
Abstract
Functional foods significantly impact health outcomes, particularly in the preventing and managing chronic diseases. However, there is a lack of studies in Bangladesh on the association between functional consumption and health outcomes in the adult population. This study aimed to explore the use of functional foods and their association with chronic multimorbidity among the adult population in Bangladesh. The study was conducted on 966 people in the southern region of Bangladesh. Data were collected on sociodemographic and lifestyle characteristics, chronic diseases, frequency of functional food consumption, and influencing factors. Binary logistic regression showed that respondents who consumed nuts weekly (OR = 0.58); natural products monthly (OR = 0.48); honey weekly (OR = 0.50), and egg occasionally (OR = 0.29) were less likely odds to chronic diseases. Furthermore, people who consumed probiotics daily (OR = 0.55) and monthly (OR = 0.39); prebiotics daily (OR = 0.19) and weekly (OR = 0.33); seeds monthly (OR = 0.51); tea and coffee daily (OR = 0.49), and black cumin daily (OR = 0.33) had lower odds to multimorbid condition. These results will support relevant policymakers in taking practical actions to improve healthy dietary practices with functional foods at the community level to prevent chronic multimorbidity in Bangladesh.
Similar content being viewed by others
Introduction
Functional foods are defined as foods intended for consumption as part of a regular diet that offers specific health benefits beyond essential nutrition1. They are primarily found in both conventional and modified food. The former, also known as “unmodified,” is composed of natural or whole food ingredients that contain functional substances. Examples of conventional functional foods include plant-based foods such as fruits, vegetables, herbs, cereals, nuts, beans, and fish. The latter is fortified with essential nutrients such as juices, dairy products, fortified eggs, and seafood2. In South Asian countries, including Bangladesh, functional foods such as herbs and spices (turmeric, black pepper, cloves, cinnamon, ginger, garlic, etc.), seeds (black cumin, pumpkin, sesame, etc.), natural products (oyster mushroom, fenugreek, honey, etc.), and fermented yogurt are commonly used to prevent and manage chronic diseases3,4,5. A study showed that regular consumption of functional foods can improve clinical outcomes in patients with comorbidity conditions6. Numbers of studies revealed that numerous phenolic compounds in herbs and spices, such as turmeric, cloves, garlic, ginger, and fenugreek, have anti-inflammatory and antioxidant properties that help lower multimorbidity, including protection from cancer, arthritis, and cardiovascular diseases3,4,5. Additionally, omega-3 fatty acid-rich foods such as flaxseeds, walnuts, and fatty fish are associated with a lower risk of cardiovascular conditions such as hypertension and coronary artery disease2,4,6. Food rich in dietary fiber, such as oat bran, chia seeds, and psyllium herbs, as well as fermented items such as probiotics, reduces the risk of gastrointestinal disorders, particularly inflammatory bowel diseases7,8,9. In addition to these foods, whole grains, different citrus fruits, dry fruits, and eggs have numerous therapeutic properties that prevent chronic diseases, as a functional food4,6,10.
Notwithstanding the numerous health benefits of functional foods, staple diets in South Asian countries, particularly Bangladesh, are heavily reliant on rice11. In Bangladesh, rice is an indispensable part of daily meals, accounting for approximately two-thirds of the daily diet, along with vegetables, small amounts of pulses, and fish11. In addition, there are differences in dietary habits between urban and rural areas of Bangladesh. A study in the southern districts of Bangladesh found that the primary dietary items in rural areas were mostly carbohydrate food sources and fish, whereas in urban areas that were sugary beverages and meat products12. Furthermore, owing to urbanization and globalization, fast foods and soft drinks are becoming popular in Bangladesh, particularly for the younger generation13. However, traditional dietary patterns often include mainly carbohydrate-source foods and recent dietary trends in fast- and high-sugar foods in Bangladesh, which do not adequately meet nutritional needs14. Consequently, the prevalence of diet-related chronic diseases have increased in Bangladesh in recent years15. According to the World Health Organization, in 2021, NCDs accounted for an estimated 67% of all deaths in Bangladesh16. Recent studies demonstrated that the prevalence of chronic diseases with double and triple burdens in Bangladesh is alarming15,17. Furthermore, diabetes, high blood pressure, and being overweight or obese are becoming common burdens for individuals aged 18–69 years in Bangladesh18. Multimorbidity is particularly concerning, with an estimated prevalence of 8.4% among adults and significantly higher rates (54%) among older adults in rural areas19,20. Considering all these, health conditions, specific healthcare and the most crucial healthy dietary habits are highly required in Bangladesh.
With the growing body of evidence of the higher prevalence of chronic diseases in Bangladesh and, at the same time, the existing health benefits of functional foods for chronic diseases, there is a need to explore whether functional consumption can act as a protective factor against chronic and multimorbid conditions in Bangladesh. Understanding these associations is crucial for developing functional foods-based dietary practices to improve the health outcomes. Therefore, it is essential to explore the use of functional foods and their association with chronic multimorbidity in Bangladesh. Although numerous studies7,10,21,22,23,24 have examined the relationship between functional food consumption and chronic diseases in various countries, comprehensive research on this topic in Bangladesh is lacking. Hence, this cross-sectional study aimed to fill this gap by determining the consumption patterns of functional foods and their associated factors in people with chronic and multimorbidity conditions in Bangladesh. These findings will contribute to the development of culturally appropriate dietary recommendations for individuals with chronic multimorbidity and support relevant policymakers in formulating effective strategies to increase functional food consumption at the community level in Bangladesh.
Methods and materials
Study setting
A cross-sectional study of the adult population was conducted in the southern region of Bangladesh. The survey was conducted from May 20 to June 30, 2023. We collected data from the Jashore, Magura, and Jenaidah districts, located in the southern part of Bangladesh. We conveniently selected one upazila (subdistrict) from each district to collect data. Then, we chose one urban and two rural locations from each upazila. These regions were selected because of their vulnerable health statuses. In 2016, the Bangladesh Health Ministry reported that 94,743, 14,995, and 18,220 cases suffered from relevant chronic morbidities (diarrhea, gastroenteritis, hemorrhages, myocardial infection, chronic obstructive pulmonary diseases, hypertension, stroke, and others). Furthermore, in terms of mortality, in 1911, 490 and 2777 deaths were primarily related to chronic diseases in the same year25,26,27.
Participants
We followed some eligibility criteria in terms of recruiting participants in the study, these are: (i) being an adult (age ≥ 18 years), (ii) participants who did not maintain any special diet to prevent or manage chronic diseases (such as diabetes, high cholesterol, myocardial infarction, stroke, and others), (iii) physical and mental abnormalities, and (iv) women who were not pregnant or lactating at the time of data collection. We set these criteria because they can affect a person’s usual diet, followed by previous studies22,28,29.
Sample size
The required sample size was calculated using the following parameters, as per as a previous study conducted in Bangladesh30,31. Whereas, n = number of samples, z = 1.96 (95% confidence level), p = prevalence estimate (50%); as no study found in Bangladesh, q = (1 - p), d = precision limit or proportion of sampling error (5%), So, n = 1.962 × 0.5 × (1–0.5)/0.052 ~ 384.16. The use of this formula is justified by its ability to establish equilibrium between statistical robustness and practical effectiveness. The conservative assumption of 50% prevalence ensures the sufficiency of the estimated sample size over a spectrum of prevalence situations. With a corresponding Z-score of 1.96 and a 95% confidence level that complies with accepted epidemiological norms, we can be confident in the accuracy of our estimations. By conducting a face-to-face survey, we collected 1022 samples from the respondents. We then excluded samples that were incomplete or missing any data from the collected survey questionnaire. Finally, the study sample consisted of 966 individuals, following the exclusion criteria.
Survey tool and data collection procedures
A structured questionnaire was used to collect data on sociodemographic and lifestyle variables, the frequency of functional food intake, and influencing factors. The questionnaire was reviewed by a public health nutrition expert and a clinical dietician, similar to a previous study32. The questionnaire was adjusted and modified in response to valuable feedback and corrections. Before the final survey, the questionnaire was pilot tested with small samples (n = 40) in face-to-face surveys to clarify and eliminate irrelevant and repeated items. In order to make the questionnaire, more straightforward to comprehend, and more reliable, it was initially developed in English and then translated into Bengali, the respondents’ native tongue.
Eight pre-trained interviewers conducted the face-to-face interviews. The interviewers had educational backgrounds in nutrition and diet, and had experience running health surveys. Interviewers were also trained on study instruments, participant recruitment, data collection procedures, and relevant ethical considerations. First, data were obtained from participants who visited the household. Anthropometric measurements (height and weight) were self-reported. If the respondents could not report, we measured their height and weight using a scale stadiometer and a digital weight balance. Subsequently, prescriptions and medical reports were reviewed by a registered physician to ensure the accuracy of the data, mainly to confirm chronic disease status. Before data collection, the enumerator reassured respondents that the information they supplied would be confidential. To complete one interview, the participants needed 15 to 20 min per sample.
Outcome variables
The primary outcome variables for this study were chronic diseases, including hypertension, heart disease, hypocalcemia, dementia, anemia, and chronic obesity21,22. Respondents with two or more diseases were considered to have multimorbidity33.
Explanatory variables
The explanatory variables examined in this study encompassed sociodemographic information (sex: male, female; Age: 18–29 years, 30–39 years, 40–49 years, > 50 years; education: illiterate, elementary school, secondary, higher secondary, and above; family members: ≤4 members, > 4 members; profession: unemployed, housewife, day labor, farmer, service holder, business, student; residence: rural, urban; monthly family income: <10,000 BDT (<83.69 USD), 10,000-20,000 BDT (83.69–167.40 USD), >20,000 BDT(> 167.40 USD); the monthly cost for functional food consumption was <500 BDT (< 4.18 USD), 500-1000 BDT (4.18–8.36 USD), >1000 BDT (> 8.36 USD); and lifestyle characteristics (BMI [kg/m2] categories: underweight, normal, overweight, obese I, and obese II, according to Asian people categories34; health status: poor, moderate, good; exercise regularly: no, yes; time of exercise: <30 min, ≥ 30 min; smoking: no, yes, and ex-smoker); Functional foods consumptions frequency of the last 1 year: never, daily (5/6 days weekly), weekly (3/4 days weekly), monthly (1/2 days weekly), and occasionally (3/4 times monthly)24,35, most available functional foods throughout the year in Bangladesh (probiotics: probiotic yogurt/cheese/apple cider vinegar; prebiotics: banana/apple/garlic/onion; nuts: peanuts/walnuts/almonds: seed: pumpkin/sesame/flaxseed; fiber rich foods: psyllium herbs/oat’s bran/chia seed; whole grain: rice/flour; tea and coffee: green or black tea/black coffee; natural products: fenugreek/mushroom/spirulina; honey; black cumin; spices: garlic/ginger/ turmeric/clove; citrus fruit: lemon/orange/grapefruit; dry fruits: dates/raisins; egg; fortified foods)4,5,36,37 as well as influencing factors (reasons for intaking FF: for health benefits, recommended by health professionals/others, meet daily requirements, motivate from online media, sensory teste, no specific reasons and reasons for not intaking FF: unrecognize them, unknown health benefits, unaffordable, disinterest, unavailable, tasteless/adverse effect)38,39.
Data analysis
SPSS™ (version 26.0) and R™ Programming (version 4.3.0) were used to analyze the data. The percentage and frequency of the descriptive statistical analyses to summarize the data distribution and multicollinearity with other model fit tests were observed using SPSS, and the factors influencing functional foods were presented graphically with percentages using Microsoft Excel 365. The anthropometric data weight in centimeters was first converted into meters, and then the BMI (kg/m2) was calculated using SPSS. The continuous variable BMI was then transformed into BMI categories according to the cut-off point for Asian people (underweight: ≤18.499: normal: 18.5–22.9; overweight: 23–24.9; obese I: 25–29.9; obese II: ≥30)34.
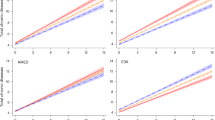
The acquired data were analyzed using descriptive statistical methods and binary logistic regression using the gtsummary-R package. After the multicollinearity test (Model 1, VIF: range = 1.06–1.56, and Model 2, range = 1.06–1.62), two binary logistic regression models were used to assess the association between functional food consumption frequency and respondents who had chronic diseases and multimorbidity. Our analysis used the forward Wald approach, 5% significance threshold (p < 0.05), and 95% confidence interval. The adjusted models contained 15 independent variables and functional food consumption frequency, as presented in Fig. 1. The dependent variable was whether the respondents had chronic diseases or multimorbidity. All predictors in the model (Model 1: frequency of FF consumption vs. chronic diseases) were statistically significant, as demonstrated by the Omnibus test of the model coefficient (x2 = 100.693, df = 60, P-value = 0.001) and the Hosmer and Lemeshow test (x2 = 14.696, df = 8, and P-value = 0.065), which showed that the model could differentiate between respondents with and without chronic diseases. A total of 66.8% of cases were accurately classified by the model, which explained 9.9% (Cox and Snell R-squared) and 13.5% (Nagelkerke R-squared) of the variation in chronic diseases. Another adjusted model (Model 2: frequency of FF consumption versus multimorbidity) was statistically significant according to the Hosmer and Lemeshow test (x2 = 2.574, df = 8, and P = 0.958) and the Omnibus test of the model coefficient (x2 = 104.027, df = 60, and P = 0.000), suggesting that the model could differentiate between respondents with and without multimorbidity. The model successfully identified 67.2% of cases and explained the variation in multimorbidity conditions between 15.7% (Cox and Snell R-squared) and 20.9% (Nagelkerke R-squared).
Ethical approval and informed consent
The ethical committee of the Faculty of Biological Science and Technology at Jashore University of Science and Technology, Jashore-7408, Bangladesh, approved and conformed to the study protocol (Ref: ERC/FBST/JUST/2024 − 198) and all of which were performed in accordance with the guidelines of the Declaration of Helsinki. All participants were asked to provide both verbal and written informed consent before participation. Those who refused to participate in the survey were excluded. Names or identifying numbers and thumbprints were obtained from participants who were unable to read and write during the data collection process.
Results
The sociodemographic, lifestyle, and health status characteristics
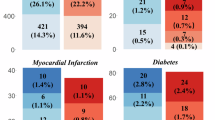
The sociodemographic and health characteristics of the participants are shown in Table 1. The findings from a sample of 966 adults revealed that more than half of the participants (55%) were female, 18.9% were illiterate, and 10.0% were farmers. Most respondents (35.6%) had a family income of more than 20,000 BDT (167.40 USD), whereas almost two-thirds (63.6%) resided in rural areas. Moreover, about 34.6% participants spent less than 500 BDT (4.18 USD) monthly for functional food consumption. In addition, 41.1% had a normal weight, 38.9% claimed good health, and 81.9% were non-smokers. Conversely, only 26.2% of the participants exercised regularly, and most participants (66.4%) exercised for more than 30 min. Notably, most participants had chronic diseases (63.0%), and approximately 50.6% had at least one chronic disease. Among the patients, 23.0% had hypertension, 15.7% had heart disease, 15.3% had hypocalcemia, 18.9% had dementia, 6.6% had anemia, and 29.6% had chronic obesity.
Consumption patterns of functional foods
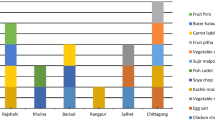
Figure 1 shows the frequency of consumption of selected functional foods. A majority of consumers (35.1%) consumed tea and coffee daily, surpassing other functional foods. In terms of weekly consumption, eggs were predominantly (43.1%) consumed, followed by prebiotics (41.3%), citrus fruits (37.4%), nuts (26.4%). Furthermore, a large number of participants never consumed some notable functional foods, including natural products (69%), fortified foods (64.5%), whole grain (51.2%).

Percentages of use of functional foods frequency among 966 respondents.
Figure 2a shows the motivations for the consumption of functional foods. The main motivation for consuming functional food among over half of the individuals was hunger (56.80%) followed by health benefits (48.30%), no specific reason (29.90%) and sensory taste (26.80%) among participants. As shown in Fig. 2b, unknown health benefits (34.10%) and inability to recognize FF (31.50%) were the leading reasons for not taking FF. Unaffordability (28.50%), disinterest (22.90%), and tastelessness (16.10%) were also responsible for not consuming FF, respectively.

(a) Motives of functional foods intaking among 966 respondents.(b) Motives of functional foods intaking among the 966 respondents.
Association of functional foods consumption frequency with chronic and multimorbid conditions
Table 2 presents the functional food consumption associated with chronic diseases and multimorbidity among the participants in the binary logistic regression model. Findings from regression analysis showed that participants who had consumed nuts such as peanuts, walnuts, and almonds weekly had lower likelihood of developing chronic diseases (OR = 0.58, 95% CI 0.34–0.97, p = 0.038) than those who had never taken them. Monthly natural products such as fenugreek, mushroom, spirulina consumption was associated with lower odds of chronic disease (OR = 0.48, 95% CI 0.23–0.96, p = 0.039) as compared to non-consumers. Weekly honey consumption was associated with lower odds of chronic disease (OR = 0.50, 95% CI 0.27–0.93, p = 0.028) than never consuming honey.
Furthermore, individuals who had eaten eggs occasionally had lower odds of developing chronic disease (OR = 0.29, 95% CI 0.11–0.78, p = 0.016) than those who had never consumed eggs.
On the other hand, those who consumed probiotics such as probiotic yogurt, cheese, and apple cider vinegar on both daily and monthly basis had lower chances of developing multimorbidity (OR = 0.55, 95% CI 0.31–0.99, p = 0.046) and (OR = 0.39, 95% CI 0.19–0.77, p = 0.008) compared to those who had never engaged in such consumption, respectively. Participants who consumed prebiotics such as banana, apple, garlic, onion daily and weekly were less likely to develop multimorbidity (OR = 0.19, 95% CI 0.06–0.60, p = 0.005) and (OR = 0.33, 95% CI 0.11–0.96, p = 0.044) than those who never consumed such food, respectively. Individuals who consumed seeds such as pumpkin, sesame, and flaxseed monthly had lower odds of multimorbidity (OR = 0.51, 95% CI 0.26–0.98, p = 0.045) compared to those who had never consumed them. Daily consumption of tea and coffee reduced the likelihood of developing multimorbidity (OR = 0.49, 95% CI 0.29–0.83, p = 0.008) compared with those who had never consumed them. The risk of multimorbidity decreased when participants had daily consumption of black cumin (OR = 0.33, 95% CI 0.12–0.82, p = 0.020) compared to those who had not consumed it.
Discussion
Functional foods provide health benefits by being enriched with essential vitamins, minerals, and fatty acids, which promote overall well-being and enhance the immune system’s ability to combat chronic diseases40. Obtaining enough of these nutrients regularly with standard diets alone can be challenging, particularly for individuals with higher requirements. Functional foods with beneficial effects on disease treatment outcomes have been shown in randomized controlled studies and experimental models. These include fatty fish, soy, nuts, seeds, legumes, yogurt, chocolate, berries, tomatoes, and whole grains that contain bioactive components41. To the best of our knowledge, our study is the first to investigate the association of multimorbidity with functional food consumption frequency in a cross-sectional nature.
From figure 1), tea and coffee were the predominant functional foods consumed on a daily basis by the participants, consistent with other study42. Regular tea consumption is a common habit throughout Bangladesh42. Based on weekly consumption, majority of the participants consumed egg. Eggs are readily accessible, cost-effective, and a significant source of proteins, lipids, vitamins, and minerals43. Previous study indicates that the availability of eggs surpasses the national average44. This expanded availability, cost-effectiveness and nutritional importance may have significant role in addressing hunger fulfilling nutritional requirements in their diets among the participants which led to consume more on weekly basis. This possible role aligns with our findings that determine motivation for FF consumption which showed majority of the participants consumed for meeting hungriness, followed by health benefits (Fig. 2a). On the other hand, most least consumed functional food were natural products including mushroom, spirulina (Fig. 1) while unknown health benefits accounted main reason for not consuming FF (Fig. 2b). The general population in Bangladesh remains mostly unaware about the nutritional and therapeutic significance of mushrooms45.
Table 2 shows that consuming nuts on a weekly basis was associated with a lower probability of developing chronic diseases than those who never consumed nuts. This finding is supported by a recent cohort study conducted among Korean adults showing that consumers taking 1–2 servings (15–30 g) of nuts weekly had a 34% reduced risk of cardiovascular disease mortality compared to non-consumers 47. We also found notable findings that consuming natural products (fenugreek, mushroom, spirulina) monthly might have the potential benefit of lowering the risks of chronic disease compared to never consuming them. Fenugreek seeds are high in antioxidants, such as polyphenols and flavonoids, which prevent oxidative stress and mitigate damage from free radicals; hence, their antioxidant activity may safeguard cells from ageing and diminish the risk of chronic diseases 50. A previous investigation from the Ohsaki cohort 2006 study indicated that consuming mushrooms three times a week or more was linked to a 19% decrease in the risk of developing dementia in those aged 65 and older in Japan 51. Participants who had consumed honey weekly had fewer odds of having chronic disease than those who had never consumed it.
Previous studies have revealed an inverse correlation between honey consumption and the likelihood of cardiovascular disease. Honey consumption can enhance lipid profile by decreasing total cholesterol and LDL while boosting HDL, thus serving a preventive function in cardiovascular health46. Another important finding was that occasional egg consumption significantly reduced the odds of chronic diseases compared to non-consumers. A recent clinical study found that enriched egg intake improved vascular function, reduced inflammation, and enhanced oxidative status in patients with chronic coronary syndrome, indicating its potential benefits for chronic disease management10.
We also found that probiotics consumption, both daily and monthly, contributed to a lower risk of multimorbidity than never probiotics consumption(Table 2). Recently, researchers have shown that obesity may be affected by gut microbes, and that specific probiotics, including Lactobacillus gaserri, can decrease weight gain and body fat6. In addition, yogurt is abundant in probiotics, including lactobacilli, which may enhance the equilibrium of intestinal flora and inhibit the proliferation of unfavorable bacteria, thereby contributing to the reduction of blood pressure52. Participants who had consumed prebiotics both daily and weekly had lower odds of having multimorbidity compared to those who had never ingested them. Research indicates that prebiotics help alleviate anemia in both clinical and animal models, likely by improving iron metabolism53. Moreover, a recent study demonstrates that prebiotic supplementation enhances iron absorption and mitigates anemia in people54. We found that participants who consumed seeds monthly had less risk of developing multimorbidity than those who had never consumed them. A past study corroborates our findings that women who take seeds 1-2 times per month had considerably reduced levels of total cholesterol (T-C) and low-density lipoprotein cholesterol (LDL-C) compared to women who do not consume seeds55. Maintaining blood cholesterol levels is crucial for reducing heart disease risk factors50. The likelihood of multimorbidity was significantly reduced among those who had drunk tea and coffee daily compared to those who had never drunk them. A previous study found that consuming two to three cups of coffee and tea daily is linked to a lower risk of cardiovascular disease (CVD), chronic respiratory disease (CRD), and both of these diseases23.
Our investigations revealed that participants who had daily consumed black cumin had a lower probability of multimorbidity than those who had never consumed it. A recent study showed that daily ingestion of Nigella sativa (black cumin) oil resulted in notable decreases in critical inflammatory markers, such as IL-1β and IL-6, associated with obesity-related inflammation and metabolic problems. Moreover, the hormone leptin, which controls appetite and adipose tissue storage but frequently becomes imbalanced in obesity, is also markedly diminished48.
Policy implications
The present study investigated the association between functional food consumption and chronic multimorbidity. These findings indicated that regular functional foods consumption positively contributed to the reduction of chronic diseases. However, the study also showed that a considerable number of participants did not take FF because they did not know its health benefits. Policymakers should first focus on promoting awareness and education about the health benefits of functional foods that could increase FF consumption among people. Public health policies should then disseminate clear definitions and health claims for functional foods to avoid confusion and misinformation to consumers. Because functional foods contain bioactive compounds that potentially reduce disease risks, they should be included in preventive health policies within healthcare systems. To increase the accessibility of FF, the government can ensure that FF is affordable and available in all districts of the country.
Limitations and strengths
The current study has several limitations. First, the cross-sectional approach in the survey permits the establishment of associations but does not allow for drawing causal judgments between functional food consumption and chronic/multimorbid conditions. Second, the data collected were based on self-reports (e.g., health status, food consumption frequency) that led to recall bias, which means that there is a possibility of affecting the accuracy of our findings. Moreover, our convenience sampling from three southern districts may not accurately represent the dietary patterns or disease frequency throughout all of Bangladesh. Therefore, the outcomes of the present study may not be generalized to different populations. Additionally, the wide classification of functional food may encompass substances with diverse bioactive qualities, thus masking or confounding the observed associations.
Notwithstanding these limitations, this study is the first to comprehensively understand functional food consumption and its association with chronic disease in Bangladesh. This study focuses on a crucial and current subject with considerable implications for public health. Moreover, the study employed a cross-sectional design with a large sample size, which enhanced its strength and fostered a reasonably high level of confidence in the acquired results. Additionally, the data were analyzed, and conclusions were drawn using suitable statistical procedures.
Future prospects
Functional foods have attracted global attention because of their capacity to prevent chronic diseases and multimorbidity. This capability was attributed to their bioactive compounds. Future studies should focus on identifying unidentified bioactive compounds in functional foods that may reduce the incidence of chronic diseases. Research attention should also be allocated to previously identified bioactive substances to elucidate their efficacy against certain yet unidentified diseases. In this context, the implementation of sophisticated clinical studies would be recommended. Further research is required about nutrition for aging or ill individuals to elucidate the factors influencing the varied responses to functional foods or nutrients and to explore their role in a comprehensive strategy for enhancing well-being and quality of life49.
Conclusion
This study aimed to explore the consumption patterns of functional foods and their association with chronic diseases and multimorbidity. The findings revealed that respondents primarily consumed functional foods to satisfy hunger, while a significant portion reported using them for perceived health benefits. The analysis showed that the weekly consumption of nuts, monthly intake of natural products, weekly honey consumption, and occasional egg consumption were all associated with reduced odds of developing chronic diseases. Additionally, daily and monthly consumption of probiotics, daily and weekly intake of prebiotics, daily consumption of tea and coffee, and daily intake of black cumin were linked to lower odds of multimorbidity. However, other functional foods demonstrated either inconsistent or non-significant associations. Chronic diseases and multimorbidity are widely recognized as being associated with persistent inflammation and metabolic dysfunction. Functional foods are believed to offer anti-inflammatory and immune-boosting properties, as supported by various research studies, including cohort and clinical trials. The results of this study further suggest that the regular consumption of certain functional foods may have a protective effect against chronic diseases. Increasing the frequency of functional food consumption could help strengthen the immune system, promote overall health, and reduce healthcare costs. Therefore, functional foods play a vital role in public health nutrition for the prevention and management of chronic and multimorbid conditions. Policymakers should take effective actions by focusing on functional foods to include national nutrition policy to reduce chronic and multimorbidity conditions among the people for achieving the sustainable goal of nutrition and health in Bangladesh and invest more in research in food and nutrition field to better understand their disease-mitigating benefits.
Data availability
The datasets used or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- FF:
-
Functional foods
- NCD:
-
Non-communicable diseases
- WHO:
-
World health organization
- CVD:
-
Cardiovascular diseases
- LDL:
-
Low density lipoprotein
- HDL:
-
High density lipoprotein
- CI:
-
Confidence interval
- OR:
-
Odds ratio
- USD:
-
US dollar
References
Entry details | FAO Terminology Portal | Food and Agriculture Organization. of the United Nations [Internet]. [cited 2024 Dec 19]. Available from: https://www.fao.org/faoterm/viewentry/en/?entryId=170967
Tafese Awulachew, M. Functional Foods: Functional Ingredients, Sources and Classification, Health Claims (Food Intolerance and Allergy, 2024).
Waisundara, V. Y. Traditional functional food of Sri Lanka and their health significance. Nutritional and Health Aspects of Food in South Asian Countries. INC; 143–158. (2020).
Platel, K. Functional Foods in Indian Tradition and their Significance for Health. Nutritional and Health Aspects of Food in South Asian Countries87–98 (INC, 2020).
Bhaskarachary, K., Vemula, S. R., Gavaravarapu, S. R. M. & Joshi, A. K. R. Traditional foods, functional foods and nutraceuticals. Proc. Indian Natl. Sci. Acad. 82 (5), 1565–1577 (2016).
Awodire, E. F., Ademosun, A. O., Ajeigbe, O. F. & Oboh, G. Functional foods and their applications in managing globally common disease-linked comorbidities. Food Mater. Res. 3. (2023).
Ramachandran, N. & Varghese, R. Cohort studies on potential use of homemade yogurt for systematic treatment of irritable bowel syndrome (IBS) for remission and cure. Int. J. Contemp. Med. Res. [IJCMR] 7(2). (2020).
Zhao, J. et al. High fiber diet attenuate the inflammation and adverse remodeling of myocardial infarction via modulation of gut microbiota and metabolites. Front. Microbiol. 13. (2022).
Keller, E. et al. Psyllium husk powder increases defecation frequency and faecal score, bulk and moisture in healthy cats. J. Feline Med. Surg. 26(4). (2024).
Breškić Ćurić, Ž. et al. Patients with chronic coronary syndrome can benefit from consumption of enriched chicken eggs: the effects on microvascular function, inflammatory biomarkers, and oxidative Status—Randomized clinical study. Appl. Sci. 13, 22 (2023).
Barois, Z. O. et al. An Overview of the Bangladesh food system: outcomes, drivers and activities. (2024).
Chakma, S., Hoque, M. S. & Alam, A. Identification of food habit of urban and rural people in the Southern district of Bangladesh. Int. J. Fish. Aquat. Stud. 2 (5), 210–212 (2015).
Monisha, S. N., Easmin, P., Rahaman, M., Mahbuba, S. & Keya, N. A. Fast food intake frequency among young generation during COVID-19 pandemic in selected area of Dhaka City. J. Ad-din Women’s Med. Coll. 11 (2), 32–38 (2023).
World Bank. Food for Improved Nutrition in Bangladesh. (2019).
Mahumud, R. A. et al. The burden of chronic diseases, disease-stratified exploration and gender-differentiated healthcare utilisation among patients in Bangladesh. Rashid TA, editor. PLoS One. 18 (5) e0284117. (2023).
Bangladesh [Internet]. Available from: https://www.who.int/about/accountability/results/who-results-report-2020-2021/2021/bangladesh (2024).
Al-Zubayer, M. A. et al. Double and triple burden of non‐communicable diseases and its determinants among adults in bangladesh: evidence from a recent demographic and health survey. Int. J. Clin. Pract. 75(10). (2021).
2018 National STEPS Survey for non-communicable diseases. risk factors in Bangladesh. Available from: https://www.who.int/bangladesh/about-us/publications-1/m/item/2018-national-steps-survey-for-non-communicable-diseases-risk-factors-in-bangladesh (2024).
Khan, N., Rahman, M., Mitra, D. & Afsana, K. Prevalence of Multimorbidity among Bangladeshi adult population: a nationwide cross-sectional study. BMJ Open. 9 (11), e030886 (2019).
Khanam, M. A. et al. Prevalence and patterns of Multimorbidity among elderly people in rural bangladesh: A cross-sectional study. J. Heal Popul. Nutr. 29 (4), 406–414 (2011).
Burkert, N. T., Muckenhuber, J., Großschädl, F., Rásky, É. & Freidl, W. Nutrition and health – The association between eating behavior and various health parameters: a matched sample study. PLoS One (2024).
Plasek, B., Lakner, Z., Kasza, G. & Temesi, Á. Consumer evaluation of the role of functional food products in disease prevention and the characteristics of target groups. Nutrients 12(1). Available from: https://pubmed.ncbi.nlm.nih.gov/31888009/ (2024).
Chen, Y. et al. Association of coffee and tea consumption with cardiovascular disease, chronic respiratory disease, and their comorbidity. Mol Nutr Food Res 66(24) 2200419. Available from: https://onlinelibrary.wiley.com/doi/full/https://doi.org/10.1002/mnfr.202200419 (2024).
Elmaliklis, I-N. et al. Increased functional foods’ consumption and mediterranean diet adherence may Have a protective effect in the appearance of gastrointestinal diseases: A Case– control study. Med (Basel, Switzerland) 6(2) 50. Available from: https://pubmed.ncbi.nlm.nih.gov/30970582/ (2019).
Welfare, F. Ministry of health and family welfare (MOHFW) Health Bulletin 2016. Sandwip Upazila Heal Complex. 1–28. (2016).
Local Health Bulletin. Available from: https://app.dghs.gov.bd/localhealthBulletin2016/publish/publish.php?org=10001876&year=2016&lvl=4 (2024).
MoHFW. Ministry of health and family welfare. health bulletin: Chandpur (Sadar). Upazila Health Office 1–89. (2014).
Tay, J. E. F. et al. Functional food consumption and its associated factors among University students in Malaysia during COVID-19 Pandemic. Malays. J. Med. Sci. 30(6) 133 (2023).
Van Dam, R. M., Grievink, L., Ocké, M. C. & Feskens, E. J. M. Patterns of food consumption and risk factors for cardiovascular disease in the general Dutch population. Am. J. Clin. Nutr. 77 (5), 1156–1163 (2003).
Hossain, A. & Munam, A. M. Factors influencing Facebook addiction among Varendra university students in the lockdown during the COVID-19 outbreak. Comput. Hum. Behav. Rep. 6. (2022).
Borg, D. N., Bach, A. J. E., O’Brien, J. L. & Sainani, K. L. Calculating sample size for reliability studies. PM R. 14 (8) 1018–25. (2022). Available from: https://pubmed.ncbi.nlm.nih.gov/35596122/
Islam, M. W., Shahjahan, M., Azad, A. K. & Hossain, M. J. Factors contributing to antibiotic misuse among parents of school-going children in Dhaka City, Bangladesh. Sci.Rep. 14(1) 1–14. Available from: https://www.nature.com/articles/s41598-024-52313-y ( 2024).
Shuvo, S. et al. Prevalence of comorbidities and its associated factors among type-2 diabetes patients: a hospital-based study in Jashore district, Bangladesh. BMJ Open. 13 (9), e076261 (2023).
Girdhar, S., Sharma, S., Chaudhary, A., Bansal, P. & Satija, M. An epidemiological study of overweight and obesity among women in an urban area of North India. Indian J. Community Med. 41 (2), 154–157 (2016).
de Jong, N., Ocké, M. C., Branderhorst, H. A. C. & Friele, R. Demographic and lifestyle characteristics of functional food consumers and dietary supplement users. Br. J. Nutr. 89 (2), 273–281 (2003).
Vignesh, A., Amal, T. C., Sarvalingam, A. & Vasanth, K. A review on the influence of nutraceuticals and functional foods on health. Food Chem. Adv. 5 100749 Available from: https://doi.org/10.1016/j.focha.2024.100749 (2024).
Essa, M. M. et al. Functional foods and their impact on health. J. Food Sci. Technol. 60 (3) 820–34. (2023). Available from: https://doi.org/10.1007/s13197-021-05193-3
Dias, P. G. I. et al. Consumers’ knowledge, attitudes, and behavior regarding functional food Products-A survey from selected areas of Sri Lanka. J. Agric. Sci. - Sri Lanka. 18 (1), 140–153 (2023).
Chammas, R., El-Hayek, J., Fatayri, M., Makdissi, R. & Bou-Mitri, C. Consumer knowledge and attitudes toward functional foods in Lebanon. Nutr. Food Sci. 49 (4), 762–776 (2019).
Suki, N. M., Akhtar, M. F. & Suki, N. M. Functional foods intention: the role of procurement goals in retailing context. J. Distrib. Sci. 21 (11), 13–21 (2023).
Sharma, M. et al. The role of functional foods and nutraceuticals in disease prevention and health promotion. Eur. J. Nutr. Food Saf. 16 (2), 61–83 (2024).
Jothi J, Rahman N, … AC-TJ of, 2021 undefined. Prevalence of tea consumption among university students of south-eastern region of Bangladesh and associated factors.Agrifoodscience.com. 9(8) 1357–61. (2021).
Nargis, S., Majumder, M., Debnath, B. & Hossain, M. Effect of Egg Consumption on Serum Lipid Profile in Young Adults. Bangladesh J. Med. Biochem. (1) 5 https://www.banglajol.info/index.php/BJMB/article/view/33270
Uddin, M., Islam, M. & Nasrin, M. A study on value added dairy products and availability of milk, meat and egg at consumers’ level in selected areas of Bangladesh. Bangladesh J. Livest. Res. 21, 45–55 (2020).
Khan, M. A. Nutritional composition and hypocholesterolemic effect of Mushroom. (2010).
Rasad, H., Entezari, M. H., Ghadiri, E., Mahaki, B. & Pahlavani, N. The effect of honey consumption compared with sucrose on lipid profile in young healthy subjects (randomized clinical trial). Clin. Nutr. ESPEN. 26, 8–12 (2018).
Shin, H. R., Kim, J. & Song, S. J. Association between nut consumption and mortality risk: a 20-year cohort study in Korea with a stratified analysis by health-related variables. Nutr. J. 23 (1), 113 (2024).
Razmpoosh, E. et al. A crossover randomized controlled trial examining the effects of black seed (Nigella sativa) supplementation on IL-1β, IL-6 and leptin, and insulin parameters in overweight and obese women. BMC Complement. Med. Ther. 24 (1), 1–11 (2024).
Delzenne, N. M. & Mullin, G. E. Benefits and risk management of functional foods in the context of chronic diseases. Curr. Opin. Clin. Nutr. Metab. Care. 21 (6), 449–450 (2018).
Hozzein, W.N., Saleh, A.M., Habeeb, T.H., Wadaan M.A.M. & AbdElgawad, H. CO2 treatment improves the hypocholesterolemic and antioxidant properties of fenugreek seeds. Food Chem 308, 125661 (2020). https://doi.org/10.1016/j.foodchem.2019.125661
Zhang, S., Tomata, Y., Sugiyama, K., Sugawara, Y. & Tsuji, I. Mushroom Consumption and Incident Dementia in Elderly Japanese: The Ohsaki Cohort 2006 Study. J Amer Geriatrics Soc 65(7), 1462–1469 (2017). https://doi.org/10.1111/jgs.14812
Li, X., Zhao, Z., Na, L., Cui, W., Che, X., Chang, J. & Xue, X. Effect of Yogurt Intake Frequency on Blood Pressure: A Cross-Sectional Study. Int J Hypertension 2024, 1–10 (2024). https://doi.org/10.1155/2024/8040917
Carvalho, L., Brait, D., Vaz, M., Lollo, P., Morato, P., Oesterreich, S., Raposo, J.Jr & Freitas, K. Partially Hydrolyzed Guar Gum Increases Ferroportin Expression in the Colon of Anemic Growing Rats. Nutrients 9(3), 228 (2017). https://doi.org/10.3390/nu9030228
Paganini, D., Uyoga, M.A., Kortman, G.A.M., Cercamondi, C.I., Moretti, D., Barth-Jaeggi, T., Schwab, C., Boekhorst, J., Timmerman, H.M., Lacroix, C., Karanja, S & Zimmermann, M.B. Prebiotic galacto-oligosaccharides mitigate the adverse effects of iron fortification on the gut microbiome: a randomised controlled study in Kenyan infants. Gut 66(11), 1956–1967 (2017). https://doi.org/10.1136/gutjnl-2017-314418
Kopčeková, J., Lenártová, P., Mrázová, J., Gažarová, M, Habánová, M & Jančichová, K. The relationship between seeds consumption lipid profile and body mass index among patients with cardiovascular diseases. Roczniki Państwowego Zakładu Higieny, 145–153. https://doi.org/10.32394/rpzh.2021.0159
Acknowledgements
The authors would like to express their sincere appreciation to all of the study participants of southern region in Bangladesh for their incredible assistance, as well as for generously dedicating their time to this research.
Funding
This study did not receive any specific grants from funding agencies from public, private, or any other organizations.
Author information
Authors and Affiliations
Contributions
Sanaullah Mazumdar: Conceptualization, Study design & Methodology, Data curation, Formal analysis, Visualization, Investigation, Writing – original draft preparation, and reviewing & editing; Md. Moshiuzzaman Adnan: Data curation, Data entry, Result interpretation, Formal analysis, Writing – original draft preparation; Tanjum Kabir Khuku: Data curation, Data entry, Result interpretation, Writing – original draft preparation; Shuvasish Das Shuvo: Study design & Methodology, Formal analysis, Supervision, Validation, Writing: critically review & editing, , Validation; Farjana Fardaus: Data curation and data entry; Sharmin Asha: Data curation and data entry; Md. Hasan Al Banna: Validation, Writing- critically reviewing the manuscript for potential intellectual content; Md Riazuddin: Data curation; Md Nowshad Mahmud Choyon: Data Curation and data entry. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mazumdar, S., Adnan, M.M., Khuku, T.K. et al. The use of functional foods and its association to chronic and multimorbid conditions: a cross-sectional study among Bangladeshi people. Sci Rep 15, 32786 (2025). https://doi.org/10.1038/s41598-025-07435-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-07435-2
