
Abstract
Recent decades have seen declining total fertility rates (TFR) globally, alongside increased use of assisted reproductive technology (ART). However, TFR includes ART births and excludes induced abortions, complicating assessments of population fecundity. Here, we examine trends in cohort total fertility rates (cTFR), induced abortions, and ART use through a nationwide cohort study of 1,648,971 pregnancies, including abortions, among Danish women aged 15–45 years born between 1958 and 1999. A new index, the Comprehensive Unassisted Pregnancy Rate (live births and induced abortions, excluding ART births), was developed. Our findings reveal a decline in unassisted pregnancy rates for women born after 1961, with an accelerated decline for those born after 1970. In contrast, cTFR increased for women born between 1958 and 1970 before decreasing, driven by trends in induced abortions and ART births. These differences highlight a disconnect between cTFR and fecundity measures. The declining unassisted pregnancy rates, reduced abortions, and increased ART demand raise concerns about population fecundity. Understanding these trends’ biological and socioeconomic drivers requires large-scale, transdisciplinary studies of representative populations. Our results emphasize the need for alternative measures, like the Comprehensive Unassisted Pregnancy Rate, to assess reproductive health and fertility trends accurately.
Similar content being viewed by others


Introduction
Declining trends in fertility rates in recent decades have been reported in all parts of the World1,2. This decline has occurred in parallel with a rising number of couples seeking help to conceive in the form of treatment with assisted reproductive technology (ART)3. In almost all OECD countries, the total fertility rates (TFRs) have been below the replacement level (i.e., 2.1 children per woman) for more than a generation, resulting in ageing populations and rising concern that a deteriorating human fecundity (i.e., the biological ability to conceive) may be involved4. However, TFRs, annually reported by the World Health Organization and national agencies to inform the public and policymakers about birth rates and population development, cannot be considered a reliable marker of population-level fecundity as (a) births following ART are included in TFR and (b) pregnancies terminated by induced abortion are not considered. Furthermore, changing birth rates, as reported in TFR, may represent a change in the use of contraception or induced abortions in societies where these are made readily available. In addition, socio-economic and cultural aspects are undoubtedly influential determinants that also shape a nation’s birth rates. The effect of these aspects can moreover be detected in the tempo effects of TFR, which can distort the interpretation of fertility trends. Nevertheless, the interplay of these factors on a population’s birth rate is important and often reliant on assumptions rather than evidence, primarily due to a lack of available data. To address this gap, we have5,6 proposed to supplement existing registries with a registry that contains comprehensive information on pregnancies, including both live births and induced abortions. While this tool is in its early stages, it could serve as a starting point for exploring population-level trends in reproductive outcomes and informing future research directions.
We report new national data showing declining trends in unassisted pregnancies as expressed in the Comprehensive Unassisted Pregnancy Rate (CUPR), defined as the generation total rate of live births and induced abortions, excluding births after ART. Our findings raise questions about changes in couple fecundity of the population.
Materials and methods
Study design and study population
This nationwide registry-based time-series study includes complete information on all registered pregnancies in Denmark for women aged 15–45 years born between 1st January 1958 and 31st December 19997. The individual personal identification numbers given to all Danes at birth or permanent residency since 1968 enabled the linkage of several Danish nationwide registries (Supplemental Material Fig. 1) and naturally conceived live births, births resulting from ART (including in vitro fertilisations, oocyte donations, and frozen embryo transfers), and induced abortions were identified. In the Danish context, admittance to fertility treatment can only occur after 12-months of attempted conception without contraception. The Danish registry specifically for ART treatments was established in 19948, and induced abortions have officially been recorded since its legalisation in 19739. This setup allowed a nearly complete follow-up on registered pregnancies for women born between 1958 and 1999 from the age of 15 up until the calendar year 2019 (the misclassification of 1,554 ART pregnancies10 during the period from 1983 to 1994, the time when the registry was established, was deemed to have only a minor impact on the results). Up until 1st April 2004, a live birth was registered due to ART if the child was born 196–308 days after ART and subsequently if the child was born 154–308 days after ART. The reason for the change in counting was a change in the differentiation between spontaneous abortion and birth in Denmark from 28 to 22 weeks of gestation. Data on contraception prescriptions, including ATC codes G03A (hormonal contraceptives for systemic use) and G02B (contraceptives for topical use) in the period 1995–2020 was retrieved from the prescription registry11 to add information on an additional factor influencing pregnancy rates.

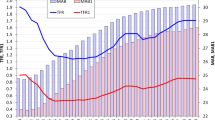
Cohort total fertility rates (green) and Comprehensive Unassisted Pregnancy Rate (red) of Danish birth cohorts. The X-axis represents the birth cohorts from 1958 to 1983. The Y-axis represents the cohort total fertility rate (cTFR) and Comprehensive Unassisted Pregnancy Rate (CUPR), ranging from 0.0 to 2.5. Two plotted trend lines further indicate the rates. Note that the measures show opposite trends from 1961 to 1970, with a gradual shift in their difference from 0.53 for women born in 1958 to 0.31 for women born in 1983.
Statistical analysis
Cohort total fertility rates, total induced abortion rates and total ART birth rates were calculated as the number of births or pregnancies per woman within each cohort1:
The rates were calculated for all cohorts c that are observed from age xmin that is equal to age 15 until age 40 or older in 2023. The cohort total fertility rate was defined as the total number of children that are born to a woman over her lifetime as a result of spontaneous or assisted conception through ART. Women’s age at the birth of a child or induced abortion was calculated by subtracting the date of birth of the child or the date of induced abortion from the date of birth of the woman. The number of women within their reproductive lifetime was calculated as the number of women alive in Denmark within the same birth cohort by the 1st of July within a year. It was calculated for each birth cohort of women born between 1958 and 1999 and for each 1-year or 5-year age group using data from the Danish Population Register. Age- and cohort-specific CUPR were calculated by adding cTFRs and induced abortion rates followed by subtraction of ART birth rates, and defined as the total number of pregnancies resulting in live birth or induced abortion, but excluding births after ART. CUPR, which is conceptually identical with the previously used term Total Natural Pregnancy Rate12, provides a more precise and neutral descriptor and is used throughout this paper.
The CUPR rates were calculated by summarising consecutive age-specific rates for birth cohorts 1958–1999. The CUPR is proposed here as a proxy measure intended to approximate the population-level unassisted pregnancy rate (live births and induced abortions). It does not directly measure biological fecundity, and should therefore be interpreted with caution and not as a definitive indicator of fecundity. For the cohorts 1979–1983 the CUPR and cTFR was calculated until the highest possible age in 2023 (i.e. 40 years in 2023).
Ethical approval
This study was conducted using data from national registers only. According to Danish law, ethics approval is not needed for this type of research under the Scientific Ethical Committee Act. All data management and analyses were carried out on Statistics Denmark’s secure research servers. The study only contains aggregated results and no personal data.
Results
The registry linkage identified 1,039,634 pregnancies resulting in a live birth, of which 20,248 were live births following ART and 609,337 pregnancies resulting in an induced abortion (Supplemental Material Fig. 1).
All birth cohorts had cTFRs below the population replacement level of 2.1 children per woman (Fig. 1). The cTFR depicted an increase from women born in 1958 (1.86 children per woman) to women born in 1970 (1.99 children per woman), followed by a decrease for women born until 1983 (1.87 children per woman). A slight increase in the CUPR was observed for women born between 1958 (2.40 pregnancies per woman) and 1961 (2.45 pregnancies per woman), whereafter the CUPR decreased for the following cohorts, reaching 2.26 pregnancies per woman in the 1983 cohort (Fig. 1).
In general, women across successive birth cohorts tended to have fewer births at younger ages. However, total and cumulative cohort fertility rates caught up at older ages and increased until the 1970 cohort (Figs. 1 and 2). In contrast, there was a distinct decline in CUPR across all age groups for each birth cohort younger than the 1961 cohort (Fig. 3).

Cumulative birth rates across birth cohorts of women born between 1958 and 1999. The X-axis represents women’s ages from 15 to 45 years. The Y-axis represents the cumulative birth rate per woman, ranging from 0.0 to 2.5. Multiple cohort lines ranging from the 1958 to the 1999 birth cohort are plotted on the figure. Each line indicates the respective cohort’s cumulative birth rate, starting from the lowest values at age 15 and peaking before age 45.

Comprehensive Unassisted Pregnancy Rates (CUPR) across birth cohorts of women born between 1958 and 1999. The X-axis represents women’s ages from 15 to 45 years. The Y-axis represents the cumulative CUPR, ranging from 0.0 to below 2.5. Multiple cohort lines ranging from the 1958 to the 1999 birth cohort are plotted on the figure. Each line indicates the respective cohort’s CUPR, starting from the lowest values at age 15 and peaking before age 45.
Women in successive cohorts exhibited a decrease in induced abortion rates across all age groups, except those born between 1985 and 1989, where the rates surpassed the three preceding cohorts (Supplemental Material Fig. 2A). Finally, there was a noticeable and gradual rise in the cohort birth rate following ART among younger cohorts and at younger ages (Supplemental Material Fig. 2B). Excluding intrauterine inseminations from the CUPR had only minor effects (Supplemental Material Fig. 2).
Discussion
In this study, utilizing data linked to personal identification numbers from nationwide registries, we were able to do a complete follow-up of all Danish women on their pregnancies covering (1) all births, (2) a separate registry on births after ART, and (3) a registry on induced abortions. Our results based on observed data align with our previous projections5,6, and we observed a decline in the Comprehensive Unassisted Pregnancy Rate (CUPR) within complete follow-up of birth cohorts of women born from 1961 onward. These changes unfolded consistently across successive decades, from their adolescence to the conclusion of their reproductive period. Notably, a rise in total births co-occurred with a decline in CUPR until the cohort of women born in 1970. These contradictory trends indicate a clear difference between the two rates and that CUPR, reflecting unassisted pregnancies (including induced abortions), is potentially better fitted as a proxy of fecundity than rates of total births. The overall declines observed in the number of pregnancies pose an essential question on whether these trends are a consequence of women’s and couples’ deliberate intentions to have fewer children than preceding birth cohorts or whether the decreases are a possible consequence of increasing reproductive health issues in the population, or lastly, whether the declines are due to a combination of reproductive health and sociocultural factors. E.g. if socio-cultural factors postpone the onset of reproduction (i.e. increased maternal and paternal age), which again would impose reduced fecundity or if reduced fecundity delays reproductive success.
Results in the context of what is known
If the declining pregnancy rates were, in fact, due to a collective change in desire for fewer children and fecundity was constant, it could be anticipated that unplanned pregnancies would more frequently result in abortions. Contrary to this anticipation, abortion rates have also declined within the same period (Supplemental Material Fig. 2A). This trend could be attributed to pregnancies becoming more planned recently. However, reports have shown that despite the availability of modern contraception, approximately half of all pregnancies are unintended, though not necessarily unwelcome13,14. Such pregnancies may occur during assumed ‘safe’ periods, during a change of contraceptive method, or due to forgetfulness. Yet, we observed a decline in prescribed contraception use amongst cohorts of Danish women, especially at younger ages (Supplemental Material Fig. 2C), providing little evidence that the declining abortion rate was a reflection of increased use of contraception. While the simultaneous decline in both the induced abortion and contraceptive prescription rates may be independent of one another, they both point to broader changes in reproductive behaviours. Although the relationship between these trends and how their decline impacts the CUPR is speculative, it is worth considering further, as it could provide valuable insights into the factors influencing population-level fecundity. The change in the abortion rate could also express a change in population fecundity, as suggested in a recent study15,16,17,18.
Study implications
Based on our findings, the declining pregnancy rates can not solely be accounted for by changes in contraception practices. Thus, it is imperative to explore additional, contributing factors. It is well documented that infertility and the need for ART are prevalent among young couples in Denmark, as well as globally, where there has been a decline in semen quality19,20,21. There has moreover been a rise in the incidences of male reproductive disorders22,23. These reproductive health problems have occurred within a short span of one or two generations, making genetic alterations an unlikely explanation. However, evidence has accumulated that environmental pollutants may be involved24,25,26. The mammalian foetal testis is particularly vulnerable to chemical exposures, which have been associated with testicular dysgenesis syndrome both in animal models and humans. This syndrome, besides cryptorchidism and hypospadias, may also manifest late effects in the form of poor semen quality, infertility, and testicular cancer2.
Exposures to endocrine disruptors may impact female reproductive health as well27. However, our recent literature review did not find substantial evidence of similar trends in female reproductive health2. Nonetheless, the global incidences of polycystic ovary syndrome28 and uterine fibroids29 have been reported to be increasing. Furthermore, the trend among young couples to postpone family planning until the female partner is above 30 (and physiologically less fecund) may decrease the chances of conception for some couples2. Physiological ageing of the ovary, combined with poor semen quality of the male partner, may well explain some of the trends in declining CUPR.
Strengths and limitations
The unique Scandinavian registry system with personal identification numbers made this study possible. It provided a complimentary tool to assist in the surveillance of all pregnancies in the population, thereby potentially reflecting changes in fecundity. The possibility of capturing all pregnancies by their source and including ART and induced abortions makes these nationwide trends highly relevant. While the comprehensive nature of the Danish registry data allows for detailed tracking of pregnancy trends, it remains an observational dataset, and alternative explanations, such as changing reproductive behaviour, must also be considered. Trends in societal norms, contraceptive efficacy and use, pregnancy timing, or changes in sexual activity could all influence CUPR independent of fecundity. Furthermore, a limitation of the current study is that our data do not allow us to differentiate between medically necessary and elective-induced abortions. While conceptions linked to medically necessary abortions are generally less likely to result in a successful live birth, the CUPR does not account for this distinction. As a result, CUPR may include abortions that could have different implications for fertility outcomes compared to elective abortions. Also, the availability of the morning-after pill since 2014 may have led to an underestimation of medically induced abortions. Therefore, some conceptions may not have been captured in our data. The morning-after pill can be purchased over the counter in Denmark16,17 and is thus not reflected in the contraceptive use shown in supplementary Fig. 2C. Nonetheless, its impact on CUPR is likely to be limited as a first-time contraceptive compared to other methods (2.1% in 2011–2012)16, particularly when considering a 20–25% chance of conception18. Furthermore, a minor limitation is the lack of complete information on fertility for birth cohorts born between 1979 and 1983, covering ages 44 and below in 2023. This limitation is, however, expected to be minor given that only about 2% of births occur after age 40.
Though we may observe a declining CUPR, our data does not allow us to isolate or directly measure fecundity. While the CUPR is designed as a population-level measure of pregnancy rates, rather than an individual-level assessment of fecundity, it is important to recognize that ART outcomes result from both female and male reproductive factors. Given these limitations, we emphasize that CUPR is a preliminary, registry-based indicator rather than a definitive measure of fecundity. Rather than replacing established metrics, it offers a complementary perspective on unassisted conception rates in a population. We recognize that additional data and methodologies, such as large-scale transdisciplinary studies of representative population samples, are necessary to address this complex question definitively.
Conclusion
In conclusion, our findings that decreasing unassisted birth rates were associated with simultaneous decreasing trends in rates of induced abortion and a high need for ART may reflect a deterioration in the fecundity of the population. However, to get a complete picture of the fertility trends, we urgently need relevant large-scale population data on behavioural and biological factors, such as voluntary and involuntary childlessness and the complex economic, social and educational profiles of young couples attempting to conceive.
Data availability
Data is provided within the supplementary information files.
References
Vollset, S. E. et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: A forecasting analysis for the global burden of disease study. Lancet 396(10258), 1285–1306 (2020).
Skakkebæk, N. E. et al. Environmental factors in declining human fertility. Nat. Rev. Endocrinol. 18(3), 139–157 (2022).
Fauser, B. C. J. M. et al. Declining global fertility rates and the implications for family planning and family building: An IFFS consensus document based on a narrative review of the literature. Hum. Reprod. Update 30(2), 153–173 (2024).
Smarr, M. M. et al. Is human fecundity changing? A discussion of research and data gaps precluding us from having an answer. Hum. Reprod. 32(3), 499–504 (2017).
Jensen, T. K. et al. Declining trends in conception rates in recent birth cohorts of native Danish women: A possible role of deteriorating male reproductive health. Int. J. Androl. 31(2), 81–92 (2008).
Lassen, T. H. et al. Trends in rates of natural conceptions among Danish women born during 1960–1984. Hum. Reprod. 27(9), 2815–2822 (2012).
Bliddal, M., Broe, A., Pottegård, A., Olsen, J. & Langhoff-Roos, J. The Danish Medical Birth Register. Eur. J. Epidemiol. 33, 27–36 (2018).
Jølving, L. R., Erb, K., Nørgård, B. M., Fedder, J. & Larsen, M. D. The Danish National Register of assisted reproductive technology: Content and research potentials. Eur. J. Epidemiol. 36(4), 445–452 (2021).
Knudsen, L. B. Induced abortions in Denmark. Acta Obstet. Gynecol. Scand Suppl. 164, 54–59 (1997).
Andersen, A. N. In vitro fertilisation during 40 years. Ugeskr Laeger 183(23), V04210371 (2021).
Pottegård, A. et al. Data resource profile: The danish national prescription registry. Int. J Epidemiol. 46(3), 798–798f (2017).
Lassen, T. H. et al. Trends in rates of natural conceptions among Danish women born during 1960–1984. Human Reprod. 27(9), 2815 (2012).
Bearak, J. et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: Estimates from a comprehensive model for 1990–2019. Lancet Glob. Health 8(9), e1152–e1161 (2020).
Finer, L. B. & Zolna, M. R. Declines in unintended pregnancy in the United States, 2008–2011. N. Engl. J. Med. 374(9), 843–852 (2016).
Lidegaard, Ø., Zernichow Borberg, H. V., Rasmussen, S. C. & Mikkelsen, A. P. Lifetime induced abortions and live births. A 40-year historical cohort study. J. Obstet. Gynaecol. Can. 46, 102612 (2024).
Guleria, S. et al. Contraceptive non-use and emergency contraceptive use at first sexual intercourse among nearly 12 000 Scandinavian women. Acta Obstet. Gynecol. Scand 96(3), 286 (2017).
Guleria, S. et al. Emergency contraceptive pill use among women in Denmark, Norway and Sweden: Population-based survey. Acta Obstet. Gynecol. Scand 99(9), 1214 (2020).
Chua, S. J. et al. Age-related natural fertility outcomes in women over 35 years: A systematic review and individual participant data meta-analysis. Hum. Reprod. 35(8), 1808 (2020).
Carlsen, E., Giwercman, A., Keiding, N. & Skakkebaek, N. E. Evidence for decreasing quality of semen during past 50 years. BMJ 305(6854), 609–613 (1992).
Levine, H. et al. Temporal trends in sperm count: A systematic review and meta-regression analysis of samples collected globally in the 20th and 21st centuries. Hum. Reprod. Update 29(2), 157–176 (2023).
Jensen, T. K. et al. Poor semen quality may contribute to recent decline in fertility rates. Hum. Reprod. 17(6), 1437–1440 (2002).
Znaor, A. et al. Testicular cancer incidence predictions in Europe 2010–2035: A rising burden despite population ageing. Int. J. Cancer 147(3), 820–828 (2020).
Znaor, A. et al. Global patterns in testicular cancer incidence and mortality in 2020. Int. J. Cancer 151(5), 692–698 (2022).
Govarts, E. et al. Harmonized human biomonitoring in European children, teenagers and adults: EU-wide exposure data of 11 chemical substance groups from the HBM4EU Aligned Studies (2014–2021). Int. J. Hyg. Environ. Health 249, 114119 (2023).
Buckley, J. P. et al. Exposure to contemporary and emerging chemicals in commerce among pregnant women in the United States: The environmental influences on child health outcome (ECHO) program. Environ. Sci. Technol. 56(10), 6560–6573 (2022).
Maekawa, R. et al. Evidence of exposure to chemicals and heavy metals during pregnancy in Japanese women. Reprod. Med. Biol. 16(4), 337–348 (2017).
Johansson, H. K. L. et al. Putative adverse outcome pathways for female reproductive disorders to improve testing and regulation of chemicals. Arch. Toxicol. 94(10), 3359–3379 (2020).
Liu, J. et al. Measuring the global disease burden of polycystic ovary syndrome in 194 countries: Global burden of disease study 2017. Hum. Reprod. 36(4), 1108–1119 (2021).
Li, B., Wang, F., Chen, L. & Tong, H. Global epidemiological characteristics of uterine fibroids. Arch. Med. Sci. 19(6), 1802–1810 (2023).
Funding
This work was supported by the Research Fund of Rigshospitalet, Copenhagen University Hospital; and the Johannes Clemmesen’s Research Foundation.
Author information
Authors and Affiliations
Contributions
RLJ: Conceptualisation, Methodology, Software, Formal analysis, Investigation, Resources, Data curation, Visualisation, Project administration, Funding acquisition, Writing—Original Draft. ALB: Conceptualisation, Methodology, Investigation, Project administration, Funding acquisition, Writing—Original Draft. LP: Conceptualisation, Investigation, Writing—Review & Editing. SAH: Investigation, Writing—Review & Editing. AMA: Investigation, Writing—Review & Editing. AJ: Investigation, Writing—Review & Editing. NES: Conceptualisation, Methodology, Formal analysis, Investigation, Project administration, Supervision, Writing—Original Draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lindahl-Jacobsen, R., Beck, A.L., Priskorn, L. et al. Changes in the comprehensive unassisted pregnancy rate as a possible marker of declining human fecundity. Sci Rep 15, 23916 (2025). https://doi.org/10.1038/s41598-025-08332-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-08332-4
