
Abstract
Current assessment of preoperative deep vein thrombosis (DVT) in elderly patients with femoral neck fracture is limited. We aimed to identify independent risk factors for preoperative DVT in patients with femoral neck fracture and to develop and validate a predictive nomogram. Patients diagnosed with femoral neck fracture from October 2014 to April 2019 were retrospectively analyzed. Baseline data, treatment information and laboratory test results were collected, and the occurrence of DVT in the preoperative period was regarded as the study outcome event. Multivariable logistic regression identified independent risk factors associated with a higher incidence of preoperative DVT. The predictive nomogram was constructed based on the analysis results. The stability of the model was further assessed in this study using patients from May 2019 to September 2022 as an external validation set. A total of 921 patients were enrolled in the study, of which 639 were used in the training cohort and the other 282 for the validation cohort. Multivariate analysis revealed age (OR 1.100, 95% CI 1.042–1.162), BMI ≥ 28 (OR 3.969, 95% CI 1.792–8.793), smoking (OR 2.998, 95% CI 1.255–7.165), LDL-C > 3.4 mmol/L (OR 2.628, 95% CI 1.316–5.250), and d-dimer > 0.475 mg/L (OR 3.157, 95% CI 1.565–6.368) were the independent risk factors of preoperative DVT. The concordance index (C-index) of the nomogram were 0.832 in the training set, and the corrected values after internal validation were 0.759. The receiver-operating characteristic (ROC) curve, the calibration curve, the Hosmer–Lemeshow test and the decision curve analysis (DCA) performed well in both the training and validation cohorts. In this study, we developed a personalised predictive nomogram containing five high-risk factors, which can help surgeons stratify the risk of preoperative DVT in elderly patients with femoral necks and guide high-risk patients to ultrasound scans or prophylactic anticoagulation as soon as possible.
Similar content being viewed by others


Introduction
Femoral neck fractures remain one of the most catastrophic fragility fractures among the elderly, accounting for 40–50% of all hip fractures and nearly 30% die within a year1. A large body of reliable evidence suggests that early surgery is effective in reducing the risk of perioperative complications and death and significantly improves prognosis2,3,4. However, once deep vein thrombosis (DVT) occurs in the lower limbs, patients have to undergo aggressive and long-term thrombolytic therapy and repeated ultrasound scans, which often leads to missed optimal treatment time, heavy psychological stress, and high medical costs5. Worse still, accidental thrombus displacement can lead to other vascular diseases such as pulmonary embolism (PE) or even death6. Unfortunately, the vast majority of DVT events are extremely insidious and difficult to diagnose early, making timely treatment difficult. Due to the ageing population, the estimated number of hip fracture patients worldwide has increased exponentially, meaning that more and more elderly patients will face the severe challenge of preoperative DVT7.
Due to coexisting medical conditions, complex comorbidities and various risk factors, elderly patients with femoral neck fracture are predisposed to developing venous thromboembolism events. However, current clinic guidelines mainly focus on the prevention of postoperative DVT in fracture repair8,9. Only a few studies have looked at preoperative DVT events in patients with femoral neck fracture. The reported rates of preoperative DVT in elderly patients with femoral neck fracture were considerable, ranging from 6.8 to 18.2%10,11. A retrospective study by Niu et al. reported the related risk factors of DVT in elderly patients with femoral neck fractures, including renal insufficiency, smoking, time from injury to duplex ultrasonography (DUS) and platelet (PLT)10. Indeed, considering risk factors in isolation makes it almost impossible to determine the actual likelihood of a patient developing DVT. Later, through the review of 203 older subjects, Chen et al. identified independent risk factors for DVT occurrence and then roughly develop a simple prediction formula11. However, they acknowledged that characters of small sample design and their many remaining confounding greatly limit the practical clinical application. Currently, there is an urgent need for an efficient and accurate decision-making tool to help identify people at high risk of DVT. By defining risk factors associated with preoperative DVT and establishing a personalized predictive model for early targeted intervention, it is a promising strategy to improve the prognosis of elderly patients with femoral neck and reduce healthcare burden.
In view of the above, this study aimed to define the incidence and risk factors of preoperative DVT in elderly patients with isolated femoral neck fracture using a large sample and to establish and validate a predictive nomogram.
Materials and methods
Ethical issue
This retrospective cohort study was approved by the Ethics Committee of the Hebei Medical University Third Hospital. All procedures were performed in accordance with the tenets of the Declaration of Helsinki and the Strengthening the Reporting of Surgical Cohort Studies (STROCSS) guidelines. All participants or their immediate family members were informed and signed an informed consent form.
Participants and data collection
We retrospectively collected hospitalized patients 60 years or older who were admitted at the Third Hospital of Hebei Medical University due to unilateral femoral neck fractures from October 2014 to April 2019. Patients were not considered in the study when there was : (1) incomplete study data, including no documentation of any DVT examination and incomplete medical records; (2) high-energy injuries; (3) open fractures; (4) multiple fractures; (5) pathological fractures; (6) old fractures; (7) past peripheral vascular disease; (8) recent anticoagulant therapy (Fig. 1).

Patients selection flow-chart.
The data of this study mainly included demographics, medical comorbidities, surgical information, and laboratory biomarkers. The demographic data comprised the age, gender(male or female), bad addiction (cigarette smoking or drinking), residence (rural or urban), height, and weight. BMI was calculated from height in meters and weight in kilograms. Comorbidities included hypertension, diabetes mellitus, heart disease, cerebrovascular disease, lung disease, liver disease, previous surgery, and history of allergy. Treatment information variables included fracture type (based on Garden classification), time from injury to admission and to DUS scan, and ASA score. Laboratory biomarkers included red blood cell count (RBC), hematocrit (HCT), hemoglobin concentration (HGB), platelet count (PLT), platelet to hemoglobin ratio (PHR), white blood cell count (WBC); level of total protein (TP), albumin (ALB), globulin (GLOB), hypersensitive C-reactive protein (HCRP), triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), alanine aminotransferase (ALT), aspartate aminotransferase (AST), fibrinogen (FIB), D-dimer level, prothrombin time (PT), activated partial thromboplastin time (APTT), and thrombin time (TT). If the patient underwent more than one haematological test before being diagnosed with DVT, we chose the test closest to the diagnosis.
The Surgical Site Infection in Orthopaedic Surgery (SSIOS) database provided all data for this study. This is a manually maintained database of all data on hospitalised patients who have undergone orthopaedic surgery at our institution since 1 October 2014, updated annually12,13. Our institution is a teaching hospital and the largest tertiary referral medical centre for orthopaedic trauma in a province in central China (covering a population of more than 75.9 million), performing 45,000–50,000 orthopaedic surgeries per year. All study data are collected manually by more than 200 investigators with standardised training and updated annually; the database has provided data support for many previous studies1,14,15,16,17. The information is more accurate than the administrative databases because it is manually collected and updated. Therefore, the quality and accuracy of the data analysed in this study can be considered high. In addition, to build a clinical prediction model, the sample size should be at least 10 times the number of variables18,19. A total of 40 variables were included in this study, and the sample size should be at least 400, so we included enough patients.
Diagnosis of DVT
In accordance with our standard management strategy, every elderly patient with femoral neck fracture underwent ultrasound as early as possible after admission to the hospital. The definitive diagnosis of preoperative DVT was confirmed by three ultrasonographers with more than 10 years of experience in the field. Duplex ultrasonography (DUS) of bilateral lower extremity veins (common femoral vein, superficial femoral vein, deep femoral vein, popliteal vein, anterior tibial vein, posterior tibial vein and peroneal vein) was performed to determine the presence of DVT. The diagnosis of DVT was strictly according to the Guidelines for Diagnosis and Treatment of DVT (3rd edition) proposed by the Chinese Medical Association. The diagnostic criteria were direct visualisation of the intraventricular thrombus, loss or non-compressibility of the vein, luminal filling defect, lack of respiratory variation in above-knee vein segments, and inadequate flow augmentation to the lower extremity with compression manoeuvres. Superficial veins (great or small saphenous veins) or intramuscular veins (e.g. soleal or gastrocnemius veins) were not included in this study due to their low clinical significance.
Statistical analysis
All statistical analyses of this study were conducted with the Statistical Package for Social Sciences (SPSS) software (version 26.0, Chicago, USA). Categorical variables were presented as numbers and percentages. The Pearson chi-squared test was used for comparisons, and the Fisher exact test was used when the number of groups was < 5. Continuous variables are presented as mean and standard deviation. If normally distributed, the Student t test was used to compare means. If not, the non-parametric Mann-Whitney U test was used to compare medians. Significant differences were defined as P < 0.05. The D-dimer level has been shown in the literature to be associated with DVT, but its elevated level may be influenced by other factors such as trauma, so in our study the Youden index was used to identify the optimal cut-off point. Multivariate logistic regression analysis was performed for variables with P < 0.05 in univariate analysis, and independent risk factors for DVT were determined using backward stepwise regression.
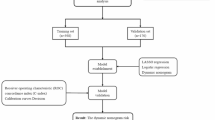
The ‘rms’ package in the R software (version 4.3.2, R Foundation for Statistical Computing, Vienna, Austria) was run to build the nomogram. The C-index and Brier score were calculated and the ROC curve, calibration curve and decision curve analysis (DCA) were plotted to visualise the combined performance of the model. The closer the C-index and the area under the curve (AUC) to 1, the better the discriminatory power of the model. The calibration curve was used to measure the accuracy of the absolute risk prediction value of the model and was further assessed using the Hosmer-Lemme-Show goodness-of-fit test. The Brier score can be interpreted as an extension of the Hosmer-Lemeshow test: the closer to 0, the better the model calibration. The DCA was used to assess the value of the clinical application of the model. Within a certain threshold range, the DCA of the model is higher than All and None, indicating that the net benefit of the model is higher than that of the extreme strategy (all treatment or no treatment), and has clinical application value. The bootstrap method was then used for internal validation to obtain the corrected C-index and corrected Brier score after 1000 sampling repetitions. Finally, the model was externally validated. The final model retained variables with P < 0.10, and the two-tailed P < 0.05 was considered statistically significant.
Results
Demographic data
On the basis of exclusion criteria, 921 of the 1064 elderly patients with femoral neck fracture were enrolled in this study, of which 639 were used as a training set (Fig. 1). In the training cohort, 301(47.1%) were male and 338 (52.9%) were female; the mean age was (65.93 ± 5.04) years (Table 1). After excluding blood clots in 31 (4.9%) intermuscular veins, 42 patients were identified to have a preoperative DVT in the training set, indicating a prevalence of 6.6%. DVTs were distributed in the common femoral vein in 5 (11.9%, 5/42), the popliteal vein in 6 (14.3%, 6/42), the anterior/posterior tibial vein in 24 (57.1%, 24/42), and the peroneal vein in 7 (16.7%, 7/42). All DVT patients were asymptomatic.
Univariate and multivariate analysis
By analyzing the Youden index, the optimal cut-off value for d-dimer to predict preoperative DVT was 0.475 mg/L. After univariate analysis, eight potential predictors were identified in all variables. In multivariate analysis, these variables were selected using backward stepwise regression, and the results showed that age, BMI ≥ 28, smoking, LDL-C > 3.4 mmol/L, d-dimer > 0.475 mg/L were the independent risk factors for the development of preoperative DVT in elderly patients with femoral neck fracture (Table 2).
Construction and validation of an individualized prediction model
The predictive nomogram was constructed based on the results of multifactorial analysis for more intuitive and convenient clinical application (Fig. 2). The AUC was 0.759 (95% CI 0.679–0.839), with sensitivity and specificity (66.0% and 81.1%), which demonstrated the excellent discriminative capacity of the model. The C-index and Brier score were 0.759 and 0.060, respectively (Fig. 3). After internal Bootstrap validation (B = 1000 repetitions), the correction values were 0.748 and 0.057, respectively, indicating that the model performed overall satisfactorily. The Hosmer-Lemeshow χ2 statistic of the calibration curve in the training and test data sets showed a favourable agreement between the probability of predicting preoperative DVT and the actual probability of occurrence in patients with femoral neck fracture (Fig. 4). Furthermore, the discriminatory power of the model performs equally well in the external validation dataset, with an AUC of 0.774.

Nomogram for predicting preoperative DVT in patients with femoral neck fracture. Five factors were calculated into the preoperative DVT prediction nomogram, with each predictor assigned a given score on the top points axis, and the predicted probability of DVT corresponding to the total points was shown on the bottom probability axis.

Receiver-operating characteristic (ROC) curves for the nomogram in the training (a) and validation sets (b). The predictive accuracy of the nomogram was positively correlated with the area under the curve (AUC). The AUC of the nomogram was 0.759 and 0.774 in the training and validation sets, respectively, indicating that the model had good discriminative ability. The specificity and sensitivity of the training set are 0.811 and 0.660, and the specificity and sensitivity of the validation set are 0.699 and 0.769.

Calibration curves of nomogram in the training set and validation set. X-axis represents the predicted probability of the model and y-axis represents the actual probability. The closer the red and green curves fit the ideal dashed line, the better the predictive consistency of the nomogram.
When using the nomogram, the LDL level was placed on the variable axis. A line is then drawn along the axis of its point in order to determine the corresponding risk score. This process was repeated for each variable on the nomogram and the total score was calculated. The final sum is found on the “Total points” axis and a vertical line is drawn intersecting the probability axis to obtain the probability of predicting the occurrence of preoperative DVT.
Clinical significance
Decision curve analysis (DCA) was performed on the prediction model to validate the net benefit of preoperative DVT in patients with femoral neck fracture. The results suggested that the model improved the net benefit of the “treat all” or “no treatment” scenario when the threshold probability was between 6 and 85%. Similarly, this range was 3–78% in the validation model (Fig. 5). The performance of the DCA showed that the model is good at guiding clinical practice.

Decision curve analysis (DCA) of nomogram in the training set (a) and validation set (b). DCA illustrated that the net benefit of the training model is higher in the threshold probability interval of 6–85%, and the net benefit of the validation model is higher in the threshold probability interval of 3–78%.
Discussion
The results showed that the incidence of preoperative DVT in elderly patients with femoral neck fracture was 6.6%, and age, BMI ≥ 28, smoking, LDL-C > 3.4 mmol/L, and d-dimer > 0.475 mg/L were identified as high risk factors for preoperative DVT formation. To our knowledge, this was the first study to develop and validate the nomogram to predict the risk of preoperative DVT in elderly patients with femoral neck fracture, with a specificity of 81.1%, a sensitivity of 66.0% and an AUC value of 0.759 (95% CI 0.679–0.839). In addition, the nomogram has been internally and externally validated for good predictive performance.
Increasing age is a recognized hazardous condition for preoperative DVT in fracture patients and its relevance has been extensively discussed in previous literature20. As the body naturally ages, the metabolic rate decreases, and the fragility of the blood vessels increases. In addition, the increased production of procoagulant substances by blood vessel endothelial cells, combined with the increased risk of chronic disease, significantly increases the risk of DVT under a combination of factors. Naess IA et al. explored differences in the distribution of DVT across age groups, and they reported that about 70% of DVT occurs in people aged over 60, and nearly 25% in patients aged 80 and over. But Barco et al. pointed out that although increasing age was associated with higher incidence of DVT, the elderly with femoral neck fracture could still get equivalent benefits from surgery as those younger patients when potential risks were resolved well21. For the older people who suffered femoral neck fracture, surgeons must be aware of their worse situation and take active measures, such as completing early anticoagulation intervention and ultrasound imaging examination for thrombus as early as possible.
Cigarette smoking was believed to have a clear negative effect on DVT in elderly femoral neck fracture patients. Similar to our findings, Niu et al. also found that smoking is approximately 2.5 times more likely than non-smoking patients to present with preoperative DVT in their retrospective study of 980 patients with femoral neck fractures. In fact, multiple studies have reported the relationship between patients with a history of smoking and preoperative DVT. Its mechanism is the result of a multifactorial combination of factors, including vascular endothelial damage, slowed blood flow, oxidative stress and inflammatory responses22,23. Although current smoking status was a modifiable factor and strict smoking cessation policies are often implemented after admission, this may have limited effect in preventing preoperative DVT, as femoral neck fractures are usually operated on within a few days rather than electively. Some high level of evidence indicated that the increased risk of DVT is not necessarily a direct consequence of smoking act, but rather of the development of smoking-related diseases or other predisposing factors, which may weaken the effect of short-term smoking cessation24.
According to our findings, obesity is a fairly significant risk factor for preoperative DVT, as a large cross-sectional survey from 32 countries came to the same conclusion25,26. Excess fat accumulation restricts venous return and is pro-inflammatory, pro-thrombotic and interferes with the low fibrinolytic environment. Even, in the acute phase of trauma, obesity, together with other factors, may have a supercumulative effect on preoperative DVT24. Furthermore, after adjustment for confounders in this study, elevated LDL-C was also significantly associated with an increased risk of preoperative DVT (OR 2.63), which was highly consistent with the results previously reported by Tan et al.27. Biochemical analyses demonstrate that low-density lipoprotein cholesterol (LDL-C) directly promotes thrombin generation and upregulates the expression of tissue factor, coagulation factor VII, and factor X. These molecular interactions provide mechanistic evidence for the potential role of LDL-C in DVT. Based on the preceding evidence, close clinical surveillance and personalized anticoagulation strategies are recommended for elderly individuals with overweight and concurrently elevated LDL-C levels.
D-dimer, a small molecular dimer produced by the action of fibrinolytic enzymes on cross-linked fibrin, is considered as a powerful indicator in the prediction of perioperative DVT28. Elevated levels in tests usually reflect an underlying hyperfibrinolytic state of the body. However, because D-dimer is susceptible to a number of influences, including trauma, the elderly, inflammation, chronic kidney failure and pregnancy, it has low specificity in predicting DVT (specificity, only 40–50%)29, making it is difficult to distinguish between DVT and non-DVT elderly patients at the traditional threshold (0.5 mg/l)30. Based on the Youden index, the optimal cut-off value for d-dimer in our study was determined to be 0.475 mg/L. Compared with the traditional threshold value, the decreased optimal cut-off value was associated with higher D-dimer sensitivity in elderly patients themselves. After adjustment, the specificity of d-dimer for detecting DVT in elderly patients with isolated femoral neck fracture increased significantly from 62.4 to 81.1%, while the reduced sensitivity (from 71.7 to 66.0%) could be compensated for by the final adjusted model.
The DCA curve helps surgeons and researchers balance the risk of missed diagnosis with the risk of overtreatment by quantifying the clinical net benefit at different thresholds. The core goal of DCA analysis is to minimize the rate of missed diagnosis within the acceptable range of false positives. The training model at low thresholds (< 6%) has reduced net benefit, while high thresholds (> 85%) may overestimate risk due to overfitting, leading to overtreatment. The validation model seems to be more suitable for routine clinical practice, balancing the decision needs of different risk levels, but its extreme threshold performance needs further validation. The difference of DCA interval between validation set and training set reflects the differences in overfitting control, data distribution and probability calibration of the model. Future work may require further optimization of the model’s performance at low threshold intervals while maintaining benefits at higher thresholds.
A large number of published medical studies have shown that nomogram has demonstrated good performance in predicting the risks of various diseases. This study integrated multiple independent risk factors (age, BMI ≥ 28, smoking, LDL-C > 3.4 mmol/L, and d-dimer > 0.475 mg/L) into an intuitive graph. Doctors only needed to simply add each index of the patients at the corresponding scale in the graph. The risk probability of DVT before surgery in patients with femoral neck fractures can be obtained quickly. For instance, our research found that factors such as the patient’s age, smoking, and D-dimer level all have clear scales and weights in the nomogram. Doctors can intuitively observe how these factors interact to affect the risk of DVT, thereby intervening in high-risk factors more specifically, such as taking strict smoking ban measures immediately after admission. Compared with some complex black-box models, such as the random forest model, although its prediction accuracy is relatively high in some scenarios, due to its complex internal structure and difficulty in interpretation, there are obstacles in its clinical promotion and application.
Strengths of this study include accurate data collection, sufficient study population, and control of confounding variables. However, some drawbacks must be recognized. First, the study subjects were all from the same institution. Although, the single-center study design allows minimization of interobserver variability, but may have introduced selection bias. In addition, some study variables were collected primarily by asking patients, meaning that accuracy relied heavily on patients’ self-reports and knowledge of their condition. Finally, to improve the diagnostic validity of the prediction model, patients with various specific conditions (e.g., multiple fracture, high-energy injury, history of DVT, or current oral anticoagulant therapy) were excluded from this study, so the final results of the study may not be applicable to this population.
Conclusion
In summary, this study demonstrated that the incidence of preoperative DVT in elderly patients with femoral neck fracture was 6.6%. Age, BMI ≥ 28, smoking, LDL-C > 3.4 mmol/L, and d-dimer > 0.475 mg/L were identified as independent risk factors for preoperative DVT. Based on this, our study developed a predictive nomogram model that demonstrated strong discrimination power and clinical applicability in both internal and external validation. Surgeons can use it to screen patients on admission, proactively optimise risk factors in the perioperative period and provide individualised early intervention where necessary.
Data availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
References
Cheng, X. et al. Association of preoperative nutritional status evaluated by the controlling nutritional status score with walking independence at 180 days postoperatively: a prospective cohort study in Chinese older patients with hip fracture. Int. J. Surg. 109 (9), 2660–2671 (2023).
Cui, S., Wang, D., Wang, X., Li, Z. & Guo, W. The choice of screw internal fixation and hemiarthroplasty in the treatment of femoral neck fractures in the elderly: a meta-analysis. Journal Orthop. Surg. Research 15(1), 433 (2020).
Xu, K., Ye, X. & Wu, L. A commentary on ‘trends and benefits of early hip arthroplasty for femoral neck fracture in china: a National cohort study’. International J. Surgery. 110(8), 5198–5199 (2024).
Wang, Y. et al. Trends and benefits of early hip arthroplasty for femoral neck fracture in china: a National cohort study. Int. J. Surg. 110(3), 1347–1355 (2024).
Xia, Z-N. et al. Risk assessment and management of preoperative venous thromboembolism following femoral neck fracture. Journal Orthop. Surg. Research 13(1), 291 (2018).
Guo, H. et al. Development and validation of a nomogram for predicting the risk of immediate postoperative deep vein thrombosis after open wedge high tibial osteotomy. Knee Surg. Sports Traumatol. Arthrosc. 31 (11), 4724–4734 (2023).
Kanis, J. A. et al. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos. Int. 23 (9), 2239–2256 (2012).
Zhang, Y-M., Jiang, X. & Sun, Y-S. Effect of Rivaroxaban on preventing deep vein thrombosis in aged diabetics with femoral neck fractures after hip replacement. Bioscience Reports 37(3), BSR20170289 (2017).
Dou, C. et al. Epidemiological status and risk factors of deep vein thrombosis in patients with femoral neck fracture. Journal Orthop. Surg. Research 17(1), 41 (2022).
Niu, S. et al. Preoperative deep venous thrombosis (DVT) after femoral neck fracture in the elderly, the incidence, timing, location and related risk factors. BMC Musculoskelet. Disorders 22(1), 264 (2021).
Chen, W. et al. Risk factors and new diagnostic index for deep venous thrombosis of lower extremities in elderly patients with traumatic femoral neck fracture. Frontiers Surgery 21(9), 1050347 (2023).
Li, C. et al. Loss of walking independence one year after primary total hip arthroplasty for osteonecrosis of the femoral head: incidence and risk prediction model. Journal Orthop. Surg. Research 19(1), 580 (2024).
Wang, T. et al. Comparison of outcomes after total hip arthroplasty between patients with osteonecrosis of the femoral head in association research circulation osseous stage III and stage IV: a five-year follow-up study. Journal Orthop. Surg. Research 19(1), 170 (2024).
Cheng, X. et al. Preoperative risk factor analysis and dynamic online nomogram development for early infections following primary hip arthroplasty in geriatric patients with hip fracture. Clin. Interv. Aging. 17, 1873–1883 (2022).
Zhang, K. et al. Role of a new age-adjusted D-dimer cutoff value for preoperative deep venous thrombosis exclusion in elderly patients with hip fractures. Journal Orthop. Surg. Research 16(1), 649 (2021).
Wang, T. et al. One-year unplanned readmission after total hip arthroplasty in patients with osteonecrosis of the femoral head: rate, causes, and risk factors. BMC Musculoskelet. Disorders 24(1), 845 (2023).
Wang, Z. et al. Treatment of tibial plateau fractures: A comparison of two different operation strategies with medium-term follow up. J. Orthop. Translation. 36, 1–7 (2022).
Riley, R. D. et al. Calculating the sample size required for developing a clinical prediction model. Bmj 368, m441 (2020).
Núñez, E., Steyerberg, E. W. & Núñez, J. Estrategias Para La elaboración de modelos estadísticos de regresión. Rev. Esp. Cardiol. 64 (6), 501–507 (2011).
Barco, S. et al. Impact of sex, age, and risk factors for venous thromboembolism on the initial presentation of first isolated symptomatic acute deep vein thrombosis. Thromb. Res. 173, 166–171 (2019).
Li, Q. et al. Can patients with femoral neck fracture benefit from preoperative thromboprophylaxis? Medicine 96(29) (2017).
Golomb, B. A., Chan, V. T., Denenberg, J. O., Koperski, S. & Criqui, M. H. Risk marker associations with venous thrombotic events: a cross-sectional analysis. BMJ Open 4(3), e003208 (2014).
Zhang, L. et al. Incidence and risk factors of admission deep vein thrombosis in patients with traumatic fracture: A multicenter retrospective study. Clinical Appl. Thrombosis/Hemostasis 29, 10760296231167143 (2023).
Du, H-C., Zheng, Y-F., Shen, M-Q. & Deng, B-Y. No genetic causality between tobacco smoking and venous thromboembolism: A Two-Sample Mendelian randomization study. Thromb. Haemost. 124 (08), 795–802 (2024).
Tan, J-S., Liu, N-N., Guo, T-T., Hu, S. & Hua, L. Genetically predicted obesity and risk of deep vein thrombosis. Thromb. Res. 207, 16–24 (2021).
Pahlkotter, M. K. et al. BMI and VTE risk in emergency general surgery, does size matter?? Am. Surgeon™. 86 (12), 1660–1665 (2020).
Li, G. H. Y. et al. Positive effects of low LDL-C and Statins on bone mineral density: an integrated epidemiological observation analysis and Mendelian randomization study. Int. J. Epidemiol. 49 (4), 1221–1235 (2020).
Anderson, D. R., Stock, W., Karrison, T. G. & Leader, A. D-dimer and risk for thrombosis in adults with newly diagnosed acute lymphoblastic leukemia. Blood Adv. 6 (17), 5146–5151 (2022).
Kruger, P. C., Eikelboom, J. W., Douketis, J. D. & Hankey, G. J. Deep vein thrombosis: update on diagnosis and management. Med. J. Aust. 210 (11), 516–524 (2019).
Cohen, A. T. et al. D-dimer as a predictor of venous thromboembolism in acutely ill, hospitalized patients: a subanalysis of the randomized controlled MAGELLAN trial. J. Thromb. Haemost. 12 (4), 479–487 (2014).
Acknowledgements
We are grateful to all patients who participated in this study.
Funding
This study was funded by the 2024 Government-funded Clinical Medicine Talent Training Program of Hebei Province (ZF2024093) and Central Guidance Fund for Local Science and Technology Development of Hebei Province (246Z7758G). This study was also funded by the Project of the Finance Department of Hebei Province (ZF 2023085).
Author information
Authors and Affiliations
Contributions
Yingze Zhang designed the study; Tianyu Wang, Dongwei Wu and Chengsi Li searched for relevant studies and abstracted the data; Hongyuan Yin, Changhui Li, Xuebin Zhang and Zhenbang Yang analyzed and interpreted the data; Tianyu Wang wrote the manuscript, and Yanbin Zhu approved the final version of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, T., Yin, H., Li, C. et al. Establishment and validation of a predictive nomogram for preoperative deep vein thrombosis in elderly patients with isolated femoral neck fracture. Sci Rep 15, 22601 (2025). https://doi.org/10.1038/s41598-025-06305-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-06305-1
Keywords
This article is cited by
-
Predicting deep vein thrombosis risk in patients with knee fractures: a nomogram-based study
Perioperative Medicine (2026)
