
Abstract
The trabeculae of the femoral head are organized in response to mechanical forces acting on the bone, becoming increasingly anisotropic with age. This may elevate fracture risk under non-primary loading conditions, such as falls. However, normal trabecular angles and directional patterns have not been fully characterized. This study examined trabecular directionality in 62 proximal femora of 38 cadavers (mean age: 87.2 ± 8.2 years, range: 65–102) using micro-CT scans. Trabecular bone direction and dispersion were measured in coronal slices along the anteroposterior axis. Differences based on side and sex were examined, as well as associations with age and neck-shaft angle. We found that direction and dispersion are side and sex independent, with no significant correlation to age. However, trabecular bone direction in the midcoronal slice, as well as the multi-slice average, showed a significant negative correlation with the neck-shaft angle (r=-0.496 and r=-0.562, respectively, p < 0.001). Furthermore, the multi-slice average demonstrated significantly lower direction and higher dispersion values than those in the single-slice analyses. Nevertheless, the two measurement types were strongly correlated. Moreover, each individual had a unique trabecular pattern, although it followed a common structural blueprint. These findings enhance our understanding of femoral head biomechanics, with implications for orthopedic surgery, implant design, and forensic medicine.
Similar content being viewed by others


Introduction
The intricate structure and adaptive nature of bone tissue are well established in the literature, revealing a complex biological system that optimizes its architecture to withstand mechanical stresses efficiently throughout an individual’s lifetime1,2. This research has long guided orthopedic physicians in the diagnosis and treatment of skeletal pathologies, such as osteoporosis and fractures3. Furthermore, the role of mechanical stress in shaping trabecular and cortical bone4,5,6,7,8,9,10,11,12,13 has implications for many other research areas, including biomechanics, bioengineering, forensic science, and anthropology. Hence, Koch14 described five groups of trabeculae in the proximal femur based on their orientation and mechanical function to resist different forces acting on the femur: principal compressive, principal tensile, secondary compressive, secondary tensile, and greater trochanter groups. Nevertheless, it is debatable whether the tensile trabeculae exclusively transmit tension or function like an arch that transmits compression, or possibly both2,15.
The five groups of trabeculae are characterized by being anisotropic, i.e., each has a unique preferred orientation that can be distinguished from its surrounding trabeculae14,16. Finite element analyses reveal that anisotropic models better capture stress distributions along trabecular groups, emphasizing the role of strongly anisotropic trabeculae like the principal compressive and principal tensile groups17. The principal compressive group, which is relatively vertical, is highly important as it emerges during infancy18,19,20 and is the last to persist in osteoporosis patients18,21,22.
As all trabecular groups except the principal compressive group are gradually lost, the entire femoral head and other regions in the proximal femur become increasingly anisotropic with age23. While a similar principle has been demonstrated in the vertebra24 the implications for this change in the femur are critical. The increased anisotropy in the proximal femur may raise the bone’s vulnerability to fractures under loading conditions that deviate from the main loading direction, such as those experienced during a fall on the hip25. However, once a crack is initiated, the anisotropic architecture may act protectively: resistance to crack propagation is higher across trabeculae than along them, suggesting that the orientation of trabeculae can slow or redirect fracture progression26. Additionally, an increased neck-shaft angle has been previously associated with a higher risk of hip fracture27, yet no study has investigated whether trabecular orientation is associated with the neck-shaft angle.
Moreover, despite this longstanding research, significant gaps remain in our understanding of bone microstructural organization and its relation to function. Specifically, the angular direction of trabecular groups in the femoral head is typically discussed in terms of absolute angles, i.e., relative to the plumbline (e.g.,28,29), rather than anatomical angles relative to other regions of the femur. This approach is limited because it does not explain the relationship between trabecular orientation and other femoral structures, such as the neck and the shaft.
In addition, the load on the superior region of the femoral head varies between subregions, e.g., anterosuperior, superior, and posterosuperior, and is influenced by joint movement and function29,30,31,32,33,34. However, there is no information on how it affects the angle of the principal compressive trabeculae in different areas of the femoral head.
The aims of this study were (1) to determine the directionality of femoral head trabeculae relative to the femoral neck in coronal sections and examine its association with side, sex, age, and neck-shaft angle; (2) to reveal the pattern of directionality change along the anteroposterior axis of the femoral head and evaluate the degree of bilateral symmetry of this pattern; (3) to evaluate the sensitivity of medical imaging tools to identify trabecular bone directionality.
Methods
Materials
The study included the right and left proximal femora of 38 human elderly cadavers (age range: 65–102). The mean age at death was 88.7 ± 8.32 years for males (N = 14) and 86.0 ± 8.07 years for females (N = 24). Due to the advanced age of the donors, most femora exhibited mild age-related degenerative changes, such as small osteophytes and mild cartilage erosion. Femora showing macroscopic signs of severe hip pathology (osteoarthritis, avascular necrosis, or malignancy), those that had undergone hip arthroplasty or fracture repair surgery, and those damaged during dissection were excluded from the study (in total, 14 femora). Accordingly, 62 femora were included in the study. The study was approved by the ethical committee of Tel Aviv University (#0005717-2), and all experiments were conducted in accordance with its guidelines. Before their death, all cadaver donors provided informed consent while in a clear state of mind, with two witnesses present, permitting the use of their bodies for scientific research.
Micro-CT (µCT) scanning and image reconstruction
All proximal femora included in the study were scanned using a microfocus X-ray computed tomography system (XT H 225 ST, Nikon Metrology NV, Leuven, Belgium) operating at 225 kV and 225 W with a reflection target. The scan parameters were a voxel size of 59 μm, 190 kV, and 120 µA. Each scanned femur underwent three-dimensional (3D) reconstruction using Nikon CT Pro 3D software (v. 6.9.1; industry.nikon.com), with default settings – no filters, enhancement or noise reduction – and a level three beam hardening correction. The reconstructed images were saved as a sequence of TIFF image files. To ensure no movement of the bone during scanning, each proximal femur was wrapped in parafilm and embedded in an OASIS® Floral Foam Maxlife block that conformed to its shape.
Positioning and reslicing of the proximal femur
Using a custom Fiji-ImageJ code incorporating available plugins35,36 (Supplementary Code 1), the scanned femora were positioned in a standardized anterior view with the head-neck axis aligned horizontally. Then, the femoral head was resliced in the coronal plane (Fig. 1). An image of the entire proximal femur and an image sequence of the resliced femoral heads were saved for further analyses.

A proximal femur volume positioned in a standardized orientation for measurement, with the femoral head resliced into coronal cross-sections. In the standardized orientation, the head-neck axis is aligned horizontally. Angular measurements obtained from the proximal femur include (a) trabecular bone direction (in degrees), (b) trabecular bone dispersion (in degrees), and (c) the neck-shaft angle (in degrees), which is measured between the midline of the femoral neck and that of the femoral shaft (Supplementary Fig. 3). Trabecular bone direction and dispersion are assessed using preferred orientation analysis with the Fiji-ImageJ Directionality plugin37. This plugin analyzed the preferred orientation within the entire femoral head image (indicated by the white frame).
Simulation of medical imaging scans
To assess the applicability of our directionality analysis methods (see below) to lower-resolution imaging, such as that produced by standard medical CT scans, we simulated reduced resolutions by progressively scaling down the original µCT image sequences to 90%, 80%, 70%, 60%, 50%, 40%, 30%, 20%, and 10% of the original resolution. This was performed using the ‘Scale’ function in Fiji-ImageJ (Supplementary Fig. 1) on a sub-sample of 15 randomly selected individuals.
Directionality analysis
To assess the preferred orientation of femoral head trabeculae we employed the Fiji-ImageJ Directionality plugin37. This tool analyzes the preferred orientation (anisotropy) within an image and provides four key outcomes: (1) direction – an angle between -90° and 90° (Fig. 1a); (2) dispersion – the standard deviation around the direction angle (Fig. 1b); (3) amount – the proportion of structures aligned with the preferred orientation, ranging from 0 to 1; (4) goodness – the accuracy of the returned direction angle in representing the image, ranging from 0 to 1 (i.e., a goodness of fit test). Images with highly isotropic structures yield lower goodness values (Supplementary Fig. 2). In this study, we analyzed the entire femoral head in coronal sections with goodness ≥ 0.8. Sagittal and horizontal sections were excluded due to their low anisotropy (goodness < 0.8).
Directionality outcomes were registered for the midcoronal slice and as the average of the angles measured in all coronal slices (hereafter named averaged multi-slice direction or dispersion). In addition, we examined the pattern of change in direction and dispersion along the femoral head from the most anterior to the most posterior coronal slice by representing it with line graphs (x-axis represented the slice number and y-axis the angle). Before analyzing the data in a multi-slice dimension, we followed these steps: (1) Slices with a goodness score below 0.8 were designated as having no preferred orientation (Supplementary Fig. 2). For such slices, the direction and dispersion were marked as “NaN,” creating a gap in the line graph; (2) Values between -90° to 90° were registered, and those falling outside of this range were converted to fit within it (e.g., 170° was converted into -10°); (3) Slices demonstrating outlier angles were examined. If no trabecular directionality was identified or the angle was affected by other factors, such as local deformity, the slice was removed. This process was relevant, for example, when in a femoral head, only a single slice out of hundreds demonstrated an extreme angle due to a bone deformation appearing only in this slice. Moreover, omitting this slice was negligible, as it represents less than 0.1% of the femoral head. Across the entire sample, only eight slices were removed because of outlier data.
Neck-shaft angle measurement
The angle between the longitudinal midline of the femoral neck and the longitudinal midline of the femoral shaft was measured (Fig. 1c). Measurements were obtained using a custom semi-automatic code in Fiji-ImageJ, based on landmarks placed on the proximal femur (Supplementary Code 2, Supplementary Fig. 3).
Statistical analysis
Statistical analysis was carried out using SPSS 26.0, with a significance threshold (α) set at 0.05.
Intraclass Correlation Coefficient (ICC) was used to evaluate both intra- and inter-rater reliability for the positioning of the proximal femur in a standardized alignment and for neck-shaft angle measurements. To assess intra-rater reliability, the primary researcher rotated 15 femora and measured the neck-shaft angle twice, with a one-week interval between sessions. Rotation around the X, Y, and Z axes, as well as the neck-shaft angle, were recorded. For inter-rater reliability, a second rater repeated the process blindly and independently. Since directionality measurements were carried out automatically using built-in algorithms according to the position of the bone, no further analysis was needed to test their repeatability level.
In the single- and multi-slice analyses, we carried out paired-samples t-tests to examine differences in the measured variables between the right and left femora, as well as to compare the direction and dispersion between the averaged multi-slice and single-slice measurements. Independent samples t-tests were used to examine differences between males and females. These tests were selected based on the normal distribution of the data, confirmed through Kolmogorov-Smirnov tests, Q-Q plots, and histograms. Additionally, Pearson correlation coefficient analyses were conducted to assess correlations between quantitative variables.
To assess the compatibility between femoral heads in direction and dispersion angles along the anteroposterior axis, three methods were used: Pearson correlation coefficient38 dynamic time warping (DTW)39 and profile-based image similarity analysis (PISA) (Supplementary Code 3) in MATLAB, version R2024a.
Specifically, the Pearson correlation coefficient analysis estimated the correlation between the direction or dispersion values between every two femora. Since image processing standardized the starting slice (i.e., the most anterior slice having the femoral cortex), ensured identical slice thickness, and selected all slices with goodness values ≥ 0.8, similar trabecular patterns were expected to yield high Pearson correlation coefficients. Similarly, as the angles were represented as line graphs, DTW attempted to align the line graphs of every two compared femora. This analysis returns a final cumulative alignment cost that reflects the minimum total distance required to align one pattern with another. Accordingly, the lower the costs the greater the similarity. Noteworthy, before applying the Pearson correlation coefficient and DTW, we removed slices with no preferred orientation, smoothed the data using a moving average filter with a window size of 40 data points to minimize small fluctuations that could obscure the underlying pattern of trabecular orientation, and normalized it using min-max scaling. This normalization method transforms the data to a range between 0 and 1 by subtracting the minimum value from each data point and dividing by the range (maximum value minus minimum value).
The PISA quantified similarity between line profiles extracted from the line graph images by combining two measures: the Pearson correlation coefficient (r), which captures the linear similarity in shape between profiles, and the mean squared error (MSE), which captures the average deviation between them. The final similarity score was computed as r×(1 − MSE), yielding values between -1 and 1, where higher values indicate greater similarity. Additionally, PISA was further used to investigate whether patterns of directional change could be identified in lower-resolution images simulating medical imaging scans. Line graphs were generated for each resolution level, and PISA was applied to assess whether a reduced-resolution graph could be correctly matched to the original graph from the same individual.
Results
Reliability of positioning and measurements
The intra- and inter-rater reliability for positioning the proximal femora into a standardized alignment was excellent (0.936 ≤ ICC ≤ 0.998). Also, excellent results were obtained for the neck-shaft angle measurement (0.833 ≤ ICC ≤ 0.884).
Trabecular directionality by side, sex, and age
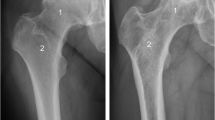
The trabeculae in the midcoronal slice of the femoral head exhibited a distinct preferred orientation (Fig. 2). On average, the right and left femoral heads demonstrated similar direction and dispersion values of the trabeculae, yet in the opposite orientation (right: 31.8°±3.22° and 13.2°±1.64°; left: -32.3°±3.14° and 12.8°±1.94°, respectively). Therefore, on absolute values, no significant differences were found between the sides for direction (p = 0.306), dispersion (p = 0.289), amount (p = 0.182) and goodness (p = 0.957) (Supplementary Table 1). Furthermore, no significant differences were found between the sexes in direction (p ≥ 0.797) and dispersion (p ≥ 0.089) (Supplementary Table 2), nor were there significant correlations between age and direction or dispersion (-0.297 ≤ r ≤ 0.295, p > 0.116). However, a slight trend toward increased orientation with advancing age was observed (Supplementary Fig. 4).

Orientation of the trabecular bone at the midcoronal section of the femoral head. The preferred orientation was colored and estimated as approximately |32°| in the right (a) and left (b) femoral heads.
Comparison of midcoronal single-slice and multi-slice methods
The averaged multi-slice direction was significantly smaller by approximately two degrees than the midcoronal single-slice direction, both on the right and left sides (p < 0.001) (Supplementary Table 3). However, the averaged multi-slice dispersion was significantly larger by approximately two degrees than the midcoronal single-slice dispersion, both on the right and left sides (p < 0.001) (Supplementary Table 3). While the averaged multi-slice direction did not differ significantly between the right and left sides (p = 0.444), the dispersions did (p = 0.044), with the right femora showing slightly higher dispersion values than the left one (Supplementary Table 4). Nevertheless, significant, positive, strong correlations were found between the single- and averaged multi-slice directions (right: r = 0.899; left: r = 0.850, p < 0.001) (Supplementary Fig. 5A). The correlations between the single- and averaged multi-slice dispersion values were strong, yet weaker than those found for the direction angles (right: r = 0.691; left: r = 0.661, p < 0.001) (Supplementary Fig. 5B).
Anteroposterior change in trabecular directionality
The direction and dispersion patterns of the trabeculae along the anteroposterior axis of the femoral head were represented by line graphs. The visual display of the direction variable suggested a unique individual signature-like pattern (Table 1). Quantitative analysis confirmed that the level of symmetry between the left and right femora varied among individuals, with Pearson correlation coefficient (r) ranging from -0.305 to 0.986 (p < 0.050), alignment cost values ranging from 2.040 to 11.250, and PISA scores ranging from -0.338 to 0.877 (Table 1, Supplementary Table 5). Most subjects demonstrated moderate to high symmetry in the trabecular direction when evaluated using Pearson correlation and alignment cost. However, based on the PISA, the majority exhibited low to moderate symmetry levels (Supplementary Fig. 6).
The dispersion variable also displayed a unique anteroposterior change pattern for each femur. However, there was a considerable resemblance between subjects, posing a challenge in distinguishing one subject from another. Quantitative analysis of the symmetry levels between the right and left femora of the same individual revealed high symmetry in most individuals when evaluated using Pearson correlation (0.563 ≤ r ≤ 0.998, p < 0.050) and PISA (between 0.012 and 0.976), but not when evaluated by alignment cost (between 0.497 and 5.881) (Table 2, Supplementary Table 6, Supplementary Fig. 6).
Nevertheless, there is a common pattern of direction characterizing all individuals, appearing as an inverted U-shaped curve (Fig. 3a,b). Accordingly, on average, the direction angle of the trabeculae in the femoral head increases towards the midcoronal section. Then, it decreases, reaching a smaller angle in the posterior aspect of the femoral head than in the anterior aspect. The change in the dispersion is the opposite, creating a U-shaped curve (Fig. 3c, d). This signifies that trabeculae not in the preferred orientation tend to converge towards the preferred orientation in the midcoronal area of the femoral head and disperse as they move more anterior or posterior. Moreover, dispersion at the posterior aspect is larger than in the anterior aspect of the femoral head (Fig. 3c-d). An animation exhibiting the change in direction and dispersion in one subject is provided (Supplementary Animation 1).

Average direction (a,b) and dispersion (c,d) in each coronal section along the anteroposterior axis of the femoral head, in the entire cadaver sample. Changes in direction (a) and dispersion (c) are presented for all subjects (colored lines) and as an average (black line; a-d). An inverted U-shaped curve is observed for direction, while a U-shaped curve is seen for dispersion.
When comparing the direction and dispersion patterns of one femur with all other femora, we expected the highest Pearson correlation and PISA values and the lowest alignment cost would be observed with the contralateral femur of the same individual, rather than with femora from other individuals. However, this was the case for only 4-18% of the femora, depending on the variable tested (direction or dispersion) and the outcome measure (Pearson correlation coefficient, alignment cost, or PISA score) (Supplementary Table 7). This indicates significant similarities between distinct subjects, often surpassing the similarities within the subject itself. Notably, only one subject showed a complete match, where the left femur had the highest Pearson correlation and PISA values, and the lowest alignment cost when compared to the right femur, and vice versa.
Diagnostic capability of contemporary imaging tools
Low resolution images mimicking contemporary medical CT scans (Supplementary Fig. 1), failed to accurately depict patterns of directionality change. For the original resolution, the PISA identification success rate was 100% both in the raw and smoothed data. Also, for scans with 90% and 80% of the original resolution, the methods had no major effect on the identification success rate. In these scans, the success rate is reduced to 93%; nevertheless, for the one individual identified incorrectly in the 90% resolution scan, it was the second choice, and in the 80% resolution scan, the second or third choice. When the resolution was further reduced, the analysis of smoothed data mostly improved the success identification rate. In 70% resolution, the success identification rate was 87%, with the correct identification in the two individuals identified incorrectly being within the top five options. In 60% resolution, the success identification rate was 73%, with four individuals identified incorrectly. Among these four individuals, the correct identification of two was within the top 10 options, and for the other two above 10. When the resolution was reduced by half or more, the success identification rate was 53% and lower (Supplementary Table 8).
Trabecular directionality and the neck-shaft angle
The average neck-shaft angle in the sample was 125.8 ± 5.59, with a significant difference between the right (126.8 ± 5.54) and left sides (124.5 ± 4.97; p = 0.007). Nevertheless, it did not correlate with age (right: r=-0.094, p = 0.585; left: r=-0.063, p = 0.750) and was sex-independent (Supplementary Table 9). Notably, males exhibited a higher mean value in the right femur and a lower value in the left femur compared to females, though this difference did not reach statistical significance. A significant moderate negative correlation was found between the neck-shaft angle and the midcoronal single-slice direction (r=-0.496, p < 0.001) and averaged multi-slice direction (r=-0.562, p < 0.001) (Fig. 4).

Scatter plots for the neck-shaft angle and trabecular single-slice direction (a), and the averaged multi-slice direction (b), in the entire sample.
Discussion
Analysis of trabecular bone is crucial for improving our understanding of load distribution in health, injury, disease, and healing processes. In this study, we demonstrated the directionality of trabeculae in the femoral head through both single- and multi-slice analyses conducted on cadavers. A better understanding of the trabecular directionality is clinically significant as it may lead to better surgical treatment of hip fractures2 and enhanced risk assessment for fracture initiation22 and propagation26. Specifically, it can guide the placement of screws, plates, or other internal fixation devices. Additionally, it can improve the design of hip implants and prosthetics, as devices that replicate the natural alignment of trabeculae may potentially achieve better integration, distribute stress more effectively, and reduce the risk of complications. Furthermore, if technological advances enable the examination of trabecular micro-architecture in vivo, clinicians could apply personalized medicine by identifying abnormality or weakness in specific bone areas and customizing interventions to match each patient’s unique anatomy and risk profile.
A key insight from our findings is that direction and dispersion in a single midcoronal slice correlate with multi-slice measurements but exhibit systematic biases: direction is overestimated by ~ 2° (more vertical), while dispersion is underestimated by ~ 2° (more converged). This underscores the necessity of multi-slice assessments for a more comprehensive analysis of the femoral head and other skeletal elements (e.g.,40,41). Right and left femora demonstrated symmetrical trabecular directionality, aligning with the expected bilateral symmetry of normal biological structures42,43, and supporting previous studies that confirm femoral symmetry across various parameters44,45,46,47,48, except for anteversion angle46. Despite well-documented anatomical sexual dimorphism49,50,51,52,53,54, which is associated with variations in hip joint kinematics and kinetics55, we found that, in older adults, trabecular direction and dispersion were sex-independent. Furthermore, as we expected for an elderly sample (> 65 years), the trabecular direction showed no correlation with age across the cohort, suggesting stability of trabecular orientation in advanced age, as reported previously56. Nonetheless, this result can also be due to a bias related to the high mean age of the sample and the low age variance (mean ± SD: 87.2 ± 8.2), limiting the statistical power to detect subtle age-related trends in the elderly cohort.
Expanding on the multi-slice analysis, we identified a consistent anteroposterior pattern in elderly humans. In the midcoronal region of the femoral head, trabeculae exhibited an upward pitch of approximately two degrees and converged toward a preferred orientation. This pattern likely reflects the cumulative alignment of individual trabeculae adopting a more vertical orientation in this region. From a biomechanical perspective, as each trabecula aligns more closely with the resultant forces generated by body weight and muscle activity, the torque exerted on it is reduced. This alignment may substantially enhance the femoral head’s resistance to the primary loads placed on the joint14. Additionally, as shown in Fig. 3, direction values in the posterior region of the femoral head were slightly lower than those in the anterior region. A recent anatomical study57 may help explain this finding, having identified that the principal tensile trabeculae comprise both anterior and posterior components. Although that study did not measure the direction angle relative to the head–neck axis as we did, it clearly demonstrates that the posterior component exhibits a lower direction angle than the anterior component. This aligns with our findings.
Despite the shared pattern, the multi-slice analysis also suggested that trabecular organization is unique in each individual, creating a signature-like graphical pattern. This personal signature has potential applications in personalized orthopedic medicine for assessing fracture risk or adjusting an optimal treatment, as well as serving as a secondary identifier in forensic anthropology. Since trabecular bone morphology is shaped by both genetic and environmental factors unique to each individual58,59,60, it may provide supplementary identification data. However, as a secondary identifier, it is inherently less definitive than DNA or fingerprints. Therefore, the development of reliable and validated protocols is crucial to improving its applicability and identification success rate61.
While our findings offer valuable insights, imaging resolution remains a limiting factor for trabecular directionality assessments in clinical settings. Our reduced-resolution images, designed to approximate contemporary medical CT scans, failed to capture the finer details of trabecular orientation, indicating that current medical CT resolution is insufficient for analyses of this kind. However, recent advancements in imaging technology have improved resolution while maintaining low radiation exposure62,63. Moreover, the integration of deep learning reconstruction and artificial intelligence in image processing has been shown to enhance image resolution without increasing radiation exposure or requiring the development of new imaging technologies64,65. As a result, high-resolution imaging techniques are expected to become increasingly prevalent in routine clinical practice. This underscores the growing importance of developing and refining such technologies to support their full integration into medical applications.
Our study also documented asymmetry in the neck-shaft angle, which aligns with some studies66,67,68,69, but contradicts others70,71. Additionally, we showed a negative correlation between trabecular direction and the neck-shaft angle which is known to decreases with age during youth19 but not in older ages72. This suggests that in early life, a decreasing neck-shaft angle is offset by an increasing trabecular direction to maintain vertical orientation – a hypothesis that requires validation in younger cohorts. In our elderly sample, trabecular direction increased as the neck-shaft angle decreased, and conversely, it decreased with higher neck-shaft angles, suggesting adaptive remodeling to maintain a consistent load orientation. Assuming that trabecular direction is determined by joint loading4,5,6,7,8,9,10,11,12,13,20 and that these loads consist of body weight, muscular forces, and the joint reaction force73,74, it is likely that the trabecular direction observed in this study (approximately 30° from the anatomical axis of the femoral neck) represents the action line of the joint reaction force and the resultant vector of body weight and muscular forces. If true, the trabeculae can serve as an easily visible anatomical indicator, pointing to the main direction of load on the joint. This insight could be valuable for clinicians when assessing whether patient pathology aligns with normal or abnormal load distributions.
The primary limitation of this study is the narrow age range of the sample. Because we used µCT scans to maximize the information on the trabecular organization, our sample was restricted to cadavers from the dissection laboratory, which consists of older individuals. Consequently, the generalization of our results to younger cohorts is limited.
To conclude, trabecular directionality in the femoral head of older adults is independent of side, sex, and age. Nevertheless, it varies along the anteroposterior axis and negatively correlates with the neck-shaft angle. While a common general pattern of change in trabecular directionality can be traced in the femoral head, each person also demonstrates a unique individual signature. Therefore, with the advancement in medical imaging to enable the examination of trabecular microarchitecture in living patients, the applications of this method can be relevant for clinicians to apply personalized medicine and assess fracture risk and for forensic anthropologists for personal identification.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request. The Supplementary materials cited in this article can be found at https://osf.io/gqmw4/files/osfstorage?view_only=f750a1a531394d30827ca5cd631f66c5.
References
Bartoníček, J. & Naňka, O. Early history of the study of bone growth (1722–1875). Int. Orthop. 48, 1915–1922 (2024).
Wang, H. et al. Biomechanical properties and clinical significance of cancellous bone in proximal femur: A review. Injury 54, 1432–1438 (2023).
Buckley, R. E., Moran, C., Apivatthakakul, T. & G. & AO Principles of Fracture Management Third Edition (AO Foundation, 2017).
Chen, J. H., Liu, C., You, L. & Simmons, C. A. Boning up on wolff’s law: mechanical regulation of the cells that make and maintain bone. J. Biomech. 43, 108–118 (2010).
Ruff, C., Holt, B. & Trinkaus, E. Who’s afraid of the big bad wolff?? ‘Wolff’s law’ and bone functional adaptation. Am. J. Phys. Anthropol. 129, 484–498 (2006).
Weinans, H., Huiskes, R. & Grootenboert, H. J. The behavior of adaptive bone-remodeling simulation models. 25, 1425–1441 (1992).
Sugiyama, T., Price, J. S. & Lanyon, L. E. Functional adaptation to mechanical loading in both cortical and cancellous bone is controlled locally and is confined to the loaded bones. Bone 46, 314–321 (2010).
Frost, H. M. Skeletal structural adaptations to mechanical usage (SATMU): 1. Redefining wolff’s law: the bone modeling problem. Anat. Rec. 226, 403–413 (1990).
Willie, B. M. et al. Diminished response to in vivo mechanical loading in trabecular and not cortical bone in adulthood of female C57Bl/6 mice coincides with a reduction in deformation to load. Bone 55, 335–346 (2013).
Barak, M. M. Cortical and trabecular bone modeling and implications for bone functional adaptation in the mammalian tibia. Bioengineering 11 (2024).
Pearson, O. M. & Lieberman, D. E. The aging of wolff’s ‘law’: ontogeny and responses to mechanical loading in cortical bone. Yearb Phys. Anthropol. 47, 63–99 (2004).
Carter, M. I. & Hinton, P. S. Physical activity and bone health. Mo Med. 111, 59–64 (2014).
Wolff, J. Das gesetz der transformation der Knochen. DMW-Deutsche Medizinische Wochenschrift. 19, 1222–1224 (1892).
Koch, J. C. The laws of bone architecture. Am. J. Anat. 21, 177–298 (1917).
Rudman, K. E., Aspden, R. M. & Meakin, J. R. Compression or tension? The stress distribution in the proximal femur. Biomed Eng. Online 5 (2006).
Enns-Bray, W. S., Owoc, J. S., Nishiyama, K. K. & Boyd, S. K. Mapping anisotropy of the proximal femur for enhanced image based finite element analysis. J. Biomech. 47, 3272–3278 (2014).
Wronski, S., Wit, A., Tarasiuk, J. & Lipinski, P. The impact of the parameters of the constitutive model on the distribution of strain in the femoral head. Biomech. Model. Mechanobiol. 22, 739–759 (2023).
Osborne, D., Effmann, E., Broda, K. & Harrelson, J. The development of the upper end of the femur, with special reference to its internal architecture. Radiology 137, 71–76 (1980).
Ding, K. et al. Age-related changes with the trabecular bone of ward’s triangle and neck-shaft angle in the proximal femur: a radiographic study. Orthop. Surg. 15, 3279–3287 (2023).
Djurić, M., Milovanović, P., Djonić, D., Minić, A. & Hahn, M. Morphological characteristics of the developing proximal femur: A Biomechanical perspective. Srp Arh Celok Lek. 140, 738–745 (2012).
Singh, M., Nagrath, A. & Maini, P. S. Changes in trabecular pattern of the upper end of the femur as an index of osteoporosis. JBJS 52, 457–467 (1970).
Tanck, E. et al. Predictive value of femoral head heterogeneity for fracture risk. Bone 44, 590–595 (2009).
Cui, W. Q. et al. Age-and region-dependent changes in three-dimensional microstructural properties of proximal femoral trabeculae. Osteoporos. Int. 19, 1579–1587 (2008).
Mc Donnell, P., Mc Hugh, P. E. & O’Mahoney, D. Vertebral osteoporosis and trabecular bone quality. Ann. Biomed. Eng. 35, 170–189 (2007).
Ciarelli, T. E., Fyhrie, D. P., Schaffler, M. B. & Goldstein, S. A. Variations in three-dimensional cancellous bone architecture of the proximal femur in female hip fractures and in controls. J. Bone Mineral. Res. 15 (2000).
Adams, G. J., Cook, R. B., Gibson, M. & Zioupos, P. Predicting the fracture toughness of human cancellous bone in fractured neck of femur patients using bone volume and micro-architecture. Life 14 (2024).
Fajar, J. K., Taufan, T., Syarif, M. & Azharuddin, A. Hip geometry and femoral neck fractures: A meta-analysis. J. Orthop. Translat. 13, 1–6 (2018).
Freeman, M. A. R. Some anatomical and mechanical considerations relevant to the surface replacement of the femoral head.
Chiba, K., Burghardt, A. J., Osaki, M. & Majumdar, S. Heterogeneity of bone microstructure in the femoral head in patients with osteoporosis: an ex vivo HR-pQCT study. Bone 56, 139–146 (2013).
Afoke, N., Byers, P. & Hutton, W. Contact pressures in the human hip joint. J. Bone Joint Surg. 69-B, 536–541 (1987).
Hoechel, S., Alder, M., Wirz, D. & Müller-Gerbl, M. The human hip joint and its long-term load intake – How X-ray density distribution mirrors bone strength. HIP Int. 23, 583–589 (2013).
Georgiou, L., Kivell, T. L., Pahr, D. H., Buck, L. T. & Skinner, M. M. Trabecular architecture of the great ape and human femoral head. J. Anat. 234, 679–693 (2019).
Greenwaldt, A. S. & O’connor, J. J. The transmission of load through the human hip joint. J. Biomech. 4, 507–528 (1971).
Carter, D. R., Rapperport, D. J., Fyhrie, D. P. & Schurman, D. J. Relation of coxarthrosis to stresses and morphogenesis: A finite element analysis. Acta Orthop. 58, 611–619 (1987).
Schmid, B. 3Dscript - Create high-quality 3D/4D animations using a natural-language based syntax. https://imagej.net/imagej-wiki-static/3Dscript
Meijering, E. TransformJ: An ImageJ plugin suite for geometrical image transformation. https://imagescience.org/meijering/software/transformj/
Tinevez, J. Y. Directionality. https://imagej.net/plugins/directionality
Goshtasby, A. A. Similarity and dissimilarity measures. Adv. Pattern Recognit. 7–66. https://doi.org/10.1007/978-1-4471-2458-0_2 (2012).
Wang, Q. Dynamic time warping (DTW). https://github.com/wq2012/dynamic_time_warping/releases/tag/v2 (2023).
Reznikov, N., Almany-Magal, R., Shahar, R. & Weiner, S. Three-dimensional imaging of collagen fibril organization in rat circumferential lamellar bone using a dual beam electron microscope reveals ordered and disordered sub-lamellar structures. Bone 52, 676–683 (2013).
Reznikov, N., Shahar, R. & Weiner, S. Three-dimensional structure of human lamellar bone: the presence of two different materials and new insights into the hierarchical organization. Bone 59, 93–104 (2014).
Holló, G. Demystification of animal symmetry: Symmetry is a response to mechanical forces. Biol Direct 12 (2017).
Johnston, I. G. et al. Symmetry and simplicity spontaneously emerge from the algorithmic nature of evolution. Proc. Natl. Acad. Sci. USA 119 (2022).
Young, E. Y., Gebhart, J., Cooperman, D. & Ahn, N. U. Are the left and right proximal femurs symmetric? Basic research. Clin. Orthop. Relat. Res. 471, 1593–1601 (2013).
Banse, X., Delloye, C. & Bourgoist, R. Comparative left-right mechanical testing of cancellous bone from normal femoral heads. J. Biomechonics. 29, 1247–1253 (1996).
Eckhoff, D. G. et al. Bilateral symmetrical comparison of femoral and tibial anatomic features. J. Arthroplasty. 31, 1083–1090 (2016).
Young, E. Y., Gebhart, J. J., Bajwa, N., Cooperman, D. R. & Ahn N. U. Femoral head asymmetry and coxa magna: Anatomic study (2013).
Bakhshayesh, P., Sandberg, O., Kumar, V., Ali, A. & Enocson, A. Volume fusion of CT images to measure femoral symmetricity. Surg. Radiol. Anat. 42, 635–639 (2020).
Fischer, B. & Mitteroecker, P. Allometry and sexual dimorphism in the human pelvis. Anat. Rec. 300, 698–705 (2017).
Patriquin, M. L., Steyn, M. & Loth, S. R. Metric analysis of sex differences in South African black and white Pelves. Forensic Sci. Int. 147, 119–127 (2005).
Nakahara, I. et al. Gender differences in 3D morphology and bony impingement of human hips. J. Orthop. Res. 29, 333–339 (2011).
Kanz, F., Fitzl, C., Vlcek, A. & Frommlet, F. Sex Estimation using the femur of Austrians born in the 19th to the middle of the 20th century. Anthropol. Anz. 72, 117–127 (2015).
Eckstein, F. et al. Sex differences of human trabecular bone microstructure in aging are site-dependent. J. Bone Miner. Res. 22, 817–824 (2007).
Lochmüller, E. M. et al. Site-specific deterioration of trabecular bone architecture in men and women with advancing age. J. Bone Miner. Res. 23, 1964–1973 (2008).
Galmiche, R., Migaud, H. & Beaulé, P. E. Hip anatomy and biomechanics relevant to hip replacement. in Personalized Hip and Knee Joint Replacement (eds Rivière, C. & Vendittoli, P. A.) 9–22 (Springer, 2020).
Whitmarsh, T. et al. A cross-sectional study on the age-related cortical and trabecular bone changes at the femoral head in elderly female hip fracture patients. Sci. Rep. 9 (2019).
Zhang, J. F. et al. The qualitative analysis of trabecular architecture of the proximal femur based on the P45 sectional plastination technique. J. Anat. https://doi.org/10.1111/joa.14210 (2025).
Judex, S., Garman, R., Squire, M., Donahue, L. R. & Rubin, C. Genetically based influences on the site-specific regulation of trabecular and cortical bone morphology. J. Bone Miner. Res. 19, 600–606 (2004).
Bjørnerem, Å. et al. Genetic and environmental variances of bone microarchitecture and bone remodeling markers: A twin study. J. Bone Miner. Res. 30, 516–524 (2015).
Ho-Pham, L. T., Hans, D., Doan, M. C., Mai, L. D. & Nguyen, T. V. Genetic determinant of trabecular bone score (TBS) and bone mineral density: A bivariate analysis. Bone 92, 79–84 (2016).
Blau, S. et al. Re-examining so-called ‘secondary identifiers’ in disaster victim identification (DVI): Why and how are they used? Forensic Sci. Int 345 (2023).
Hussain, S. et al. Modern diagnostic imaging technique applications and risk factors in the medical field: A review. BioMed Res.Int. https://doi.org/10.1155/2022/5164970 (2022).
Pacult, M. A., Walker, C. T., Godzik, J., Turner, J. D. & Uribe, J. S. Emerging Technologies in Spinal Surgery: Ultra-Low Radiation Imaging Platforms. Operative Neurosurgery 21, S39–S45. https://doi.org/10.1093/ons/opaa324 (2021).
Wang, T. J. et al. Deep learning reconstruction improves the image quality of low-dose Temporal bone CT with otitis media and mastoiditis patients. Heliyon 10 (2024).
Clement David-Olawade, A. et al. AI-driven advances in low-dose imaging and enhancement—a review. Diagnostics 15. https://doi.org/10.3390/diagnostics15060689 (2025).
Zaghloul, A. Computing measurements of femoral neck shaft angle in children and adolescents from nile Delta. Orthopedics Rheumatol. Open. Access. J. 17 (2020).
Gilligan, I., Chandraphak, S. & Mahakkanukrauh, P. Femoral neck-shaft angle in humans: variation relating to climate, clothing, lifestyle, sex, age and side. J. Anat. 223, 133–151 (2013).
Kumar, V. & Gajbhiye, V. M. A comparative study of neck shaft angle of femur in Madhya Pradesh. Int. J. Health Sci. (Qassim) 1–7. https://doi.org/10.53730/ijhs.v6ns2.4983 (2022).
Fischer, C. S. et al. The neck–shaft angle: an update on reference values and associated factors. Acta Orthop. 91, 53–57 (2020).
Mohamad Khan, S. & Shaik, H. S. Study on neck shaft angle and femoral length of South Indian femurs. Int. J. Anat. Res. 2, 633–635 (2014).
Haddad, B. et al. Femoral neck shaft angle measurement on plain radiography: Is standing or supine radiograph a reliable template for the contralateral femur? BMC Musculoskelet. Disord 23 (2022).
Clinger, B. N. et al. Differences in CT scan measurements of femoral neck shaft angle and acetabular version among sex, age, and ethnicity from a large cadaveric database. WJO 12, 67–71 (2023).
Martin, R. B., Burr, D. & Sharkey, N. A. Skeletal Tissue Mechanics (Springer, 1998).
Neumann, D. A. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation (Elsevier, 2018).
Acknowledgements
We sincerely thank Prof. David Elad and Christos Damalas for their valuable insights, and the Gerda Henkel Foundation which made this study possible.
Funding
This study is part of Amit Hadad’s PhD thesis which is supported by grant #AZ 06/F/22 from the Gerda Henkel Foundation. The funding organization had no role in the design or conduct of this research.
Author information
Authors and Affiliations
Contributions
AH: Collection and assembly of data, analysis and interpretation of data, drafting of the article. All authors: Conception and design, critical revision of the article for important intellectual content, final approval of the article.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hadad, A., Bar-Ziv, Y. & May, H. New insights on femoral head trabecular bone directionality in elderly humans using a micro-CT-based analysis. Sci Rep 15, 24228 (2025). https://doi.org/10.1038/s41598-025-05991-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-05991-1
