. In terms of relative inequality, the CI index slightly increased from 0·71 in 1990 to 0·73 in 2021 (Fig. 6C), reflecting that the burden inequality driven by SDI remains significant. From 1990 to 2021, the SII consistently declined, with an average annual decrease of 111·61 (Fig. 6D), further confirming the trend of decreasing absolute inequality. However, the CI index did not show a significant upward or downward trend during this period, remaining stable around 0·70 (Fig. 6E), indicating that the severity of relative inequality in the burden of NTDs and malaria persisted over the 31-year period.

The analysis results and trends of global NTDs and malaria burden inequality from 1990 to 2021. Panel A SII analysis of global NTDs and malaria burden inequality in 1990 and 2021; Panel B LOESS regression of global NTDs and malaria burden inequality in 1990 and 2021; Panel C Lorenz curve of global NTDs and malaria burden inequality in 1990 and 2021; Panel D Trend of SII changes from 1990 to 2021; Panel E Trend of CI changes from 1990 to 2021.
Natural Environment Index (NEI) construction
Using the NTDs and malaria ASDR risk groups (based on median split) as the dependent variable and 15 natural environmental variables as independent variables, Lasso regression was performed for variable selection. After diagnosing and removing collinear variables, five variables were retained: the proportion of a country’s coastal area, the proportion of the population living below 100 m and above 1500 m, the proportion of the population living at absolute latitudes of 30–40, and the absolute latitude of the country’s center. A Logistic regression model was then constructed based on these variables, identifying the coastal area proportion and the absolute latitude of the country’s center as independent factors associated with ASDR, as shown in Annexed Fig. 1A-D.
Based on this model, the NEI was calculated to reflect the environmental impact on disease burden, with NEI scores for each region shown in Annexed Fig. 1E. An ROC curve was plotted using NEI to classify ASDR risk groups (AUC = 0.943, cutoff value = 0.484), and, based on the cutoff value obtained from the ROC curve, the NEI was divided into high- and low-risk groups. High NEI risk areas were concentrated near the equator, including regions in Africa, northern South America, Southeast Asia, and island nations in Oceania, as shown in Annexed Fig. 1F and G.
Impact of NEI, SDI, and their Interaction on NTDs and malaria
LOESS regression shows that both NEI and SDI have a significant impact on the burden of NTDs and malaria, with Spearman correlation coefficients of 0.843 and − 0.892, respectively, and both exhibit a nonlinear trend. High NEI and Low SDI are more sensitive to the burden of NTDs and malaria, whereas Low NEI and High SDI regions show lower sensitivity. The Interaction Partial Dependence heatmap and 3D plot further reveal that the sensitivity of NTDs and malaria burden to NEI varies across different SDI regions, with low SDI regions being significantly more sensitive to NEI than high SDI regions, as shown in Annexed Fig. 2A-D.
The RCS analysis shows that the sensitivity of NTDs and malaria burden to SDI also varies across different NEI regions, with high NEI regions being significantly more sensitive to SDI than low NEI regions. The Generalized Additive Model based on the Gamma distribution was used to analyze the effects of NEI, SDI, and their interaction on the burden of NTDs and malaria. The main effects of NEI (edf = 1·000, F = 46·024, P < 0·001) and SDI (edf = 4·283, F = 11·428, P < 0·001) were statistically significant. Additionally, the interaction between NEI and SDI was also significant (edf = 6·152, F = 3·181, P = 0·003), indicating that their synergistic effect plays an important role in the burden distribution, see Annexed Fig. 2E and F.
Frontier analysis
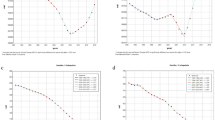
The frontier analysis results show that, from 1990 to 2021, countries made overall positive progress in the management of NTDs and malaria burden. Most countries gradually approached the optimal frontier boundary during this period, as shown in Fig. 7A and C.
As shown in Fig. 7B, the frontier analysis of High NEI risk areas is as follows: In Low SDI regions, Somalia, Afghanistan, and Timor-Leste are the countries with the best burden management, while Sierra Leone, Burkina Faso, and Liberia have the greatest governance potential. In Low-middle SDI regions, Cambodia, Tuvalu, and Belize are the countries with the best governance, while Nigeria, Cameroon, and Congo have the greatest governance potential. In Middle SDI regions, Nauru, Tokelau, and Iran have the best governance, while Equatorial Guinea, Gabon, and Guyana have the greatest governance potential. In High-middle SDI regions, Oman, Trinidad and Tobago are the countries with the best governance, while Malaysia and Seychelles have the greatest governance potential. Additionally, the country with the best governance performance in the High SDI region is Brunei Darussalam, while the country with the greatest governance potential is Singapore., see Annexed Table 3.
As shown in Fig. 7D, the frontier analysis of Low NEI risk areas is as follows: Compared to High NEI regions, there are no Low SDI countries in Low NEI risk areas. In Low-middle SDI regions, the countries with the best burden management are Democratic People’s Republic of Korea, Morocco, and Kyrgyzstan, while the countries with the greatest governance potential are Cabo Verde, Vanuatu, and Egypt. In Middle SDI regions, the countries and regions with the best burden management are Palestine, Albania, and Azerbaijan, while the countries with the greatest governance potential are the Syrian Arab Republic, Fiji, and Tonga. In High-middle SDI regions, Italy, Malta, and Bahrain are the countries with the best burden management, while the countries with the greatest governance potential are Mauritius, American Samoa, and Libya. In High SDI regions, the countries with the best burden management are Canada, Iceland, and Switzerland, while the countries with the greatest governance potential are Republic of Korea, the United States Virgin Islands, and Monaco, see Annexed Table 3.

illustrates the frontier analysis results for High and Low NEI risk areas. Panel A shows the frontier trend of High NEI risk areas from 1990 to 2021; Panel B shows the current frontier analysis status of High NEI risk areas in 2021; Panel C shows the frontier trend of Low NEI risk areas from 1990 to 2021; and Panel D shows the current frontier analysis status of Low NEI risk areas in 2021.
Bayesian age-period-cohort
To better understand the trends in the burden of NTDs and malaria beyond 2021, we applied the BAPC model to project the ASDR of NTDs and malaria globally and across different SDI regions over the next 20 years (2022–2041). The results indicate that the global burden of NTDs and malaria is expected to increase overall, rising from 1020·27 per 100,000 in 2021 to 1411·37 per 100,000 in 2041. Specifically, the increasing trends in the burden are particularly notable in the Middle SDI and Low-middle SDI regions, as shown in Fig. 8.

illustrates the projected trends in the burden of NTDs and malaria (measured as age-standardized DALY rates) globally and across different SDI regions over the next 20 years (2022–2041).
Discussion
Although the global burden of NTDs and malaria has declined over recent decades, these diseases remain a major public health challenge worldwide, warranting sustained attention and action. The morbidity and mortality from NTDs and malaria are disproportionately concentrated in children under five years old. As a result, even with the same mortality rates, NTDs and malaria cause a significantly higher DALY burden compared to other diseases. Fortunately, most of these diseases are fully controllable or even eradicable20which highlights the considerable feasibility and potential for reducing the burden of NTDs and malaria.
Between 1990 and 2021, the global incidence of NTDs and malaria was not well-controlled, showing no significant downward trend. In contrast, the incidence of NTDs and malaria in Low SDI regions decreased, whereas it significantly increased in High SDI regions. Several studies suggest that this rise may be associated with international travel, particularly the return of travelers and the importation of cases from endemic areas21,22,23. The decline in mortality from 1990 to 2021 may be attributed to improvements in healthcare systems and international aid. Notably, studies prior to 2019 indicated a declining trend in the burden of NTDs and malaria24,25. However, this study shows that in 2019, there was an inflection point in the mortality rate of NTDs and malaria, which can primarily be attributed to the global outbreak of COVID-19 26. The pandemic disrupted the supply of NTDs and malaria medications and severely limited healthcare services in certain regions27making the management of tropical diseases exceptionally difficult during this period. The observation that high-risk countries exhibited greater vulnerability during specific periods (e.g., the COVID-19 outbreak) indicates a possible spatiotemporal interaction in the distribution of disease burden. In future research, we will further explore the spatiotemporal relationship of the NTDs and malaria burden to elucidate the dynamic process of changes in disease burden.
The study also found that the incidence of NTDs and malaria is generally higher in females across all age groups, whereas the mortality rate and DALYs for NTDs and malaria are higher in males across all age groups. This phenomenon is closely related to gender differences in the immune system. Females typically exhibit a stronger immune response to infectious diseases and tend to have better prognostic outcomes28. In addition, a study from Kenya suggests that women play more roles in agriculture, and the humid agricultural activities may make them more susceptible to malaria29. Another survey from Uganda revealed that, compared to men, women are more likely to seek timely treatment at local health centers after experiencing a fever30. Men, on the other hand, may delay treatment due to a lack of awareness about the importance of seeking medical care, which can exacerbate the disease burden.
NTDs and malaria exhibit extremely high levels of inequality worldwide31. Although the widespread use of vaccines and international aid have significantly reduced the disease burden of NTDs and malaria in low-income countries32the issue of health inequality between low-income and high-income countries remains a serious concern. Studies show that NTDs and malaria exhibit a clear geographic concentration, with the disease burden disproportionately focused in the African region33particularly in Western Sub-Saharan Africa. In 2021, the burden of NTDs and malaria in Western Sub-Saharan Africa accounted for 51·18% of the global total, while the region’s population represented less than 10% of the global population. As a result, the burden rate of NTDs and malaria in Western Sub-Saharan Africa was 10·32 times higher than the global average. These alarming figures highlight the severity of the NTDs and malaria burden in Western Sub-Saharan Africa, while also revealing the global health inequalities associated with these diseases. Although the absolute inequality of the NTDs and malaria burden has been on a downward trend from 1990 to 2021, the relative inequality has not changed significantly. The burden of these diseases remains concentrated in lower- and middle-income countries. NTDs and malaria not only consume significant medical resources and strain already limited financial resources, but they also lead to a substantial reduction in labor productivity34thereby exacerbating the vicious cycle of poverty and inequality.
Certainly, the impact of climate and environment on NTDs and malaria cannot be overlooked. Existing studies have shown that almost all NTDs are significantly affected by climate change35. Since 1950, climate change has rapidly increased the suitability for the transmission of infectious diseases, leading to a sustained rise in the incidence of diseases such as dengue fever, malaria, and vibrio infections36. To this end, this study explores the impact of environmental factors on the burden of NTDs and malaria. We found that inland areas with lower latitudes had significantly higher burden rates of NTDs and malaria. Humid and warm environments provide favorable conditions for the transmission of parasitic diseases37while coastal areas, due to the alternation of sea and land airflows, may partially inhibit the spread of parasitic diseases. In addition, we also explored the interaction between environmental risk factors and socioeconomic indicators. The results indicate that the impact of environmental risk factors and socioeconomic indicators on the burden of NTDs and malaria is not a simple linear relationship. In contrast, the burden of NTDs and malaria in low-SDI regions and high-NEI risk areas is more sensitive to changes in environmental and economic indicators. This means that the burden of NTDs and malaria resulting from global climate change will be disproportionately concentrated in tropical, impoverished regions, further exacerbating the disease burden in these areas.
After controlling for environmental influences, we found that some impoverished regions with high NEI risk have successful experiences in managing the burden of NTDs and malaria that could serve as valuable lessons. For example, the government of Eritrea launched the National Malaria Control Programme (NMCP) in 1995, and by 2017, the country’s malaria mortality rate had decreased by over 97%38. Similarly, the government of Timor-Leste, through the World Health Organization’s drug donation program, implemented the combination mass drug administration (MDA) project39achieving significant results in addressing the burden of NTDs and malaria.
Projections indicate that over the next 20 years, the global burden of NTDs and malaria will show an upward trend, particularly in the Middle SDI and Low-middle SDI regions. High SDI and High-middle SDI regions, with their well-developed healthcare systems and advanced sanitary conditions, are better equipped to manage the burden of NTDs and malaria effectively. In contrast, while Low SDI regions face poor sanitary conditions, their high baseline burden combined with increasing international assistance gives them significant potential for effective control. Consequently, the burden in Low SDI regions is expected to decline steadily over the next 20 years.
On the other hand, Middle SDI and Low-middle SDI regions lack both the capacity to effectively address the disease burden and adequate international aid. In the face of future extreme climate events and the resulting burden of NTDs and malaria, these regions are likely to exhibit lower governance effectiveness. Therefore, future strategies to address NTDs and malaria should not only focus on increasing support for Low SDI regions but also pay more attention to Middle SDI and Low-middle SDI regions, particularly those located in tropical areas.
Limitations
Like all studies based on the GBD database, this research has certain limitations in case identification. The GBD data is based on estimates of global disease burden derived from existing cases, which may introduce some degree of bias in the results. These biases may cause the study results to not fully reflect the actual global disease burden.
Conclusions
Over the past few decades, the overall burden of NTDs and malaria has steadily decreased, which is undoubtedly an encouraging outcome. However, the global distribution of this burden still reveals significant inequality, with a large gap between low-income and high-income countries, particularly in the Western Sub-Saharan Africa region. While the absolute inequality in the burden of NTDs and malaria has declined over the years, little progress has been made in reducing relative inequality. The study also identified significant interactions between environmental risk factors and socio-economic factors in relation to the burden of NTDs and malaria, with regions exhibiting high NEI and low SDI showing greater sensitivity to the impact of these factors. As global warming and the ongoing effects of extreme weather events continue, low-income countries are far less equipped to cope with the burden of NTDs and malaria compared to high-income nations. This suggests that the future disease burden resulting from climate change is likely to disproportionately affect tropical, low-income countries.Over the next 20 years, the global burden of NTDs and malaria is expected to show an upward trend, particularly in the Middle SDI and Low-middle SDI regions.
Data availability
All data used in this study were obtained from the publicly accessible Global Burden of Disease (GBD) database, which can be accessed and downloaded from the following website: https://ghdx.healthdata.org/gbd-2021. Statistical analysis was carried out according to R4.4.1.
References
World Health Organization. Neglected tropical diseases. https://www.who.int/news-room/questions-and-answers/item/neglected-tropical-diseases. Accessed 2024 Nov 22.
Global Health Progress. The London Declaration on NTDs. https://globalhealthprogress.org/collaboration/the-london-declaration-on-ntds. Accessed 2024 Nov 22.
World Health Organization. Accelerating Work To Overcome the Global Impact of Neglected Tropical Diseases: a Roadmap for Implementation (World Health Organization, 2012).
The Lancet. Neglected tropical diseases: Ending the neglect of populations. Lancet 399 (10323), 411 (2022).
World Health Organization. Ending the Neglect To Attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030 (World Health Organization, 2020).
Maxmen, A. How to defuse malaria’s ticking time bomb. Nature 559 (7715), 458–465 (2018).
Imwong, M., Hien, T. T., Thuy-Nhien, N. T., Dondorp, A. M. & White, N. J. Spread of a single multidrug resistant malaria parasite lineage (PfPailin) to Vietnam. Lancet Infect. Dis. 17 (10), 1022–1023 (2017).
White, N. J. Artemisinin resistance—the clock is ticking. Lancet 376 (9758), 2051–2052 (2010).
Ménard, D. & Fidock, D. A. Accelerated evolution and spread of multidrug-resistant *Plasmodium falciparum* takes down the latest first-line antimalarial drug in Southeast Asia. Lancet Infect. Dis. 19 (9), 916–917 (2019).
World Health Organization. World Malaria Report 2023 (World Health Organization, 2023).
World Health Organization. Global Technical Strategy for Malaria 2016–2030: 2021 Update (World Health Organization, 2021).
Hotez, P. J. & Molyneux, D. H. Tropical anemia: One of africa’s great killers and a rationale for linking malaria and neglected tropical disease control to achieve a common goal. PLoS Negl. Trop. Dis. 2 (7), e270 (2008).
Klepac, P. et al. Climate change, malaria and neglected tropical diseases: A scoping review. Trans. R. Soc. Trop. Med. Hyg. 118 (9), 561–579 (2024).
Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2021. Socio-Demographic Index (SDI) 1950–2021. Seattle, United States of America: Institute for Health Metrics and Evaluation (IHME), 2024.GBD (2021).
Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2021 (GBD 2021) Covariates 1980–2021 (Institute for Health Metrics and Evaluation (IHME), 2024).
GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: A systematic analysis for the global burden of disease study 2021. Lancet 403 (10440), 2133–2161 (2024).
World Health Organization. Handbook on health inequality monitoring with a special focus on low- and middle-income countries. https://www.who.int/publications/i/item/9789241548632. Accessed 2024 Jul 7.
Institute for Health Metrics and Evaluation (IHME). Global Fertility, Mortality, Migration, and Population Forecasts 2017–2100 (Institute for Health Metrics and Evaluation (IHME), 2020).
Institute for Health Metrics and Evaluation (IHME). GBD Compare Data Visualization. Seattle, WA: IHME, University of Washington. (2024). http://vizhub.healthdata.org/gbd-compare(link is external). Accessed Nov 18, 2024.
Liese, B., Rosenberg, M. & Schratz, A. Programmes, partnerships, and governance for elimination and control of neglected tropical diseases. Lancet 375 (9708), 67–76 (2010).
Daily, J. P., Minuti, A. & Khan, N. Diagnosis, treatment, and prevention of malaria in the US: A review. JAMA 328 (5), 460–471 (2022).
Zhu, Y. et al. Malaria cases in China acquired through international travel, 2013–2022. J. Travel Med. 31 (8), taae056. https://doi.org/10.1093/jtm/taae056 (2024).
Kurcheid, J. et al. Neglected tropical diseases in australia: A narrative review. Med. J. Aust. 216 (10), 532–538. https://doi.org/10.5694/mja2.51533 (2022).
Liu, Q. et al. Incidence and mortality trends of neglected tropical diseases and malaria in China and ASEAN countries from 1990 to 2019 and its association with the socio-demographic index. Glob Health Res. Policy. 8 (1), 22 (2023).
Shi, D. et al. Trends of the global, regional and National incidence, mortality, and disability-adjusted life years of malaria, 1990–2019: An analysis of the global burden of disease study 2019. Risk Manag Healthc. Policy. 16, 1187–1201 (2023).
Rasoanaivo, T. F. et al. The impact of COVID-19 on clinical research for neglected tropical diseases (NTDs): A case study of bubonic plague. PLoS Negl. Trop. Dis. 15 (12), e0010064 (2021).
Adepoju, P. NTDs in the time of COVID-19. Lancet Microbe. 1 (6), e244 (2020).
Briggs, J., Murray, M., Nideffer, J. & Jagannathan, P. Sex-linked differences in malaria risk across the lifespan. Curr. Top. Microbiol. Immunol. 441, 185–208 (2023).
Woldu, D. O. & Haile, Z. T. Gender roles and perceptions of malaria risk in agricultural communities of Mwea division in central Kenya. Women Health. 55 (2), 227–243 (2015).
Okiring, J. et al. Gender difference in the incidence of malaria diagnosed at public health facilities in Uganda. Malar. J. 21 (1), 22 (2022).
Houweling, T. A. et al. Socioeconomic inequalities in neglected tropical diseases: A systematic review. PLoS Negl. Trop. Dis. 10 (5), e0004546 (2016).
Zhang, H. et al. Global vaccine coverage and childhood survival estimates: 1990–2019. Bull. World Health Organ. 102 (4), 276–287 (2024).
George, N. S. et al. Addressing neglected tropical diseases in Africa: A health equity perspective. Glob. Health Res. Policy. 8 (1), 30 (2023).
Andrade, M. V. et al. The economic burden of malaria: A systematic review. Malar. J. 21 (1), 283 (2022).
Booth, M. Climate change and the neglected tropical diseases. Adv. Parasitol. 100, 39–126 (2018).
Watts, N. et al. The 2020 report of the lancet countdown on health and climate change: responding to converging crises. Lancet 397 (10269), 129–170 (2021).
Githeko, A. K., Lindsay, S. W., Confalonieri, U. E. & Patz, J. A. Climate change and vector-borne diseases: A regional analysis. Bull. World Health Organ. 78 (9), 1136–1147 (2000).
Mihreteab, S. et al. Retrospective data analyses of social and environmental determinants of malaria control for elimination prospects in Eritrea. Parasit. Vectors. 13 (1), 126 (2020).
Le, B. et al. The impact of ivermectin, diethylcarbamazine citrate, and albendazole mass drug administration on the prevalence of scabies and soil-transmitted helminths in school-aged children in three municipalities in Timor-Leste: A before-after assessment. Lancet Glob Health. 11 (6), e924–e932 (2023).
Acknowledgements
This research was supported by the Natural Science Foundation of Shandong Province (ZR2023QH259), the project of National Administration of Traditional Chinese Medicine (GZY-KIS-SD-2023-026), and the Key Research and Development Program of Jining City (2022YXNS170). We would like to extend our sincere gratitude to the Global Burden of Disease (GBD) collaborators and research teams for their tireless efforts in collecting, analyzing, and disseminating high-quality global health data. Their work provides an invaluable foundation for our study and continues to advance understanding and action in addressing global health inequalities. We also wish to thank all individuals and organizations dedicated to research on tropical diseases, whose invaluable contributions have greatly enhanced the field. Without their dedication and commitment, this research would not have been possible.
Author information
Authors and Affiliations
Contributions
Yang Lin, Qipeng Long: Responsible for data organization, data analysis, and manuscript writing. Jin Liu, Yiming Zhang: Assisted with manuscript preparation, including data collection and organization. Jialian Li, Yang Li: Assisted with manuscript preparation, data verification, and proofreading. Jihong Sun: Conducted code verification and results reproduction. Shulong Jiang, Yufei Wang: Provided guidance on topic selection and writing, verified data and code, and offered financial support.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lin, Y., Long, Q., Sun, J. et al. Global trends, health inequalities, and projections in the burden of neglected tropical diseases and malaria from 1990 to 2021. Sci Rep 15, 20958 (2025). https://doi.org/10.1038/s41598-025-05530-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-05530-y
