
Abstract
Rheumatoid arthritis (RA) significantly drives global morbidity and mortality, yet its evolving impact in low- and middle-income countries remains underexplored. This study harnesses extensive global burden of disease (GBD) data to delineate the temporal trends of RA burden in the Islamic Republic of Pakistan from 1990 to 2021, examine its association with socio-demographic development, and forecast future trajectories through 2036. This retrospective epidemiological study quantified RA disease metrics in Pakistan through GBD data interrogation. Joinpoint regression modeling delineated temporal trajectories, calculating average annual percent change (AAPC) with 95% confidence intervals (CIs). Spearman’s rank correlation assessed the relationship between socio-demographic index (SDI) values and age-standardized rates (ASRs) of RA across 204 regions. A Bayesian age–period–cohort (BAPC) model was employed to project RA burden trends in Pakistan from 2022 to 2036. Stratified comparative assessments revealed age- and sex-specific demographic disparities. Although age-standardized incidence rate (ASIR) and age-standardized prevalence rate (ASPR) exhibited modest declines (AAPC: -0.10% and − 0.09%, respectively), the absolute numbers of incident and prevalent RA cases increased markedly—from 8,606 to 19,454 and from 134,628 to 318,963, respectively—between 1990 and 2021. Mortality rates showed a slight upward trend (AAPC: 0.35%), with total deaths rising from 478 to 1,006, while Disability-adjusted life years (DALYs) nearly doubled, increasing from 27,314 to 62,774. Age-specific analyses revealed peak incidence among younger individuals (20–24 years) and higher mortality and DALYs among older populations, particularly those aged 75 and above. Additionally, females consistently experienced a greater burden across all metrics compared to males. SDI exhibited significant positive correlations with ASIR (r = 0.42), ASPR (r = 0.47), age-standardized mortality rate (ASMR) (r = 0.32), and age-standardized DALYs rate (ASDR) (r = 0.46; all p < 0.001), indicating that higher socio-demographic development was associated with a greater documented RA burden. BAPC projections forecast a gradual decline in age-standardized RA rates through 2036, although absolute case numbers are expected to remain high owing to population growth and demographic aging. The RA burden in Pakistan has escalated over the past three decades, with higher-SDI regions demonstrating disproportionately greater age-standardized rates and documented cases. Despite anticipated per-capita declines in RA incidence, prevalence, mortality, and DALYs by 2036, demographic shifts will likely sustain a substantial absolute burden. These findings emphasize the necessity of precise public health measures to advance early diagnosis, optimize disease management, and reinforce prevention—particularly in rapidly developing areas and among high-risk groups such as women and the elderly.
Similar content being viewed by others
Introduction
Rheumatoid arthritis is a chronic, systemic autoimmune disorder that imposes a substantial burden on global public health through its association with increased morbidity, mortality, and disability. Despite extensive research in high-income regions, the evolving epidemiology of RA in low- and middle-income countries, such as Pakistan, remains underexplored1,2,3. The country’s rapid demographic changes and limited healthcare resources underscore the need for a nuanced understanding of RA trends and gender-specific disparities, as well as how socio-economic development influences disease burden.
Recent epidemiological studies have highlighted the significant burden of RA in Pakistan. A systematic review and meta-analysis found that RA patients in Pakistan are predominantly female, with a low to moderate prevalence in the general population4. Another study conducted in a tertiary care hospital in Karachi reported a higher prevalence among patients visiting the orthopedic outpatient department, also noting a greater proportion of females affected5. These findings underscore the need for comprehensive epidemiological studies to better understand the temporal trends and gender disparities of RA in Pakistan.
Led by the Institute for Health Metrics and Evaluation (IHME), the GBD study integrates data from vital records, surveys, registries, and the literature to systematically estimate health losses across a broad spectrum of diseases, risk factors, and anatomical sites6,7. Employing standardized indicators and Bayesian meta-regression techniques, it produces socio-demographically adjusted comparisons that facilitate cross-national health assessments8. Annual updates monitor evolving epidemiological trends, enabling policymakers to prioritize interventions and optimize resource allocation. In addition to quantifying incidence, prevalence, mortality, and DALYs, contemporary GBD analyses often examine the relationship between socio-demographic development—captured by the SDI—and disease burden, and also employ predictive modeling to forecast future trends9,10.
In this study, we leverage robust GBD datasets from 1990 to 2021 to conduct a comparative decomposition analysis of RA epidemiology in Pakistan. By employing joinpoint regression modeling and stratified assessments, our objective is to delineate temporal trends and elucidate the underlying demographic and gender-specific factors driving the evolving burden of RA. We further explore the association between SDI and RA burden across 204 countries and territories to understand socio-economic influences. Finally, we apply a Bayesian age–period–cohort (BAPC) model to project RA burden trajectories in Pakistan from 2022 to 2036. This comprehensive approach aims not only to fill existing gaps in the literature but also to provide actionable insights for the development of targeted public health interventions and optimized disease management strategies in Pakistan.
Methods
Data source
This study is a retrospective epidemiological analysis based on publicly available data from the Global Burden of Disease (GBD) 2021 study. The GBD 2021, coordinated by the Institute for Health Metrics and Evaluation (IHME) at the University of Washington, provides a comprehensive and systematic assessment of the incidence, prevalence, mortality, disability-adjusted life years (DALYs), and risk factors for 371 diseases and injuries, including RA, across 204 countries and territories from 1990 to 202111. In this study, we utilized the Global Health Data Exchange platform (https://ghdx.healthdata.org/gbd-2021) to retrieve and download the raw data pertaining to RA in Pakistan. To facilitate regional comparisons and epidemiological analyses, the GBD organizes countries into hierarchical geographic categories, notably “super regions” which cluster countries based on shared socioeconomic, demographic, and health system characteristics. Specifically, the GBD 2021 divides the world into seven super regions:1 High Income2, Latin America and Caribbean3, Sub-Saharan Africa4, North Africa and Middle East5, South Asia6, Southeast Asia, East Asia, and Oceania, and7 Central Europe, Eastern Europe, and Central Asia12. Pakistan is classified within the “South Asia” super region, comprising densely populated countries facing high burdens of communicable and non-communicable diseases amid diverse socioeconomic environments and rapid epidemiologic transitions13,14. This classification provides a critical framework for contextualizing Pakistan’s RA burden relative to comparable countries with similar health challenges and development trajectories.
Definition of RA
Rheumatoid arthritis is a chronic systemic autoimmune disorder characterized by joint pain, swelling, and deformity, often accompanied by systemic symptoms. The case definitions for RA in the GBD database are based on the International Classification of Diseases (ICD) codes: ICD-9 codes 714.0–714.9 and ICD-10 codes M05, M06, and M0815.
Measures of disease burden
Descriptive statistics were employed to summarize the annual incidence, prevalence, mortality rates, and disability-adjusted life years (DALYs) for RA. These estimates included 95% uncertainty intervals (UIs), which were computed as the 2.5th and 97.5th ordered estimates derived from 1,00 draws from the posterior distribution16. Additionally, we utilized age-standardized rates, including age-standardized incidence rates (ASIR), prevalence rates (ASPR), mortality rates (ASMR), and DALYs rates (ASDR), to facilitate comparisons of disease burden17.
Joinpoint regression
Joinpoint regression models were used to analyze temporal trends by segmenting the study period based on the distribution characteristics of the disease18. A logarithmic linear model was applied for segmented regression analysis. The grid search method identified all possible joinpoints, calculating the corresponding mean squared errors (MSEs) and selecting the point with the smallest MSE as the joinpoint. A Monte Carlo permutation test was employed to determine the appropriate number of joinpoints, allowing for 0 to 5 joinpoints. The average annual percent change (AAPC) along with its 95% confidence interval (CI) was computed to describe overall trend changes; an AAPC greater than 0 with a p-value < 0.05 indicates an increase over the period. For example, if the AAPC for RA incidence from 1990 to 2021 is reported as 2.0 (p < 0.05), this signifies an annual increase of 2.0% in incidence. The Joinpoint software is provided by the National Cancer Institute and can be accessed at https://surveillance.cancer.gov/joinpoint/.
Socio-demographic index (SDI)
The Socio-Demographic Index (SDI) is a summary indicator that reflects a country or region’s health-related development status on a global scale. It incorporates factors such as birth rates, educational attainment, and economic status. The SDI ranges from 0 to 1, where higher values indicate greater social and economic development19. Based on these values, the 204 countries/territories were categorized into quintiles: high, high-middle, middle, low-middle, or low20. For comparative analyses, countries included in the SDI correlation assessments are classified by their respective GBD super regions, as defined above. This stratification aids in identifying region-specific patterns and the socio-demographic context influencing RA burden globally. We employed Spearman’s correlation coefficient to explore potential associations between ASIR, ASPR, ASMR, and the SDI, thereby enhancing our understanding of socio-economic influences on the RA burden.
Bayesian age-period-cohort (BAPC) model
The Bayesian age-period-cohort (BAPC) model is a method widely used in epidemiology and biostatistics to analyze the relationships between incidence, prevalence, mortality, and DALYs rates over time. This model combines sample information with prior knowledge to obtain unique parameter estimates, resulting in robust and reliable outcomes21. In this study, the BAPC package was employed to predict trends for RA incidence, prevalence, mortality, and DALYs from 2022 to 203622. The insights generated from this modeling can assist in formulating effective public health policies aimed at prevention and management strategies for RA.
Ethical considerations
This research utilized publicly accessible data from the GBD database, which does not necessitate ethical approval. All procedures were conducted in compliance with relevant guidelines and regulations.
Statistical analysis
All statistical computations were executed in R (v4.0.3) using Joinpoint software (v4.9.0.0) and visualized via the ggplot2 package.
Results
Overview of RA burden in the Islamic Republic of Pakistan (1990–2021)
The burden of RA in the Islamic Republic of Pakistan from 1990 to 2021 reveals notable trends (Table 1). Despite a modest decline in age-standardized incidence (AAPC: -0.10%, 95% CI: -0.15 to -0.05) and prevalence (AAPC: -0.09%, 95% CI: -0.15 to -0.03) rates, the total number of incident cases increased significantly from 8,606 (95% CI: 7,396–10,011) in 1990 to 19,454 (95% CI: 16,729–22,566) in 2021, while prevalent cases surged from 134,628 (95% CI: 113,051–158,450) to 318,963 (95% CI: 266,005–379,802). In contrast, age-standardized mortality (AAPC: 0.35%, 95% CI: 0.29 to 0.41) and disability-adjusted life years (DALY) rates (AAPC: 0.06%, 95% CI: -0.05 to -0.17) exhibited slight increases or remained stable. Total deaths rose from 478 (95% CI: 294–703) to 1,006 (95% CI: 624–1,401), and DALYs nearly doubled from 27,314 (95% CI: 20,080–35,286) to 62,774 (95% CI: 46,290–83,502). These findings suggest that while the per capita risk of developing RA has marginally decreased, the absolute burden—measured by incidence, prevalence, mortality, and DALYs—has significantly increased in Pakistan over the past three decades, highlighting the critical necessity for the development and implementation of more effective public health strategies to alleviate this escalating challenge.
Temporal trends in the age-standardized rates of RA in the Islamic Republic of Pakistan (1990–2021)
Figure 1 illustrates the AAPC in age-standardized rates of RA, including ASIR, ASPR, ASMR, and ASDR in Pakistan from 1990 to 2021. From 1990 to 1999, the ASIR exhibited a significant decline (AAPC = -1.14), followed by a rise (AAPC = 0.36 from 1999 to 2012) and a sharper increase (AAPC = 1.18 from 2012 to 2019). The period from 2019 to 2021 saw a marked decrease (AAPC = -2.77), possibly indicating improvements in primary prevention or diagnostic practices. The ASPR followed a similar pattern, decreasing significantly from 1990 to 1999 (AAPC = -1.10), then rising gradually thereafter, with the most notable increase occurring from 2013 to 2019 (AAPC = 1.37). A decline in the ASPR from 2019 to 2021 (AAPC = -3.35) may reflect improvements in disease management or reduced incidence. The ASMR demonstrated an early significant increase (AAPC = 2.20 from 1990 to 1992; AAPC = 3.19 from 1992 to 1996), followed by stabilization (AAPC = 1.01 from 1996 to 2002) and a subsequent decline (AAPC = -0.97 from 2005 to 2015 and AAPC = -0.40 from 2015 to 2021), suggesting progress in therapeutic interventions or secondary prevention strategies that have reduced RA-related mortality. Similarly, the ASDR rose significantly (AAPC = 0.48 from 1990 to 2004), but showed a decline (AAPC = -0.35 from 2004 to 2013), with subsequent fluctuations. The recent decrease in ASDR (AAPC = -2.08 from 2019 to 2021) further indicates improvements in reducing the disease burden through enhanced management or prevention.

The APC of ASIR, ASPR, ASMR, and ASDR of RA in the Islamic Republic of Pakistan from 1990 to 2021. (A) ASIR; (B) ASPR; (C) ASMR; (D) ASDR; ASIR, age-standardized incidence rates; ASPR, age-standardized Prevalence Rate; ASMR, age-standardized mortality rates; ASDR, age-standardized DALYs rates; DALYs, disability-adjusted life years; APC, annual percentage change; RA, Rheumatoid arthritis.
Comparative analysis of RA metrics by age group in the Islamic Republic of Pakistan (1990 vs. 2021)
As shown in Fig. 2, the age-specific burden of RA in Pakistan underwent substantial changes between 1990 and 2021. The highest number of new RA cases was consistently observed in the 20 − 24 age group across both years. However, the CIR peaked in the 70 − 74 age group, indicating a higher risk of onset in older populations. In terms of prevalence, the 40 − 44 age cohort recorded the highest number of cases in 1990; however, by 2021, this shifted to the 35 − 39 age group. Despite this change, the 70 − 74 age group remained the group with the highest prevalence rate in both years, indicating the sustained presence of RA among the elderly population. Regarding mortality, the 75 − 79 age group experienced the most RA-related deaths in both 1990 and 2021, while the highest mortality rate was observed in individuals aged 95 and older. This trend highlights the severe impact of RA in advanced age. Similarly, the 65 − 69 age group accounted for the largest number of DALYs in both years, with the highest disease burden seen in the 95 + age group, further emphasizing the significant health burden RA imposes on older adults.

Comparative of the incidence, prevalence, deaths, and DALYs counts, along with their crude rates, by age group in the Islamic Republic of Pakistan from 1990 and 2021. (A, B) Incident cases and CIR; (C,D) Prevalent cases and CPR; (E,F) Death cases and CMR; (G,H) DALYs counts and CDR; CIR, Crude Incidence Rate; CPR, Crude Prevalence Rate; CMR, Crude Mortality Rate; CDR, Crude DALYs Rate; DALYs, disability-adjusted life years.
Comparative analysis of age- and sex-specific trends of RA in the Islamic Republic of Pakistan (1990 vs. 2021)
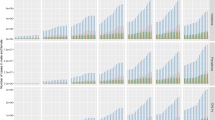
Figure 3 delineates the age-stratified and sex-specific epidemiological profile of RA incidence, prevalence, mortality, and DALYs across the 1990–2021 observation period. Notably, age-resolved analyses revealed persistent sex-based discrepancies in all evaluated parameters. The incidence disparity was most pronounced in the 20-24-year cohort, with male cases rising from 382 (1990) to 869 (2021), while female cases surged from 896 to 1,965 in corresponding years. Evolution of prevalence patterns demonstrated temporal shifts in peak burden: female prevalence maxima transitioned from 9,325 cases (40–44 years, 1990) to 25,640 cases (35–39 years, 2021), concurrent with male maxima progression from 4,919 cases (45–49 years) to 12,405 cases (40–44 years). Mortality analysis identified persistent female predominance with maximal deaths in the 75-79-year group for both sexes. DALYs quantification revealed diverging trajectories: female peak burden persisted in the 65-69-year cohort, whereas males experienced an epidemiologic transition with peak DALYs migrating from 70 to 79 years (1990) to 35–39 years (2021). This comprehensive stratification highlights critical sex-specific variations in RA’s epidemiologic progression over three decades.

Comparison of the number of incidence, prevalence, mortality, and DALYs of RA in males and females of different age groups in the Islamic Republic of Pakistan in 1990 and 2021. (A) 1990 number of Incidence; (B) 1990 number of Prevalence; (C) 1990 number of Deaths; (D) 1990 number of DALYs; (E) 2021 number of Incidence; (F) 2021 number of Prevalence; (G) 2021 number of Deaths; (H) 2021 number of DALYs; DALYs, disability-adjusted life years; RA, Rheumatoid arthritis.
Full-age cases and age-standardized rates of RA in the Islamic Republic of Pakistan (1990–2021)
Figure 4 offers an in-depth depiction of RA burden in Pakistan from 1990 to 2021, highlighting pronounced gender disparities. In 1990, the ASIR was 83,853.04 per 100,000 for men and 112,629.51 per 100,000 for women, with both sexes experiencing a general increase by 2021 (81,454.75 for men and 105,691.14 for women). Similarly, the ASPR increased from 1,410,557.40 for men and 2,303,344.70 for women in 1990 to 1,361,879.18 for men and 2,151,903.56 for women in 2021. Between 1990 and 2021, the ASMR modestly declined, with 1990 rates of 4,873.25 for men and 17,321.88 for women shifting to 4,804.06 for men and 18,448.28 for women by 2021.The ASDR also exhibited an upward trend, increasing from 270,545.96 for men and 620,924.75 for women in 1990 to 262,246.52 for men and 604,055.75 for women in 2021. Throughout the study period, women consistently had higher ASIR, ASPR, ASMR, and ASDR values compared to men, with the gender gap remaining relatively stable.

comparison of full-age cases and age-standardized rates of incidence, prevalence, mortality and DALYs among men and women in the Islamic Republic of Pakistan from 1990 to 2021. (A, B) Incident cases and ASIR; (C,D) Prevalent cases and ASPR;(E,F) Death cases and ASMR; (G,H) DALYs counts and ASDR; ASIR, age-standardized incidence rates; ASPR, age-standardized Prevalence Rate; ASMR, age-standardized mortality rates; ASDR, age-standardized DALYs rates; DALYs, disability-adjusted life years.
Correlation between SDI values and RA burden
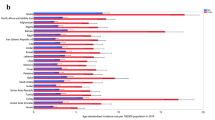
To investigate the potential association between SDI and the burden of RA, a Spearman rank correlation analysis was performed to assess the relationship between SDI values and ASR across 204 geographical regions (Fig. 5). The analysis revealed significant correlations, indicating that higher SDI values are associated with lower RA incidence, prevalence, mortality, and DALYs. Specifically, the ASIR showed a correlation coefficient of 0.42 (p < 0.001) with SDI, while the ASPR exhibited a coefficient of 0.47 (p < 0.001). Additionally, the ASMR had a correlation coefficient of 0.32 (p < 0.001), and the ASDR demonstrated a correlation coefficient of 0.46 (p < 0.001). These findings emphasize the significant role of SDI as a socio-economic indicator influencing the epidemiology of RA, suggesting that improvements in socio-economic conditions may lead to a reduction in health burdens associated with this chronic disease.

Age-standardized rates of incidence, prevalence, deaths and DALYs of RA in 204 countries globally by SDI in 2021. (A) ASR of incidence for 204 countries and territories by SDI in 2021; (B) ASR of prevalence for 204 countries and territories by SDI in 2021; (C) ASR of deaths for 204 countries and territories by SDI in 2021; (D) ASR of DALYs for 204 countries and territories by SDI in 2021; DALYs, disability-adjusted life years; RA, Rheumatoid arthritis.
Forecasting future RA burden in Pakistan (2022–2036)
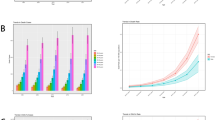
Utilizing the BAPC model, we forecasted the trends in ASIR, ASPR, ASMR, and ASDR for RA in Pakistan from 2022 to 2036 (Fig. 6). Our projections suggest a gradual decline in all age-standardized RA metrics over the next 15 years, driven by potential improvements in early detection, disease management, and therapeutic interventions. However, the absolute burden of RA is anticipated to remain significant due to the growing population and demographic aging. These trends underscore the importance of continuing to strengthen healthcare infrastructure and public health interventions to manage RA effectively in the coming years.

BAPC prediction of RA burden in the next 15 years. (A) The change trends of the ASIR from 1990 to 2036 in the Islamic Republic of Pakistan; (B) The change trends of the ASPR from 1990 to 2036 in the Islamic Republic of Pakistan; (C) The change trends of the ASMR from 1990 to 2036 in the Islamic Republic of Pakistan; D: The change trends of the ASDR from 1990 to 2036 in the Islamic Republic of Pakistan; BAPC, Bayesian Age-Period-Cohort; ASIR, age-standardized incidence rates; ASPR, age-standardized Prevalence Rate; ASMR, age-standardized mortality rates; ASDR, age-standardized DALYs rates; DALYs, disability-adjusted life years.
Discussion
Our investigation into the temporal trends and sex-based differences in RA burden in Pakistan from 1990 to 2021 provides crucial insights into the shifting epidemiological landscape of this chronic disease. Despite modest reductions in ASIR and ASPR, the overall burden—reflected in incident cases, prevalence, mortality, and DALYs—has escalated significantly over the past three decades. These results underscore the intensifying public health challenge of RA in Pakistan, particularly among female and older populations.
The increasing absolute numbers of RA cases, deaths, and DALYs in Pakistan highlight a concerning trend. While the ASRs suggest a marginal reduction in per capita risk, the population growth and aging have driven a significant rise in the absolute burden, indicating that RA continues to be a major contributor to disability, particularly in LMICs such as Pakistan, where healthcare resources are constrained and access to effective treatments is limited23. The doubling of DALYs from 27,314 in 1990 to 62,774 in 2021 underscores the substantial disability and economic impact of RA, reinforcing the urgent need for focused interventions.
Our findings consistently demonstrate a higher burden of RA among females compared to males; a pattern well-documented in epidemiological studies. Hormonal, genetic, and immunological factors are thought to contribute to this disparity24,25,26. The peak incidence among younger women (20–24 years) suggests that RA onset often coincides with reproductive age, potentially exacerbating its impact on quality of life and socioeconomic productivity. The higher mortality and DALYs among older women further highlight the need for gender-sensitive healthcare strategies, including early diagnosis and tailored treatment regimens. The age-specific analysis reveals that RA incidence peaks in younger individuals (20–24 years), while mortality and DALYs are concentrated among older populations, particularly those aged 75 and above. This dual burden—early onset and late-life complications—necessitates a life-course approach to RA management. Early diagnosis and aggressive treatment in younger patients could mitigate long-term disability, while improved palliative and supportive care for older adults could reduce mortality and improve quality of life27,28.
Utilizing Joinpoint regression analysis yields critical insights into the evolving temporal patterns of RA burden in Pakistan. The initial decline in ASIR and ASPR during the 1990s may reflect improvements in primary prevention or diagnostic practices, while the subsequent rise suggests increasing awareness and reporting of RA. The recent decline in ASIR and ASPR (2019–2021) could indicate enhanced disease management or the impact of public health interventions; however, further research is needed to confirm these trends. The slight increase in ASMR underscores the need for better access to effective therapies, particularly in resource-limited settings.
Spearman correlation analysis demonstrated robust, statistically significant positive associations between SDI and every RA burden metric—incidence, prevalence, mortality, and DALYs—underscoring that regions with higher socio-demographic development report substantially greater RA rates. This pattern likely reflects superior diagnostic infrastructure, more comprehensive reporting systems, and greater health-seeking behavior in higher-SDI settings, whereas lower-SDI areas may systematically underreport cases due to limited healthcare access and diagnostic capacity29,30. Thus, socio-economic development exerts a dual influence: it both enhances case detection and management and reveals a previously hidden burden of disease. To address these disparities, public health strategies must target underdiagnosis in low-SDI regions and guarantee equitable access to care throughout Pakistan.
Bayesian age–period–cohort (BAPC) projections suggest that, although age-standardized RA rates in Pakistan are expected to decline modestly between 2022 and 2036, demographic pressures—specifically ongoing population growth and aging—will keep the absolute number of RA cases high. This divergence—falling per-capita rates alongside rising case counts—poses a significant policy challenge: interventions must not only curb incidence and improve outcomes but also anticipate and accommodate the healthcare needs of a growing elderly population. Strengthening diagnostic services, expanding the availability of disease-modifying antirheumatic therapies, and implementing focused prevention and support programs for women and older adults will be crucial to mitigate RA’s social and economic burden through 2036 and beyond.
Specifically, the increased absolute burden necessitates enhanced healthcare capacity, including more rheumatology services and trained specialists, particularly in underserved areas. Persistent gender disparities highlight the need for gender-sensitive policies, such as targeted screening for women and integrating RA awareness into women’s health programs. Age-specific trends suggest a life-course approach: early intervention for younger patients and comprehensive care for older adults. To address potential underdiagnosis in low-SDI regions, strengthening primary healthcare and diagnostic capabilities is crucial. Policy measures should focus on improving screening, ensuring treatment accessibility, conducting awareness campaigns, and planning for future healthcare needs based on demographic projections.
Our study leverages the comprehensive and globally comparable data from the GBD study, providing robust estimates of RA burden in Pakistan. The use of Joinpoint regression allows for a nuanced analysis of temporal trends, offering valuable insights for public health planning. However, the study is limited by the inherent constraints of GBD data, including potential underreporting of RA cases in LMICs and the reliance on modeling estimates. Additionally, the absence of granular data on individual-level socioeconomic status, healthcare access, and treatment patterns limits our ability to explore all underlying drivers. Future research should integrate the forthcoming GBD 2023 estimates and investigate regional variations within Pakistan to refine these insights and guide localized interventions.
The escalating burden of RA in Pakistan calls for a multi-faceted public health response. Strengthening healthcare infrastructure to facilitate early diagnosis and access to disease-modifying antirheumatic drugs is critical. Public awareness campaigns targeting high-risk groups, particularly women and the elderly, could improve early detection and adherence to treatment. Furthermore, longitudinal studies are needed to elucidate the socioeconomic and environmental determinants of RA in Pakistan and to evaluate the effectiveness of targeted interventions.
Despite the strengths of our comprehensive GBD database and rigorous Joinpoint regression analyses, this study has several limitations. First, our findings are based on the GBD 2021 estimates, which were the latest available data at the time of analysis. We acknowledge that the GBD 2023 data are scheduled for release imminently and will supersede the 2021 estimates. The updated data may yield different estimates and temporal trends; therefore, our results should be interpreted within the context of the GBD 2021 dataset. Future research incorporating the GBD 2023 estimates will be essential to validate and update these findings.
Conclusions
In summary, our analysis reveals that the burden of RA in Pakistan has escalated markedly over the past three decades, with significant disparities observed across gender, age, and socio-demographic development. Although age-standardized metrics show modest improvements, the absolute burden continues to grow, primarily driven by population expansion, demographic aging, and increasing disease detection in higher-SDI regions. This widening burden highlights the dual role of socio-economic development: while it facilitates better detection and management, it also uncovers a previously underreported disease burden. These findings underscore the urgent need for precision-targeted public health interventions that address the underdiagnosis in low-SDI regions while ensuring equitable access to care across Pakistan. Moreover, given the projected future burden, particularly among women and the elderly, overcoming this challenge will require a synergistic approach integrating healthcare, policy, and research efforts. Strengthening healthcare infrastructure, expanding access to disease-modifying therapies, and implementing targeted prevention programs will be essential in mitigating RA’s socio-economic and disability impacts through 2036 and beyond.
Data availability
All data utilized in this study were obtained from public repositories, including the Institute for Health Metrics and Evaluation (IHME) and other official sources. The datasets generated and/or analyzed during the current study are available in the GBD database (https://vizhub.healthdata.org/gbd-results/).
Abbreviations
- GBD:
-
Global Burden of Disease
- IHME:
-
Institute for Health Metrics and Evaluation
- RA:
-
Rheumatoid arthritis
- ASRs:
-
Age-Standardized Rates
- ASIR:
-
Age-Standardized Incidence Rate
- ASPR:
-
Age-Standardized Prevalence Rate
- ASMR:
-
Age-Standardized Mortality Rate
- ASDR:
-
Age-Standardized DALYs Rate
- AAPC:
-
Average Annual Percent Change
- CIs:
-
Confidence Intervals
- DALYs:
-
Disability-Adjusted Life Years
- CIR:
-
Crude Incidence Rate
- CPR:
-
Crude Prevalence Rate
- CMR:
-
Crude Mortality Rate
- CDR:
-
Crude DALYs Rate
- LMICs:
-
Low- and Middle-Income Countries
- SDI:
-
Socio-Demographic Index
- ICD:
-
International Classification of Diseases
References
Di Matteo, A., Bathon, J. M. & Emery, P. Rheumatoid arthritis. Lancet (London England). 402, 2019–2033 (2023).
Brown, P., Pratt, A. G. & Hyrich, K. L. Therapeutic advances in rheumatoid arthritis. BMJ (Clinical Res. ed.). 384, e070856 (2024).
Konzett, V. & Aletaha, D. Management strategies in rheumatoid arthritis. Nat. Rev. Rheumatol. 20, 760–769 (2024).
Naqvi, A. A., Hassali, M. A. & Aftab, M. T. Epidemiology of rheumatoid arthritis, clinical aspects and socio-economic determinants in Pakistani patients: A systematic review and meta-analysis. J. Pak. Med. Assoc. 69, 389–398 (2019).
Mohsin, Z. et al. Prevalence of rheumatic diseases in a tertiary care hospital of Karachi. Cureus 10, e2858 (2018).
Ward, Z. J. & Goldie, S. J. Global burden of disease study 2021 estimates: implications for health policy and research. Lancet (London England). 403, 1958–1959 (2024).
Global fertility. In 204 countries and territories, 1950–2021, with forecasts to 2100: a comprehensive demographic analysis for the global burden of disease study 2021. Lancet (London England). 403, 2057–2099 (2024).
Bartoš, F., Maier, M., Stanley, T. D. & Wagenmakers, E. J. Robust bayesian meta-regression: Model-averaged moderation analysis in the presence of publication bias. Psychological Methods. https://doi.org/10.1037/met0000737 (2025).
Global National mortality among young people aged 10–24 years, 1950–2019: a systematic analysis for the global burden of disease study 2019. Lancet (London England). 398, 1593–1618 (2021).
Liu, J., Liu, Y., Ma, W., Tong, Y. & Zheng, J. Temporal and Spatial trend analysis of all-cause depression burden based on global burden of disease (GBD) 2019 study. Sci. Rep. 14, 12346 (2024).
Murray, C. J. L. Findings from the global burden of disease study 2021. Lancet (London England). 403, 2259–2262 (2024).
Global National burden of diseases and injuries for adults 70 years and older: systematic analysis for the global burden of disease 2019 study. BMJ (Clinical Res. ed.). 376, e068208 (2022).
Mahipala, P., Dorji, G., Tisocki, K. & Rani, M. A critical review of addressing cardiovascular and other non-communicable diseases through a primary health care approach in the South-East Asia region. Cardiovasc. Diagnosis Therapy. 9, 150–157 (2019).
Haq, Z., Afaq, S., Ibrahim, M., Zala, M. & Asim Prevalence of communicable, non-communicable diseases, disabilities and related risk factors in Khyber Pakhtunkhwa pakistan: findings from the Khyber Pakhtunkhwa integrated population and health survey (2016-17). PloS One. 20, e0308209 (2025).
Lee, H. et al. Validation of serostatus of rheumatoid arthritis using ICD-10 codes in administrative claims data. Pharmacoepidemiol. Drug Saf. 32, 586–591 (2023).
Global & national burden of rheumatoid arthritis. 1990–2020, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. 5, e594–e610 (2023).
Burden of disease scenarios. For 204 countries and territories, 2022–2050: a forecasting analysis for the global burden of disease study 2021. Lancet (London England). 403, 2204–2256 (2024).
Kim, H. J., Fay, M. P., Feuer, E. J. & Midthune, D. N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 19, 335–351 (2000).
Global National progress towards sustainable development goal 3.2 for neonatal and child health: all-cause and cause-specific mortality findings from the global burden of disease study 2019. Lancet (London England). 398, 870–905 (2021).
Dong, Y. et al. Leukemia incidence trends at the global, regional, and National level between 1990 and 2017. Experimental Hematol. Oncol. 9, 14 (2020).
Cai, Y. et al. The burden of rheumatoid arthritis: findings from the 2019 global burden of diseases study and forecasts for 2030 by bayesian Age-Period-Cohort analysis. Journal Clin. Medicine 12(4), 1291 (2023).
Jiang, K. et al. Examining the dietary contributions of lipids to pancreatic cancer burden (1990–2021): incidence trends and future projections. Lipids Health Dis. 24, 62 (2025).
Ahmed, S. H. et al. The current state of primary healthcare in pakistan: a way forward for low-to-middle income countries. Prim. Health Care Res. Dev. 25, e59 (2024).
Srivastava, S. & Rasool, M. Genetics, epigenetics and autoimmunity constitute a Bermuda triangle for the pathogenesis of rheumatoid arthritis. Life Sci. 357, 123075 (2024).
Alpízar-Rodríguez, D., Pluchino, N., Canny, G., Gabay, C. & Finckh, A. The role of female hormonal factors in the development of rheumatoid arthritis. Rheumatol. (Oxford England). 56, 1254–1263 (2017).
Berglin, E. et al. Influence of female hormonal factors, in relation to autoantibodies and genetic markers, on the development of rheumatoid arthritis in Northern sweden: a case-control study. Scand. J. Rheumatol. 39, 454–460 (2010).
Herndon, S. et al. Top ten tips palliative care clinicians should know about rheumatology. Journal Palliat. Medicine, (2025).
Ramirez, C. T. & Verma, R. K. Early palliative care improves patient and caregiver quality of life. Clin. J. Oncol. Nurs. 28, 496–501 (2024).
Piety, N. Z. & Shevkoplyas, S. S. Paper-Based diagnostics: rethinking conventional sickle cell screening to improve access to High-Quality health care in Resource-Limited settings. IEEE Pulse. 8, 42–46 (2017).
Xu, S. et al. Prevalence and predictability of Low-Yield inpatient laboratory diagnostic tests. JAMA Netw. Open. 2, e1910967 (2019).
Acknowledgements
We gratefully acknowledge the Institute for Health Metrics and Evaluation (IHME) and other organizations for providing access to the GBD data. We also thank our colleagues and reviewers for their constructive feedback and support throughout the research and manuscript preparation process.
Author information
Authors and Affiliations
Contributions
(I) Conception and design: Hong Cheng, Tao Li; (II) Administrative support: Hong Cheng, Tao Li; (III) Provision of study materials or patients: Hong Cheng, Tao Li; (IV) Collection and assembly of data: Hong Cheng, Tao Li, Canxuan Li, Wei Su; (V) Data analysis and interpretation: Hong Cheng, Tao Li, Canxuan Li, Wei Su; (VI) Manuscript writing: Hong Cheng, Tao Li, Canxuan Li, Wei Su; (VII) Final approval of manuscript: Hong Cheng, Tao Li, Canxuan Li, Wei Su.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cheng, H., Li, T., Li, C. et al. Trends and gender disparities in the burden of rheumatoid arthritis in Pakistan from 1990 to 2021. Sci Rep 15, 21667 (2025). https://doi.org/10.1038/s41598-025-05627-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-05627-4
