
Abstract
While Glycoantigen 724 (CA72-4) is well-established as a tumor marker, its association with gout has yet to be fully explored. Our study aimed to investigate the expression levels of CA72-4 and other tumor markers at different stages of gout in patients and to assess any changes in their expression levels following treatment with colchicine. For this observational clinical study, participants with gout were recruited and divided into two groups: a gout-flare group and a gout-no-flare group. Additionally, healthy volunteers were recruited as controls. The clinical characteristics of the three groups were compared, and the ROC curve was used to compare the diagnostic value of C-reactive protein (CRP) and CA72-4 for gout flare. Gout flare is divided into two subgroups: a group receiving colchicine and a group receiving without colchicine; comparing the clinical characteristics of the two groups. Serum CA72-4 levels were significantly higher in gout flare compared to gout no flare and healthy controls (P < 0.01). There was no significant difference regarding other tumor markers (Glycoantigen 125 (CA12-5), Glycoantigen 199 (CA19-9), and Carcinoembryonic antigen (CEA)) among the various groups. Elevated levels of CA72-4 and CRP, BMI, and tophi were independent correlates of acute gout attacks (OR = 1.438, 95% CI: 1.240 ~ 1.668, P < 0.01; OR = 1.533, 95% CI: 1.282~1.834, P < 0.01; OR = 3.368, 95% CI: 1.229~9.230, P = 0.018; OR = 1.451, 95% CI: 1.020~2.064, P = 0.038). ROC curve analysis showed that CA72-4 had a higher area under the curve compared to CRP (AUC = 0.966, 95% CI: 0.944~0.981, P < 0.01; AUC = 0.900, 95% CI: 0.867~0.927, P < 0.01). However, serum CA72-4 levels were further elevated during gout flare in the group receiving colchicine (P < 0.01). During gout flare, serum CA72-4 levels were significantly elevated. Serum CA72-4 and CRP can be considered diagnostic serum markers for the acute phase of gout. Colchicine can cause further elevation of serum CA72-4 in gouty flares.
Similar content being viewed by others

Introduction
Gout is a common metabolic disease, and its prevalence is increasing annually. Most gout is over 1% in most developed countries, particularly in North America and Europe1, whereas in China, it ranges between 1 and 3%2. Although gout attacks result from hyperuricemia, the levels can be falsely low during acute attacks. Currently, some studies suggest that C-reactive protein (CRP) levels may increase during the acute phase of gout3; however, CRP is not highly specific, and its elevation can be observed in various other diseases. Despite CRP increasing with acute attacks, more particular biomarkers are still desirable.
Glycoantigen 724 (CA72-4) is a widely used clinical tumor marker that shows increased expression in various types of tumors, such as gastrointestinal and ovarian tumors4,5. Nevertheless, several studies have reported that CA72-4 levels are also significantly elevated in non-cancerous diseases, such as pancreatic, biliary, liver, and type 2 diabetes6,7. This study suggested that CA72-4 was not exclusively produced by cancer cells or tumors. Previous studies have reported an association between gout and CA72-48,9. Gout is recognized as an inflammatory disease, and some studies have proposed that CA72-4 may play a significant role in the inflammatory response. CA72-4 is a high molecular weight mucin with a pan-cancerous tissue distribution that can provoke an immune response, leading to inflammation9. However, it was not explicitly stated whether CA72-4 is associated with gout at all stages, and further analysis is required to determine if other markers are also associated with gout.
In this cross-sectional study, we comprehensively analyzed the relationship between acute and remissive phases of gout, pure hyperuricemia, and CA72-4 levels while also analyzing the impact of gout medications on CA72-4 levels. Additionally, we investigated the correlation between gout and other tumor markers.
Methods
Participants information
A total of 850 participants were enrolled in this study as inpatients or outpatients at the Second Hospital of Fujian Medical University from 2020 to 2023. Of these registered individuals, 535 were diagnosed with gout based on the 2015 ACR/EULAR gout classification criteria. Senior gout experts and rheumatologists confirmed the diagnoses. They were divided into the gout flare group and the gout no flare group. Gout flare is divided into two subgroups: a group receiving colchicine and a group receiving without colchicine. Of these enrolled individuals, 315 volunteers were enrolled as healthy controls. The exclusion criteria were various carcinomas, non-gouty arthritis (rheumatoid arthritis, spondyloarthritis, osteoarthritis, septic arthritis), age < 20 years or > 70 years, long-term alcohol abuse, pregnancy, kidney or liver insufficiency, perioperative, severe infection, and blood disease. In this study, the enrolled patients continued to use their previous urate-lowering regimen. All participants were informed about the study and signed consent forms. The Ethics Committee of the Second Affiliated Hospital of Fujian Medical University has approved this study.
Indicator measurement
The same one-piece scale measured standing height and weight while fasting without shoes. The BMI value was calculated by dividing the participant’s weight (in kilograms) by the square of their size (in meters). The participant’s blood pressure was measured on their right arm using a mercury sphygmomanometer after 30 min of sitting and resting. Venous blood was collected from each participant in the morning after a 10–12 h fast. An electrochemiluminescence immunoassay was used to measure CA72-4, Glycoantigen 125 (CA12-5), Glycoantigen 199 (CA19-9), and Carcinoembryonic antigen (CEA) using the Modular E601 automated analyzer (Roche, Basel, Switzerland), according to the manufacturer’s instructions. HbA1c was measured using high-performance liquid chromatography (D10; Bio–Rad, Berkeley, CA). We used automatic biochemical analyzers (Cobas 8000; Roche, Germany) to measure sUA, CRP, kidney function (serum creatinine), liver function (aspartate transaminase (AST), alanine transaminase (ALT)), and blood lipids (low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, and total cholesterol (TC)) uniformly. The glomerular filtration rates were calculated using the formula “Ccr= {[140-age (years) × weight (kg)]/[0.818 × serum creatinine (Scr, µmol/L)]} for men and Ccr × 0.85 for women”.
Statistical analysis
Statistical analysis was performed on most of the data using SPSS version 19.0 and GraphPad Prism version 8.0. Continuous variables with normal distribution were expressed as mean ± standard deviation (SD), while non-normally distributed variables were presented as median (interquartile range, IQR). Categorical variables were described as frequencies (percentages)10. One-way analysis of variance (ANOVA) and Kruskal-Wallis were used for two-way comparisons between the three groups. Data were compared between the two subgroups using a t-test. The chi-square test was used to compare count data of characteristics. Logistic regression was performed by adding CA72-4, CRP, etc., to control for possible confounding factors. A receiver operating characteristic (ROC) curve was used to determine a cutoff value for CA72-4 and CRP in people with gout. A p-value of less than 0.05 was considered statistically significant.
Results
A total of 850 participants were included in the study. Among them, 315 were healthy controls, 286 had gout no flare, and 249 had gout flare (Table 1). CA72-4 and CRP levels were significantly higher in participants with gout flare than those with no flare and healthy controls (Table 1). There were no significant differences between the three groups regarding CA12-5, CA19-9, CEA, age, duration, BMI, blood pressure (DBP and SBP), hypertension history, diabetes history, cardiac disease history, smoking history, drinking history, tophi, LDL, HDL, TC, AST, ALT, and UACR (Fig. 1A,B). The participants with gout were predominantly male (Table 1). After adjustment, CA72-4, CRP, tophi, and BMI remained independently associated with acute phase of gout (odds ratio 1.438 [1.240 ~ 1.668], P < 0.01; odds ratio 1.533 [1.282~1.834], P < 0.01; odds ratio 3.368 [1.229~9.230], P = 0.018; odds ratio 1.451 [1.020~2.064], P = 0.038) (Table 2). However, in participants with gouty flares, CA72-4 levels were significantly higher in participants receiving colchicine than in those not. There was no significant difference in CRP, NSAID use, and other tumor marker indicators (Table 3).

(A) Comparison of serum CA72-4 levels in four groups. (B) Serum CA72-4, CA12-5, CA19-9 and CEA levels in gout patients.
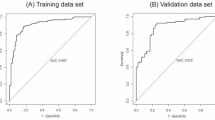
The cutoff value for CA72-4 measured using the ROC curve was 9.1 U/mL, with an area under the curve of 0.966, a sensitivity of 94.49%, and a specificity of 90.38% (95% CI: 0.944–0.981, P < 0.001). The optimal cutoff point for CRP was 7.01 mg/L, with the highest AUC of 0.900, a sensitivity of 83.46%, and a specificity of 85.58% (P < 0.001) (Fig. 2).

ROC curve of CA72-4 and CRP.
Discussion
Based on a gout study in China, our study revealed that CA72-4 levels were significantly higher during gouty flares. Interestingly, these levels increased even further after treatment with colchicine. In contrast, other tumor markers and medications commonly used for gout treatment did not show significant changes. Moreover, we found that similar to CRP, CA72-4 can be a useful diagnostic biomarker for gouty flares. However, CA72-4 demonstrated better diagnostic accuracy than CRP in this regard. About CA72-4 being better, the gouty flare patients were being treated, so CRP was less than it should be. This study suggests that CA72-4 may have better clinical significance as a more reliable and sensitive marker for diagnosing gouty flares than CRP rather than just showing statistical significance.
Gout is a type of joint disease due to the accumulation of sodium urate crystals in the bloodstream caused by prolonged hyperuricemia11. Nevertheless, epidemiological studies have indicated that up to 90% of individuals with hyperuricemia do not develop gout12,13,−14. Furthermore, high uric acid levels are not necessarily present in individuals with gout3, consistent with our findings that the blood uric acid level was lower during the gouty flares. CRP is a commonly used biomarker for determining the onset of gouty flares, but its specificity is low.
In the past, CA72-4 was considered a high-molecular-weight mucin 5 with a broad distribution in cancer tissues6. However, increasing evidence suggests that elevated levels of CA72-4 are not only expressed in cancerous diseases but also non-cancerous conditions, including diabetes, liver disease, etc7,8. Recently, some studies9,15, primarily retrospective, have suggested a link between gout and CA72-4. Our study conducted further prospective research and found that CA72-4 only significantly increased during gouty flares, while it remained unchanged during the remission phase of gout. Our study also found that only CA72-4 among the tumor serum markers increased during gouty flares, while other tumor markers, such as CEA, CA19-9, and CA12-5, remained unchanged. In addition, our study found that during gouty flares, patients who received colchicine treatment showed a further increase in CA72-4, while there was no change in CA72-4 levels in patients receiving other drug treatments.
Here, we will attempt to analyze the potential mechanisms that may lead to the increase in CA72-4 during acute gout attacks and after colchicine treatment, even though we did not conduct such an analysis in our study. CA72-4 acts as an adhesion molecule during the inflammatory process16. Gout is an inflammatory disease; therefore, CA72-4 may play an unknown but crucial role in the inflammatory response9. Another study on autoimmune inflammatory diseases also reported similar results, where patients showed an increase in CA72-4 levels, while the other three glycoproteins did not increase17. There is still limited research on the specific mechanisms of CA72-4 during acute gout attacks. The exact mechanism of colchicine’s effect on CA72-4 is still unclear. It may be related to the stimulation of the gastrointestinal tract by oral colchicine, resulting in a series of inflammatory reactions and an increase in CA72-4. It is also possible that colchicine or its metabolites interfere with the conditions of CA72-4 detection, leading to a rise in its level.
As far as we know, CRP is a standard marker of inflammation during gouty flares and is often used to indicate whether the patient is in the acute phase17. Moreover, we used ROC curve analysis to evaluate the diagnostic value of CA72-4 in acute gout attacks, and our study found that the area under the ROC curve was 0.966 (greater than 0.9), indicating that CA72-4 has a high diagnostic value for acute gout attacks. Furthermore, compared to CRP, CA72-4 has higher diagnostic value, specificity, and sensitivity.
Conclusions
In conclusion, serum CA72-4 was closely associated with the gouty flares and it may be considered as a potential serum marker for diagnosing the acute phase of gout, in conjunction with CRP. In addition, clinicians can provide explanations to patients with elevated serum CA72-4 levels who are without cancer but in the acute phase of gout and/or undergoing colchicine treatment. However, our study has some limitations. This study was conducted at a single center with a relatively small sample size, consisting only of Chinese participants. This study was the relatively high proportion of participants with diabetes, hypertension, or a history of smoking. Since these conditions—along with their associated medications and the biochemical effects of smoking—may influence the measured outcomes. Additionally, since the majority of gout patients are male, the inclusion of very few female patients may have an impact on the study results. Therefore, further comprehensive research with larger sample sizes and more diverse ethnic groups is needed.
Data availability
The datasets used or analysed during the current study are available from the corresponding author on reasonable request.
References
Kuo, C. F. et al. Global epidemiology of gout: prevalence, incidence and risk factors. Nat. Rev. Rheumatol. 11 (11), 649–662 (2015).
Chinese Society of Rheumatology, Chinese Medical Association. Chinese gout diagnosis and treatment guidelines. Chin. J. Internal Med. 55 (11), 892–899. (2016).
Vedder, D. et al. Neutrophil activation identifies patients with active polyarticular gout. Arthritis Res. Ther. 22 (1), 148 (2020).
Mariampillai, A. I. et al. Cancer antigen 72 – 4 for the monitoring of advanced tumors of the Gastrointestinal tract, lung, breast and ovaries. Anticancer Res. 37 (7), 3649–3656 (2017).
Schmiegel, W. Tumor markers in pancreatic cancer–current concepts. Hepatogastroenterology 36 (6), 446–449 (1989).
Demirci, H. et al. CA 72 – 4 levels in patients with type 2 diabetes mellitus. Int. J. Clin. Pract. 64 (1), 34–38 (2010).
Carpelan-Holmström, M. et al. CEA, CA 19 – 9 and CA 72 – 4 improve the diagnostic accuracy in gastrointestinal cancers. Anticancer Res. 22 (4), 2311–2316 (2002).
Bai, X. et al. Serum CA72-4 is specifically elevated in gout patients and predicts flares. Rheumatol. (Oxford). 59 (10), 2872–2880 (2020).
Zhang, Y. et al. Increased serum CA724 levels in patients suffering gout vs cancers. Prog Mol. Biol. Transl Sci. 162, 177–186 (2019).
Doğan, İ. et al. 14-3-3 η ETA protein as a potential marker of joint damage in gout. Clin. Biochem. 118, 110611 (2023).
Riccitelli, M. L. Etiology and treatment of gout–modern concepts. J. Am. Geriatr. Soc. 16 (6), 719–728 (1968).
Trifirò, G. et al. Epidemiology of gout and hyperuricaemia in Italy during the years 2005–2009: a nationwide population-based study. Ann Rheum. Dis. 72 (5), 694–700. (2005).
Luk AJ, Epidemiology of hyperuricemia and gout. Am. J. Manag. Care 11 (15 Suppl), S435-42; quiz S465-8. (2013).
Guadagni, F. et al. CA 72 – 4 serum marker–a new tool in the management of carcinoma patients. Cancer Invest. 13 (2), 227–238 (1995).
Szekanecz, E. et al. Increased production of the soluble tumor-associated antigens CA19-9, CA125, and CA15-3 in rheumatoid arthritis: potential adhesion molecules in synovial inflammation? Ann. N Y Acad. Sci. 1108, 359–371 (2007).
Balaban, Y. H. et al. Tumor markers in Familial mediterranean fever and their correlation with the frequency of attacks. Clin. Exp. Rheumatol. 26 (4 Suppl 50), S114–S116. (2008).
Okuda, C. et al. Serum CRP in patients with gout and effects of benzbromarone. Int. J. Clin. Pharmacol. Ther. 49 (3), 191–197 (2011).
Acknowledgements
We thanked Lijun Chen and Jiayu Lin for their kind help.
Author information
Authors and Affiliations
Contributions
Yong Zhuang, Qingyan Cai, Xinna Yang, and Huibin Huang designed the study and contributed to the discussion. Yong Zhuang and Huibin Huang wrote, reviewed, and edited the manuscript, are the guarantor of this work, has full access to all the data in the study, and takes responsibility for the data’s integrity and the data analysis’s accuracy. Xin Hu and Qingyan Cai collected and researched data. Xinna Yang and Huibin Huang reviewed the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Second Afliated Hospital of Fujian Medical University (Date 2020/No. 244). Informed consent was obtained from all individual participants included in the study.
Consent for publication
All authors agree to publish it.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhuang, Y., Hu, X., Cai, Q. et al. Elevated serum CA72-4 as a novel diagnostic biomarker for acute gout flares. Sci Rep 15, 20728 (2025). https://doi.org/10.1038/s41598-025-07665-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-07665-4
