
Abstract
Paraben esters are commonly used as preservatives in cosmetics, personal hygiene products, food and drugs. However, there is a lack of evidence regarding the impact of exposure to Paraben esters on adolescent liver function. We analyzed data from the 2007–2016 National Health and Nutrition Examination Survey (NHANES). Finally, a random sample of 1845 adolescents aged 12 to 19 was selected for the study. The effect of urinary parabens on liver function indexes was analyzed using weighted linear regression to ensure accurate representation of the population. Then, we applied the weighted quantile sum (WQS) analysis and the Bayesian kernel machine regression (BKMR) to examine the associations between parabens and liver function indicators. Based on the results from three different models, four parabens and their total were negatively associated with Albumin (ALB) and Alkaline Phosphatase (ALP), and positively associated with Total Bilirubin (TBIL). Moreover, among the parabens, butyl paraben and propyl paraben had the highest weights. Overall, our results indicate that parabens are significantly but weakly associated with changes in liver function in US adolescents. Further research is needed to explore these relationships.
Similar content being viewed by others


Introduction
Parabens are a widely used class of preservatives in cosmetic and pharmaceutical products. These compounds are esters of p-hydroxybenzoic acid, include methyl paraben, ethyl paraben, propyl paraben, and butyl paraben. As acidic preservatives, they are effective in a variety of formulations1,2. While the FDA generally recognizes parabens as safe when used in small amounts, some people may be sensitive to them. Studies have reported that common food preservatives, such as sodium bisulfite and sodium metabisulfite, exhibit bactericidal and bacteriostatic effects on beneficial gut bacteria at safe food concentrations3. Parabens display estrogen-like activity by binding to estrogen receptors (ER) and other related receptors (e.g., ERRγ), mimicking estrogen’s effects. At low concentrations, para-hydroxybenzoates can also induce the proliferation of breast cancer cells (e.g., MCF-7 cells). Moreover, combined exposure to multiple parabens significantly enhances cell proliferation compared to individual exposure4. In addition, some studies have suggested that certain preservatives may be harmful to beneficial bacteria in the human body. Some common acidic preservatives include benzoic acid, sorbic acid5,6,7,8,9,10. and propionic acid. Despite Americans, high exposure to these endocrine-disrupting parabens, few studies have examined their potential health effects.
Liver diseases, including non-alcoholic liver disease, alcoholic liver disease, and viral hepatitis, are major contributors to morbidity and mortality on a global scale. An estimated 2 million people succumb to these illnesses annually11. Nonalcoholic liver disease continues to increase in the general adolescent population, but immunization and new drugs have reduced the burden of viral liver disease12, Ultimately, this leads to more cases of end-stage liver disease, such as liver failure, cirrhosis, and liver cancer. Exposure to environmental chemicals, along with factors such as alcohol consumption, viral infections, genetic predisposition, and unhealthy lifestyle choices, has been linked to liver dysfunction in teenagers13,14.
The liver plays an important role in the detoxification of parabens. While studies have shown that exposure to parabens does not affect liver function in children15, studies linking paraben exposure to liver function in young adults are lacking. It should be noted that liver dysfunction is a process of gradual damage to the liver, early prevention and intervention can significantly reduce the incidence of adult liver disease16. The objective of this study was to investigate the correlation between paraben exposure and indicators of liver function among US adolescents aged 12–19 years, using a sample that is representative of the nation as a whole.
To achieve this objective, we used data from the National Health and Nutrition Examination Survey (NHANES) conducted by the Centers for Disease Control and Prevention (CDC) from 2007 to 2016. NHANES is a cross-sectional survey that collects information on the health and nutritional status of the US population through interviews and physical examinations.
Materials and methods
Data collection
The National Health and Nutrition Examination Survey (NHANES, https://wwwn.cdc.gov/nchs/nhanes/) is a collection of surveys conducted across the United States. These surveys are designed to be representative of the non-institutionalized population of US citizens and are conducted using a multilevel stratified probability sampling method. We analyzed data from 2007 to 2016, which were collected in five phases (2007–2008, 2009–2010, 2011–2012, 2013–2014 and 2015–2016). A total of 31,951 participants had complete liver function test data. Out of the total number of samples, 10,244 were part of the urine parabens subset and had complete data on parabens without any missing values. The study sample consisted of 1,852 participants between the ages of 12 and 19, but 7 samples with TBIL = 0 needed to be excluded. In the absence of complete documentation, including liver function tests and covariates, adolescents who were seropositive for hepatitis B virus or hepatitis C virus were excluded. Ultimately, 1,845 adolescents were selected as the final sample (see Fig. 1 and Table S1). The 2007–2016 NHANES survey protocol was reviewed and approved by the Institutional Review Board of the Centers for Disease Control and Prevention (CDC) National Center for Health Statistics. All participants gave written informed consent.

Flowchart of obtaining data from research subjects.
Liver function measure outcomes
Fasting blood samples were collected from NHANES participants aged 12 years and older at a mobile screening center after fasting. The samples were then refrigerated and shipped to a central laboratory where serum markers of liver function were measured using a Beckman Coulter DxC800 Synchron clinical system17. The liver is abundant in alanine aminotransferase (ALT) and aspartate aminotransferase (AST), and their serum levels increase when there is damage to the liver cell membrane or hepatocytes undergo necrosis18. The AST/ALT ratio is a useful tool in distinguishing between acute and chronic liver diseases during differential diagnosis. Albumin (ALB) is synthesized only in the liver. Impaired liver function results in decreased albumin (ALB) and total protein (TP)19. Alkaline phosphatases (ALPs) are a group of isoenzymes found on the outer layer of cell membranes, where they catalyze the hydrolysis of organic phosphate esters in the extracellular space. They are also present in the cytosol of liver cells and on the canalicular membrane of hepatocytes20. Gamma glutamyl transferase (GGT) is an important reference diagnostic index indicative of liver disease and disorders of the biliary tract, especially cholestasis21. Bilirubin is a yellow pigment produced by the liver when it breaks down old red blood cells. The liver converts water-insoluble indirect bilirubin into water-soluble direct bilirubin, which is then excreted through bile. Impaired liver function can cause bilirubin to accumulate in the blood, resulting in jaundice22.
Measurements of paraben
Participants provided urine samples during the visit. The samples were transported on dry ice to the National Center for Environmental Health at the Centers for Disease Control and Prevention and were kept at a temperature below − 20 °C until they were analyzed. Urine Total Concentration—Propyl paraben (PP), Butyl paraben (BP), Ethyl paraben (EP) and Methyl paraben (MP)23 determined by online high performance liquid chromatography using solid phase extraction and tandem mass spectrometry (https://wwwn.cdc.gov/Nchs/Data/Nhanes/Public/2011/DataFiles/EPH_G.htm, https://wwwn.cdc.gov/nchs/data/nhanes/public/2011/labmethods/EPH_G_met.pdf). The limit of detection (LOD) for each phenol and paraben was calculated as 3S0. where S0 is the standard deviation when the concentration is close to zero. The LOD for both EP and MP was 1.0 ng/ml. The LOD values for PP and BP have varied over the years, ranging from 0.1 to 0.2 ng/mL. For participants who scored below the LOD, their score was calculated as the LOD divided by the square root of 2. This approach was recommended by the Centers for Disease CDC during their review of the NHANES data. Low-level and high-level quality controls for each paraben were analyzed using standards, reagent blanks, and NHANES samples, respectively. Creatinine is measured using the Jaffe rate method with the Beckman UniCel® DxC800 Synchron clinical system (https://wwwn.cdc.gov/nchs/data/nhanes/public/2011/labmethods/biopro_g_met_creatinine.pdf). All procedures were conducted in accordance with the relevant year’s Laboratory Procedures Manual published by the CDC, which provides detailed laboratory analysis methods for the NHANES, including the calculation of the LOD (https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/overviewlab.aspx?BeginYear=2015).
Covariates
Data collection for each wave included standardized home interviews, detailed physical examinations, and follow-up visits to mobile screening centers. Household interviews collected data on age, race/ethnicity, sex, and education level using standardized questionnaires. Height and weight were measured by trained interviewers during visits to the mobile screening center (https://wwwn.cdc.gov/nchs/nhanes/search/datapage.aspx?Component=Examination&CycleBeginYear=2011), and BMI was calculated (weight [kg]/height [m2]).
Statistical analysis
Demographic characteristics were reported as percentages. Quartile range and Mean ± SD were used to describe parabens concentrations and liver function levels. In all statistical analyses, urine creatinine was used to adjust the concentrations of parabens. To make them normally distributed, paraben concentrations adjusted for creatinine and liver function indices were naturally log-transformed24. Spearman’s coefficient was used to test for pairwise correlations of paraben concentrations. We used study weighted linear regression to examine the relationship between urinary parabens and indicators of liver function, producing direct and understandable results. The rationale behind these models is as follows: Model I: The base model, which does not include any covariate adjustments. We first present this model to illustrate the raw association between the independent and dependent variables and to establish the unadjusted trend. Model II: This model incorporates adjustments for age and gender, as these factors are well-recognized potential confounders that may influence the observed relationships. By controlling for these variables, we aim to obtain a more refined understanding of the independent–dependent variable relationship while accounting for demographic influences. Model III: In addition to age and gender, this model further adjusts for race and BMI, as these variables are also key contributors to health outcomes. Including these covariates in the final model ensures greater accuracy and reliability of the results, mitigating potential confounding effects. This stepwise adjustment approach is a commonly applied methodology in cross-sectional studies utilizing the NHANES database, allowing for a more comprehensive examination of covariate influence on the main associations. Subsample weights for parabens were used in all analyses, to account for complex sample designs and nonresponse to NHANES. The total weight for the NHANES collection cycle is calculated according to NHANES guidelines, specifically implemented using the “survey” package in R.
To evaluate the combined effect of parabens on liver function indicators, we applied weighted quantile sum regression models (WQS)25. This method can calculate the individual’s total exposure burden value26 by finding the weights and concentrations of different parabens that are related to the outcome, analyzing the overall exposure levels of a group of highly correlated parabens, and discovering the parabens that are more influential on the outcome. This method took into account all parabens and assumed that they all had the same direction of relationship with liver function indicators. The paraben regression model estimated a weighted linear index that reflected the whole-body load of parabens. The weight of each paraben reflects its weight in the WQS Index. Specifically, this study created quartile-based WQS indices for these parabens. Because we lacked a priori knowledge of liver function markers and individual parabens, we ran two models using WQS regression analysis. In one model, we hypothesized that all components of the WQS index would be positively associated with liver function markers. In contrast, the second model assumes that all index components are generally negatively correlated. The regression coefficient of the WQS index was interpreted as the mean change in the liver function index. In this study, bootstrap = 200,quantile = 4.validation = 0.6, seed = 2023. This step was implemented using the gWQS package in R.
Next, we applied the BKMR model, which enables us to detect potential interactions among multiple pollutants and account for exposure-response associations for each mixture component27.
R 4.2.2 was used to perform all statistical analyses. All test results are two-sided, P < 0.05.
Ethical approval and participant consent
The Research Ethics Review Board of the National Center for Health Statistics has endorsed the protocol for the NHANES. Written informed consent has been secured from each individual participating in the NHANES.
Results
Study population
Table 1 displays the characteristics of the study subjects. Of the 1845 participants, male subjects accounted for 52.5% and the average age was 15.5 ± 2.3 years. Non-Hispanic White was the majority of participants and 82.9% of participants reported education less than high school. Among the study participants, 52.0% have a Body Mass Index (BMI) within the normal range. In comparison with the entire NHANES cohort within the selected age range and sampling period, this subset of participants showed similar demographic trends, although certain differences in age distribution and education levels may provide additional context for interpreting the results. This demographic comparison helps to contextualize the findings and further enhance the generalizability of the study outcomes.
Levels of liver function indicators and urinary parabens
Table 2 presents descriptive statistics for liver function and paraben indicators.
The results of the liver function indicators are as follows: TP had a mean value of 73.26 ± 4.04 g/L, ALB had a mean value of 44.83 ± 3.0 g/L, GLB had a mean value of 27.43 ± 3.64 g/L. ALT had a mean value of 20.22 ± 15.44 U/L, AST had a mean value of 24.35 ± 11.58 U/L, GGT had a mean value of 11.95 ± 5.49 U/L, LDH had a mean value of 130.87 ± 28.9 U/L, TBIL had a mean value of 14.3 ± 5.2 µmol/L, ALP had a mean value of 129.95 ± 87.81 U/L, and the AST/ALT ratio was 1.34 ± 0.37.The detection rates of the four parabens ranged from 33.40 to 98.10%. its average concentration of MP, EP, BP, and PP were 34.10 ng/ml, 0.71 ng/ml, 3.90 ng/ml, and 0.14 ng/ml respectively. Table 3 shows descriptive statistics of four parabens with two different creatinine units. The median concentrations of MP1, EP1, BP1, and PP1 were 27.32 ng/mg Cr, 0.93 ng/mg Cr, 3.04 ng/mg Cr, and 0.13 ng/mg Cr respectively. The median concentrations of MP2, EP2, BP2, and PP2 were 3.91 ng/umol Cr, 0.106 ng/umol Cr, 0.344 ng/umol Cr, and 0.0144 ng/umol Cr respectively. Subsequent analyses used MP2, EP2, BP2, and PP2 as independent variables. Spearman correlation analysis indicated significant correlations among all of them (Tables S2, S3).
Survey-weighted liner regression
Model I was not adjusted for covariates. Model II was adjusted for age and gender. Model III, which we used in this analysis, was adjusted for age, gender, race, and BMI, providing a more comprehensive control for potential confounders. This adjustment helps to reduce bias and improve the accuracy of the associations between parabens and liver function indicators. Table 4 shows that MP had negative associations with ALB (β = −0.0035, P = 0.0403) and ALP (β = −0.0302, P = 0.0015) and positive associations with TBIL (β = 0.0357, P = 0.0006). PP showed similar associations as methyl paraben. Moreover, EP had a positive association with TBIL (β = 0.0459, P = 0.0410). Furthermore, BP had positive associations with GLB (β = 0.0363, P = 0.020), GGT (β = 0.0811, P = 0.0147), and TBIL (β = 0.1112, P = 0.054) and negative associations with ALP (β = − 0.0785, P = 0.0270). The use of Model III, which accounts for a broader range of covariates, enhances the reliability of these findings. By including these covariates in Model III, we can eliminate their influence and ensure that the results are more accurate and reliable.
WQS analysis
Table 5 shows the associations between the positive and negative WQS indices of paraben and the liver function markers, after adjusting for confounders. The positive WQS index of paraben had positive associations with GLB (β = 0.0272, P = 0.0171) and TBIL (β = 0.0907, P = 0.0146). The positive WQS index of paraben had negative associations with ALB (β = − 0.0132, P = 0.0102) and ALP (β = − 0.0840, P = 0.0025). In the negative model, the WQS index of paraben was also positively associated with TBIL (β = 0.0420, P = 0.0249) and GLB (β = 0.0110, P = 0.0131), and negatively associated with ALP (β = − 0.0309, P = 0.0210) and ALB (β = − 0.0085, P = 0.0029) in adolescent.
Figure 2 shows the weights of the parabens in the WQS index. BP had the highest weight in the positive model. In the negative model, PP, EP and MP had the highest weights for different liver function outcomes.

Weight of each paraben in the WQS model. Mp methyl paraben, Ep ethyl paraben, Pp propyl paraben, Bp butyl paraben. (a–d) were the weight of each paraben in the positive WQS model. (a) ALB; (b) GLB; (c) ALP; (d) TBIL. (e–l) were the weight of each paraben in the negative WQS model. (e) ALB; (f) GLB; (g) ALP; (h) LDH; (i) TBIL; The model was adjusted by age, race and BMI. All urine paraben and function indicators variables were ln-transformed before analysis.
The association between urine parabens and liver function markers by BKMR modeling
We analyzed mixed associations of urinary parabens with markers of liver function, as shown in Fig. 3. Exposure to mixed parabens was inversely related to ALT and ALP when other parabens were detected at moderate concentrations.

The BKMR model (N = 1845) showed how each liver function indicator changed with the level of a single paraben, while keeping the levels of all other parabens at their median values. Mp methyl paraben, Ep ethyl paraben, Pp propyl paraben, Bp butyl paraben. (a) ALT, (b) AST, (c) ALP, (d) GGT, (e) LDH, (f) TBIL. The model was adjusted by age, race and BMI. All urine paraben and function indicators variables were ln-transformed before analysis.
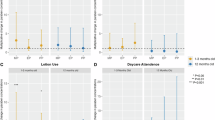
We applied the SingVarRiskSummaries function to the single-pollutant model. The primary function of SingVarRiskSummaries is to assess and summarize the risk associated with a single pollutant. Specifically, this function helps us understand the statistical characteristics and risk profile of a variable in a dataset. The results are shown in Fig. 4, Only PP was found to be negatively correlated with ALP. Other associations did not reach significance levels in Fig. 4. These findings suggest that different parabens may have distinct impacts on liver function, although further research is needed to confirm the significance of these associations.

Single-pollutant model of BKMR (N = 1845): the effect of paraben on liver function indicators. Mp methyl paraben, Ep ethyl paraben, Pp propyl paraben, Bp butyl paraben. (a) ALT, (b) AST, (c) ALP, (d) GGT, (e) LDH, (f) TBIL. The model was adjusted by age, race and BMI. All urine paraben and function indicators variables were ln-transformed before analysis.
To explore the effects of different parabens on liver function markers, we plotted the exposure-response relationship function for each paraben in Fig. 5. When the confidence interval includes 0, it typically means that there are no statistically significant results. In other words, in such cases, we cannot rule out the possibility of no relationship. Therefore, a confidence interval that includes 0 often means that the association or effect is not statistically significant. However, this does not entirely mean that the research results are meaningless. It might indicate that the sample size is insufficient or that there is a high variability in the data, leading to a lack of statistical power to detect a significant relationship. Further research and more sample data may help better understand this relationship.

The BKMR model (N = 1845) examined how liver function indicators were jointly affected by the mixture of paraben exposure. Mp methyl paraben, Ep ethyl paraben, Pp propyl paraben, Bp butyl paraben. (a) ALT, (b) AST, (c) ALP, (d) GGT, (e) LDH, (f) TBIL. The model was adjusted by age, race and BMI. All urine paraben and function indicators variables were ln-transformed before analysis.
Discussion
Parabens are used as preservatives in more than 22,000 cosmetic products at concentrations up to 0.8% in individual parabens and up to 0.4% in paraben mixtures28. Parabens are unstable compounds that are rapidly metabolized (within hours or days) and excreted from the body. In addition to estrogenic effects, some parabens also have antiandrogenic effects by binding to androgen receptors29. thereby inhibiting testosterone-induced transcription. In vivo studies have shown that parabens can affect reproduction, development and homeostasis30.
Parabens are a common class of antimicrobial preservatives, widely used in the cosmetics, pharmaceutical, and food industries due to their low cost, ease of formulation, and favorable toxicological profile. The shorter-chain types—MP, EP, PP, and BP—are the most frequently used either individually or in combination31 and have been in use for over half a century. However, their safety as preservatives has long been debated, primarily because of potential endocrine-disrupting effects. In recent years, a series of studies have suggested that parabens may exhibit estrogen-like effects, anti-androgenic properties, impacts on uterine tissues, and even influence sperm count and testosterone levels in the male reproductive system32. They can be absorbed through the skin or gastrointestinal tract and undergo extensive metabolism, including glucuronidation and sulfation reactions, leading to their excretion in conjugated forms33.
Although parabens are generally considered safe, previous studies have found that exposure to them may have potential health implications. For instance, paraben exposure has been negatively correlated with sex hormone levels28,34, a link that is particularly evident in growing children and may affect normal puberty development. Additionally, some research suggests that certain parabens may be associated with changes in reproductive and thyroid hormone levels during pregnancy, thereby influencing maternal or infant health35,36. These findings have sparked extensive discussions about whether long-term use of parabens disrupts the endocrine system. On the other hand, studies have also shown that although albumin is thought to possess esterase activity, it does not participate in paraben hydrolysis at physiological concentrations37. This may lead to the accumulation of these chemicals in the body, further exacerbating their endocrine-disrupting effects, particularly in terms of their impact on male and female reproductive systems38.
Notably, some parabens also exhibit anti-androgenic activity as they can bind to androgen receptors, thereby inhibiting testosterone-induced transcription. In vivo studies have indicated that parabens can disrupt reproduction, development, and homeostasis. In humans, they have been detected in serum, urine, umbilical cord blood, meconium, milk, amniotic fluid, and placental tissue. The correlation observed between MP and hormones affecting metabolic health and energy suggests its potential obesogenic effects. The association between methylparaben and hormones influencing energy balance and metabolic health further implies its obesogenic potential39, whereas the lack of P-gp effects with isobutylparaben may indicate insignificant interactions with P-gp drug substrates40. These discoveries provide researchers with new perspectives, encouraging further exploration of parabens’ metabolism and health effects across different populations. Overall, previous studies have summarized the structure-metabolism relationships of parabens and systematically evaluated their safety to guide future usage strategies in cosmetics, food, and pharmaceuticals41. The research into the bioaccumulation of parabens within the human body and the subsequent implications for hepatic function has garnered increasing attention. Parabens, a ubiquitous class of preservatives employed across a spectrum of consumer products, including cosmetics, pharmaceuticals, and foodstuffs, have been ubiquitously detected in various human tissues and biological fluids. This pervasive presence has engendered concerns regarding their potential adverse health effects.
Although parabens are typically characterized by rapid metabolic degradation and subsequent excretion, their structural mimicry of estrogen and affinity for androgen receptors have raised the specter of more pernicious impacts on the endocrine system. Given the liver’s pivotal role in metabolic regulation—encompassing the detoxification of xenobiotics and the metabolism of pharmacological agents—any perturbation attributable to parabens could precipitate significant pathophysiological outcomes. Thus, understanding the extent and mechanisms by which parabens influence hepatic function is imperative for assessing their safety profile.
Recent empirical investigations have suggested a potential association between exposure to parabens and hepatic function alterations, a phenomenon particularly observed in adolescent populations. These hepatic changes are frequently asymptomatic, eluding detection in the absence of systematic screening. Hepatic biomarkers, including ALT, AST, ALP, GGT, and TBIL, are quintessential in evaluating hepatic health. Deviations in these biomarker levels may be indicative of incipient hepatic impairment or presage the onset of hepatic pathology.
Furthermore, parabens’ interactions with hepatic drug-metabolizing enzymes and transport proteins, such as p-glycoprotein (p-gp), may modulate the pharmacokinetic profiles of concomitant medications, thereby heightening the risk of adverse pharmacological events. The biotransformation of parabens into hydroxybenzoate esters, followed by their conjugation to glucuronides and sulfates, constitutes a principal detoxification route. Nonetheless, the efficacy of this metabolic pathway and the risk of hepatic bioaccumulation of parabens warrant further investigation.
In the present study, the WQS analysis emerges as a sophisticated multivariate methodology that quantifies the cumulative effect of exposure, with a particular emphasis on the diverse parabens present in the environmental mixture. The WQS model innovatively employs Bootstrap techniques to allocate weights ranging from 0 to 1 to each pollutant, thereby enhancing the precision of exposure assessments. This method demonstrates a marked improvement over univariate analyses, particularly in its ability to accurately identify pivotal environmental factors. Further augmenting the analytical prowess of this research, the BKMR model is adeptly utilized to discern the complex interplay among various pollutants. It meticulously evaluates the exposure-response relationship for each constituent within the mixture, providing a nuanced understanding of their collective impact. The construction of the WQS and BKMR models is deftly executed using an array of R packages, namely nhanesA, gWQS, bkmrs, ltm, and gtsummary. These tools are employed in strict accordance with established academic protocols and regulatory guidelines, ensuring that all analyses maintain the highest standards of scientific integrity and rigor.The employment of advanced statistical models, such asWQS regression and BKMR, has shed light on the intricate interplay between various parabens and hepatic function markers. These analytical models consider both the aggregate and discrete impacts of paraben exposure on hepatic function, offering a nuanced understanding of their potential effects.
Our study has some limitations. First, since the NHANES data are cross-sectional, conclusions about causality cannot be drawn. Thus, all relationships are correlated and more prospective studies are needed to overcome this methodological limitation. However, this study provides important information on how changes in paraben levels are associated with previously unreported asymptomatic changes in liver function tests in adolescents in the United States. Second, individual urine samples from each individual were used to measure paraben exposure, presumably without accounting for changes in the body over time.
Conclusions
Paraben metabolites in US adolescents are significantly associated with liver dysfunction. Excessive use of paraben metabolites can lead to decreased levels of serum globulin, reduced total bile acids, and impaired liver function in the human body.Further investigation into the impact of parabens, which are widely used and persistent in many products, on endocrine disruption could offer valuable insights into their association with liver disease. Future work should explore these relationships in more detail.
Data availability
The data presented in this study are openly available in the NHANES database (https://www.cdc.gov/nchs/nhanes/index.htm, (accessed on 28 March 2024));The R language code for all the analytical processes is available upon request by emailing the corresponding author. If you need further assistance or have any questions, please feel free to reach out.
Abbreviations
- TP:
-
Total protein
- ALB:
-
Albumin
- GLB:
-
Globulin
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- GGT:
-
Gamma glutamyl transferase
- LDH:
-
Lactate dehydrogenase
- TBIL:
-
Total bilirubin
- ALP:
-
Alkaline phosphatase
- MP:
-
Methyl paraben
- EP:
-
Ethyl paraben
- PP:
-
Propyl paraben
- BP:
-
Butyl paraben
References
Calafat, A. M., Ye, X., Wong, L. Y., Bishop, A. M. & Needham, L. L. Urinary concentrations of four Parabens in the U.S. Population: NHANES 2005–2006. Environ. Health Perspect. 118 (5), 679–685. https://doi.org/10.1289/ehp.0901560 (2010).
Han, C., Lim, Y. H. & Hong, Y. C. Ten-year trends in urinary concentrations of triclosan and benzophenone-3 in the general U.S. Population from 2003 to 2012. Environ. Pollut. 208, 803–810. https://doi.org/10.1016/j.envpol.2015.11.002 (2016).
Irwin, S. V., Fisher, P., Graham, E., Malek, A. & Robidoux, A. Sulfites inhibit the growth of four species of beneficial gut bacteria at concentrations regarded as safe for food. PLoS ONE. 12 (10), e0186629. https://doi.org/10.1371/journal.pone.0186629 (2017).
Błędzka, D., Gromadzińska, J. & Wąsowicz, W. Parabens. From environmental studies to human health. Environ. Int. 67, 27–42. https://doi.org/10.1016/j.envint.2014.02.007 (2014).
Azzouz, A., Rascon, A. J. & Ballesteros, E. Simultaneous determination of parabens, alkylphenols, phenylphenols, bisphenol A and triclosan in human urine, blood and breast milk by continuous solid-phase extraction and gas chromatography-mass spectrometry. J. Pharm. Biomed. Anal. 119, 16–26. https://doi.org/10.1016/j.jpba.2015.11.024 (2016).
Baker, B. H. et al. Methylparaben in meconium and risk of maternal thyroid dysfunction, adverse birth outcomes, and attention-deficit hyperactivity disorder (ADHD). Environ. Int. 139, 105716. https://doi.org/10.1016/j.envint.2020.105716 (2020).
Kolatorova Sosvorova, L. et al. Determination of selected bisphenols, Parabens and estrogens in human plasma using LC-MS/MS. Talanta 174, 21–28. https://doi.org/10.1016/j.talanta.2017.05.070 (2017).
Pollack, A. Z. et al. Urinary levels of environmental phenols and Parabens and antioxidant enzyme activity in the blood of women. Environ. Res. 186, 109507. https://doi.org/10.1016/j.envres.2020.109507 (2020).
Vela-Soria, F. et al. Simplified matrix solid phase dispersion procedure for the determination of Parabens and benzophenone-ultraviolet filters in human placental tissue samples. J. Chromatogr. A. 1371, 39–47. https://doi.org/10.1016/j.chroma.2014.10.063 (2014).
Vitku, J. et al. Endocrine disruptors of the bisphenol and Paraben families and bone metabolism. Physiol. Res. 67 (Suppl 3), S455–S464. https://doi.org/10.33549/physiolres.934005 (2018).
Asrani, S. K., Devarbhavi, H., Eaton, J. & Kamath, P. S. Burden of liver diseases in the world. J. Hepatol. 70 (1), 151–171. https://doi.org/10.1016/j.jhep.2018.09.014 (2019).
Lawlor, D. A. et al. Nonalcoholic fatty liver disease, liver fibrosis, and cardiometabolic risk factors in adolescence: a cross-sectional study of 1874 general population adolescents. J. Clin. Endocrinol. Metab. 99 (3), E410. https://doi.org/10.1210/jc.2013-3612 (2014).
Xu, C. et al. Urinary biomarkers of polycyclic aromatic hydrocarbons and their associations with liver function in adolescents. Environ. Pollut. 278, 116842. https://doi.org/10.1016/j.envpol.2021.116842 (2021).
Praveena, S. M. et al. Recent updates on phthalate exposure and human health: a special focus on liver toxicity and stem cell regeneration. Environ. Sci. Pollut Res. Int. 25 (12), 11333–11342. https://doi.org/10.1007/s11356-018-1652-8 (2018).
Midya, V. et al. Association of prenatal exposure to endocrine-disrupting chemicals with liver injury in children. JAMA Netw. Open. 5 (7), e2220176. https://doi.org/10.1001/jamanetworkopen.2022.20176 (2022).
Wang, J. et al. Platelets in alcohol-associated liver disease: interaction with neutrophils. Cell. Mol. Gastroenterol. Hepatol. 18 (1), 41–52. https://doi.org/10.1016/j.jcmgh.2024.03.001 (2024).
Zipf, G. et al. National health and nutrition examination survey: plan and operations, 1999–2010. Vital Health Stat. 1 (56), 1–37 (2013).
Whitehead, M. W., Hawkes, N. D., Hainsworth, I. & Kingham, J. G. A prospective study of the causes of notably Raised aspartate aminotransferase of liver origin. Gut 45 (1), 129–133. https://doi.org/10.1136/gut.45.1.129 (1999).
Whitfield, J. B. Gamma Glutamyl transferase. Crit. Rev. Clin. Lab. Sci. 38 (4), 263–355. https://doi.org/10.1080/20014091084227 (2001).
Liang, Q., Huang, R., Peng, Z. & Zou, M. Impact of dietary selenium and blood concentration on liver function: a population-based study. Front. Nutr. 11, 1415288. https://doi.org/10.3389/fnut.2024.1415288 (2024).
Arora, A. et al. Indian National association for the study of the liver-Federation of obstetric and gynaecological societies of India position statement on management of liver diseases in pregnancy. J. Clin. Exp. Hepatol. 9 (3), 383–406. https://doi.org/10.1016/j.jceh.2019.02.007 (2019).
Vítek, L., Tiribelli, C. & Bilirubin The yellow hormone? J. Hepatol. 75 (6), 1485–1490. https://doi.org/10.1016/j.jhep.2021.06.010 (2021).
Ye, X., Kuklenyik, Z., Bishop, A. M., Needham, L. L. & Calafat, A. M. Quantification of the urinary concentrations of Parabens in humans by on-line solid phase extraction-high performance liquid chromatography-isotope Dilution tandem mass spectrometry. J. Chromatogr. B Analyt Technol. Biomed. Life Sci. 844 (1), 53–59. https://doi.org/10.1016/j.jchromb.2006.06.037 (2006).
O’Brien, K. M., Upson, K., Cook, N. R. & Weinberg, C. R. Environmental chemicals in urine and blood: improving methods for creatinine and lipid adjustment. Environ. Health Perspect. 124 (2), 220–227. https://doi.org/10.1289/ehp.1509693 (2016).
Tanner, E. M., Bornehag, C. G. & Gennings, C. Repeated holdout validation for weighted quantile sum regression. MethodsX 6, 2855–2860. https://doi.org/10.1016/j.mex.2019.11.008 (2019).
Gennings, C., Sabo, R. & Carney, E. Identifying subsets of complex mixtures most associated with complex diseases: polychlorinated biphenyls and endometriosis as a case study. Epidemiology 21 (Suppl 4), S77–S84. https://doi.org/10.1097/EDE.0b013e3181ce946c (2010).
Bobb, J. F., Claus Henn, B., Valeri, L. & Coull, B. A. Statistical software for analyzing the health effects of multiple concurrent exposures via bayesian kernel machine regression. Environ. Health. 17 (1), 67. https://doi.org/10.1186/s12940-018-0413-y (2018).
Honda, M., Robinson, M. & Kannan, K. Parabens in human urine from several Asian countries, greece, and the united States. Chemosphere 201, 13–19. https://doi.org/10.1016/j.chemosphere.2018.02.165 (2018).
Deierlein, A. L., Rock, S. & Park, S. Persistent endocrine-disrupting chemicals and fatty liver disease. Curr. Environ. Health Rep. 4 (4), 439–449. https://doi.org/10.1007/s40572-017-0166-8 (2017).
Bledzka, D., Gromadzinska, J. & Wasowicz, W. Parabens. From environmental studies to human health. Environ. Int. 67, 27–42. https://doi.org/10.1016/j.envint.2014.02.007 (2014).
Fransway, A. F. et al. Parabens. Dermatitis 30 (1):3–31. https://doi.org/10.1097/DER.0000000000000429 (2019).
Moos, R. K., Angerer, J., Dierkes, G., Bruning, T. & Koch, H. M. Metabolism and elimination of methyl, iso- and n-butyl Paraben in human urine after single oral dosage. Arch. Toxicol. 90 (11), 2699–2709. https://doi.org/10.1007/s00204-015-1636-0 (2016).
Soni, M. G., Carabin, I. G. & Burdock, G. A. Safety assessment of esters of p-hydroxybenzoic acid (parabens). Food Chem. Toxicol. 43 (7), 985–1015. https://doi.org/10.1016/j.fct.2005.01.020 (2005).
Adoamnei, E. et al. Urinary concentrations of Parabens and reproductive parameters in young men. Sci. Total Environ. 621, 201–209. https://doi.org/10.1016/j.scitotenv.2017.11.256 (2018).
Aker, A. M. et al. Phenols and Parabens in relation to reproductive and thyroid hormones in pregnant women. Environ. Res. 151, 30–37. https://doi.org/10.1016/j.envres.2016.07.002 (2016).
Aker, A. M. et al. A repeated measures study of phenol, Paraben and triclocarban urinary biomarkers and Circulating maternal hormones during gestation in the Puerto Rico PROTECT cohort. Environ. Health. 18 (1), 28. https://doi.org/10.1186/s12940-019-0459-5 (2019).
Abbas, S. et al. Metabolism of Parabens (4-hydroxybenzoic acid esters) by hepatic esterases and UDP-glucuronosyltransferases in man. Drug Metab. Pharmacokinet. 25 (6), 568–577. https://doi.org/10.2133/dmpk.dmpk-10-rg-013 (2010).
Barr, L., Metaxas, G., Harbach, C. A., Savoy, L. A. & Darbre, P. D. Measurement of Paraben concentrations in human breast tissue at serial locations across the breast from axilla to sternum. J. Appl. Toxicol. 32 (3), 219–232. https://doi.org/10.1002/jat.1786 (2012).
Simkova, M. et al. Endocrine disruptors, obesity, and cytokines—how relevant are they to PCOS? Physiol. Res. 69 (Suppl 2), S279–S293. https://doi.org/10.33549/physiolres.934521 (2020).
Alshogran, O. Y., Ghraiybah, N. F. A. & S IA-A Evaluation of the effect of isobutyl Paraben and 2-ethyl hexyl Paraben on P-glycoprotein functional expression in rats: a Pharmacokinetic study. Curr. Mol. Pharmacol. 15 (7), 987–995. https://doi.org/10.2174/1874467215666220127121817 (2022).
Obringer, C., Wu, S., Troutman, J., Karb, M. & Lester, C. Effect of chain length and branching on the in vitro metabolism of a series of Parabens in human liver S9, human skin S9, and human plasma. Regul. Toxicol. Pharmacol. 122, 104918. https://doi.org/10.1016/j.yrtph.2021.104918 (2021).
Author information
Authors and Affiliations
Contributions
Authors Statement: Conceptualization, L.L. and J.H.; software, L.L.; resources, G.H. and Z.W.; data curation, X.L.; writing—original draft preparation, G.H.; writing—review and editing, L.L.-J.H.,and G.H; visuali-zation, L.L; supervision, J.H.; All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, L., Hu, G., Luo, X. et al. Association of urine parabens with liver function in US adolescents based on NHANES 2007–2016. Sci Rep 15, 21198 (2025). https://doi.org/10.1038/s41598-025-08435-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-08435-y
