
Abstract
Although the bimodal diurnal pattern of intracerebral hemorrhage (ICH) onset has been well established, the exact timing of these peaks remains inconsistent across previous studies. Sunrise and sunset times serve as critical zeitgebers closely tied to diurnal rhythms, but whether their geographical and seasonal variations can explain the observed differences in peak timing remains unknown. This study aimed to investigate potential correlations between sunrise/sunset times and morning/afternoon onset peaks of ICH. In this retrospective cross-sectional study, we categorized data by hemorrhage location and seasonal onset. Primary analysis examined monthly variations in morning/afternoon peaks relative to corresponding sunrise/sunset time fluctuations, with partial correlation analysis controlling for confounders to refine associations. The study included 11,946 patients with first-ever primary ICH. These findings revealed that morning peaks commenced before sunrise, peaked at sunrise, while afternoon peaks peaked before sunset and concluded at sunset. Significant correlations were observed exclusively in the Deep ICH group, with morning peak times showing association with sunrise (partial r = 0.85, p = 0.002) and afternoon peak times with sunset (partial r = 0.69, p = 0.025). No other correlations reached significance. Our study found that sunrise/sunset times showed significant correlations with morning/afternoon onset peaks of ICH exclusively in Deep ICH cases. When addressing peak onset periods in Deep ICH, regional and seasonal variations in daylight hours should be considered.
Similar content being viewed by others

Introduction
Over the past few decades, numerous studies have been conducted on the diurnal rhythms of primary intracerebral hemorrhage (ICH) onset. These findings are encouraging in that the majority of studies have confirmed the existence of a peak time period for the ICH onset, with the peak period almost always occurring during the daytime1,2,3. However, the timing of peak occurrence varies considerably across studies. The beginning times of the morning peak were reported to be at 06:00 in some studies, and at 8:00 or 10:00 in others, with the reason for this discrepancy remaining unclear4,5,6,7,8.
Previous studies have shown that diurnal rhythms in ICH onset may be affected by a variety of endogenous and exogenous factors. These include diurnal rhythms in vascular tone, coagulation homeostasis, and blood pressure. Additionally, the temporal patterns in postural, physical activity, emotional stress, and medication effects have been supposed to affect these rhythms potentially9,10,11,12,13. Some studies have suggested that sunlight is a potential factor in the development of cardiovascular and cerebrovascular diseases14,15. Previous studies have found a correlation between the duration of sunlight exposure and the level of ultraviolet radiation and the ICH onset16. A large epidemiological study showed that the incidence of ICH was significantly higher in winter and spring than in summer and autumn, which may be related to seasonal changes in sunlight17. In addition, some animal experiments have confirmed that moderate sunlight exposure can regulate the physiological indexes of the body, such as blood pressure and coagulation function, and thus affect the risk of ICH18. It is well known that the modulation of diurnal rhythms in the human body is significantly influenced by sunlight, which is characterized by differences in geographical location and season. Sunrise and sunset times serve as critical zeitgebers closely tied to diurnal rhythms, but whether their geographical and seasonal variations can explain the observed differences in peak timing remains unknown.
The city of Chongqing is situated in southwestern China, with a longitude of 106°35′ East and a latitude of 29°31′ North, and it experiences four distinct seasons. The objective of this study was to investigate potential correlations between sunrise/sunset times and morning/afternoon onset peaks of ICH with preliminary exploration of whether geographical/seasonal variations in daylight duration may serve as potential influencing factors for diurnal variations in ICH peak onset timing.
Methods
Study design and participants
In this retrospective cross-sectional study, the data were obtained from the medical information systems of three medical institutions: University-Town Hospital of Chongqing Medical University, The Affiliated Rehabilitation Hospital of Chongqing Medical University, and Chongqing University Three Gorges Hospital. This study was approved by the hospital ethics committee with a waiver of informed consent due to its retrospective design (Ethics Approval Number: Scientific Research No. 6, 2021. Date: February 22, 2021). All methods were performed in accordance with relevant guidelines and regulations.
A total of 13,574 patients with primary ICH were initially included in the study, with data collected from January 1, 2012, to December 31, 2023. The study population consisted of patients with the first primary ICH and an age of 18 years or above. A complete cranial computed tomography and/or magnetic resonance imaging was performed on all patients within 24 h of symptom onset. The diagnosis of primary ICH was confirmed by a local neurologist and/or neurosurgeon in accordance with the criteria set forth in the relevant literature19. Cases with comorbidities involving aneurysm, coagulopathy, intracranial tumor, vascular malformation, and a previous history of ICH were excluded from the study. In addition to the previously described exclusion criteria, cases with unclear time of onset were excluded. All clinical data, including the patient’s sex, age, date and time of onset (hour-specific), health-related behaviors, past medical history, and location of hemorrhaging, were recorded.
Clinical data
The subjects were classified into three groups according to the site of hemorrhage in ICH: Deep, Lobar and Unclassified. Deep hemorrhage is defined as hemorrhaging in the basal ganglia, thalamus, pons, and deep cerebellum. Lobar hemorrhage is defined as hemorrhaging in the white matter of the frontal, parietal, temporal, or occipital lobes20. Unclassified hemorrhage is defined as hemorrhaging in areas other than deep and lobar hemorrhage. Participants were categorized by occupation into unemployed, office workers, farmers, self-employed, and retired individuals. Alcohol Consumption is defined to be those that self-reported consuming alcohol more than three times per week. Smoking was defined as current regular use (any amount). Hypertension was defined as a self-reported history of hypertension or blood pressure of 140/90 mmHg or higher. Diabetes was defined as a self-reported history of diabetes mellitus or an HbA1c level of 6.5% or higher.
Meteorologic data
The seasons are classified into four periods according to the prevailing local climate. The four seasons are defined as follows: spring (March to May), summer (June to August), autumn (September to November), and winter (December to February). The data on sunrise and sunset times for each day of the year, from January 1st to December 31st, was obtained from the local weather service. The earliest sunrise occurs at 05:53 in June, while the latest sunrise occurs at 07:49 in January. The earliest sunset occurs at 17:54 in December, while the latest sunset occurs at 19:58 in July.
Statistical analyses
Age is presented as mean (standard deviation, SD), while other variables are expressed as counts (percentages). Baseline clinical characteristics across hemorrhage location subgroups were compared using chi-square or ANOVA tests. For significant findings, post hoc pairwise comparisons were performed with Bonferroni correction. If time of day had no effect on ICH onset, an approximately uniform distribution would be expected; thus, hourly mean values served as expected frequencies. The χ2 goodness-of-fit test compared observed versus expected case frequencies per 24-hour interval to determine significant deviations. Data are reported as odds ratios (ORs) with 95% confidence intervals (CIs). Morning/afternoon peak periods identified through this method were subsequently analyzed for monthly variations correlating with sunrise/sunset time changes. Bivariate correlation analysis assessed associations between monthly shifts in morning/afternoon peak onset times and corresponding sunrise/sunset times (reported as correlation coefficient r). Partial correlation analysis further refined these relationships by controlling for confounders (reported as partial correlation r). All statistical tests used two-tailed p < 0.05 for significance. Analyses were conducted using IBM SPSS Statistics 24.0.
Results
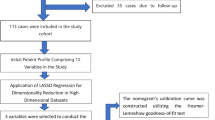
A total of 11,946 patients with the first primary ICH, with a mean age of 62.72 (12.88) years, were included in this study (Fig. 1).

Flow of participants through the screening process.
Of these, 7,310 (61.19%) were males. The patients were divided into three groups according to the location of the hemorrhage: 4,570 (63.26%) in the Deep group, 1,182 (56.39%) in the Lobar group, and 1,558 (59.33%) in the Unclassified group. Baseline characteristics differed significantly across hemorrhage location subgroups (p < 0.05). The Deep group showed significant differences in sex, smoking, and alcohol consumption compared with the other two groups (p < 0.05). The Unclassified group differed significantly in age and diabetes mellitus from the other two groups (p < 0.05). All pairwise comparisons of hypertension history among the three groups reached statistical significance (p < 0.05) (Table 1). Complete cross-tabulation data of hemorrhage locations and occupational classifications among all participants are presented in the Table S1.
Data are presented as n (%) or mean ± SD. Chi-square or ANOVA tests were performed across three hemorrhage location-based subgroups, with P-values indicating overall intergroup differences. For significant findings, pairwise post hoc comparisons were conducted using Bonferroni correction. * denotes significant differences in sex, smoking, and alcohol consumption between the Deep group and the other two groups. # indicates significant differences in age and diabetes mellitus between the Unclassified group and the other two groups. Hypertension history showed significant differences in all pairwise comparisons among the three groups. P < 0.05 was considered statistically significant.
The onset of ICH exhibited a diurnal rhythm, manifesting as a bimodal pattern, and this pattern presented similarly across all subgroups. The peaks of ICH onset showed seasonal variations. The monthly changes in morning and afternoon peaks corresponded with the shifting patterns of sunrise and sunset, respectively. The morning peak begins before sunrise and reaches its apex at sunrise, while the afternoon peak reaches its apex before sunset and ends at sunset (Fig. 2).

Seasonal variations in morning/afternoon onset peaks of primary ICH, with corresponding mean sunrise/sunset times. Data are shown as odds ratios (ORs) with 95% confidence intervals (95% CIs). (A) Spring, (B) Summer, (C) Autumn, (D) Winter.
Initial correlation analysis revealed a significant association between morning peak onset time and sunrise time in the overall cohort (r = 0.62, p = 0.032). When stratified by hemorrhage location, the Deep ICH group demonstrated significant correlations between: (1) morning peak time and sunrise (r = 0.87, p < 0.001), and (2) afternoon peak time and sunset (r = 0.77, p = 0.004). No other significant correlations were observed. After adjusting for confounders in partial correlation analysis, the Deep ICH group maintained significant associations for: (1) morning peaks with sunrise (partial r = 0.85, p = 0.002), and (2) afternoon peaks with sunset (partial r = 0.69, p = 0.025). No other correlations reached significance (Table 2).
r denotes the correlation coefficient. r# represents the partial correlation coefficient. P# indicates the p-value derived from partial correlation analysis. *P < 0.05 was considered statistically significant. The partial correlation analysis incorporated gender, age, smoking status, alcohol consumption, hypertension, and diabetes history as control variables.
Discussion
Our study confirmed a correlation between peak onset times of primary ICH and sunrise/sunset times, though this significant association was observed exclusively in the deep ICH subtype. In deep ICH, both the morning and afternoon onset peaks exhibited synchronous variations with solar events: the morning peak commenced before sunrise and peaked at sunrise, while the afternoon peak peaked before sunset and concluded at sunset.
Our observations indicated that the primary ICH onset exhibits a typical bimodal pattern, with peaks occurring in the early morning and late afternoon, which is consistent with previous findings21,22,23. Although researchers have proposed numerous potential factors influencing the diurnal rhythm of ICH onset, including both endogenous and exogenous factors, the majority of explanations have been attributed to short-term blood pressure changes24,25,26,27. Currently, hypertension as a long-term risk factor for ICH development has been relatively well defined28. In recent years, an increasing number of studies have demonstrated that the final stage of ICH onset may be associated with multiple triggers29,30,31,32,33. However, most explanations for triggers leading to ICH onset have also been attributed to short-term blood pressure changes34,35. As is well established, hypertension represents the primary etiology of deep primary ICH, which may explain our finding that significant correlations between sunrise/sunset times and onset peaks were observed exclusively in the deep ICH subtype.
This study found that the morning peak of ICH onset begins before sunrise and reaches its apex at sunrise, while the afternoon peak reaches its apex before sunset and ends at sunset. Previous studies have demonstrated that the typical 24-hour blood pressure pattern is characterized by a nocturnal rise before awakening, a marked morning surge upon waking, and two daytime peaks. The first peak occurs within 2–3 h after awakening, and the second peak typically appears during mid-to-late activity periods36. For individuals maintaining regular daytime schedules, sunrise likely coincides with morning awakening, while sunset corresponds to late activity phases. The traditional Chinese adage “work at sunrise and rest at sunset” reflects this activity pattern still prevalent in local populations, particularly among farmers and retirees. In our deep ICH cohort, farmers, retirees and unemployed individuals accounted for 64.4% of participants, suggesting most subjects presumably adhered to conventional daylight-oriented routines. These findings indicate that sunrise/sunset times may indirectly mark blood pressure peaks - known to correlate with ICH onset peaks21,22,23,24,25,26,27 - through their linkage to daily activity patterns.
Changes in sunlight affect physiological rhythms in humans, including sleep-wake cycles, body temperature fluctuations, and hormone secretion patterns37,38. These physiological rhythm alterations induce a cascade of physiological responses that subsequently influence blood pressure diurnal variations. Research has demonstrated that sunlight variations impact the human circadian clock, which regulates pituitary-adrenal axis activity, thereby modulating blood pressure diurnal rhythms39,40. Furthermore, blood pressure diurnal patterns are primarily governed by the neuroendocrine system. Sunlight-induced changes in neuroendocrine system activity consequently affect blood pressure diurnal variations41,42. Studies have revealed that sunlight variations influence the secretion of the renin-angiotensin system, sympathetic nervous system activity, and adrenocorticotropic hormone levels, ultimately regulating blood pressure diurnal rhythms43,44. These findings support that sunrise/sunset variations may indirectly regulate blood pressure peak periods through modulation of human physiological rhythms, thereby associating with ICH onset peak periods.
This study has several strengths. First, unlike most previous studies, this investigation focused on factors associated with dynamic changes in ICH onset peaks rather than on ICH incidence or replication of diurnal rhythm findings. Second, while peak periods of ICH onset have been previously established, this study uniquely associated these peak periods with sunrise/sunset times, representing a novel approach as no similar studies have been reported to date. Several limitations should be acknowledged. First, although the data were collected from multiple centers, all were located in Southwest China, leaving the generalizability of these findings to regions with different daylight hours uncertain. Second, the conclusions may be more applicable to populations with conventional diurnal activity patterns. However, due to the retrospective study design limitations, we could not include populations with atypical activity patterns and blood pressure variations, such as shift workers, insomniacs, and non-dipper hypertension patients. Finally, certain potential influencing factors (e.g., artificial lighting, physical activity, and COVID-19 pandemic-related factors) could not be comprehensively assessed due to the retrospective nature of this study. Therefore, future multi-regional prospective studies are warranted to validate and expand upon these findings.
The study confirmed a correlation between peak onset times of primary ICH and sunrise/sunset times, but this significant association was only observed in the deep ICH subtype. These findings provide a potential explanation for the variations in peak periods observed in previous studies and suggest that when addressing peak onset periods in Deep ICH, regional and seasonal variations in daylight hours should be considered.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Nyquist, P. A., Brown, R. D., Wiebers, D. O., Crowson, C. S. & O’Fallon, W. M. Circadian and seasonal occurrence of subarachnoid and intracerebral hemorrhage. Neurology 56, 190–193 (2001).
Elliott, W. J. Circadian variation in the timing of stroke onset: A meta-analysis. Stroke 29, 992–996 (1998).
Manfredini, R. et al. Circadian variation in stroke onset: Identical Temporal pattern in ischemic and hemorrhagic events. Chronobiol Int. 22, 417–453 (2005).
Passero, S., Reale, F., Ciacci, G. & Zei, E. Differing Temporal patterns of onset in subgroups of patients with intracerebral hemorrhage. Stroke 31, 1538–1544 (2000).
Sloan, M. A. et al. Circadian rhythmicity of stroke onset. Intracerebral and subarachnoid hemorrhage. Stroke 23, 1420–1426 (1992).
Wang, Y. Y., Yan, N., Wang, E. Y. & Pu, Y. T. Circadian variations in the occurrence of first-ever intracerebral hemorrhage from different sources of income: a hospital‐based cross‐sectional study. BMC Neurol 21, (2021).
Gallerani, M. et al. Acute intracerebral haemorrhage: Circadian and circannual patterns of onset. Acta Neurol. Scand. 89, 280–286 (2009).
Ricci, S. et al. Diurnal and seasonal variations in the occurrence of stroke: A Community-Based study. Neuroepidemiology 11, 59–64 (1992).
Panza, J. A., Epstein, S. E. & Quyyumi, A. A. Circadian variation in vascular tone and its relation to α-Sympathetic vasoconstrictor activity. N Engl. J. Med. 325, 986–990 (1991).
Ameriso, S. F., Mohler, J. G., Suarez, M. & Fisher, M. Morning reduction of cerebral vasomotor reactivity. Neurology 44, 1907–1907 (1994).
Stergiou, G. S. et al. Parallel morning and evening surge in stroke onset, blood pressure, and physical activity. Stroke 33, 1480–1486 (2002).
Shin, D. W. et al. Numbers of stroke patients and stroke subtypes according to highest and lowest daily temperatures in Seoul. J. Clin. Neurol. 12, 476 (2016).
Yamamoto, S. et al. Impact of low ambient temperature on the occurrence of spontaneous intracerebral Hemorrhage-Analysis of Population-Based stroke registry in toyama, Japan. J Stroke Cerebrovasc. Dis 31, (2022).
Wang, P. et al. Daily meteorological parameters influence the risk of intracerebral hemorrhage in a subtropical monsoon basin climate. Risk Manag Healthc. Policy. 14, 4833–4841 (2021).
Bodis, J., Koppan, M., Boncz, I. & Kriszbacher, I. Time of sunrise and hours with daylight May have an effect on the seasonality and diurnal variation of heart attack. Chin. Med. J. (Engl). 122, 2107–2110 (2009).
Feigin, V. L. et al. Is there a Temporal pattern in the occurrence of subarachnoid hemorrhage in the Southern hemisphere?? Pooled data from 3 large, Population-Based incidence studies in australasia, 1981 to 1997. Stroke 32, 613–619 (2001).
Shinkawa, A., Ueda, K., Hasuo, Y., Kiyohara, Y. & Fujishima, M. Seasonal variation in stroke incidence in hisayama, Japan. Stroke 21, 1262–1267 (1990).
Mayne, S. T. Antioxidant nutrients and chronic disease: use of biomarkers of exposure and oxidative stress status in epidemiologic research. J. Nutr. 133, 933S–940S (2003).
Hastings, M. H., Maywood, E. S. & Brancaccio, M. Generation of circadian rhythms in the Suprachiasmatic nucleus. Nat. Rev. Neurosci. 19, 453–469 (2018).
Covassin, N. & Somers, V. K. Sleep, melatonin, and cardiovascular disease. Lancet Neurol. 22, 979–981 (2023).
Turin, T. C. et al. Wake-Up stroke: incidence, risk factors and outcome of acute stroke during sleep in a Japanese population. Takashima stroke registry 1988–2003. Eur. Neurol. 69, 354–359 (2013).
Izumi, M. & Suzuki, K. Differentiation between stroke subtypes and the causes of monthly variations: The Akita stroke registry. Intern. Med. 60, 2933–2938 (2021).
Ripamonti, L., Riva, R., Maioli, F., Zenesini, C. & Procaccianti, G. Daily variation in the occurrence of different subtypes of stroke. Stroke Res. Treat. 2017, 1–12 (2017).
Raj, K. et al. Seasonal differences and circadian variation in stroke occurrence and stroke subtypes. J. Stroke Cerebrovasc. Dis. 24, 10–16 (2015).
Fodor, D. M., Babiciu, I. & Perju-Dumbrava, L. Circadian variation of stroke: a hospital based study. Med. Pharm. Rep. 87, 242–249 (2014).
Gross, B. A., Jankowitz, B. T. & Friedlander, R. M. Cerebral intraparenchymal hemorrhage: A review. JAMA 321, 1295 (2019).
Van Etten, E. S. et al. Trigger factors for spontaneous intracerebral hemorrhage: A Case-Crossover study. Stroke 53, 1692–1699 (2022).
Liu, J. et al. Behavioral trigger factors for hemorrhagic stroke: a case-crossover study. Postgrad. Med. J. 99, 1013–1019 (2023).
Ekker, M. S. et al. Trigger factors for stroke in young adults: A Case-Crossover study. Neurology 100, (2023).
Liu, J., Luo, C., Guo, Y., Cao, F. & Yan, J. Individual trigger factors for hemorrhagic stroke: Evidence from case-crossover and self-controlled case series studies. Eur. Stroke J. 8, 808–818 (2023).
Pu, Y. T., Yan, N., Wang, E. Y. & Wang, Y. Y. Weekly variations of intracerebral hemorrhage occurrence among different populations: A Cross-Sectional study. Front. Neurol. 12, 701929 (2021).
Pantoni, L. Cerebral small vessel disease: From pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 9, 689–701 (2010).
Hartley, T. R. et al. Hypertension risk status and effect of caffeine on blood pressure. Hypertension 36, 137–141 (2000).
Hermida, R. C. et al. Circadian rhythm of double (rate-pressure) product in healthy normotensive young subjects. Chronobiol Int. 18, 475–489 (2001).
Czeisler, C. A. et al. Stability, precision, and Near-24-Hour period of the human circadian pacemaker. Science 284, 2177–2181 (1999).
Hastings, M. H., Reddy, A. B. & Maywood, E. S. A clockwork web: Circadian timing in brain and periphery, in health and disease. Nat. Rev. Neurosci. 4, 649–661 (2003).
Scheer, F. A. J. L., Hilton, M. F., Mantzoros, C. S. & Shea, S. A. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc. Natl. Acad. Sci. 106, 4453–4458 (2009).
Dibner, C., Schibler, U. & Albrecht, U. The mammalian circadian timing system: Organization and coordination of central and peripheral clocks. Annu. Rev. Physiol. 72, 517–549 (2010).
Smolensky, M. H., Hermida, R. C. & Portaluppi, F. Circadian mechanisms of 24-hour blood pressure regulation and patterning. Sleep. Med. Rev. 33, 4–16 (2017).
Portaluppi, F., Smolensky, M. H., Touitou, Y., Ethics & and methods for biological rhythm research on animals and human beings. Chronobiol Int. 27, 1911–1929 (2010).
Scheer, F. A. J. L., Ter Horst, G. J., Van Der Vliet, J. & Buijs, R. M. Physiological and anatomic evidence for regulation of the heart by Suprachiasmatic nucleus in rats. Am. J. Physiol. -Heart Circ. Physiol. 280, H1391–H1399 (2001).
Martino, T. A. & Sole, M. J. Molecular time: an often overlooked dimension to cardiovascular disease. Circ. Res. 105, 1047–1061 (2009).
Greenberg, S. M. et al. 2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline From the American Heart Association/American Stroke Association. Stroke 53, (2022).
Sheth, K. N. Spontaneous intracerebral hemorrhage. N Engl. J. Med. 387, 1589–1596 (2022).
Funding
The study was supported by Medical research project of Chongqing Municipal Health Commission (2024WSJK079).
Author information
Authors and Affiliations
Contributions
Study design: Y.Y.W., and Y.T.P.; Data collection: Y.Y.X., M.Z, and E.Y.W.; Data analysis: Y.Y.W., and Y.T.P.; Writing of the original version: Y.Y.W., and Y.T.P.; Revision: Y.T.P.; Approval: All authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, YY., Wang, EY., Xiang, YY. et al. Correlation between sunrise/sunset times and peak onset periods of primary intracerebral hemorrhage. Sci Rep 15, 24002 (2025). https://doi.org/10.1038/s41598-025-09170-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-09170-0
