
Abstract
Older adults are a rapidly increasing demographic in the U.S. whose longevity depends on high quality healthcare. Unfortunately, older adults often face ageism in healthcare settings. Ageism involves not only explicit age discrimination (e.g., refusal to engage with older adults due to a stated dislike), but also more subtle age discrimination (e.g., systematic avoidance of eye contact with older adults). Both forms of age discrimination are largely underexplored in medical settings. Furthermore, it is unclear what impact subtle age discrimination has on health-related outcomes. This study examines the effects of subtle age discrimination on the experiences of older adults in healthcare-related interactions. Through scripted interactions between researchers and participants (65 + years of age), we found negative biopsychosocial impacts of subtle age discrimination on older adults; subtle age discrimination led to substandard physiological (i.e., lowered HRV), psychological (i.e., reduced trust), and behavioral (i.e., increased avoidance of future interactions) outcomes. Increasing awareness and recognition of age discrimination in health-related settings is critical for ensuring that older adults can navigate a more optimal healthcare system that improves rather than compromises older adults’ health.
Similar content being viewed by others

Introduction
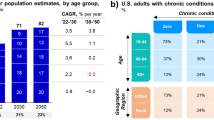
In the next twenty-five years, the number of U.S. adults ages 65 and older is anticipated to increase by 47%1. This rapid shift warrants an increasing amount of attention on the pressing issues that older adults face, one of which is the quality of healthcare that older adults receive2. As adults age, they face an increase in the likelihood of having at least one chronic disease, the necessity of increased medical care, and increased costs associated with healthcare3,4. Despite the growing population of older adults and their frequent utilization of healthcare, there is mounting evidence that ageism is present in healthcare settings. This ageism includes both prejudicial beliefs as well as discriminatory actions based on a person’s age. For instance, evidence shows that older patients receive a poorer quality of healthcare than younger patients5,6,7. This is especially alarming given that older adults spend a significant amount of time in healthcare spaces8,9. The question of healthcare equity for older adults is urgent and critical; in 2022, the World Medical Association issued a statement emphasizing the ethical duty of providers to raise awareness of and eliminate ageism against older adult patients10.
Much of the research on aging and health has focused on age stereotypes (attitudes about older adults), while less has focused on age discrimination (behaviors targeting older adults)5,11,12. In a review of 67 articles related to ageism and health, only two high quality studies examined the relationship between age discrimination and health, finding negative associations between age discrimination and mental health, while no high-quality studies looked at the relationships between age discrimination and disease, health behaviors, or mortality5. A closer look at the research literature suggests that there is still a lot to be understood about age discrimination against older adults in healthcare settings including the effects of experiencing age discrimination on health outcomes.
The present study focuses on age discrimination, which is targeted treatment based on age. In understanding how age discrimination manifests, there are at least two forms. Age discrimination includes overt forms such as blatantly and openly expressing negative thoughts or engaging in negative behaviors toward older individuals. For example, a healthcare provider might state “I prefer not to work with older adults because they are difficult. They don’t listen to what I tell them or follow instructions.” and then proceed to avoid working with older adults. Age discrimination also includes more subtle, less obvious nonverbal and paraverbal cues such as frowning, avoiding eye contact, and a negative tone13. In observational research, subtle discrimination has been detected; medical providers are more likely to engage in slower, louder, and more patronizing speech with older (versus younger) patients14. Older adults report that providers are impatient and annoyed, do not make eye contact, ignore older adults, act without emotional consideration, do not want to care for older adults, try to end interactions quickly, and provide insufficient information15. Providers also tend to depersonalize treatment by talking to others about an older adult patient’s treatment rather than talking to the older adult directly16. Surprisingly, some research has suggested that subtle discrimination may be even more consequential than overt discrimination for targets of discrimination17; however, this research has focused neither on age discrimination nor on health-related settings. Most research on the negative health outcomes of discrimination has focused on sexism and racism, rather than ageism, and has used non-experimental methods17,18. These methods make it difficult to determine if age discrimination causes negative health outcomes or is merely associated with them.
Examining the impact of subtle age discrimination in health-related settings is important for a number of reasons, both theoretically and practically. First, and as mentioned, existing research, particularly research involving experimental paradigms, is scarce. Rather, research has focused on cross-sectional surveys19,20. This research is foundational to understand how subtle age discrimination manifests in day-to-day interactions. At the same time, it is difficult to draw causal conclusions about the effects of subtle age discrimination on health outcomes due to the lack of control over environmental factors (e.g., different healthcare providers, different healthcare environments, different healthcare treatments). Second, there are multiple ways that subtle age discrimination might impact the well-being of older adults which should all be unpacked. In this study, we build on previous research by conducting an experiment in which older adults encounter subtle age discrimination (or neutral treatment) from a health lab experimenter. We utilize this experimental paradigm to assess the effects of subtle age discrimination on older adults’ physiological, psychological, and behavioral health-related outcomes. Each outcome represents a unique impact of subtle age discrimination, which we describe in greater detail below. Overall, we predict that subtle age discrimination:
-
Lowers heart rate variability (physiological effect).
-
Reduces levels of trust toward a health authority (psychological effect).
-
Increases avoidance of a health authority and decreases the intent to return for future visits (behavioral effect).
Physiological responses
In self-report surveys, perceived age discrimination has been both cross-sectionally and longitudinally linked with several negative health outcomes including coronary heart disease, chronic lung disease, limiting long-standing illness, and depressive symptoms21. This can be explained because negative health outcomes may reflect stress in response to age discrimination. One physiological measure of health is vagally mediated heart rate variability (HRV). HRV can reliably indicate stress, with lower scores predicting pathological conditions and cardiovascular mortality22,23. Lifetime experiences of discrimination, including subtle age discrimination, are related to increased stress, reflected through HRV. Past research finds that people who are members of stigmatized groups (e.g., African American people, obese individuals) tend to have lower HRV the more they experience discrimination20,24,25. In summary, past research finds that experiences of discrimination are linked to negative health outcomes such as lowered HRV. Importantly, much of this research studies stigmatized social identities other than age and relies on self-reported, rather than controlled, experiences of discrimination.
In this study, we measure physiological reactions to subtle age discrimination, specifically HRV, to better understand a pathway through which subtle age discrimination impacts health-related outcomes. There is some initial research that examines the connection between age discrimination and cardiovascular health. A recent review of research linking social stigma to cardiovascular health found that no studies had examined the relationship between age discrimination and HRV, and only two of 84 studies had examined any relationship between age discrimination and cardiovascular health20. Both studies that included age discrimination measured participants’ perceptions of chronic discrimination using the Everyday Discrimination Scale (e.g., In your day-to-day life, how often are you treated with less courtesy than others are?)26. Notably, age discrimination was not the primary focus of either study but was included as a part of a larger measure of discrimination. In the first study, Huynh and colleagues found that the frequency of everyday experiences of discrimination, including age discrimination, were associated with increased cortisol output in adolescents27. In the second study, Lewis and colleagues found that the frequency of everyday experiences of discrimination, including age discrimination, were associated with increased coronary artery calcification in middle-aged African-American women28. These studies established the negative relationship between experiences of age discrimination in everyday life and cardiovascular health. Importantly, we extend these studies by focusing on older adults, measuring HRV, and studying a specific instance of subtle age discrimination in a health-related setting. Additionally, we employ a novel experimental method to establish a causal pathway between subtle age discrimination and decreased HRV. We posit that subtle age discrimination induces physiological stress, indicated through lower HRV.
Psychological responses
Studies have also found that discrimination can lead to psychological reactions. For instance, research has shown that those experiencing discrimination are more likely to perform worse on tasks that require executive functioning and selective attention skills29,30. It is less clear, however, how subtle age discrimination influences the cognitions and behaviors of older adults in health-related interactions. One particularly important psychological construct to health outcomes is that of trust. Meta-analytic findings of 47 studies have shown that patient trust in healthcare professionals is positively related to self-reported patient outcomes including health behaviors, patient satisfaction, quality of life, and symptom-related outcomes32. At the same time, patient trust in healthcare professionals was not related to objective or observer-rated health outcomes32. Importantly, the relationships between provider trust and health outcomes are stronger for older adults; for older adults, trust is more positively associated with patient satisfaction and more negatively associated with hospital admissions33. Perhaps unsurprisingly, interpersonal treatment influences the trust a patient has in a provider. Sensitivity in interpersonal communication, namely genuine attention and time reinforce older patients’ trust and confidence in their physicians31. While attention and time may increase trust in a physician, the opposite (i.e., disregard, disinterest, and hurried interactions) are characteristics of subtle age discrimination and may decrease trust in a physician. In this study, we measure older adults’ trust in a health laboratory experimenter after the experimenter acts either neutrally or with subtle age discrimination. We posit that subtle age discrimination has a psychological effect on older adults, indicated by reduced levels of trust toward a health authority.
Behavioral responses
Perceived discrimination is generally linked to less engagement in healthy behaviors (e.g., sleep, medication adherence) and more engagement in unhealthy behaviors (e.g., substance abuse, missing doctor’s appointments)18. Furthermore, experiences of discrimination based on race, socioeconomic status, and medical condition have been linked to mistrust and subsequent medical non-adherence or avoidance34,35. This may be due to a reticence to engage with a healthcare professional in future interactions when one holds negative expectations for that interaction. These behavioral outcomes mean that those experiencing discrimination are likely to receive worse healthcare. Additionally, when older adults hold negative perceptions of aging, they tend to engage less in preventative health behaviors, such as regularly visiting the doctor or adhering to medical advice36. Negative perceptions of aging may be exacerbated by encountering age discrimination from healthcare professionals. In this study, we measure participants’ avoidance of a health laboratory experimenter as well as participants’ intent to return for a future visit with a health laboratory experimenter. We anticipate that subtle age discrimination from a health authority leads to greater avoidance of a health authority and decreases the intent to return for future visits.
Method
Power analysis
We conducted a power analysis to determine adequate sample size. We used the effect size of Cohen’s d = 1.07 as an estimate. There was not a previous study that looked at the exact independent variable (i.e., subtle age discrimination) and dependent variables (i.e., HRV, trust, avoidance, willingness to interact again) that we examined. The estimate of effect size was based off a study with a similar manipulation of subtle discrimination37. Power analysis in G*Power indicated that a sample size of 48 participants was adequate detect a similar effect size.
Participants
Participants were recruited from an existing participant pool of older adults as well as through a community sample via an online neighborhood posting board. They took part in the study in exchange for a $50 Amazon gift card. Participants were screened for major cognitive, auditory, vision, or motor impairments. Before analyses, three participants were excluded from analyses due to difficulties with hearing, dexterity, and comprehension during the task during sessions. After exclusions, a total of 64 participants aged 65 years or older (M = 75.1, SD = 5.1) were included in analyses. Demographic information was missing for one participant. Participants were predominantly women (66%) and White (86%, 5% Black, 5% Asian, 3% Other). The majority of participants held at least a bachelor’s degree (77%, 16% no college degree, 6% chose not to respond).
In analyses of the outcome variables, 64 participants were included in analyses of avoidance, 62 in intent to return, and 63 in trust. These numbers varied due to missing data. In analyses of HRV, 55 participants were included in analyses due to malfunctioning of devices resulting in missing data for 8 participants and high readings above 1000 RMSSD for 1 participant. These participants were not included in analyses for HRV. We chose to use all available data for each analysis because the inclusion did not change the results.
Experimenters
Each participant session was run by one of two male experimenters in their early twenties, one White and one East Asian American. They wore white lab coats that simulated a healthcare provider’s attire. Both experimenters underwent two training sessions to learn the experimental procedure. Both experimenters conducted a trial run in each condition (i.e., discrimination, neutral) with a researcher to ensure proper execution of the script.
Procedure
The study was a between-subjects 2-cell experimental design in which participants were randomly assigned to the age discrimination or neutral condition. Participants were recruited on the phone to take part in a study described as “working to understand the difficulties associated with everyday health-related skills”. They were told they would complete a pill sorting task with fake pills and that their heart rate variability would be measured. Before each session, the participant was read the consent form over the phone and verbally consented.
The actual study took place at a university laboratory in a health research building and occurred individually for each participant. When participants came to the lab, an experimenter assistant unaware of the study condition introduced the study, administered a written consent form, and recorded participants’ baseline HRV. Informed consent was obtained from all participants. Then, using a script to ostensibly provide instructions, the experimenter engaged in a standardized scripted interaction with the participant. The age discrimination and neutral conditions’ scripts had identical verbal statements, but different paraverbal and nonverbal cues. To manipulate subtle age discrimination13, the experimenter followed cues throughout the script to (a) stand farther apart, (b) avoid eye contact, (c) frown (d) cross their arms (e) furrow their brow, (f) use a hostile tone, and (g) sigh disinterestedly at specific points in time. These behaviors reflected older adults’ descriptions of their interactions with healthcare providers15.
In their interactions with the experimenter, participants first completed a pill sorting task to simulate a realistic healthcare task, during which their HRV was measured. Then, participants completed a questionnaire to assess experimenter trust, experimenter avoidance, willingness to interact with the experimenter again, and perceived experimenter discrimination (a manipulation check). Throughout the study, all responses to measures and questionnaires were collected with pen and paper. Lastly, participants were debriefed by the experimenter as to the true purpose of the study. This research was approved by the Rice University Institutional Review Board. Research was performed in accordance with all relevant guidelines and regulations including the Declaration of Helsinki.
Materials
Heart rate variability
Heart rate variability was measured at two time points during the experimental session using a Polar s810 wristwatch and Polar H10 heart rate sensor. Time 1 HRV was measured at the beginning of the session, before the experimental manipulation had begun. At time 1, HRV was measured for 5 continuous minutes while participants were at rest. Participants were told “For the next few minutes we would like you to relax quietly, however you like. We find that people often feel some anxiety when they arrive for a study, after driving here, finding parking, and perhaps being unsure of what to expect. So, we like to give people some time to relax and feel more comfortable here. Please do not use your phone or any other distractions.” Time 1 HRV was a baseline HRV measurement before participants interacted with the experimenter. Time 2 HRV was measured during the experimental manipulation while participants were completing a medically relevant task (a pill sorting activity). During this task, HRV was measured for an average of 4 min and 41 s (SD = 43s, minimum = 2 min 28s, maximum = 5 min 4s). At both time 1 and time 2, participants were seated and maintained silence. The HRV data was analyzed and cleaned for artifacts with the Kubios HRV Premium software. As a measure of HRV, we analyzed the root mean of successive differences (RMSSD), which is less influenced by breathing patterns than other measures of HRV38. Before analyzing the HRV data, we conducted a natural log transformation to achieve a more normal distribution as is convention38.
Experimenter evaluations
Participants reported their evaluation of and reaction to the experimenter.
Trust
Participants assessed how much they trusted the experimenter on an eight-item scale39. Items were rated on a five-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). An example item was “I sometimes distrusted the experimenter” (reverse-scored; α = 0.82). One participant did not respond to items related to trust.
Avoidance
Participants assessed how much they wanted to avoid the experimenter on a five-item scale40. Items were rated on a five-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). An example item was “I would want to avoid interacting with the experimenter” (α = 0.92).
Willingness to interact again
Participants responded to one-item asking about their behavioral intention to engage in future health research with the experimenter. “There is a chance the experimenter might be conducting another study with a similar task. If they were to do so, would you be interested in participating in another similar study with them? If so, I would contact you at the phone number and email address that we have on record.” Participants could respond “YES, I am interested in participating in another study with the experimenter.” or “NO, I am not interested in participating in another study with the experimenter.”
Manipulation check of perceived age discrimination
Perceptions of experimenter age discrimination were assessed using an eight-item scale based on previous research on interpersonal discrimination13. Participants assessed the extent to which the experimenter was (a) smiling, (b) friendly, (c) rude, (d) comfortable, (e) made eye contact, (f) courteous, (g) cold, and (h) awkward (α = 0.91). Items were assessed on a 5-point Likert-type scale ranging from 1 (not at all) to 5 (extremely). Items a, b, d, e, and f were reverse-scored. Higher scores indicate greater perceived age discrimination.
Results
Manipulation check
The manipulation check was analyzed using a Welch’s t-test. The conditions differed on perceived age discrimination. Participants in the age discrimination condition (M = 2.91, SD = 0.73) perceived greater discrimination than participants in the neutral condition (M = 1.79, SD = 0.45; t(53.88) = 7.42, p < .001, Cohen’s d = 1.86).
Descriptive statistics
The sample size, means, standard deviations, minimums, and maximums for all continuous variables including physiological (ln(RMSSD)), psychological (experimenter trust), and behavioral measures (experimenter avoidance) are presented below (see Table 1). Sample size varied due to missing data.
Physiological response
To assess whether there was an impact of condition and time on participants’ HRV (as measured by ln(RMSSD)), we conducted a mixed ANOVA with the condition as the between-subjects variable and time as the within-subjects variable. This analysis allowed us to account for individual differences in participants while assessing these effects. There was not a significant main effect of condition or time on ln(RMSSD); however, there was a significant interaction of condition and time (see Table 2). The nature of this interaction was such that, over time those in the neutral condition tended to increase more from their rest period to the time they interacted with the experimenter, while those who were in the age discrimination condition tended to decrease more from their rest period to the time they interacted with the experimenter (see Fig. 1). This suggests that older adults in the neutral condition had increased HRV, associated with positive health outcomes, while older adults in the age discrimination condition had decreased HRV, associated with negative health outcomes. This may suggest that older adults in the neutral condition were able to engage in adaptive physiological regulation, while those in the age discrimination condition were not.

Effect of time and condition on ln(RMSSD).
Psychological response
A Welch’s t-test found that participants in the age discrimination condition (M = 3.40, SD = 0.55) trusted the experimenter less than participants in the neutral condition (M = 4.00, SD = 0.53; t(60.69) = 4.47, p < .001, Cohen’s d = 1.14).
Behavioral response
A Welch’s t-test found that participants in the age discrimination condition (M = 2.45, SD = 0.97) wanted to avoid the experimenter more than participants in the neutral condition (M = 1.65, SD = 0.57; t(52.08) = 4.07, p < .001, Cohen’s d = 1.02).
To test whether treatment of the participant had an impact on intent to return for future interactions, a chi-square test of independence was conducted. The distribution of participants across the age discrimination and neutral conditions differed from a null distribution such that more people in age discrimination condition (6 no/25 yes) said they would not return for a future interaction than in the neutral condition (0 no/31 yes; χ2 (1, N = 62) = 6.64, p = .010). In the age discrimination condition, 2 participants did not respond to this item.
Exploratory analyses
Gender
More women than men participated in the study (42 women, 21 men, 1 no gender reported). Participant gender distribution across the age discrimination (11 men, 22 women) and control conditions (10 men, 20 women) did not significantly differ (χ2 (1, N = 63) = 0.00, p = .99). To ensure that the results were not moderated by gender, analyses were also conducted including participant gender as a predictor. In summary, gender did not moderate the effects of age discrimination on trust or avoidance. Gender did moderate the effect of condition and time on HRV as well as the effect of condition on intent to return. Further descriptions of analyses follow.
In addition to a two-way interaction of condition and time on HRV, there was also a three-way interaction between condition, time, and gender (F(1, 50) = 5.60, p = .022, np2 = 0.101). To break down this three-way interaction, we looked at two separate two-way mixed ANOVAs: one for men and one for women. For men, there was an interaction of condition and time on HRV (as previously described); however, for women there was no interaction. This indicated that there may be more pronounced effects of age discrimination on HRV for men than for women; however, this was exploratory in nature and should be further studied.
To assess the independence of intent to return, condition, and gender, a Cochran-Mantal-Haenszel test was conducted with gender as the strata. This was significant (χ2 (1, N = 63) = 6.29, p = .01) indicating that the three variables were not independent. To break this down by gender, we found that in a chi-square test of indepdendence for men, intent to return and condition were independent (χ2 (1, N = 21) = 1.05, p = .30), whereas for women, they were not independent (χ2 (1, N = 42) = 5.42, p = .020). For both genders, participants only said they would not return for a future visit in the age discrimination condition; however, there were more responses from women indicating that they would not want to return (see Table 3).
Discussion
In this study we examined the outcomes of subtle age discrimination in a health context, and, in line with expectations, age discrimination led to several nonoptimal health-related outcomes. These results underscore the critical importance of understanding and reducing subtle forms of age discrimination in the emerging public health agenda. Indeed, older adults who encountered subtle age discrimination in a health context experienced concerning physiological, psychological, and behavioral consequences.
First, the HRV results indicated that the stress induced by the discriminatory encounter produced a measurable negative physiological response. Importantly, those in the neutral condition had greater increases in HRV scores than those in the age discrimination condition, which is indicative of better health outcomes41. Thus, the HRV findings demonstrate a direct physiological pathway through which discriminatory interpersonal interactions in a health-related environment can impact older adults’ health. Specifically, by studying the effects of age discrimination on HRV in a controlled experimental setting, these findings provide critical causal support for the relationship between discrimination and decreased HRV. Notably, changes in HRV can indicate self-regulatory effort; HRV increases during tasks that require a high amount of self-regulation in comparison to tasks that require a low amount of effort because the body adaptively uses its resources to complete a challenging task42. Consequently, we would expect that HRV would increase during a challenging task, such as the pill sorting task in this study. We found that those in the neutral condition increased HRV which indicates a positive and engaged physiological state. The older adults in the discrimination condition decreased HRV which indicates that they did not respond in an adaptive way but rather were overwhelmed physiologically and unable to regulate during the task. Given that older adults already tend to have a higher number of chronic illnesses and health concerns, additional physiological stressors – such as those caused by subtle discrimination – may have an amplified negative effect on their health. Future studies should continue to incorporate other physiological measures into studies of discrimination. For instance, Schvey and colleagues used saliva testing to assess participants’ cortisol reactivity, finding that participants exhibited greater cortisol reactivity after viewing a weight stigmatizing video43. These different measures will help us better understand the multifaceted ways in which age discrimination impacts health.
Second, the current study also showed the impact that age discrimination has on psychological outcomes. Previous research has shown that patients who report higher levels of trust with their healthcare professionals were also more likely to report more beneficial health behaviors, less symptomatology, higher quality of life, and greater satisfaction with the treatment they receive32. Recent research has shown that patients’ trust in the healthcare system often centers around patient-centered communication44. The critical importance of fostering good paraverbal and nonverbal communication with older patients is particularly evident from the result of this study; older adults who experienced subtle age discrimination simply did not trust the experimenter as much.
Third, the results showed that there were behavioral health outcomes associated with experiencing subtle age discrimination. Because participants experienced greater amounts of physiological stress and trusted the experimenter less, it was not surprising that they also made health-related decisions to avoid that experimenter in futurehealth-related interactions.
These findings have detrimental, real-life implications. For healthcare interactions, this could mean that older adults who interact with a discriminatory healthcare provider may fail to schedule or appear for appointments, reducing older adults’ chances of receiving proper and necessary treatment. Low trust in a healthcare provider could also lead to non-adherence to medication instructions or an exercise or diet plan. Ultimately, increased stress, low trust, and decisions not to return may contribute to worsening medical conditions or even untimely death.
Although the experimental method in the current study allowed us to infer causality between subtle age discrimination and health outcomes, there were also limitations to the design. One limitation was the demographics of the research team. None of the researchers were 65 years or older. Although there were no older adults on the research team, we based our research on a literature review of research on ageism in healthcare settings to better understand older adults’ experiences and previous findings in this area. However, it would be valuable for future research teams to include researchers who are 65 years and older that share the identity of the focal group. Researchers who are older adults themselves may bring valuable perspectives to the research.
Another limitation of our study was the sample demographics. The participants were predominantly White (86%) and high socioeconomic status (77% had at least a bachelor’s degree). These demographics are not representative of the United States. Despite the racially and socioeconomically advantaged identities of these participants, they still experienced significant negative effects of subtle discrimination on health outcomes, which could be exacerbated by co-occurring disadvantaged identities. Given that Black individuals face disparities in healthcare and have lower trust in the healthcare system45, it is possible that age discrimination could exacerbate disparate outcomes. Our study did not focus on how intersectional identities may influence the perception and subsequent effects of subtle age discrimination.
However, in exploratory analyses, we found that the effects of age discrimination on health outcomes varied some by gender. The effect of age discrimination on HRV was more pronounced for men, whereas the effect of age discrimination on the likelihood to return was more pronounced for women. These effects of gender were not consistent across outcome and were exploratory in nature but warrant future investigation. These results indicate that there may be intersectional experiences that uniquely impact the health outcomes. Past research has found this to be true of age and gender, such that, in medical settings, older women areless likely than older men to be on organ transplant lists andclinical trial lists, and receive less thorough examinations and less preventative care16. Additionally, it is worth noting that experimenter gender was consistent across conditions: all confederates were men. In future research it may also be fruitful to explore if there are interactive effects of age discrimination, patient gender, and healthcare provider gender on older adults’ health outcomes.
Our results might be a conservative test of the impact of age discrimination on older adults in health-related interactions due to the relatively low stakes, limited exposure to discrimination, and subtlety of the age discrimination. In this study, there were relatively low stakes (i.e., study participation with guaranteed compensation) in comparison to healthcare interactions in which patients may be trying to alleviate distress, pain, and fear. Additionally, in real-world settings, older adults must navigate the health insurance system, identify viable providers, vigilantly monitor their health, and engage in follow-up visits. The frequent anxiety older adults experience in these interactions can dissuade them from seeking treatment46. In this study, age discrimination added barriers to health-related interactions; older adults distrusted, avoided, and did not intend to interact with discriminatory individuals, even when it could benefit them (through payment for participation). Outside of this study, this could extend to distrust and avoidance of medical treatment. Even though the discriminatory cues in our study were subtle, participants in the discrimination condition still faced adverse consequences physiologically, psychologically, and behaviorally, highlighting the significance of age discrimination irrespective of its overt visibility.
One important feature of this study was that we focused on the the effect of exposure to subtle age discrimination on health outcomes rather than the effect of of perceptions of subtle age discrimination (i.e., labeling age discrimination as such) on health comes47. In our manipulation check, we found that participants in the age discrimination condition reported that the experimenter exhibited more age discrimination than participants in the neutral condition. The measure of age discrimination contained items that indicated that the experimenter in the age discrimination condition smiled less, made less eye contact, was less friendly, comfortable, and courteous and was more rude, cold, and awkward. We did not measure if participants attributed these behaviors to ageism or thought of them as age discrimination. It is possible that some participants attributed the experimenter’s behaviors to individual disposition (e.g., personality), external conditions (e.g., having a bad day), or a non-age-related participant characteristic (e.g., inattentiveness). Future research should investigate the importance of both exposure to age discrimination and attribution of behaviors to age discrimination on health outcomes. It may be the case that labeling age discrimination as such may buffer the negative effects of age discrimination by allowing older adults to engage in less self-blame while attributing discrimination to ageism47,48.
In summary, we found evidence that exposure to subtle age discrimination leads to detrimental physiological, psychological, and behavioral outcomes for older adults. As the demographic of older adults continues to grow, the importance of quality health-related interactions is increasingly critical to maintain population health2. The persistence of subtle discrimination in health encounters can quickly become a deterrent that prevents older adults from accessing care. Age discrimination, including the behaviors that we manipulated in this study, is preventable; we should work to identify and eradicate age discrimination in healthcare49. Future research should continue to explore the myriad outcomes of age discrimination in health-related interactions to understand how to best serve older adults.
Data availability
Data analyzed in this article are available at https://osf.io/y6npe/?view_only=9db30f016a594ac4b9357676318bc835. Participant demographic variables have been removed for de-identification.
References
Mather, M. & Scommegna, P. Fact sheet: aging in the united States. Population Ref. Bureau (2024). https://www.prb.org/resources/fact-sheet-aging-in-the-united-states/
Jones, C. H. & Dolsten, M. Healthcare on the brink: navigating the challenges of an aging society in the united States. Npj Aging. 10, 22 (2024).
Atella, V. et al. Trends in age-related disease burden and healthcare utilization. Aging Cell. 18 (1), e12861 (2019).
Prasad, S., Sung, B. & Aggarwal, B. B. Age-associated chronic diseases require age-old medicine: role of chronic inflammation. Prev. Med. 54 (Suppl), S29–S37 (2012).
Hu, R. X., Luo, M., Zhang, A. & Li, L. W. Associations of ageism and health: A systematic review of quantitative observational studies. Res. Aging. 43 (7–8), 311–322 (2021).
Lombardi, F. et al. Underprescription of medications in older adults: causes, consequences and solutions—a narrative review. Eur. Geriatr. Med. 12, 453–462 (2021).
Rambachan, A. et al. Pain management inequities by demographic and geriatric-related variables in older adult inpatients. J. Am. Geriatr. Soc. 72 (10), 3000–3010 (2024).
Ganguli, I., Chant, E. D., Orav, E. J., Mehrotra, A. & Ritchie, C. S. Health care contact days among older adults in traditional medicare: A cross-sectional study. Ann. Intern. Med. 177 (2), 125–133 (2024).
Gupta, A. et al. Health care contact days among older cancer survivors. JCO Oncol. Pract. 20, 943–952 (2024).
WMA declaration on discrimination against elderly individuals within healthcare settings. World Medical Association (2024). https://www.wma.net/policies-post/wma-declaration-on-discrimination-against-elderly-individuals-within-healthcare-settings/
Lamont, R. A., Swift, H. J. & Abrams, D. A review and meta-analysis of age-based stereotype threat: negative stereotypes, not facts, do the damage. Psychol. Aging. 30, 180–193 (2015).
Warmoth, K., Tarrant, M., Abraham, C. & Lang, I. A. Older adults’ perceptions of ageing and their health and functioning: A systematic review of observational studies. Psychol. Health Med. 21, 531–550 (2016).
Hebl, M. R., Foster, J. B., Mannix, L. M. & Dovidio, J. F. Formal and interpersonal discrimination: A field study of bias toward homosexual applicants. Pers. Soc. Psychol. Bull. 28 (6), 815–825 (2002).
Schroyen, S. et al. Communication of healthcare professionals: is there ageism? Eur. J. Cancer Care. 27 (1), e12780 (2018).
Liu, X., Wang, D., Gu, C., Bao, H. & Luo, Y. Perceived ageism in health care: A hybrid concept analysis. J. Appl. Gerontol. 43 (9), 1326–1342 (2024).
Chrisler, J. C., Barney, A. & Palatino, B. Ageism can be hazardous to women’s health: ageism, sexism, and stereotypes of older women in the healthcare system. J. Soc. Issues. 72 (1), 86–104 (2016).
Jones, K. P., Peddie, C. I., Gilrane, V. L., King, E. B. & Gray, A. L. Not so subtle: A meta-analytic investigation of the correlates of subtle and overt discrimination. J. Manag. 42 (6), 1588–1613 (2016).
Pascoe, E. A. & Smart Richman, L. Perceived discrimination and health: a meta-analytic review. Psychol. Bull. 135 (4), 531–554 (2009).
Hartgerink, J. M., Cramm, J. M., Bakker, T. J., Mackenbach, J. P. & Nieboer, A. P. The importance of older patients’ experiences with care delivery for their quality of life after hospitalization. BMC Health Serv. Res. 15, 1–7 (2015).
Panza, G. A. et al. Links between discrimination and cardiovascular health among socially stigmatized groups: A systematic review. PloS One. 14 (6), e0217623 (2019).
Jackson, S. E., Hackett, R. A. & Steptoe, A. Associations between age discrimination and health and wellbeing: Cross-sectional and prospective analysis of the english longitudinal study of ageing. Lancet Public. Health. 4 (4), e200–e208 (2019).
Tiwari, R., Kumar, R., Malik, S., Raj, T. & Kumar, P. Analysis of heart rate variability and implication of different factors on heart rate variability. Curr. Cardiol. Rev. 17 (5), e160721189770 (2021).
Tsuji, H. et al. Impact of reduced heart rate variability on risk for cardiac events. The Framingham heart study. Circulation 94 (11), 2850–2855 (1996).
Hill, L. K. et al. Examining the association between perceived discrimination and heart rate variability in African Americans. Cult. Divers. Ethnic Minor. Psychol. 23 (1), 5–14 (2017).
Hoggard, L. S., Hill, L. K., Gray, D. L. & Sellers, R. M. Capturing the cardiac effects of Racial discrimination: do the effects keep going? Int. J. Psychophysiol. 97 (2), 163–170 (2015).
Williams, D. R., Yu, Y. & Jackson, J. S. Racial differences in physical and mental health: socioeconomic status, stress and discrimination. J. Health Psychol. 2 (3), 335–351 (1997).
Huynh, V. W., Guan, S. S. A., Almeida, D. M., McCreath, H. & Fuligni, A. J. Everyday discrimination and diurnal cortisol during adolescence. Horm. Behav. 80, 76–81 (2016).
Lewis, T. T. et al. Chronic exposure to everyday discrimination and coronary artery calcification in African-American women: the SWAN heart study. Psychosom. Med. 68 (3), 362–368 (2006).
Schmader, T., Johns, M. & Forbes, C. An integrated process model of stereotype threat effects on performance. Psychol. Rev. 115 (2), 336–356 (2008).
Inzlicht, M., McKay, L. & Aronson, J. Stigma as ego depletion. Psychol. Sci. 17 (3), 262–269 (2006).
Evans, N. et al. Older patients’ attitudes towards and experiences of patient-physician end-of-life communication: A secondary analysis of interviews from british, Dutch and Belgian patients. BMC Palliat. Care. 11, 24 (2012).
Birkhäuer, J. et al. Trust in the health care professional and health outcome: A meta-analysis. PloS One. 12 (2), e0170988 (2017).
Katz, E., Edelstein, B. & Turiano, N. A. Age as a moderator of health outcomes and trust in physicians. J. Aging Health. 36 (5–6), 308–319 (2024).
Jaiswal, J. & Halkitis, P. N. Towards a more inclusive and dynamic Understanding of medical mistrust informed by science. Behav. Med. 45 (2), 79–85 (2019).
McQuaid, E. L. & Landier, W. Cultural issues in medication adherence: disparities and directions. J. Gen. Intern. Med. 33 (2), 200–206 (2018).
Levy, B. R. & Myers, L. M. Preventive health behaviors influenced by self-perceptions of aging. Prev. Med. 39 (3), 625–629 (2004).
Word, C. O., Zanna, M. P. & Cooper, J. The nonverbal mediation of self-fulfilling prophecies in interracial interaction. J. Exp. Soc. Psychol. 10 (2), 109–120 (1974).
Shaffer, F. & Ginsberg, J. P. An overview of heart rate variability metrics and norms. Front. Public. Health. 5, 258 (2017).
Anderson, L. A. & Dedrick, R. F. Development of the trust in physician scale: A measure to assess interpersonal trust in patient-physician relationships. Psychol. Rep. 67 (3 Pt 2), 1091–1100 (1990).
Plant, E. A. & Devine, P. G. The antecedents and implications of interracial anxiety. Pers. Soc. Psychol. Bull. 29(6), 790–801. (2003).
Zulfiqar, U., Jurivich, D. A., Gao, W. & Singer, D. H. Relation of high heart rate variability to healthy longevity. Am. J. Cardiol. 105 (8), 1181–1185 (2010).
Segerstrom, S. C. & Nes, L. S. Heart rate variability reflects self-regulatory strength, effort, and fatigue. Psychol. Sci. 18 (3), 275–281 (2007).
Schvey, N. A., Puhl, R. M. & Brownell, K. D. The stress of stigma: exploring the effect of weight stigma on cortisol reactivity. Psychosom. Med. 76 (2), 156–162 (2014).
Hong, H. & Oh, H. J. The effects of patient-centered communication: exploring the mediating role of trust in healthcare providers. Health Commun. 35 (4), 502–511 (2020).
Guerrero, N., de Leon, M., Evans, C. F., Jacobs, E. A. & D. A., & Determinants of trust in health care in an older population. J. Am. Geriatr. Soc. 63 (3), 553–557 (2015).
Phibbs, S. & Hooker, K. An exploration of factors associated with ageist stereotype threat in a medical setting. J. Gerontol. Ser. B, Psychol. Sci. Soc. Sci. 73(7), 1160–1165. (2018).
Major, B., Quinton, W. J. & McCoy, S. K. Antecedents and consequences of attributions to discrimination: Theoretical and empirical advances. Adv. Exp. Soc. Psychol. 34, 251–330 (2002).
Major, B., Quinton, W. J. & Schmader, T. Attributions to discrimination and self-esteem: impact of group identification and situational ambiguity. J. Exp. Soc. Psychol. 39 (3), 220–231 (2003).
Pillemer, K., Burnes, D. & MacNeil, A. Investigating the connection between ageism and elder mistreatment. Nat. Aging. 1 (2), 159–164 (2021).
Acknowledgements
We would like to thank the members of the Hebl lab for assisting with data collection.
Funding
There are no funding sources to declare for this research.
Author information
Authors and Affiliations
Contributions
L.C.N.: Conceptualization, project administration, data analysis, data interpretation, writing (draft, editing, reviewing)H.K.: Writing (draft, editing, reviewing)M.H.: Conceptualization, writing (draft, editing, reviewing)E.K.: Conceptualization, writing (editing, reviewing) C.F.: Conceptualization, writing (editing, reviewing).
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ng, L.C., Kim, H.J., Hebl, M. et al. Ageism in a health-related context: the physiological, psychological, and behavioral impacts of subtle age discrimination on older adults. Sci Rep 15, 30895 (2025). https://doi.org/10.1038/s41598-025-07489-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-07489-2
