
Abstract
The relations between ambient air pollution, meteorological factors, and the number of emergency hospital admissions due to chronic obstructive pulmonary disease (COPD) were analyzed. The study utilized a nationwide collection of emergency hospital admissions from anonymous public registries covering the period of 8 years (2012–2019). Separated analyses were presented by sex, age group, and place of residence (rural vs. urban area), a group of major pollutants (PM2.5, PM10, SO2, NOx, and NO2), and meteorological factors (daily air temperature minimum (Tmin), air temperature maximum (Tmax) and the daily change of an average air temperature (dTc), relative humidity (Rh) and wind speed (Ws)). This analysis confirmed association between environmental factors and an increase in the number of emergency hospital admissions of COPD patients. The greatest correlations (p < 0.001) were r = 0.58 and day lag = 5 days for PM10, r = 0.63 and day lag = 20 days for PM2.5, r = 0.73 and day lag = 20 days for SO2, r = 0.57 and day lag = 25 days for NO2 and r = 0.51 and day lay = 30 for NOx as well as r = -0.78 and day lag = 19 days for Tmax, r = -0.79 and day lag = 19 days for Tmin, r = − 0.57 and day lag = 22 days for dTc, r = 0.42 and day lag = 30 days for Rh and r = 0.40 and day lay = 14 for Ws. Variations of SO2 and temperature were the most important factors associated with emergency hospital admissions of COPD patients in Poland. Women, patients aged 60–79 as well as inhabitants of urban areas showed stronger and faster responses to changes in environmental elements.
Similar content being viewed by others


Introduction
Ambient air pollution poses a significant risk to human health1,2 and is associated with excess mortality3. In 2021, exposure to particulate matter air pollution accounted for 5% of the global disease burden measured in disability-adjusted life-years (DALYs)2. Long-term exposure to ambient air pollution increases the risk of cardiovascular diseases, respiratory diseases, cancers, and diseases of the endocrine and nervous systems3,4. Short-term exposure to air pollution can evoke exacerbations of respiratory diseases like asthma or chronic obstructive pulmonary disease (COPD)5,6.
Particulate matter (PM), nitrogen dioxide (NO2), sulfur dioxide (SO2), carbon monoxide (CO), and ozone (O3) are listed by the World Health Organization (WHO) as air pollutants of public health concern7. Both particulate and gaseous pollutants pose significant health risks and are associated with disease development and progression5,6,8.
Between 1990 and 2021 in Europe, the average annual gross-weighted PM2.5 exposure decreased by 33.7% which also led to a 42.4% decrease in the number of air pollution attributable deaths9. At the same time, emissions of several PMs decreased significantly10. Moreover, emissions of gaseous pollutants also decreased, e.g., CO by 69%, NOx by 63%, and SOx by 93%10. Air pollution levels differ across the EU9,10. Poland is among the EU countries with the highest levels of air pollution emissions10. European Environment Agency estimated that in 2021, Poland was responsible for 22.3% of PM2.5, 19.2% of PM10, 14.2% of CO, 28.1% of SOx, 10.5% of NOx, and 38% of benzo(a)pyrene emission reported in the whole EU10. It is estimated that in 2021 in Poland, exposure to PM2.5 concentrations above the 2021 WHO guideline level of 5 µg/m3 was linked to 47,300 attributable deaths and 519,000 years of life lost11.
Ambient air pollution exposure in Poland is also associated with healthcare burden related to increased risk of hospital admissions among patients with chronic respiratory diseases like COPD12,13. COPD is a common chronic respiratory disease14. Exposure to air pollution is a well-documented risk factor for COPD exacerbation12,13,15,16,17. Patients with severe COPD exacerbation may require urgent hospitalization and additional healthcare utilization during the recovery process which generates substantial economic costs18.
Air pollutants and climate change are closely linked and have similar sources related to industrialization and environmental emissions resulting from human activities3,19. Meteorological factors like air temperature, relative humidity, and wind speed are influencing population behaviors and environmental emissions20 which changes pollutant concentrations in the air24, e.g., from utilization of heating systems and urban traffic21. Moreover, meteorological factors may impact the transmission of respiratory viruses like influenza or SARS-CoV-222,23. However, there is still limited detailed evidence on the impact of meteorological conditions on respiratory disease exacerbations25,26.
Associations between ambient air pollution and COPD exacerbations were analyzed in previously published studies, but most of them were limited to single centers or administrative regions12,13,15,16,17. Poland is an example of an EU country with higher emissions of air pollutants that poses a health risk for approximately 3 million people suffering from COPD27. Nationwide data on the correlations between environmental factors (like air pollution and meteorological conditions) and emergency hospital admissions due to respiratory diseases, (e.g. COPD) may be used to strengthen national policies related to environmental protection and public health safety.
This study aimed to assess the impact of air pollution and meteorological factors on the number of emergency hospital admissions due to COPD in Poland between 2012 and 2019, based on nationwide registries.
Material and methods
Study design
In this study, associations between 7-day average ambient air pollution, meteorological factors, and the 7-day average number of emergency hospital admissions due to COPD were analyzed. Separated analyses were presented by sex, age group, and place of residence (rural vs. urban area). Nationwide data were collected from the anonymous public registries. The observation period covered 8 years (2012–2019). The study protocol was approved (decision number 401/2023) by the Ethical Committee at the Centre of Postgraduate Medical Education in Warsaw, Poland. All methods were performed in accordance with the relevant guidelines and regulations. This is a secondary data analysis based on the nationwide registry managed by the National Institute for Public Health. Data obtained from the Institute were anonymous and generated based on the public statistics system in Poland. As this is a secondary analysis of data generated within the public statistics, consent to participate was waived.
Data collection
Data on COPD admissions
Data on patients hospitalized with COPD were obtained from the public registry on hospitalizations carried out by the National Institute of Public Health National Institute of Hygiene—National Research Institute within the Nationwide General Hospital Morbidity Study28,29. Hospitals are legally obligated to report hospital discharge reports to the registry using a dedicated template28. Medical conditions were coded by physicians using the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10)30. Patients diagnosed with COPD were identified using ICD-10 code J4429. A similar approach was used in other registry-based studies in Poland12,29. Admission date and admission mode (scheduled or emergency) were defined based on the data presented in discharge reports. Demographic data included sex, age on the day of admission, and place of residence defined with geographical codes (TERYT)31. Based on the geographical location of the place of residence (TERYT) codes, patients were classified into groups of urban or rural inhabitants.
Out of 910,372 total hospital admissions of patients diagnosed with COPD in Poland between 2012 and 2019, data on 630,059 emergency hospital admissions of patients diagnosed with COPD were included in this analysis. This timeframe results from the quality of data available in the registry. Moreover, 2019 was the last year before the COVID-19 pandemic onset, which had an impact on healthcare utilization, including a number of hospital admissions.
Data on air pollution
Data on the average daily concentration of air pollutants were obtained from the Chief Inspectorate of Environmental Protection (165 imission stations; Supplementary Table S1) – a government institution responsible for environmental monitoring32. The following air pollutants were included in this analysis: PM2.5: particulate matter ≤ 2.5 μm in diameter (PM2.5), particulate matter with diameter 10 (PM10), sulfur dioxide (SO2), nitrogen oxides (NOx) and nitrogen dioxide (NO2). The selection of air pollutants included in this analysis was based on previously published data on air pollution exposure and respiratory health as well as the list of pollutants with the strongest evidence for public health concerns listed by the WHO7.
Data on meteorological conditions
Data on the average daily values of meteorological factors were obtained from the 55 synoptic stations (Supplementary Table S2) of the Institute of Meteorology and Water Management—National Research Institute – a scientific institution responsible for weather monitoring and forecasting33. The following meteorological factors were included in this analysis: daily maximum (Tmax) and minimum (Tmin) air temperatures, average daily temperature change (dTc), relative humidity (Rh), and wind speed (Ws). The selection of meteorological factors was based on previously published data on relations between weather and health25,26.
Data analysis
The analysis utilized 7-day averages from Poland, as providing adequate statistical weight for analysis and justified by the activity cycle and confirmed by good fit in this type of analysis in our previous studies focused on COVID, concerning the number of emergency hospital admissions of patients diagnosed with COPD, average daily levels of air pollutants (PM2.5; PM10; SO2; NOx; NO2), and average values of meteorological factors (Tmax, Tmin, dTc, Rh, Ws).
Lagged correlation between 7-day averages hospitalizations and (1) 7-day averages air pollution, as well as (2) 7-day averages meteorological factors with a maximum of 30 days difference, were calculated. Then, separate analyses were presented by sex, age group, and place of residence (rural vs. urban area). In rural–urban analysis, a total of 31,534 hospitalizations (< 2% of all hospitalizations analyzed in this study) were excluded due to the lack of TERYT codes in discharge reports. The statistical significance value was set at p < 0.05. In the first step, data were analyzed for all patients.
Ternary plots were prepared with the ggtern R library34 to analyze the complex interactions between air pollutants, meteorological factors, and hospital admissions of patients diagnosed with COPD. By plotting three variables on the three axes of a ternary plot, interactions between different variables were presented.
Granger causality analysis35 was performed to analyze potential predictive relationships among various smoothed variables derived from meteorological and pollution data. This analysis was crucial for identifying directional influences between different environmental factors. For each pair of variables, excluding self-pairings, a statistical model was constructed to test whether the historical values of one variable could predict the future values of another, implementing the Granger causality test at a lag of one variable.
Results
Figure 1 presents the annual course of the 7-day average and anomalous values of air pollutants, meteorological factors, and the number of emergency hospital admissions of patients diagnosed with COPD in Poland between 2012 and 2019. Positive/negative anomaly value indicates that given parameter has higher/lower 7-day average that day, than the mean value from all years for that day. There were seasonal differences in the air pollution levels, values of meteorological factors, and the number of hospital admissions (Fig. 1). A drop in air pollution levels and the number of hospital admissions was observed in 2019, compared to previous years.

The annual course of 7-day average and anomalous values of air pollutants, meteorological factors and the number of emergency hospital admissions of patients diagnosed with COPD, Poland, 2012–2019.
Associations between air pollution and emergency hospital admissions
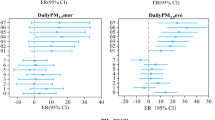
There were statistically significant correlations (p < 0.001) between air pollutants 7-day averages analyzed in this study and 7-day averages emergency hospital admissions of patients diagnosed with COPD (Fig. 2).

Associations between 7-day average daily air pollution levels and the 7-day average number of emergency hospital admissions of patients diagnosed with COPD.
Exposure to all air pollutants resulted in an increased number of emergency hospital admissions on the days of exposure as well as in the subsequent days (Fig. 2 and Supplementary Table S3). The greatest correlations were r = 0.58 and day lag = 5 days for PM10, r = 0.63 and day lag = 20 days for PM2.5, r = 0.73 and day lag = 20 days for SO2, r = 0.57 and day lag = 25 days for NO2 and r = 0.51 and day lay = 30 for NOx (Fig. 2 and Supplementary Table S4).
The analysis showed that with the best matching coefficient, the multi-year variation of emergency admissions of patients diagnosed with COPD can be described by the variation of SO2 concentration. As SO2 pollution increases, there is also an increase in the number of hospitalizations for women, with a shift of 20 days (r = 0.73), and for men, with a shift of 19 days (r = 0.71).
The local variation in PM 2.5 concentration levels describes up to 65% of the variation in COPD patient emergency admissions, with a much more pronounced (m-shape, with a second smaller peak) for the women, and the effect of increased admissions evident after just 10 days of exposure to fine dust, compared to 20 days in the male group (Fig. 2 and Supplementary Tables S4 and S5).
The association of hospitalization with NO2 and NOx variation occurred respectively at r = 0.58 and r = 0.53 for women and r = 0.55 and r = 0.49 for men, with a lag of up to 30 days.
The greatest associations between air pollution levels and emergency admission were observed among patients aged 60–79 years (Fig. 2 and Supplementary Tables S6-8).
The weakest associations, although also statistically significant, are for the group of the youngest patients, aged 40–59. The greatest associations and earlier peaks were observed among urban inhabitants when compared to rural inhabitants (Fig. 2 and Supplementary Tables S9 and S10). For particular matters, the highest hospitalization rates were observed just 5 and 7 days after exposure to increased PM10 and PM2.5 values for patients from urban areas, while after 21 days for patients living in rural areas.
Associations between meteorological factors and emergency hospital admissions
There were statistically significant correlations (p < 0.001) between all meteorological factors 7-day averages analyzed in this study and 7-day averages emergency hospital admissions of patients diagnosed with COPD (Fig. 3).

Associations between 7-day average daily values of meteorological factors and the 7-day average number of emergency hospital admissions of patients diagnosed with COPD.
The greatest correlations were r = − 0.78 and day lag = 19 days for maximum air temperature (Tmax), r = − 0.79 and day lag = 19 days for minimum air temperature (Tmin), r = − 0.57 and day lag = 22 days for day-to-day thermal change (dTc), r = 0.42 and day lag = 30 days for relative humidity (Rh) and r = 0.40 and day lay = 14 for wind speed (Ws) (Fig. 3 and Supplementary Table S7).
Emergency hospital admissions of patients diagnosed with COPD presented a negative trend with air temperature extremes (Tmax and Tmin) as well as with the daily changes in mean air temperature (Fig. 3 and Supplementary Table S4). For women, the variability of COPD hospitalization can be described as high as 80% in relation to changes in maximum and minimum daily air temperature, with a shift of 18 days (Supplementary Table S4). The increase in the number of patients hospitalized for COPD can be explained by the variation in humidity conditions of up to 47% and 37% and the delay of up to 30 days after humidity growth, respectively in the group of men and women urgently admitted to the hospital.
Similarly to air pollution exposure, the greatest associations between meteorological factors and emergency admission were observed among patients aged 60–79 years (Fig. 3 and Supplementary Tables S6-S8) and the greatest associations and earlier peaks were observed among urban inhabitants when compared to rural inhabitants (Fig. 3 and Supplementary Tables S9 and S10).
Emergency admissions of patients from urban areas presented a negative trend with air temperature extremes (Tmax, Tmin) as well as with the daily changes in mean air temperature—at a similar level as in the general population—as high as 80% concerning changes in maximum and minimum daily air temperature, with a shift of 18 days—similarly as for women (Fig. 3). The largest difference concerns the correlation coefficient of the level of emergency hospital admissions with relative air humidity: r = 0.49 for patients from urban areas and r = 0.33 for patients from rural areas (Fig. 3 and Supplementary Tables 9 and 10).
Complex interactions between air pollutants, maximum air temperature, and emergency hospital admissions
Complex interactions between 7-day averages emergency hospital admission, SO2 levels, and maximum air temperature (Tmax) values are presented in Fig. 4. Where frequencies for each three ratio variables range from 0 to 100%. The top row presents relationships between Tmax and SO2 (left side), Tmax and hospitalizations (middle), and hospitalizations and SO2 (right side). The bottom part of Fig. 4 presents the ternary plot of those three variables.

Complex interactions between 7-day average SO2, maximum air temperature and emergency hospital admissions—ternary plot.
The very low number of emergency hospital admissions, highlighted with blue colors (right-titled lines, bottom axis), are related mainly to low levels of SO2 up to 5% (horizontal lines, right axis) as can also be seen on the top right plot. High values of Tmax, from 60 to 100% of values (left-tilted lines, left axis) are also present mainly with low levels of SO2 up to 20% of SO2 values, as can be seen also on the left upper panel (Fig. 4). The majority of the highest number of hospital admissions (red dots) can be found mainly between 10 and 40% of Tmax and from 20 to 60% of SO2 values indicating a close to the linear relationship between hospitalizations and Tmax, but more exponential one between hospitalization and SO2 (Fig. 4). Similar interactions, but not as strong can be seen for PM2.5 levels (Fig. 5).

Complex interactions between 7-day average PM2.5, maximum air temperature and emergency hospital admissions—ternary plot.
Granger causality analysis—potential predictive relationships between various smoothed variables derived from meteorological and pollution data
Potential predictive relationships between the 7-day average and anomalous values of air pollutants, meteorological factors, and the number of emergency hospital admissions of patients diagnosed with COPD are presented in Fig. 6.

Possible relationships between 7-day average values of air pollutants, meteorological factors and the number of emergency hospital admissions of patients diagnosed with COPD, Poland, 2012–2019.
Air pollutant levels and emergency hospital admissions were significantly influenced by changes in thermal conditions, especially as expressed in the values of the highest and lowest daily air temperature (Fig. 6). Change in minimum temperature may be the best predictor of changes in other environmental elements and emergency hospital admissions, although for patients aged 80 years and over more accurate would be a change in maximum temperature (Fig. 6). The strongest association between changes in air pollutant levels and hospital admissions was observed for SO2, PM2.5, and PM10, respectively. Analysis of the average variability of these factors across Poland was the best predictor of upcoming changes in the need for urgent hospital care for COPD patients (Fig. 6).
Discussion
This nationwide analysis confirmed that elevated levels of particulate and gaseous air pollutants as well as variations in meteorological factors are associated with an increase in the number of emergency hospital admissions of patients diagnosed with COPD. SO2 levels and temperature variations (especially Tmax and Tmin) were the most important factors associated with emergency hospital admissions. Sulphur dioxide has a demonstrated strong irritant effect on the respiratory tract, and interestingly, a higher rate of respiratory problems after exposure to SO2 was also found in regions of the world with a different climate profile. In the work of Phaswan et al. (published in 2022) a preceding 5-day average SO2 exposure had the largest loss (7.5 L/minute) in PEFR in young patients from South Africa36. Women diagnosed with COPD as well as inhabitants of urban areas showed stronger and faster responses to changes in environmental elements (air pollution levels and meteorological factors). The group of patients aged 60–79 showed the strongest increase in the number of emergency hospitalizations in response to changes in environmental conditions.
Associations between air pollution and hospitalizations of patients with COPD were documented in several studies from Poland12, Germany15, Italy17, England26 and China13,16. In a time‑stratified, case‑crossover study (2011–2018) concerning 26,948 hospital admissions due to COPD exacerbations in 3 largest urban agglomerations in Poland, Dąbrowiecki et al. showed that PM2.5, PM10, NO2, and SO2 levels were associated with an increased risk of COPD exacerbations that needed hospitalization12. Dąbrowiecki et al. reported a peak with 10-day lag for PM2.5 and PM10 exposure and no lag for SO2 and NO2 exposure12. In this study, a nationwide data on all emergency hospital admissions of patients with COPD were used. In line with the study by Dąbrowiecki et al., imissions of PM2.5, PM10, SO2, NO2, and NOx were significantly associated with the number of emergency hospital admissions of patients with COPD. However, in this study, different day lags were observed when compared to Dąbrowiecki et al., including 5 days vs. 10 days for PM10, 20 days vs. 5 days for PM2.5, 20 days for SO2 and 25 days for NO2 vs. no day lag in study by Dąbrowiecki et al.12. Differences between this study and the study by Dąborwiecki et al. may result from the fact that in this study nationwide data were used (including urban and rural inhabitants), compared to 3 largest urban agglomerations in a study by Dąbrowiecki et al.12. Moreover, in this study separated analyses by sex, age, and place of residence were presented.
Hoffmann et al. showed that exposure to NO2 in the metropolitan area of Berlin (Germany) was associated with an increased risk of COPD exacerbation15. In the study by Hoffmann et al. there were no associations between ozone exposure and particulate air pollutants (PM2.5 and PM10) and risk for COPD exacerbation15. Pini et al. showed that among 431 COPD patients in Brescia (Italy), both PM2.5 and PM10 exposures were significantly associated with the risk of COPD exacerbation and hospital admission17. Cheng et al. based on 4014 hospital admissions for COPD in Jijan (China) between 2014 and 2020, showed that SO2 and NO2 exposure was associated with increased risk of hospital admission16. In the study by Cheng et al. there were no associations between PM2.5, PM10, CO, and ozone levels and risk of hospital admission16. Moreover, Cheng et al. reported that the health effects of increased SO2 concentration were stronger in women16, which is in line with the data presented in this study. In a nationwide case-crossover study in England (2007–2018) published by Konstantinoudis et al., the association between ambient heat exposure and COPD hospitalizations was reported26. Konstantinoudis et al. reported a 1.47% increase in the COPD-related hospitalization risk for every 1 °C increase in temperatures above 23.2 °C26. In this study, temperature variations were also identified as important factors associated with the risk of emergency hospital admission. There are limited data on meteorological factors and COPD hospitalizations25,26 so direct comparisons with other studies are unavailable.
Among all EU member states, Poland is the country with one of the highest levels of air pollution10. Data on emergency admissions of patients with COPD were driven from the nationwide registry, so different populations and regions of the country were included in this analysis. Compared to previously published data, this study also presented a separated analysis by sex, age, and place of residence. Epidemiological data showed that there is a growing COPD burden in females, and sex differences in COPD incidence and mortality are blurring27. Findings from this study showed that women diagnosed with COPD had stronger and faster responses to changes in air pollution levels and variations of meteorological factors. This observation is in line with epidemiological data on the growing COPD burden in women27. As expected, the lowest associations between environmental factors and emergency hospital admissions were observed among the youngest patients (40–59 years). COPD is a progressive chronic disease, so younger patients may present mild to moderate COPD and are less vulnerable to exacerbations1,14. The greatest associations were observed among COPD patients aged 60–79, which may partially result from the fact that this age group is the most numerous as well as due to the clinical course of the disease1,14. Age is a risk factor for COPD as well as may influence worse psychological and clinical outcomes, so older adults with COPD are at higher risk of exacerbation in response to air pollution exposure14.
Urban inhabitants are generally exposed to higher levels of air pollution, e.g., related to urban traffic and industrialization37,38. In this study, urban inhabitants showed stronger and faster responses to changes in environmental elements. This observation underlines the need to strengthen local interventions related to the mitigation of air pollution emissions as well as the implementation of policies related to healthy and sustainable cities39,40.
The complex interactions between emergency hospital admission, SO2 levels, and maximum air temperature (Tmax) values were presented that pose an attempt to visualize the complexity of environmental research and the multifactorial nature of health events related to respiratory health. SO2 levels, followed by PM2.5 and PM10 levels were the best predictors of further increase in the emergency hospital admissions of patients diagnosed with COPD, so monitoring of these air pollutants may be used to forecast utilization of healthcare resources related to respiratory care.
This is the first nationwide study analyzing associations between air pollution, meteorological factors, and emergency hospital admissions of patients diagnosed with COPD. Findings from this study indicate an urgent need to improve the quality of air in Poland as with an increase in air pollution levels, an increase in the number of emergency hospital admissions was observed10. Moreover, data presented in this study may pose a basis for developing early warning systems that will inform patients and healthcare providers about weather conditions that may be associated with the higher number of emergency hospital admissions of patients with chronic respiratory diseases.
Limitations
This study has typical limitations for correlation analysis41. Moreover, this nationwide analysis was limited to one respiratory disease – COPD that was identified using ICD-10 code J4429. In some studies, other ICD-10 codes like J42, and J43 were used to identify patients with COPD42. However, ICD-10 code J44 was also used in other studies on COPD and air pollution in Poland12. The scope of analysis was limited to 5 air pollutants and 5 meteorological factors selected based on literature review and data availability7,12,13,15,16,17,25,26. Further studies may include a wider range of air pollutants, as well as regional differences mediated by other e.g., socioeconomic factors. Conversely for a given sample, the number of patients narrowed down to a specific medical indication may be too small to make qualitative statistical inferences. The number of stations that measured air quality and synoptic characteristics over Poland was moderate; their location may not fully reflect local specifics, so the results should be treated at a general level. Further analyses may include more extended data on environmental factors.
In conclusion, this study confirmed significant associations between air pollution levels, meteorological factors, and the number of emergency hospital admissions of patients diagnosed with COPD. Variation of SO2 levels has the greatest association with emergency hospital admissions. Among patients urgently admitted to the hospital with COPD, women, individuals aged 60–79, and inhabitants of urban areas were more vulnerable to the health impact of ambient air pollution exposure and meteorological factors variation. Complex relationships between SO2 levels and temperature variation indicate the interaction of these environmental factors that may have significant health effects in patients with respiratory diseases.
Data availability
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.
References
Pozzer, A. et al. Mortality attributable to ambient air pollution: A review of global estimates. Geohealth 7(1), e2022GH000711. https://doi.org/10.1029/2022GH000711 (2023).
GBD 2021 Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: A systematic analysis for the global burden of disease study 2021. Lancet 403(10440), P2162–2203. https://doi.org/10.1016/S0140-6736(24)00933-4 (2024).
Manisalidis, I., Stavropoulou, E., Stavropoulos, A. & Bezirtzoglou, E. Environmental and health impacts of air pollution: A review. Front. Public Health 8, 14. https://doi.org/10.3389/fpubh.2020.00014 (2020).
Kim, Y. & Radoias, V. Severe air pollution exposure and long-term health outcomes. Int. J. Environ. Res Public Health 19(21), 14019. https://doi.org/10.3390/ijerph192114019 (2022).
Bălă, G. P., Râjnoveanu, R. M., Tudorache, E., Motișan, R. & Oancea, C. Air pollution exposure-the (in)visible risk factor for respiratory diseases. Environ. Sci. Pollut. Res. Int. 28(16), 19615–19628. https://doi.org/10.1007/s11356-021-13208-x (2021).
Tiotiu, A. I. et al. Impact of air pollution on asthma outcomes. Int J. Environ. Res. Public Health 17(17), 6212. https://doi.org/10.3390/ijerph17176212 (2020).
World Health Organization. Air quality, energy and health. [Accessed 18 June 2024]. Available online: https://www.who.int/teams/environment-climate-change-and-health/air-quality-and-health/health-impacts/types-of-pollutants.
Dominski, F. H. et al. Effects of air pollution on health: A mapping review of systematic reviews and meta-analyses. Environ. Res. 201, 111487. https://doi.org/10.1016/j.envres.2021.111487 (2021).
Juginović, A., Vuković, M., Aranza, I. & Biloš, V. Health impacts of air pollution exposure from 1990 to 2019 in 43 European countries. Sci. Rep. 11(1), 22516. https://doi.org/10.1038/s41598-021-01802-5 (2021).
European Environment Agency. European Union emission inventory report 1990 2021 under the UNECE Convention on Long range Transboundary Air Pollution (Air Convention) 2023. [Accessed 18 June 2024]. Available online: https://www.eea.europa.eu/publications/european-union-emissions-inventory-report-1990-2021.
Khomenko, S. et al. Premature mortality due to air pollution in European cities: A health impact assessment. Lancet Planet Health 5(3), e121–e134. https://doi.org/10.1016/S2542-5196(20)30272-2 (2021).
Dąbrowiecki, P., Chciałowski, A., Dąbrowiecka, A., Piórkowska, A. & Badyda, A. Air pollution and long-term risk of hospital admission due to chronic obstructive pulmonary disease exacerbations in Poland: A time-stratified, case-crossover study. Pol. Arch. Intern. Med. 133(7–8), 16444. https://doi.org/10.20452/pamw.16444 (2023).
Duan, R. R., Hao, K. & Yang, T. Air pollution and chronic obstructive pulmonary disease. Chronic Dis. Transl. Med. 6(4), 260–269. https://doi.org/10.1016/j.cdtm.2020.05.004 (2020).
Celli, B. R. & Wedzicha, J. A. Update on clinical aspects of chronic obstructive pulmonary disease. N. Engl. J. Med. 381(13), 1257–1266. https://doi.org/10.1056/NEJMra1900500 (2019).
Hoffmann, C. et al. Asthma and COPD exacerbation in relation to outdoor air pollution in the metropolitan area of Berlin, Germany. Respir Res. 23(1), 64. https://doi.org/10.1186/s12931-022-01983-1 (2022).
Cheng, C. et al. Associations between air pollutants and hospital admissions for chronic obstructive pulmonary disease in Jinan: Potential benefits from air quality improvements. Environ. Sci. Pollut. Res. Int. 30(16), 46435–46445. https://doi.org/10.1007/s11356-023-25567-8 (2023).
Pini, L. et al. Emergency department admission and hospitalization for COPD exacerbation and particulate matter short-term exposure in Brescia, a highly polluted town in northern Italy. Respir. Med. 179, 106334. https://doi.org/10.1016/j.rmed.2021.106334 (2021).
Gutiérrez Villegas, C., Paz-Zulueta, M., Herrero-Montes, M., Parás-Bravo, P. & Madrazo Pérez, M. Cost analysis of chronic obstructive pulmonary disease (COPD): a systematic review. Health Econ. Rev. 11(1), 31. https://doi.org/10.1186/s13561-021-00329-9 (2021).
Keswani, A., Akselrod, H. & Anenberg, S. C. Health and clinical impacts of air pollution and linkages with climate change. NEJM Evid. 1(7), EVIDa2200068. https://doi.org/10.1056/EVIDra2200068 (2022).
Ebi, K. L. et al. Extreme weather and climate change: Population health and health system implications. Annu. Rev. Public Health 42, 293–315. https://doi.org/10.1146/annurev-publhealth-012420-105026 (2021).
Turrisi, T. B. et al. Seasons, weather, and device-measured movement behaviors: a scoping review from 2006 to 2020. Int. J. Behav. Nutr. Phys. Act. 18(1), 24. https://doi.org/10.1186/s12966-021-01091-1 (2021).
van Noort, S. P., Águas, R., Ballesteros, S. & Gomes, M. G. The role of weather on the relation between influenza and influenza-like illness. J. Theor. Biol. 298, 131–137. https://doi.org/10.1016/j.jtbi.2011.12.020 (2012).
Bochenek, B. et al. Weather as a potential cause of regional differences in the dynamics of COVID-19 transmission in Poland: Implications for epidemic forecasting. Pol. Arch. Intern. Med. 132(1), 16110. https://doi.org/10.20452/pamw.16110 (2022).
Danek, T., Weglinska, E. & Zareba, M. The influence of meteorological factors and terrain on air pollution concentration and migration: a geostatistical case study from Krakow, Poland. Sci Rep. 12(1), 11050. https://doi.org/10.1038/s41598-022-15160-3 (2022).
Javorac, J. et al. What are the effects of meteorological factors on exacerbations of chronic obstructive pulmonary disease?. Atmosphere 12(4), 442. https://doi.org/10.3390/atmos12040442 (2021).
Konstantinoudis, G. et al. Ambient heat exposure and COPD hospitalisations in England: A nationwide case-crossover study during 2007–2018. Thorax 77(11), 1098–1104. https://doi.org/10.1136/thoraxjnl-2021-218374 (2022).
Marshall, D. C. et al. Trends in prevalence, mortality, and disability-adjusted life-years relating to chronic obstructive pulmonary disease in Europe: An observational study of the global burden of disease database, 2001–2019. BMC Pulm Med. 22(1), 289. https://doi.org/10.1186/s12890-022-02074-z (2022).
Poznańska, A. et al. Nationwide general hospital morbidity study as a source of data about Polish population health. Przegl Epidemiol. 73, 69–80 (2019).
Jankowski, M. et al. Epidemiological characteristics of 101,471 patients hospitalized with chronic obstructive pulmonary disease (COPD) in Poland in 2019: Multimorbidity, duration of hospitalization, in-hospital mortality. Adv. Respir. Med. 91(5), 368–382. https://doi.org/10.3390/arm91050029 (2023).
World Health Organization (WHO) International Statistical Classification of Diseases and Related Health Problems 10th Revision. [Accessed 18 June 2024]. Available online: https://icd.who.int/browse10/2010/en.
Statistics Poland. National Official Register of the Territorial Division of the Country (TERYT), 2024. [Accessed 18 June 2024]. Available online: https://eteryt.stat.gov.pl/eTeryt/english.aspx?contrast=default.
Chief Inspectorate for Environmental Protection. Measurement stations. [accessed 18 June 2024]. Available online: https://powietrze.gios.gov.pl/pjp/maps/measuringstation?lang=en&woj=.
Institute of Meteorology and Water Management - National Research Institute. Weather monitoring and measurements. [accessed 18 June 2024]. Available online: https://meteo.imgw.pl/.
RDocumentation. ggtern. [accessed 18 June 2024]. Available online: https://www.rdocumentation.org/packages/ggtern/versions/3.5.0.
R Package Documentation. grangertest: Test for Granger Causality. [accessed 18 June 2024]. Available online: https://rdrr.io/cran/lmtest/man/grangertest.html.
Phaswana, S., Wright, C. Y., Garland, R. M., Khumalo, T. N. & Naidoo, R. N. Lagged acute respiratory outcomes among children related to ambient pollutant exposure in a high exposure setting in South Africa. Environ. Epidemiol. 6(6), e228. https://doi.org/10.1097/EE9.0000000000000228 (2022).
Sicard, P., Agathokleous, E., De Marco, A., Paoletti, E. & Calatayud, V. Urban population exposure to air pollution in Europe over the last decades. Environ. Sci. Eur. 33(1), 28. https://doi.org/10.1186/s12302-020-00450-2 (2021).
Cipoli, Y. A., Furst, L., Feliciano, M. & Alves, C. Respiratory deposition dose of PM2.5 and PM10 during night and day periods at an urban environment. Air Qual. Atmos. Health. 16, 2269–2283. https://doi.org/10.1007/s11869-023-01405-1 (2023).
Giles-Corti, B. et al. Creating healthy and sustainable cities: What gets measured, gets done. Lancet Glob. Health. 10(6), e782–e785. https://doi.org/10.1016/S2214-109X(22)00070-5 (2022).
Jonidi Jafari, A., Charkhloo, E. & Pasalari, H. Urban air pollution control policies and strategies: A systematic review. J. Environ. Health Sci. Eng. 19(2), 1911–1940. https://doi.org/10.1007/s40201-021-00744-4 (2021).
Janse, R. J. et al. Conducting correlation analysis: Important limitations and pitfalls. Clin. Kidney J. 14(11), 2332–2337. https://doi.org/10.1093/ckj/sfab085 (2021).
Gothe, H. et al. Algorithms to identify COPD in health systems with and without access to ICD coding: A systematic review. BMC Health Serv. Res. 19(1), 737. https://doi.org/10.1186/s12913-019-4574-3 (2019).
Acknowledgements
The authors would like to acknowledge the Department of Population Health Monitoring and Analysis, National Institute of Public Health—National Institute of Hygiene, Warsaw, Poland for data sharing.
Funding
Work performed in the frame of statutory research projects conducted by Polish. National Meteorological & Hydrological Service (PSHM) to support forecasting and early warning of threats to public safety, health, and life of citizens. There was no external funding for this study.
Author information
Authors and Affiliations
Contributions
BB: Conceptualization, Methodology, Software, Formal Analysis, Investigation. MJ: Conceptualization, Data curation, Methodology, Writing- Original draft preparation, Investigation. JW: Validation, Investigation, Methodology. MG: Visualization, Data curation, Software, Formal Analysis. PS: Resources. AJ: Writing- Reviewing and Editing. AW: Validation, Writing- Reviewing and Editing. JP: Supervision, Writing- Reviewing and Editing. MF: Supervision, Writing- Reviewing and Editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Bochenek, B., Jankowski, M., Wieczorek, J. et al. The impact of ambient air pollution and meteorological factors on emergency hospital admissions of COPD patients in Poland (2012–2019). Sci Rep 15, 21915 (2025). https://doi.org/10.1038/s41598-025-07684-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-07684-1
