
Abstract
Numerous studies have explored root anatomy and root canal morphology variations across ethnic groups, but few have focused on the Jordanian population. This study, aimed to assess the prevalence of root anatomy and canal morphology in permanent teeth of a Jordanian subpopulation using cone-beam computed tomography (CBCT). This part of a four-part series focused on mandibular first and second molar teeth. Subsequent parts will address the root anatomy and canal morphology of (1) mandibular anterior teeth, (2) maxillary molars, and (3) maxillary and mandibular premolars. CBCT scans of 332 mandibular molars from patients treated at The University of Jordan Hospital between June and December 2022 were analysed. Canal configurations were categorized according to Vertucci’s classification. The majority of mandibular first and second molars had two roots (96.2% and 85%, respectively), with variations such as a third root or a single C-shaped root. Most mesial roots had two canals (100% of first molars, 98.6% of second molars), and distal roots predominantly had one canal (77.9% of first molars, 97.4% of second molars). The most common mesial canal configuration was type II (68% in first molars, 83.7% in second molars), while type I was most common in distal roots (77.8% in first molars, 97.4% in second molars). No significant gender-related differences were found. The study also revealed asymmetry in root morphology between the right and left sides. The root and canal morphology of Jordanian mandibular molars closely resembled the average features observed in Arab and Caucasian populations.
Similar content being viewed by others


Introduction
Successful root canal treatment relies on the thorough debridement and disinfection of the root canal system. A major cause of endodontic treatment failure is the inability to identify and treat all root canals1. Therefore, knowledge of possible root canal anatomy variations is essential for achieving successful outcomes2. Additionally, understanding root canal anatomy holds significance in anthropological research, particularly in reconstructing human population histories3.
Various methods have been used to study the internal anatomy of teeth, yielding variable results. Laboratory techniques include clearing and staining techniques (diaphonization)4, magnetic resonance imaging5, microcomputed tomography6, and cross-sectioning and histological examinations of extracted teeth7. Clinically, preoperative periapical radiographs taken at different angles remain the most commonly used method to assess the number of roots and the root canal morphology of teeth prior to root canal treatment8. Cone-beam computed tomography (CBCT) has emerged as an adjunctive diagnostic tool, particularly in cases involving highly complex root canal systems9. CBCT technology addresses the inherent limitations of conventional radiographs by providing three-dimensional imaging, enabling a more detailed visualization of anatomical structures10.
Numerous studies have explored root anatomy and root canal morphology variations across different ethnic groups. However, relatively few studies have focused on these aspects in Jordanian populations4,11,12,13,14,15,16,17. The Jordanian subpopulation represents a distinct ethnic group with unique genetic and environmental factors that may influence root and root canal anatomy18. Understanding these population-specific variations is critical for endodontic practitioners, as it allows them to deliver more precise and effective care to patients in Jordan.
Studies examining root canal morphology in Jordanian populations have primarily utilized the clearing and staining technique13,14,15,16. Only three studies have employed CBCT for this purpose. One study investigated the incidence and morphology of the second mesiobuccal canal in the maxillary first molars17, another evaluated the C-shaped canal configuration in mandibular second molars12, and a third assessed the prevalence of multiple canals in mandibular anterior teeth19. Hence, this study aims to assess the prevalence of root anatomy and root canal morphology in permanent mandibular first and second permanent molar teeth of a Jordanian subpopulation using CBCT.
Materials and methods
This study was conducted in accordance with the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines20,21 and utilized the STROBE Checklist for Cross-sectional Studies to guide the study’s design and reporting of results.
This study was approved by the Institutional Review Board at Jordan University Hospital/University of Jordan (IRB-JUH) and was conducted in full accordance with the World Medical Association Declaration of Helsinki. All Jordanian patients who were treated at the University of Jordan Hospital and had undergone CBCT scanning between June 2022 and December 2022 were identified. Patients were included if they had fully developed permanent mandibular first and/or second molars, and if the CBCT scan quality was sufficient to assess the complete root canal morphology. CBCT scans were excluded if they showed:
-
Root canal treatment that altered the native canal anatomy.
-
Posts, crowns, or restorations causing artefacts.
-
Internal or external root resorption.
-
Poor image quality or limited field of view that impeded clear identification of the root canal anatomy.
The scans were performed for various clinical purposes, including implant planning, assessment of maxillofacial pathology, and oral surgical, orthodontic and endodontic evaluations. As such, variations in field of view, voxel size, and diagnostic intent may have influence on the results, these methodological limitations are further elaborated upon in the discussion section. No patient underwent CBCT scanning solely for the purposes of this study.
CBCT scans were acquired using a CS9300 scanner (Carestream health, Rochester, New York). The scanner offers a range of fields of view (5 × 5 cm to 17 × 13.5 cm), isotropic resolutions (90 mm to 500 μm), and scan times between 12 and 20 s. Carestream 3D imaging software was used to view and analyse the images.
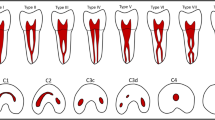
Two examiners collaboratively: LAG, a specialist in dentomaxillofacial radiology, and RAZ, a specialist in endodontics analysed the CBCT images in a darkened room. Brightness, contrast, and sharpness settings were adjusted as necessary to enhance visualisation. The two examiners assessed the scans in the axial, coronal and sagittal planes. In cases of interexaminer disagreement, they reviewed the images together to reach a consensus. The canal configurations were categorised according to Vertucci’s classification22, as shown in Table 1.
The sample size for this study was determined to assess the anatomical features of mandibular molars, with a particular focus on the number and configuration of root canals as classified by Vertucci. To calculate the appropriate sample size, we employed a standard formula for estimating proportions with a 95% confidence level and a 5% margin of error. Given the variability in molar anatomy, particularly in root canal systems, we used an expected proportion (P) of 0.5, which represents the most conservative estimate when prior data are unavailable. The calculation indicated a required sample size of approximately 384 roots. A total of 332 molars were included in the study, comprising 78 right first molars, 81 right second molars, 81 left first molars, and 92 left second molars, yielding a total of 663 roots. This sample size provides sufficient statistical power to analyse the anatomical variation of mandibular molars and to determine the distribution of root canal systems across different molar types within a Jordanian population. Statistical analysis was performed using SPSS for Windows, version 16.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were generated to summarize the data. Group differences were analysed using the chi-square test for categorical variables when the assumptions of the test were met (i.e., all expected cell counts ≥ 5). When expected frequencies were small, Fisher’s exact test was applied. A significance level was set at P < 0.05.
Results
During the study period, 127 patients underwent CBCT scans. Of these, 20 scans were excluded due to the absence of all four mandibular molars, and 2 scans were excluded because the limited field of view did not include the mandibular molars. This resulted in a final sample of 105 scans. Additionally, 87 teeth were missing across the sample. One mandibular first molar was excluded due to external inflammatory resorption.
The final sample comprised 332 mandibular first and second molars, of which 202 (60.8%) were from female patients and 130 (39.2%) were from male patients.
Significant differences were observed in the number of roots between the mandibular first and second molars (P = 0.001) (Table 2). Most mandibular molars had two roots, with 90.2% of mandibular first molars and 85% of second molars exhibiting this feature. Single-rooted molars were more common among second molars (9.8%) compared to first molars (0.6%), while all three cases of four-rooted molars occurred in second molars. Although the number of roots did not significantly differ between male and female patients (P = 0.22), single-rooted (C-shaped root) and three-rooted molars were more frequently observed in female patients compared to male patients (Fig. 1).

Number of roots of mandibular permanent molars according to sex.
Significant differences were observed in the number of root canals between mandibular first and second molars (P < 0.001) (Table 3). A single root canal was identified in only four mandibular second molars. Two root canals were found in nine mandibular second molars, representing 2.7% of the sample.
Among the mandibular first molars, 76.1% had three root canals, and 23.9% had four root canals. In contrast, 87.3% of the mandibular second molars had three root canals, with only 5.2% had four root canals.
No significant differences were found in the number of root canals between males and females (P = 0.34). However, molars with four root canals were more prevalent in male patients (17.7%) compared to female patients (11.9%). Similarly, no significant differences in the prevalence of root canals were observed between the right and left sides (P = 0.72).
The number of root canals in each root of the mandibular molars included in this study is shown in Table 4.
In mandibular molars with two roots (mesial and distal), all the mesial roots of the mandibular first molars and 98.6% of those in the second molars contained two root canals. In contrast, 77.9% of the distal roots in the mandibular first molars and 97.4% of those in the second molars had a single root canal, with the remainder having two canals.
The number of root canals in the distal roots did not significantly differ based on to the patient’s sex or the tooth’s side (right or left).
Among mandibular molars with a single c-shaped root (n = 18), the likelihood of having one root canal was 22.2%, while the likelihood of having two or three root canals was 38.9% each. In mandibular molars with three or four roots, each root consistently contained a single root canal.
The Vertucci classification of the root canals in mandibular molars is shown in Table 5. The most common root canal configurations were type I (46.3%) and type II (40.9%), followed by type IV (11.3%). Type III was rare, observed in only one distal root of a right second molar and two mesial roots of right second molars. Type VIII and an additional root canal configuration (three canals joining near the apex) were found exclusively in single-rooted molars. Types V, VI, and VII were not identified in this study.
There were no significant differences between males and females in the Vertucci classifications of root canals for any root: the mesial (P = 0.27) or distal (P = 0.53) roots of right first molars; the mesial (P = 0.52) or distal (P = 0.28) roots of left first molars; the mesial (P = 0.96) or distal (P = 0.24) roots of right second molars; and the mesial (P = 0.35) or distal (P = 0.80) roots of left second molars.
Asymmetry in root and root canal morphology was detected when comparing the right and left sides of the same patient (Fig. 2). Among the 63 patients with both mandibular first molars intact (25 males and 38 females), 7 patients (11.1%) exhibited asymmetry in the number of roots, root canals, or canal configurations. Similarly, of the 76 patients with intact mandibular second molars, 14 patients (18.4%) displayed asymmetry.

CBCT scan axial section reveals asymmetry in the number of roots of the mandibular second molars, with the right side displaying four roots, while the left side has only three roots.
Discussion
Knowledge of the varying morphologies of root canals among individuals is essential for successful endodontic treatment1. Clinicians must be aware of the prevalence of different configurations in mandibular first and second molars to ensure adequate root canal preparation, effective debridement and proper obturation1. The use of CBCT for the assessment of root canal morphologies has increased recently and is widely recognized as a valuable tool for mapping the complex root canal system23.
A review of the literature revealed that numerous studies have employed CBCT imaging to assess the root canal morphologies of permanent mandibular molars across diverse ethnic populations24,25,26. However, no previous studies have specifically investigated these morphologies in the Jordanian population. One Jordanian study focused solely on the prevalence of C-shaped canals in mandibular second molars using CBCT12. Another study evaluated mandibular molar morphologies in a Jordanian population using the visual tooth-clearing technique16. While tooth-clearing methods provide detailed in vitro examination of internal anatomy, CBCT offers a clinically applicable, three-dimensional visualization of spatial canal configurations27.
The present study examined the root and root canal morphology of mandibular first and second permanent molars in a Jordanian subpopulation using CBCT scans obtained for clinical purposes unrelated to this research. Although the sample may not represent the entire Jordanian population, it is reasonable to assume that root and canal morphology remains relatively consistent within a population of uniform ethnic background16. Consequently, the findings of this study are likely generalizable to the broader Jordanian population.
First molars
Our findings align with previous research, demonstrating that the majority of mandibular molars have two roots. Approximately 96.2% of mandibular first molars in our study had 2 roots, consistent with findings from a previous study using the extracted tooth clearing and staining technique (96%)16. This prevalence is comparable to studies utilizing CBCT in other populations, such as the Chilean (99.8%)28,29, Greek (96.4%)25, and Iranian (96.7%)30. However, these rates were significantly higher than those reported for the Chinese population using the same methodology, where only 70% of mandibular first molars had two roots24. Such discrepancies may reflect ethnic differences in dental anatomy.
Additionally, the prevalence of three-rooted mandibular first molars (3.1%) was similar to findings in the Jordanian (4%)16, Sudanese (3%)31, Greek (3.3%)25, Turkish (2.06%)29 and Iranian (1.9%)30 populations. These rates are substantially lower than those observed in studies on the Chinese population (29%)24 and Thai population (12.7%)32, highlighting ethnic variability. The accurate detection of three roots using CBCT emphasises the importance of high-quality pretreatment radiographs to confirm the presence of additional roots.
Regarding root canal morphology, 76.1% of mandibular first molars had three canals, while 23.9% had four canals. This suggests a greater likelihood of encountering three canals in these teeth, consistent with Demirbuga et al. (79.9%)29. However, Al-Qudah and Awawdeh reported a more balanced prevalence of three and four canals (48% and 46%, respectively)16, which may be attributed to methodological differences. Similarly, Zhang et al. (2011) found a comparable distribution (56% and 43%, respectively)24, further supporting the potential influence of ethnic variations on root canal anatomy.
The mesial roots of all mandibular first molars in this study consistently presented with two canals, exceeding the percentages reported by Al-Qudah and Awawdeh (93%)16 andDemirbuga et al. (2013) (96.9%)29. Lower percentages were noted in studies conducted on other populations (95%24, 81.5%28) and via extracted tooth-clearing methods (86%)31. All the studies cited seem to agree that the mesial canals of mandibular first molars most commonly present as two canals, implying that a dentist can be confident that they will encounter two canals in the mesial root when accessing this tooth. Among the distal roots, 77.8% had one root canal, in accordance with other studies but with a lower prevalence (84%24 and 85.9%28). This is clinically significant when accessing the tooth, as the clinician should not assume that all distal roots contain only a single canal; a significant minority may contain two canals, necessitating thorough exploration for optimal treatment outcomes.
In terms of the Vertucci classification, the most common configurations in this study were type II and type IV canals, particularly in the mesial roots of mandibular first molars (68% and 32%, respectively). This aligns with findings in the Greek population, where type II canals predominated (69.9%), followed by type IV (26.3%)25. However, other studies reported type IV as the most common configuration in the mesial roots, with prevalences ranging from 53 to 81% depending on the population and methodology16,24,29,30,33. The absence of type V canals in our study contrasts with previous findings16,24, which may be due to differences in sample size or study design.
Asymmetry in root and canal morphology was observed in 11.1% of patients with both mandibular first molars present. This finding emphasizes the need for clinicians to be vigilant when treating homologous teeth within the same patient, as asymmetry could influence treatment planning and outcomes34.
Second molars
The vast majority of second molars in our study had two roots (85%), a percentage comparable to those reported by Al-Qudah & Awawdeh (2009) (82%, excluding 5.4% with fused roots)16, Demirbuga et al. (2013)(85%)29, Kantilieraki et al. (2019)(82.8%)25, Abarca et al. (2020) (86%)28, and Madani et al. (2017) (81.6%)30. However, our findings were slightly higher than those of Zhang et al. (2011) (76%)24 and Ahmed et al. (2007) (78%, excluding 8% with fused roots)31.
In this study, 9.8% of second molars were single-rooted, which is slightly lower than the 12.7% reported by Al-Qudah and Awawdeh (2.3% of these were conically rooted)16. Higher percentages of single-rooted second molars were reported by Zhang et al. (2011) (22%)24, and Abarca et al. (2020) (13.6%)28.
Across studies, the number of canals in second molars varied widely, although three canals were most commonly observed. In our study, 87.3% of second molars had three root canals, while 5.2% had two root canals and 5.2% had four root canals. These results contrast with those of Al-Qudah and Awawdeh16, who reported that 58% of mandibular second molars had three canals, 19% had two canals, and 17% had four canals. Similarly, in a study conducted on the Turkish population, Demirbuga et al. (2013), found that 72.8% of second molars had three canals, while 22.8% had two canals29.
In this study, 98.6% of the mesial roots of second molars had two root canals. This percentage is significantly higher than those reported in studies on the Jordanian population using direct visualisation methods, including Al-Qudah and Awawdeh (2009)(81%)16 and Ahmed et al. (2007) (83%)31. However, our findings closely align with the results of Demirbuga et al. (2013) (97.75%)29 and Zhang et al. (2011) (97%)24. These results highlight the enhanced capability of CBCT to identify secondary canals that may be missed with direct visualisation methods.
Most studies agree that the majority of distal roots of second molars have a single root canal, although the reported prevalence varies. In our study, 97.4% of distal roots in second molars had one root canal, closely aligning with the findings of Zhang et al. (2011) (97%)24. However, this percentage was higher than those reported by Al-Qudah & Awawdeh (2009) (79%)16, Abarca et al. (2020) (84.3%, in the cervical third of the distal root)28 and Ahmed et al. (2007) (69%)31. Clinicians should remain vigilant about potential variations in root canal morphology and avoid assuming uniformity across patients.
Clinicians should be mindful of the high likelihood of second canals in both the mesial and distal roots to ensure effective disinfection of the entire root canal system, which is essential for successful endodontic outcomes.
With respect to Vertucci classification, our results revealed that the most common configuration in mesial roots was type II (83.7%), followed by type IV (13.6%). This differs from most other studies, which identified type IV as the most prevalent configuration, followed by type II, with prevalence rates of 40% and 33%, respectively16; 37.3% and 35.9%29, 42.9% and 28%30, 63% and 18%31, and 57.4% and 20.4%32. These discrepancies may reflect differences in sample sizes, ethnic variations, or methods used to assess canal morphology. Interestingly, Kantilieraki et al. (2019)25 reported a similar finding, with mesial roots predominantly exhibiting type II (64.1%), followed by type IV (14.1%).
For distal canals, our study revealed that most presented as type I, consistent with findings across all previously cited studies, regardless of ethnicity or the methods employed to visualize the root canal system16,24,28,29,32,33.
Among the 76 patients with mandibular second molars present, 14 patients (18.4%) exhibited asymmetry. These data should alert clinicians when treating homologous teeth within the same patient34.
Previous studies have suggested a relationship between root development and the X chromosome, which may influence specific aspects of tooth and root formation, contributing to variations in root canal numbers and systems35. In this study, no significant differences were found between genders regarding Vertucci classification or the number of canals in each root. However, a greater percentage of molars in male patients (17.7%) compared to female patients (11.9%) contained four root canals. These findings align with similar studies conducted on other ethnic populations, which also reported no significant differences between genders36,37,38.
Our study also revealed no significant sex-related difference in the root canal system of mesial and distal roots. This observation is consistent with the findings of Martins et al. (2018), who used CBCT to assess root and canal morphology differences by sex in a Portuguese subpopulation39. However, it contrasts with the study by Mashyakhy et al. (2021), which identified significant differences in a Saudi Arabian population40. In their study, distal roots in females exhibited a higher prevalence of Vertucci types II and III, while males had a higher prevalence of Vertucci type V.
While variations in the reported root and root canal morphology across populations may partly reflect ethnic variations, it is important to acknowledge that methodological differences can significantly influence the reported prevalence rates. Even among studies utilizing CBCT to assess root canal anatomy, substantial variability exists in the type of CBCT machines used, as well as in critical exposure settings (e.g., Kilovoltage [Kv], milliamperage [mA], voxel size, field of view [FOV], and slice thickness), in addition to the software employed for data reconstruction and visualization33. Therefore, variability between studies is likely influenced not only by ethnic differences but also by these methodological factors.
The present study has certain limitations. First, the CBCT scans analysed were retrospectively sourced from a clinical archive and had been acquired for a variety of diagnostic reasons, rather than solely for endodontic purposes. This broader clinical context may reduce the selection bias often linked to studies including CBCT scans taken solely for endodontic indications because CBCT is typically employed in endodontics when traditional imaging methods prove inadequate due to intricate anatomical variations41,42. Which could limit the generalizability of the results to the wider population and overestimate the prevalence of atypical root canal anatomy. On the other hand, the reliability of CBCT imaging is highly dependent on the voxel size, with smaller voxel sizes providing more accurate and detailed results. The scans used in this study were acquired not only for endodontic purposes but also for surgical, orthodontic, and prosthetic purposes. The CS9300 scanner used in this study offers fields of view ranging from 5 cm x 5 cm to 17 cm x 13.5 cm and voxel size between 90 and 500 μm. If only small field-of-view and small voxel size scans obtained specifically for endodontic purposes were analysed, finer details may have been more visible. Although Hatipoğlu et al. reported that voxel size (above or below 150 μm) does not significantly affect the detection of third mesial canals in mandibular molars43. Despite this, variation in CBCT scanner models and acquisition settings remain critical factors in CBCT-based anatomical research and may affect the reproducibility of findings across different studies. Furthermore, while the sample size in the present study was sufficient for preliminary morphological assessment, increasing the sample size of teeth studied could enhance the consistency and reliability of the data, allowing for more definitive conclusions about the common morphological characteristics of these teeth.
While all images were evaluated jointly by a specialist in dentomaxillofacial radiology and specialist endodontist through consensus, and efforts were made to ensure consistent interpretations, no statistical measure (e.g., Cohen’s kappa) was applied. This may limit the reproducibility of the findings, and future studies should consider employing independent, blinded evaluations by multiple examiners, followed by statistical agreement analysis (e.g., Cohen’s kappa), to enhance methodological rigour and reproducibility.
Clinical relevance
The present study demonstrated a common occurrence of multiple root canals within individual roots of mandibular first and second molars. In light of these findings, conventional intraoral periapical radiography should be supplemented with additional angulated views (10–20° mesial or distal shifts) to better visualize complex root canal systems and reduce anatomical overlap44. In cases where conventional imaging yields inconclusive results, the use of a small field-of-view cone-beam computed tomography (CBCT) scan is recommended to provide a detailed three-dimensional assessment of the root canal anatomy41.
The occurrence of joining canals (Vertucci Types II, III, and the 3 − 1 canal pattern) was found to be common. This finding further highlights the clinical value of employing electronic apex locators for early identification of canal convergence before the initiation of mechanical shaping. Early confirmation of confluence facilitates more conservative canal preparation, thereby reducing the risk of procedural complications such as dentinal wall stripping, apical transportation, or instrument separation45.
Furthermore, roots exhibiting joining canal configurations often contain isthmuses that are difficult to adequately clean with conventional mechanical instrumentation. This highlights the importance of adopting modern endodontic instruments specifically designed to better conform to the native canal anatomy while minimizing unnecessary dentin removal. Among these, the XP-endo Shaper (FKG Dentaire, Switzerland) which has demonstrated superior efficacy in bacterial reduction compared to traditional systems46. Additionally, activation of sodium hypochlorite through ultrasonic techniques is advised to optimize disinfection within these intricate anatomical spaces47.
Due to the higher prevalence of anatomical variations observed in mandibular second molars compared to first molars; thorough evaluation of these teeth is essential. Referral to an endodontic specialist may be prudent in situations where complex morphology is anticipated, in order to optimize treatment outcomes and reduce the risk of procedural errors48.
Conclusion
CBCT provides a reliable clinical method for assessing root canal morphology, with results comparable to those obtained from other in vitro techniques. The root and canal morphology of Jordanian mandibular first and second molars closely resemble the typical features observed in Caucasian populations. The findings of this study highlight the importance of preoperative imaging and thorough exploration during endodontic treatment. Recognizing potential anatomical variations within the same patient can impact the success of root canal therapy, emphasising the need for individualized treatment planning.
Data availability
The datasets used and/or analysed during this study are available upon request from the corresponding author.
Abbreviations
- CBCT:
-
cone-beam computed tomography
- STROBE:
-
The strengthening the reporting of observational studies in epidemiology
References
Costa, F. et al. Association between missed canals and apical periodontitis. Int. Endod J. 52, 400–406 (2018).
Siqueira Junior JF, Rôças I das N, Marceliano-Alves MF, Pérez AR, Ricucci D. Unprepared root canal surface areas: causes, clinical implications, and therapeutic strategies. Braz. Oral. Res. (2018).
Katge, F. & Dixit, U. B. Root and root Canal anatomy of primary mandibular central incisor, lateral incisor, and canine in Indian children: A cone beam computed tomography study, https://doi.org/10.1155/2022/7191134 (2022).
Khraisat, A. & Smadi, L. Canal configuration in the mesio-buccal root of maxillary first molar teeth of a Jordanian population. Aust Endod J. 33, 13–17. https://doi.org/10.1111/J.1747-4477.2007.00055.X (2007).
Timme, M. et al. Imaging of root Canal treatment using ultra high field 9.4T UTE-MRI – a preliminary study. Dentomaxillofacial Radiol. 49 https://doi.org/10.1259/DMFR.20190183 (2020).
Verma, P. & Love, R. M. A Micro CT study of the mesiobuccal root Canal morphology of the maxillary first molar tooth. Int. Endod J. 44, 210–217. https://doi.org/10.1111/J.1365-2591.2010.01800.X (2011).
Melton, D. C., Krell, K. V. & Fuller, M. W. Anatomical and histological features of C-shaped canals in mandibular second molars. J. Endod.. 17, 384–388. https://doi.org/10.1016/S0099-2399(06)81990-4 (1991).
Horner, K. & Eaton, K. A. Selection Criteria for Dental Radiography 3rd edn (FGDP (UK), (2018).
Patel, S. et al. European society of endodontology position statement: the use of CBCT in endodontics. Int. Endod J. 47, 502–504. https://doi.org/10.1111/IEJ.12267 (2014).
Cotton, T. P., Geisler, T. M., Holden, D. T., Schwartz, S. A. & Schindler, W. G. Endodontic applications of cone-beam volumetric tomography. J. Endod. 33, 1121–1132. https://doi.org/10.1016/J.JOEN.2007.06.011 (2007).
Smadi, L. & Khraisat, A. Detection of a second mesiobuccal Canal in the mesiobuccal roots of maxillary first molar teeth. oral surgery, oral medicine, oral pathology. Oral Radiol. Endodontol.. 103 https://doi.org/10.1016/j.tripleo.2006.10.007 (2007).
Al Omari, T. et al. A CBCT based cross sectional study on the prevalence and anatomical feature of C shaped molar among Jordanian. Sci. Rep.. 12, 1. https://doi.org/10.1038/s41598-022-20921-1 (2022).
Al-Qudah, A. A. & Awawdeh, L. A. Root Canal morphology of mandibular incisors in a Jordanian population. Int. Endod. J. 39, 873–877. https://doi.org/10.1111/J.1365-2591.2006.01159.X (2006).
Awawdeh, L. A. & Al-Qudah, A. A. Root form and Canal morphology of mandibular premolars in a Jordanian population. Int. Endod. J. 41, 240–248. https://doi.org/10.1111/J.1365-2591.2007.01348.X (2008).
Awawdeh, L., Abdullah, H. & Al-Qudah, A. Root form and Canal morphology of Jordanian maxillary first premolars. J. Endod.. 34, 956–961. https://doi.org/10.1016/J.JOEN.2008.04.013 (2008).
Al-Qudah, A. A. & Awawdeh, L. A. Root and Canal morphology of mandibular first and second molar teeth in a Jordanian population. Int. Endod. J. 42, 775–784. https://doi.org/10.1111/J.1365-2591.2009.01578.X (2009).
Alsaket, Y. M., El-Ma’aita, A. M., Aqrabawi, J. & Alhadidi, A. Prevalence and configuration of the second mesiobuccal Canal in the permanent maxillary first molar in Jordanian population sample. Iran. Endod. J. 15, 217–220. https://doi.org/10.22037/IEJ.V15I4.27692 (2020).
Alzer, H., Alhadidi, A., Al-Shayyab, M. H., Sabrah, A. H. & Alsoleihat, F. Unexpectedly low levels of dental morphological asymmetry suggesting developmental resilience amongst living jordanians: A cone beam computed tomography study. HOMO 71, 1–8. https://doi.org/10.1127/HOMO/2019/1029 (2020).
Taha, N. A., Makahleh, N. & Hatipoglu, F. P. Root Canal morphology of anterior permanent teeth in Jordanian population using two classification systems: a cone-beam computed tomography study. BMC Oral Health. 24, 170. https://doi.org/10.1186/S12903-024-03934-2/TABLES/6 (2024).
von Elm, E. et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int. J. Surg. 12, 1495–1499. https://doi.org/10.1016/J.IJSU.2014.07.013 (2014).
Vandenbroucke, J. P. et al. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. Int. J. Surg. 12, 1500–1524. https://doi.org/10.1016/J.IJSU.2014.07.014 (2014).
Vertucci, F. J. Root Canal anatomy of the human permanent teeth. oral surgery, oral medicine. Oral. Pathol. 58, 589–599. https://doi.org/10.1016/0030-4220(84)90085-9 (1984).
Tomaszewska, I. M. et al. Internal and external morphology of mandibular molars: an original micro-CT study and meta-analysis with review of implications for endodontic therapy. Clin. Anat. 31, 797–811. https://doi.org/10.1002/CA.23080 (2018).
Zhang, R. et al. Use of cone-beam computed tomography to evaluate root and Canal morphology of mandibular molars in Chinese individuals. Int. Endod. J. 44, 990–999. https://doi.org/10.1111/J.1365-2591.2011.01904.X (2011).
Kantilieraki, E., Delantoni, A., Angelopoulos, C. & Beltes, P. Evaluation of root and root Canal morphology of mandibular first and second molars in a Greek population: A CBCT study. Eur. Endod. J. 4, 62–68. https://doi.org/10.14744/EEJ.2019.19480 (2019).
Celikten, B. et al. Cone beam CT evaluation of mandibular molar root Canal morphology in a Turkish Cypriot population. Clin. Oral. Investig.. 20, 2221–2226. https://doi.org/10.1007/S00784-016-1742-2 (2016).
Patel, S. et al. Cone beam computed tomography in Endodontics – a review of the literature. Int. Endod. J. 52, 1138–1152. https://doi.org/10.1111/IEJ.13115 (2019).
Abarca, J. et al. Root morphology of mandibular molars: a cone-beam computed tomography study. Folia Morphol. (Warsz). 79, 327–332. https://doi.org/10.5603/FM.A2019.0084 (2020).
Demirbuga, S., Sekerci, A. E., Dinçer, A. N., Cayabatmaz, M. & Zorba, Y. O. Use of cone-beam computed tomography to evaluate root and Canal morphology of mandibular first and second molars in Turkish individuals. Med. Oral. Patol. Oral Cir. Bucal. 18 https://doi.org/10.4317/MEDORAL.18473 (2013).
Madani, Z. S., Mehraban, N., Moudi, E. & Bijani, A. Root and Canal morphology of mandibular molars in a selected Iranian population using Cone-Beam computed tomography. Iran. Endod. J. 12, 143–148. https://doi.org/10.22037/IEJ.2017.29 (2017).
Ahmed, H. A., Abu-bakr, N. H., Yahia, N. A. & Ibrahim, Y. E. Root and Canal morphology of permanent mandibular molars in a Sudanese population. Int. Endod. J. 40, 766–771. https://doi.org/10.1111/J.1365-2591.2007.1283.X (2007).
Gulabivala, K., Opasanon, A., Ng, Y. L. & Alavi, A. Root and Canal morphology of Thai mandibular molars. Int. Endod. J. 35, 56–62. https://doi.org/10.1046/J.1365-2591.2002.00452.X (2002).
Ahmed, H. M. A. A critical analysis of laboratory and clinical research methods to study root and Canal anatomy. Int. Endod J. 55, 229–280. https://doi.org/10.1111/IEJ.13702 (2022).
Felsypremila, G., Vinothkumar, T. S. & Kandaswamy, D. Anatomic symmetry of root and root Canal morphology of posterior teeth in Indian subpopulation using cone beam computed tomography: A retrospective study. Eur. J. Dent. 9, 500. https://doi.org/10.4103/1305-7456.172623 (2015).
Varrela, J. Effect of 45,X/46,XX mosaicism on root morphology of mandibular premolars. J. Dent. Res. 71, 1604–1606. https://doi.org/10.1177/00220345920710091101 (1992).
Mashyakhy, M. & Gambarini, G. Root and root Canal morphology differences between genders: A comprehensive in-vivo CBCT study in a Saudi population. Acta Stomatol. Croat. 53, 231–246. https://doi.org/10.15644/ASC53/3/5 (2019).
Sert, S. & Bayirli, G. S. Evaluation of the root Canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J. Endod. 30, 391–398. https://doi.org/10.1097/00004770-200406000-00004 (2004).
Alhujhuj, R. R. et al. Evaluation of root Canal configuration of maxillary and mandibular first molar by CBCT: A retrospective Cross-Sectional study. Diagnostics 12 https://doi.org/10.3390/DIAGNOSTICS12092121 (2022).
Martins, J. N. R., Marques, D., Francisco, H. & Caramês, J. Gender influence on the number of roots and root Canal system configuration in human permanent teeth of a Portuguese subpopulation. Quintessence Int. 49, 103–111. https://doi.org/10.3290/J.QI.A39508 (2018).
Mashyakhy, M. et al. Anatomical evaluation of mandibular molars in a Saudi population: An in vivo cone-beam computed tomography study. Int. J. Dent.https://doi.org/10.1155/2021/5594464 (2021).
Patel, S., Brown, J., Semper, M., Abella, F. & Mannocci, F. European society of endodontology position statement: use of cone beam computed tomography in endodontics: European society of endodontology (ESE) developed by. Int. Endod. J. 52, 1675–1678. https://doi.org/10.1111/IEJ.13187 (2019).
Fayad, M. I. et al. AAE and AAOMR joint position statement: use of cone beam computed tomography in endodontics 2015 update. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 120, 508–512. https://doi.org/10.1016/J.OOOO.2015.07.033 (2015).
Pertek Hatipoğlu, F. et al. Assessment of the prevalence of middle mesial Canal in mandibular first molar: A multinational Cross-sectional study with Meta-analysis. J. Endod. 49, 549–558. https://doi.org/10.1016/J.JOEN.2023.02.012 (2023).
Sarsam, W., Davies, J. & Al-Salehi, S. K. The role of imaging in endodontics. Br. Dent. J. 2025. 238, 7. https://doi.org/10.1038/s41415-025-8511-z (2025).
Do, S. & Seo, M-S. The effect of different confluence confirmation strategies on the obturation of Vertucci type II canal: micro-CT analysis. Restor. Dent. Endod.. 46, e12. https://doi.org/10.5395/RDE.2021.46.E12 (2021).
Loyola-Fonseca, S. C. et al. Disinfection and shaping of Vertucci class II root canals after Preparation with two instrument systems and supplementary ultrasonic activation of sodium hypochlorite. J. Endod.. 49, 1183–1190. https://doi.org/10.1016/J.JOEN.2023.06.017 (2023).
Zou, X. et al. Expert consensus on irrigation and intracanal medication in root canal therapy n.d. https://doi.org/10.1038/s41368-024-00280-5
British Dental Journal. BES publishes A guide to good endodontic practice. Br. Dent. J. 233, 456 (2022).
Acknowledgements
The authors would like to thank Dr Heba Alzer for her help in the references formatting.
Author information
Authors and Affiliations
Contributions
R.A.Z: Conceptualization, data curation, original draft preparationL.A.Q: Data curationF.M.: original draft preparationF.M.: original draft preparationF.S.: Formal analysisAll the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was approved by the Institutional Review Board at Jordan University Hospital/University of Jordan (IRB-JUH). This research was conducted in full accordance with the World Medical Association Declaration of Helsinki. The informed consent was waived by the ethics committee as the study is retrospective.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zaghlan, R.A., Qdais, L.A., Mansour, F. et al. Root and root canal morphology of mandibular first and second molars in a Jordanian subpopulation: a cross-sectional cone-beam computed tomography study. Sci Rep 15, 33969 (2025). https://doi.org/10.1038/s41598-025-11117-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-11117-4
