
Abstract
The hormonal changes in menopause predispose women to health risks, including type 2 diabetes. Therefore, diabetes prevention in this age group is important. Considering the fewer side effects of herbal medicines compared to chemical drugs, the present study investigated the impact of barley savigh consumption on blood sugar levels in pre-diabetic postmenopausal women. This randomized clinical trial study was conducted on 64 pre-diabetic postmenopausal women referred to Community Health Centers in Gonabad city, Iran. The intervention group (n = 32) received 60 g of barley savigh daily (20 g before each meal), and the control group (n = 32) received no intervention. Fasting blood sugar (FBS) and blood sugar two hours post-prandial were checked in both groups at baseline and after two and four weeks. Data analysis was done using SPSS software (version 16) and chi-square, independent t-test, and Mann-Whitney tests at the significance level of p < 0.05. There was no significant difference in the mean FBS at baseline (109.31 ± 5.06 in the intervention and 109.03 ± 8.49 mg/dL in the control group, p = 0.904) and after two weeks after intervention (105.25 ± 5.92 in the intervention and 108.06 ± 8.75 mg/dL in the control group, p = 0.13), but the mean FBS after four weeks was significantly lower in the intervention (102.93 ± 7.75 mg/dL) compared to the control (107.90 ± 8.29 mg/dL) group (p = 0.019). The mean blood sugar two hours post-prandial was significantly lower in the intervention group compared to the control group after two (127.53 ± 8.03 and 143.68 ± 26.46 mg/dL, respectively, p = 0.006) and four weeks (127.09 ± 17.96 and 142.46 ± 27.06 mg/dL, respectively, p = 0.009). The results of the present study showed that barley savigh consumption could improve blood sugar regulation in pre-diabetic postmenopausal women.
Trial registration: The present study was conducted as a randomized clinical trial. The study protocol was approved by the Iranian Registry of Clinical Trials (IRCT code 20200929048880N1). Registration date (25/10/2020).
Similar content being viewed by others

Introduction
Menopause is a physiological event in the life of women1. Menopause is diagnosed when a woman does not have menstruation for 12 months due to the loss of ovarian follicular activity2. During the transition from childbearing phase to menopause, the level of 17-beta-estradiol, which is a reproductive estrogen, drops from 100 to 250 pg/ml to less than 10 pg/ml3. It has been shown that estrogen reduces insulin resistance, decreases insulin levels, and decreases insulin sensitivity to glucose. Therefore, the decrease in the ratio of estrogen to androgen around menopause can result in central accumulation of fat, abdominal obesity, insulin resistance, hyperinsulinemia, and type 2 diabetes, as well as predisposition to some cancers4,5,6.
Diabetes is a group of metabolic diseases characterized by high blood sugar (hyperglycemia) due to either a defect in insulin secretion or insulin action7. Chronic hyperglycemia may damage various organs, especially the eyes, kidneys, nervous system, and cardiac blood vessels, causing loss of vision, kidney failure, leg ulcers that may result in amputation, sexual dysfunction, high blood pressure, and dyslipidemia7. Some of these complications could be delayed or prevented by proper interventions5. Diabetes is divided into several types. In type 1 diabetes, beta-pancreatic cells, which secrete insulin, are destroyed by an autoimmune reaction. This type of diabetes has an acute onset, usually before the age of 30, and requires insulin injection to control blood glucose levels. Type 2 diabetes is characterized by resistance to insulin and reduced insulin. Type 2 diabetes can be managed through exercise, diet control, and oral anti-diabetic medications8. The American Diabetes Association proposed a pre-diabetes state as elevated blood sugar from the normal range but below the diagnostic cut-off for diabetes. The risk of type 2 diabetes and vascular diseases is higher among pre-diabetic individuals compared to the healthy population9. Adhering to a healthy diet and increasing physical activity play a significant role in controlling this disease and preventing more advanced stages of diabetes in individuals at pre-diabetic stage10. Pre-diabetes is impaired glucose tolerance, fasting glucose, or mildly increased hemoglobin A1C level below the cut-off for diabetes11. The prevalence of pre-diabetes among menopausal women was reported to range between 7 and 26% worldwide and between 19 and 26% in Iran based on age group and province12,13,14,15,16. Annually, 10% of individuals with pre-diabetes develop diabetes11.
Herbal medicines are widely prescribed worldwide due to their low side effects, low cost, availability, and effectiveness. Various plants have been traditionally used to reduce blood sugar and treat diabetes17. Barley is among the medicinal plants that have blood sugar-reducing effects18. The role of barley seeds in treating diabetes is also mentioned in the ancient texts of traditional Iranian medicine19. Barley and oat seeds contain alkaloids, beta-carotene, steroid compounds, saturated fatty acids, starch, beta-glucan fiber, B1, B2, A, C, D, and E vitamins. They are the richest plant sources of zinc. Due to the effects of these compounds, barley has been used as a laxative, diuretic, pain reliever, and heart and blood tonic, as well as reducing blood cholesterol and blood pressure and maintaining the balance between blood sugar and blood insulin20. Therefore, regular consumption of barley is said to reduce the risk of chronic diseases, including diabetes, cancer, obesity, and cardiovascular diseases21.
The blood sugar-lowering effects of barley are due to its low glycemic index, high chromium and magnesium content, and water-soluble fibers, including beta-glucan22. Beta-glucan binds to the ingested sugars and lipids and indirectly changes the intestinal environment, thus affecting blood sugar levels (19). So far, many studies have reported barley’s blood sugar reduction effects18,23,24,25. The beneficial metabolic effects of oats in terms of appetite suppression and insulin sensitivity improvement have been attributed to its beta-glucan26. Although there is evidence of the acute effects of barley products on post-prandial glucose, to the best of our knowledge, the short and long term effects of different compartments of barley on blood sugar has not been studied27,28. Therefore, the present study investigated the impact of consuming barley savigh on the blood sugar levels of pre-diabetic postmenopausal women.
Methods
Trial design
The present study was conducted as a randomized clinical trial. The study protocol was approved by the Iranian Registry of Clinical Trials (IRCT code: 20200929048880N1). Registration date: (25/10/2020). The study was approved by the Ethics Committee of the Gonabad University of Medical Sciences (Code: IR.GMU.REC.1399.070). The study protocol was published earlier21.
This clinical trial was reported based on the CONSORT Statement 2010 checklist29. All methods were performed following the relevant guidelines and regulations.
Participants and setting
The study was conducted on 68 postmenopausal women referring to Community Health Centers in Gonabad city, Iran. Inclusion criteria were menopause (complete cessation of menstruation for at least 12 months), age between 45 and 65 years, pre-diabetic (FBS = 125 mg/dl or two-hour post-prandial plasma glucose level between 140 and 199 mg/dl), not consuming herbal supplements to control blood glucose, literacy, having cardiovascular or other systemic diseases, hypertension, history of smoking, alcohol and drug use, history of grain allergy or celiac disease, and being normal or overweight (Body Mass Index [BMI] between 19 and 28 kg/m2). The exclusion criteria were documented diagnosis of diabetes during the study period, taking anti-diabetic medications or consuming herbal supplements to control blood glucose, need for insulin therapy or anti-diabetic medicines during the study period, occurrence of stressful events, irregular consumption of barley or experiencing complications, including dermatitis, bloating, and diarrhea, hospitalization during the intervention, failure to complete the study questionnaires, occurrence of hypoglycemia based on self-monitoring blood glucose or signs and symptoms of hypoglycemia, and refusing to participate in the study. The complete list of inclusion and exclusion criteria has been published elsewhere21.
Sample size and randomization
The sample size for this clinical trial was calculated based on the findings of a previous study, where barley beta-glucan reduced mean FBS from 175.7 ± 29.1 to 140.5 ± 60.9 mg/dl23.
Based on the following equation and considering type I and II errors of 5% and 20%, respectively, the sample size was determined as 31 participants in each group, which was increased to 34 participants in each group (total sample size of 68 participants) considering 10% dropout.
Study instruments
-
a.
Demographic characteristics questionnaire: This questionnaire included age, BMI, systolic and diastolic blood pressure, duration of pre-diabetes, duration of menopause, parity, gravida, number of abortions, stillbirth, and live children. The questionnaire was filled out based on interviews or from their medical records.
-
b.
Three-Day Food Record: Since the daily diet is an essential factor in blood sugar levels, it was controlled as a confounding factor in this study. For this purpose, all participants were asked to record their food intake during three-week days. A three-day food record was obtained at baseline, during the first two weeks of the intervention, and during the second two weeks. The validity of the three-day food record has been confirmed by the content validity method, and the reliability was approved using an r coefficient of > 0.999 in a previous study24.
-
c.
Beck Physical Activity Questionnaire: Since physical activity is an essential factor in blood sugar levels, it was controlled as a confounding factor in this study. For this purpose, the Beck Physical Activity Questionnaire was used. This questionnaire is an international and standard tool for assessing the level of physical activity30. This questionnaire includes 16 questions that are scored using a four-point Likert scale. Beck’s physical activity questionnaire consists of three sections: work-related, sports, and leisure-time physical activity. Based on the intensity of physical activity, each question is scored from one, indicating the lowest level of physical activity, to five, indicating the highest level. The level of physical activity for each participant is obtained by summing up the score of each question. The validity and reliability of this questionnaire have been checked and confirmed in different countries, different groups, and Iran. In Iran, the validity and reliability of the Beck’s physical activity questionnaire was approved27,31.
-
d.
Barley Savigh consumption and complication checklist: Participants in the intervention group were asked to complete the checklist daily. The checklist included recording daily consumption of barely savigh and questions on the experience of bloating or increased frequency of defecation.
Intervention
The researcher referred to the community health centers of Gonabad city to identify the women based on the inclusion criteria. Eligible women were approached, and the study’s aim and procedure were described. In case of agreement, informed and written consent was obtained from the women included in the study. To diagnose pre-diabetes, 5 ml of venous blood was obtained after overnight fasting (8–10 h) to measure FBS, and 5 ml was obtained two hours after eating a standard breakfast to measure 2-hour post-prandial blood glucose. All tests were performed in one laboratory to avoid laboratory errors.
The eligible participants were randomly assigned to the intervention and control groups using four permutation blocks. At the beginning of the study, all participants completed the demographic questionnaire, and FBS and 2-hour post-prandial blood sugar were recorded. Participants also completed a three-day food record and Beck’s physical activity questionnaire.
The participants in the intervention group were asked to consume 60 g of barley savigh (20 g of savigh five minutes before each main meal/three times daily), preferably in dry form, for four weeks. This dose was determined based on previous studies that indicated that at least 4 g of beta-glucan and 30–80 g of available carbohydrates from barley could reduce blood sugar20.
For the preparation of barley savigh, barley was bought from a local farmer in the region, and a sample from the barley was sent to the Gonabad Agricultural and Natural Resources Research and Training Center for identification. The identified sample was approved by the Gonabad Agricultural and Natural Resources Research and Training Center (Herbarium Code: Hordeum vulgare L. Family: poaceae. voucher sp.no.E-1401 FUMH). Then, the mill and bran were separated and ground. The mill flour was roasted. Bran was roasted and then ground and mixed with roasted barley flour.
Participants were asked to complete the barley savigh consumption and complications checklist daily to ensure regular consumption of barely savigh. As mentioned in the exclusion criteria, participants with irregular consumption of barley or experiencing complications were excluded from the study. The control group received no intervention.
The four-week study was chosen due to the findings of previous studies that indicated short-term changes in FBS and post-prandial glucose, which can be seen within four weeks in nutrition intervention studies that may reduce dropout from the study32,33,34.
All participants in the intervention and control groups were given the same training about healthy diet, foods that increase blood sugar that should be avoided, and information on the number of appropriate meals and snacks to control the effect of confounding factors. Participants were asked not to change their physical activities during the study.
In both groups, FBS and 2-hour post-prandial blood glaucus were evaluated at the end of the second and the fourth weeks after the start of the intervention. Evaluating the FBs and 2-hour post-prandial blood glaucus in the second week was made better to determine the trend in changes in the variables. They also simultaneously filled out the Beck Physical Activity Questionnaire and Three-Day Food Record.
Statistical analysis
After collecting the data, statistical analysis was done using the Statistical Package for Social Sciences (SPSS) version 16 software. The normality of the continuous variables was evaluated using the Kolmogorov-Smirnov test. The independent t-test (for normally distributed variables) or Mann-Whitney (for non-normally distributed variables) was used to compare continuous variables between groups. The chi-square test was used to compare the distribution pattern of the categorical variables between groups. The statistical significance level was considered as p < 0.05.
Results
Study dropouts
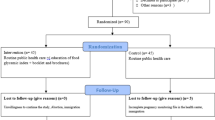
Out of 68 participants, two participants from the intervention group were excluded from the study due to lack of regular consumption of the barley savigh (n = 1) and hospitalization (n = 1), and two participants from the control group were excluded due to not completing the questionnaires (n = 1) and refusal to continue the study (n = 1). Therefore, 64 participants remained in the study (32 participants in each group) (Fig. 1).

The flow diagram of the study.
Demographic characteristics
In both groups, 15 (46.9%) participants were rural, and 17 (53.1%) were urban residents, which was not statistically different based on the chi-square test (p = 0.617). The mean age of the participants in the intervention and control groups was 56.86 ± 5.86 and 56 ± 6.02 years, respectively. There was no significant difference in age between the two groups (p = 0.615). Demographic characteristics of the participants are shown in Table 1. There was no significant difference between groups regarding demographic characteristics (p > 0.05).
A comparison of physical activity and nutrition intake between the intervention and control groups at study time points is shown in Table 2. There was only a significant difference in fat intake between groups at week four (p = 0.013). This finding indicated that fat intake was significantly higher in the intervention group compared to the control group at week four.
Effects of barley savigh on FBS
Comparison of the values of FBS between the intervention and control groups at study time points are shown in Table 3; Fig. 2a. There was a significant difference between groups regarding FBS at week four (p = 0.019). This finding indicated that FBS was significantly lower in the intervention group compared to the control group. Within the group, the comparison revealed a significant difference in FBS between study time points (p < 0.001) only among the participants in the intervention group. This finding indicated that FBS significantly decreased over time in the intervention group. Furthermore, the trend in the change in FBS was different between the groups, indicating a time-dependent reduction in FBS in the intervention group (Fig. 2a).

Changes in FBS (a) and 2-hour post-prandial blood sugar (b) levels in the intervention and control groups after adjusting for fat intake.
Effects of barley savigh on 2-hour post-prandial blood sugar
Comparison of 2-hour post-prandial blood sugar between the intervention and control groups at study time points are shown in Table 4; Fig. 2b. There was a significant difference between groups regarding 2-hour post-prandial blood sugar at week two (p = 0.006) and four (p = 0.009). These findings indicated that 2-hour post-prandial blood sugar levels were significantly lower in the intervention group compared to the control group. The within-group comparison revealed a significant difference in 2-hour post-prandial blood sugar levels between study time points (p < 0.001) only among the participants in the intervention group. This finding indicated that 2-hour post-prandial blood sugar levels significantly decreased over time in the intervention group (Table 4). Furthermore, the trend in the change in 2-hour post-prandial blood sugar was different between the groups, indicating a time-dependent reduction in 2-hour post-prandial blood sugar in the intervention group (Fig. 2b).
Discussion
Barley is a good source of fiber. The beta-glucan soluble fiber in barley can reduce the absorption of sugar in the digestive system24. Therefore, this study used barley savigh as a potential blood sugar-reducing agent that can help reduce post-prandial blood sugar.
Effects of barley savigh on FBS
In the present study, FBS was significantly lower in the intervention group compared to the control group four weeks after the intervention. Furthermore, there was a significant decrease in FBS in the intervention group over time. The FBS levels slightly decreased in the control group. Still, this decrease was neither statistical nor clinically important and could be due to the effects of their education on a healthy diet. This observation might be due to the soluble fiber (beta-glucan) content of barley savigh. Although beta-glucan can have acute effects on gastric emptying and glucose absorption, its effect on gut microbiota can be the reason for its persistent effects35,36. This hypothesis can be justified by the observed significant reduction in FBS at the final assessment, where it can be hypothesized that the microbiota had reached the adequate quantity to affect FBS. To the best of our knowledge, no human studies evaluated the effects of barley savigh on FBS in postmenopausal women. Previous studies’ findings regarding the effect of barley products on FBS were controversial. An earlier study reported that daily consumption of barley bread containing 4 g beta-glucan with or without aerobic exercise for 12 weeks reduced FBS and blood pressure and improved body composition in type 2 diabetic women23. An animal study observed a significant decrease in fasting serum glucose four weeks after barley consumption in diabetic rats22.
In contrast, an animal study showed that none of the tested barley seed hydroalcoholic extract doses (0.1, 0.25, 0.5 g/kg) effectively reduced FBS among healthy and diabetic rats in the acute phase of treatment (first day). Nevertheless, barley hydroalcoholic extract at doses of 0.25 and 0.5 g/kg reduced FBS in diabetic rats only after 11 days of continued daily consumption27. The reason for the difference in the findings of previous studies might be related to the study subjects (animals and humans) and different dosages and forms of barley product administration (barley bread vs. barley seed hydroalcoholic extract). However, considering the effects of barley priducts on FBS in the mentioned studies, it can be implied that the process of formulation, duration, and dosage of the barley extracts are the key factors that determin its effects on blood sugar and that the dose used in the present study could reduce FBS efficiently without important complications.
Effects of barley savigh on post-prandial blood sugar
In the present study, 2-hour post-prandial blood sugar two and four weeks after the intervention was significantly lower in the intervention group compared to the control group. Furthermore, there was a significant decrease in post-prandial blood sugar in the intervention group over time. Similar to FBS, the observed non-significant decrease in post-prandial blood sugar in the control group could be due to the effects of the education they received in a healthy diet. Similar to the findings of the present study, a systematic review that examined the impact of barley products consumption on post-prandial blood sugar reported that whole grains and a variety of barley foods that contain at least 4 g of beta-glucan and 30 to 80 g of carbohydrates, can reduce post-prandial blood18which was in line with the present study that used 60 g of barley savigh containing 40 g of carbohydrates. In a cross-over randomized controlled trial study on 67 healthy normoglycemic adults, the acute effects of administration of barley dietart fiber was evaluated. The study revealed that barley dietary fiber reduced post-prandial glycemia and improved satiety in the intervention group28. In another survey of 20 men, beta-glucan derived from barley better controlled post-prandial rise in blood glucose level compared to resistant starch35. Beta-glucan is a soluble fiber that delays gastric emptying by increasing the smack intestine viscosity37. It is also believed that it can reduce glucose absorption in the intestine38. A study on 17 obese women at risk of developing insulin resistance showed that consuming breakfast cereals containing 10 g of beta-glucan in oats significantly reduced post-prandial blood sugar levels in these people30. The results of a study on the effects of barley consumption on post-prandial blood sugar in Duke’s type diabetic patients who did not receive anti-diabetic medications showed that rice mixed with barley reduced post-prandial glucose concentration31. These researchers stated that using diets containing barley as a therapeutic diet may be useful in improving blood sugar control in diabetic patients31.
Strengths and weaknesses
One of the strengths of this study was the form of barley product that was used, which included all parts of barley seeds. One of the limitations of this study was the individual differences in terms of unknown and unpredictable neurological factors that affect blood sugar, which could not be comprehensively controlled. Also, it is suggested that the positive effects of barley savigh on glycemic control and lipid profile be evaluated over a longer period. Although insulin measurement could provide more accurate data on the impact of barely savigh on blood glucose, we could not measure insulin levels due to limited financial resources and laboratory facilities. It is suggested that insulin levels be examined in future studies.
Conclusion
Barley savigh can be important in regulating blood sugar in pre-diabetic postmenopausal women. Considering the importance of fiber consumption and its beneficial effects in preventing and controlling diabetes and other metabolic diseases, conducting more research can be helpful in this field.
Data availability
The datasets generated and analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.
References
Farokhi, F., Narenji, F., Salehi, B., Mehrabi, F. & Rafiei, M. Effect of skill life training in quality of life in menopausal women. Avicenna J. Nurs. Midwifery Care. 23, 54–64 (2015).
Azadi, T., Arghavani, H., Karezani, P. & Sayehmiri, K. Estimation of mean age of menopause in iran: a systematic review and meta-analysis. J. Ilam Univ. Med. Sci. 26, 85–93 (2018).
Sayahi, M., Zakerkish, M., Haghighizadeh, M. H. & Ziagham, S. Relationship between menopausal symptoms, age, body mass index and metabolic syndrome in postmenopausal women in a number of health centers in Ahvaz in2013. J. Arak Univ. Med. Sci. 17, 50–57 (2015).
Mehdizadeh, R. The effect of core stability training on body composition and lipoprotein in menopausal older women. Iran. J. Ageing. 10, 156–163 (2015).
Shabani, R. The effect of concurrent Aerobic–Resistance exercise training on Estrogen level and glucose homeostasis of menopausal females with blood glucose impairment. Iran. J. Rehabilitation Res. 3, 1–10 (2017).
Ziaei, S., Ziagham, S. & Sayahi, M. Relationship between menopausal age and metabolic syndrome in non-obese postmenopausal women. J. Arak Univ. Med. Sci. 16, 41–48 (2013).
Association, A. D. Diagnosis and classification of diabetes mellitus. Diabetes Care. 28, S37 (2005).
Sarshar, N. & Chamanzari, H. The Survey Of Complications In Thepatients Of Gonabad Diabete Clinic. (2003).
Bakhtiari, M. R. A review on the latest criteriA for laboratory diagnosis of diabetes mellitus, pre-diabetes and gestational diabetes. Lab. Diagnosis. 6, 4–8 (2014).
Yazdani, A., Mansourian, M., Faghihimani, E., Zareh, M. & Amini, M. The effects of macronutrient intake on the risk of pre-diabetes in first-degree relatives of patients with type 2 diabetes. J. Isfahan Med. School. 32, 1475–1486 (2014).
Echouffo-Tcheugui, J. B., Perreault, L., Ji, L. & Dagogo-Jack, S. Diagnosis and management of Pre-diabetes: A review. Jama 329, 1206–1216. https://doi.org/10.1001/jama.2023.4063 (2023).
Kabat, G. C. et al. A Longitudinal Study of the Metabolic Syndrome and Risk of Postmenopausal Breast Cancer. Cancer Epidemiology, Biomarkers & Prevention 18, 2046–2053, (2009). https://doi.org/10.1158/1055-9965.EPI-09-0235 Cancer Epidemiology, Biomarkers & Prevention.
Joshu, C. E. et al. Glycated hemoglobin and cancer incidence and mortality in the atherosclerosis in communities (ARIC) study, 1990–2006. 131, 1667–1677, (2012). https://doi.org/10.1002/ijc.27394
Shih, Y. H., Yang, C. Y., Wang, S. J. & Lung, C. C. Menopausal hormone therapy decreases the likelihood of diabetes development in peri–menopausal individuals with pre-diabetes. Diabetes Metab. 50, 101546. https://doi.org/10.1016/j.diabet.2024.101546 (2024).
Ghaemmaghami, Z. et al. Pre-diabetes, diabetes mellitus and related Cardio-metabolic risk factors in the Southern coastal region of Iran Middle-aged and elderly population; Bandare-Kong cohort study. Arch. Iran. Med. 25, 409–416 (2022).
Oraii, A. et al. Prevalence, awareness, treatment, and control of type 2 diabetes mellitus among the adult residents of tehran: Tehran cohort study. BMC Endocr. Disord. 22, 248 (2022).
Bathaie, S., Mokarizade, N. & Shirali, S. An overview of the mechanisms of plant ingredients in the treatment of diabetes mellitus. J. Med. Plants. 11, 1–24 (2012).
Tosh, S. Review of human studies investigating the post-prandial blood-glucose Lowering ability of oat and barley food products. Eur. J. Clin. Nutr. 67, 310–317 (2013).
Arbabi, F., Zangi, M. & Sadooghi, M. The effect of hordeum vulgare L. on the development of lung tissues in the embryo of diabetic albino rats. J. Comp. Pathobiology. 11, 1429–1436 (2015).
Nazari, H. et al. The effect of Avena sativa alcoholic and aqueous extract on the wound healing and skin inflammation. Stud. Med. Sci. 22, 467–473 (2011).
Zeng, Y. et al. Preventive and therapeutic role of functional ingredients of barley grass for chronic diseases in human beings. Oxidative medicine and cellular longevity (2018). (2018).
Kamrani Moghadam, L., Sadooghi, M. & Minaei Rangi, B. The effects of barley grain (Hordeum vulgare L.) during pregnancy on development and heart histopathological changes of embryos of diabetic rats. Razi J. Med. Sci. 22, 80–88 (2015).
Mokhtari, F., Esfarjani, F. & Kargar Fard, M. The effect of combined aerobic exercise and barley β-glucan on lipid profile and glucose blood of women with diabet type two. Iran. J. Diabetes Metabolism. 13, 340–351 (2014).
Najjar safari, Faraji, H. & Rashidkhani, B. m. The effect of real oat bread or regular barley bread distributed in Tehran on serum glucose and lipids in patients with dyslipidemia and type 2 diabetes. Iranian Journal of Endocrinology and Metabolism 13, 233–242 (2011).
Montazerifar, F., Ali Keikhaie, M. A., Dashipoor, A. R., Amian, M. & Nekuie, E. The effect of consumed breads on glycemic response of patients with type 2 diabetes. yafte 18 (2016).
Miyamoto, J. et al. Barley β-glucan improves metabolic condition via short-chain fatty acids produced by gut microbial fermentation in high fat diet fed mice. PLoS One. 13, e0196579 (2018).
Minaiyan, M., Ghannadi, A., Movahedian, A. & Hakim-Elahi, I. Effect of Hordeum vulgare L.(Barley) on blood glucose levels of normal and STZ-induced diabetic rats. Res. Pharm. Sci. 9, 173 (2014).
Kim, I. S., Park, S., Park, M. J., Kim, K. J. & Kim, J. Y. Effect of barley on Post-prandial blood glucose response and appetite in healthy individuals: A randomized, Double-Blind. Placebo-Controlled Trial. 16, 3899 (2024).
Paola, F., Walker, R. & Nixon, L. Medical Ethics and Humanities (Jones & Bartlett Learning, 2010).
Lewis, S. J. et al. Effect of Pravastatin on cardiovascular events in women after myocardial infarction: the cholesterol and recurrent events (CARE) trial. J. Am. Coll. Cardiol. 32, 140–146 (1998).
Osonoi, T. et al. Effects of barley intake on glycemic control in Japanese patients with type 2 diabetes mellitus undergoing anti-diabetic therapy: a prospective study. Diabetol. Int. 13, 1–9 (2021).
Kwak, J. H. et al. Dietary treatment with rice containing resistant starch improves markers of endothelial function with reduction of post-prandial blood glucose and oxidative stress in patients with pre-diabetes or newly diagnosed type 2 diabetes. Atherosclerosis 224, 457–464. https://doi.org/10.1016/j.atherosclerosis.2012.08.003 (2012).
Bahri, N. et al. Menopause research studies through passage of time: Shifting from biomedical to holistic approaches. IJOGI 18, 19–34 (2015).
Handjieva-Darlenska, T. et al. Clinical correlates of weight loss and attrition during a 10-week dietary intervention study: results from the NUGENOB project. Obes. Facts 5, 928–936 (2012).
Behall, K. M., Scholfield, D. J. & Hallfrisch, J. G. Barley β-glucan reduces plasma glucose and insulin responses compared with resistant starch in men. Nutr. Res. 26, 644–650. https://doi.org/10.1016/j.nutres.2006.10.001 (2006).
Telle-Hansen, V. H. et al. A three-day intervention with granola containing cereal beta-glucan improves glycemic response and changes the gut microbiota in healthy individuals: A cross-over study. Front. Nutr. 9, 796362 (2022).
Giuntini, E. B., Sardá, F. A. H. & de Menezes, E. W. J. F. The effects of soluble dietary fibers on glycemic response: an overview and futures perspectives. Foods 11, 3934 (2022).
Liu, Y. et al. Characterization of glucans from diverse sources and their influence on fat and carbohydrate absorption, digestion in vitro, and glucose tolerance in vivo. Int. J. Biol. Macromol. 308, 142025 (2025).
Acknowledgements
The authors express their gratitude to the Gonabad University of Medical Sciences for approving the project and the Community Health Centers of Gonabad city for their cooperation in identifying the participants, and also to all the participants who helped us in the implementation of this research with their active participation.
Funding
The study was funded by the Gonabad University of Medical Sciences (Code: 396).
Author information
Authors and Affiliations
Contributions
Study concept and design: N. B., and K. K.; analysis and interpretation of data: F. HT., and S. TZ.; drafting of the manuscript: N. K. and S.D.; critical revision of the manuscript for important intellectual content: S. D. and N. B.; statistical analysis: N. K. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Gonabad University of Medical Sciences (Code: IR.GMU.REC.1399.070). All methods were performed following the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kamali, K., Hadizadeh Talasaz, F., Tabatabaei Zadeh, S.A. et al. The effect of barley savigh consumption on blood sugar among pre-diabetic postmenopausal women. Sci Rep 15, 23072 (2025). https://doi.org/10.1038/s41598-025-08576-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-08576-0
