
Abstract
Buddhist ordination involves significant lifestyle changes including meal timing, diet, and sleep patterns, yet short-term physiological effects remain poorly understood. This study examined effects of two-week ordination on dietary intake, body composition, and sleep quality in newly ordained Thai Dhammayut monks. Fifty-two participants (mean age 30.03 ± 1.13 years; BMI 26.70 ± 0.46 kg/m²) underwent assessments at baseline, one week, and two weeks post-ordination. While total energy intake remained stable, macronutrient composition shifted significantly: protein decreased > 20%, sugar nearly doubled, and fiber increased substantially. Body composition improved with reductions in weight, BMI, waist and hip circumference. Muscle mass modestly decreased while body fat percentage and visceral fat remained stable. Sleep quality improved significantly, particularly sleep latency and subjective restfulness, despite unchanged efficiency. Findings suggest Buddhist ordination may produce beneficial short-term physiological adaptations similar to time-restricted eating. Though improvements in abdominal adiposity and sleep quality were observed, declining muscle mass highlights nutritional adequacy concerns. Monastic routines may provide culturally appropriate frameworks for structured lifestyle interventions.
Similar content being viewed by others


Introduction
Obesity poses a major global health burden, with prevalence steadily rising across diverse populations. Current estimates suggest that more than 650 million adults, approximately 13% of the global population, are classified as obese1. This condition is associated with increased risk of noncommunicable diseases such as type 2 diabetes, cardiovascular disorders, and certain cancers, while also diminishing quality of life and elevating healthcare costs2,3. The multifactorial nature of obesity, encompassing genetic, behavioral, and environmental contributors, demands multifaceted interventions that extend beyond traditional calorie focused approaches. This has prompted interest in lifestyle-based strategies, particularly those aligned with cultural and religious practices, as potentially sustainable models for metabolic health. Spiritual traditions, which emphasize mindfulness, intentional living, and self-discipline, may offer unique frameworks for influencing behavioral and physiological health outcomes.
Conventional strategies for managing obesity typically emphasize achieving a negative energy balance through increased physical activity and reduced caloric intake4. However, emerging evidence highlights the importance of the timing and frequency of food consumption as independent modulators of metabolic health5. Meal timing influences circadian rhythms, hormonal regulation, and energy homeostasis, thereby affecting body composition and disease risk6. In this context, time-restricted eating (TRE), which limits food intake to a defined window of 4 to 12 h per day without necessarily altering caloric content, has demonstrated promising health outcomes7. Clinical studies have reported improvements in insulin sensitivity, reductions in inflammation, and modest weight loss even in the absence of intentional calorie restriction8,9. Notably, short term TRE interventions (2 to 4 weeks) have been shown to induce rapid metabolic and anthropometric changes10,11. These findings support the potential of TRE as a simple yet powerful tool to synchronize metabolic processes with the body’s internal clock.
Buddhist monastic practices, particularly within the Dhammayut and Mahanikaya tradition which follow strict disciplinary codes, resemble time-restricted eating (TRE) while also promoting spiritual development through mindfulness, monastic discipline (Vinaya), and detachment from material desires. Both TRE and Buddhist monastic routines involve limiting caloric intake to a specific time window7,12. Monks typically consume two meals between dawn and noon, resulting in an 18- to 19-hour fasting period—closely aligned with modern TRE protocols12,13. Despite these similarities, several important differences distinguish monastic fasting from conventional TRE. Modern TRE generally permits only water during fasting periods, whereas Buddhist practices may allow herbal teas, clear fruit juices, or medicinal tonics such as honey or ghee14. Moreover, TRE is typically adopted as a voluntary health intervention, while monastic fasting is embedded within a religious framework and upheld through communal norms and doctrinal discipline7,15.
Interestingly, despite this TRE-like eating pattern, recent studies have reported high rates of obesity, metabolic syndrome, and type 2 diabetes among Thai monks15,16,17,18. Contributing factors include low levels of physical activity, extended sedentary behavior, and regular consumption of energy-dense foods received during alms rounds, which are often high in sugar and fat. This practice limits personal food selection and reduces dietary variability17,18,19. While TRE usually involves control over both meal timing and dietary quality, monastic routines restrict the timing of meals but not their nutritional content. These findings suggest that time restriction alone may be insufficient to reduce metabolic risks without concurrent improvements in diet quality and physical activity.
Nonetheless, the core principle of limiting caloric intake to a specific daily window aligns with TRE guidelines16. Moreover, while TRE in free-living populations relies on individual self-discipline, monastic fasting is enforced through religious commitment and institutional norms7,19, potentially enhancing adherence and long-term consistency. This structured environment creates a naturally compliant setting ideal for studying the physiological effects of lifestyle modifications.
In parallel with dietary changes, the healthy lifestyle of monks is defined by structured, spiritually guided routines that support physical, mental, and emotional well-being. Core components of this lifestyle include early morning barefoot alms rounds, temple cleaning, meditation, chanting, and the study of Buddhist scriptures14,15,17. These daily activities not only fulfill religious obligations but also promote physical movement, mindfulness, and stress reduction. For example, alms rounds involve prolonged barefoot walking, which increases daily energy expenditure and supports cardiovascular health20. Meditation and chanting, which are central to monastic practice, foster emotional regulation, reduce stress, and enhance psychological resilience, thereby reinforcing the healthy lifestyle of monks20,21. Collectively, these practices represent a culturally embedded model of health that integrates physical discipline with spiritual and community based well-being. In addition, the healthy lifestyle of monks involves adaptations in physical activity and sleep patterns. While routines such as alms rounds and temple maintenance contribute to moderate physical activity, the broader monastic lifestyle emphasizes meditative and ceremonial practices that are generally less physically demanding14,17. Nonetheless, the consistency and discipline of the monastic schedule may promote circadian alignment and improved restfulness over time, further supporting overall health and well-being.
Sleep patterns also undergo significant changes, with monks rising at 4:00 AM and concluding evening practices around 8:00 to 9:00 PM14. These structured schedules may initially disrupt circadian alignment and impact sleep quality during the adaptation phase19. However, over time, the regularity of the monastic schedule may promote circadian stability, contrasting with the irregular sleep–wake patterns common in modern lifestyles. Psychological studies suggest that structured spiritual routines, such as early rising for meditation and chanting, can improve mood and reduce stress22. The spiritual motivation underpinning ordination may also foster intrinsic commitment to behavioral change, supporting greater adherence and potentially amplifying health benefits. Taken together, these characteristics position Buddhist monasticism as a unique and culturally embedded model for studying the physiological impact of comprehensive lifestyle interventions.
Despite the conceptual parallels between monastic discipline and therapeutic fasting, there is a limited understanding of the physiological and spiritual adaptations that occur during the early phase of ordination. Newly ordained monks provide a unique opportunity to observe rapid health-related changes in a controlled lifestyle shift rooted in religious discipline. This population is ideal for investigating the short-term impacts of a highly structured routine involving dietary, physical, spiritual, and sleep modifications in a real-world yet regimented setting. This study aimed to examine the short-term effects of Buddhist ordination on dietary intake, body composition, and sleep quality among newly ordained Thai Dhammayut monks. We hypothesized that this spiritually structured lifestyle transition would lead to measurable improvements in body composition, dietary quality, and sleep parameters during the early adaptation phase.
Results
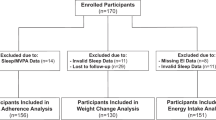
Seventy-four individuals were initially screened for eligibility (Fig. 1). Of these, eight were excluded before baseline assessment—five did not meet the inclusion criteria, and three declined participations. During the first week of ordination, five participants withdrew after relocating to other temples. Nine additional participants were excluded due to incomplete dietary records or questionnaires, and six could not be contacted at the two-week follow-up. All analyses presented in this study were conducted based on data obtained from these 52 participants.

Participant flow diagram. A total of 74 individuals were assessed for eligibility. After exclusions, 66 participants completed baseline and one-week assessments. Five withdrew before the two-week assessment, and nine were excluded from final analysis due to incomplete data or loss to follow-up, resulting in 52 participants included in the final analysis.
Baseline characteristics of the participants are presented in Table 1. All were male, newly ordained Dhammayut Buddhist monks with a mean age of 30.03 ± 1.13 years and a mean body mass index (BMI) of 26.70 ± 0.46 kg/m². The majority held a bachelor’s degree, and approximately 21% reported having at least one underlying health condition, such as hypertension, diabetes, or other chronic illnesses.
Changes in dietary intake
Table 2 illustrates the longitudinal changes in dietary parameters among Thai monks measured at baseline (pre-ordination) and during the subsequent two weeks post-ordination. Total energy intake, carbohydrate intake, and fat intake showed no statistically significant differences throughout the observation period (p > 0.05). However, significant alterations were observed in specific macronutrient composition. Protein intake decreased significantly from baseline (79.96 ± 9.85 g) to week 1 (60.90 ± 6.77 g; p = 0.009) and week 2 (62.50 ± 6.37 g; p = 0.005) post-ordination, representing 23.83% and 21.84% reductions, respectively. While protein intake declined significantly, a concurrent and substantial increase in sugar consumption was observed, reflecting a notable shift in the types of foods consumed during the ordination period, likely influenced by the nature of alms-based offerings. Sugar consumption exhibited a significant and substantial increase from baseline (34.60 ± 4.91 g) to week 1 (67.96 ± 11.60 g; p = 0.008) and week 2 (69.85 ± 9.46 g; p < 0.001), corresponding to 96.42% and 101.88% elevations, respectively. Dietary fiber intake demonstrated progressive enhancement, significant increase from baseline (5.07 ± 0.60 g) to week 1 (6.84 ± 0.77 g; p = 0.025) and week 2 (8.32 ± 0.76 g; p < 0.001), reflecting 34.91% and 64.10% increments, respectively. Analysis of variance revealed significant interaction effects between treatment and time (p < 0.05) for all three parameters exhibiting statistically significant changes (protein, sugar, and dietary fiber).
Body composition
The effects of ordination on body composition parameters in Thai monks is displayed in Table 3. The results demonstrated statistically significant reductions in several anthropometric parameters between baseline and two weeks post-ordination. Body weight significantly decreased by 0.69%, from 80.98 ± 1.69 kg at baseline to 80.42 ± 1.75 kg at week 2 (p < 0.001). Similarly, BMI declined by 0.86%, showed a significant reduction from 26.70 ± 0.46 kg/m² at baseline to 26.47 ± 0.48 kg/m² at week 2 (p < 0.001). The most notable anthropometric changes were observed in waist and hip circumferences, which significantly decreased by 4.88%, from 96.17 ± 1.43 cm at baseline to 91.47 ± 1.39 cm at week 2 (p < 0.001), while hip circumference reduced by 2.94%, from 101.98 ± 1.19 cm at baseline to 98.99 ± 1.12 cm at week 2 (p < 0.001). Consequently, waist to hip ratio demonstrated a significant decline of 2.13%, from 0.94 ± 0.01 at baseline to 0.92 ± 0.01 at week 2 (p = 0.008). Muscle mass also showed significant reduction of 1.75%, from 58.29 ± 0.87 at baseline to 57.27 ± 0.82 at week 2 (p = 0.01). In contrast, percentage of body fat exhibited a no significant increase from 23.51 ± 0.74% at baseline to 24.18 ± 0.65% at week 2 (p = 0.104), and visceral fat level remained relatively stable (11.20 ± 0.44 at baseline versus 11.06 ± 0.44 at week 2, p = 0.532).
Sleep quality
The effects of ordination on sleep quality parameters in Thai monks as assessed by the Pittsburgh Sleep Quality Index (PSQI), with scores greater than 5 generally indicating poor sleep quality23 (Table 4). Following 2 weeks of ordination, the global PSQI score showed a statistically significant reduced from 6.88 ± 0.41 at baseline to 6.10 ± 0.33 at week 2 (p = 0.046). Analysis of individual PSQI components revealed significant improvements in several parameters when compared between baseline and 2 weeks post-ordination. Overall subjective sleep quality significantly improved, with scores decreasing from 1.23 ± 0.09 at baseline to 0.96 ± 0.09 at week 2 (p = 0.029). Sleep latency showed the most notable improvement, significantly decreasing from 1.38 ± 0.13 to 0.90 ± 0.13 (p < 0.001). Sleep duration scores significant increase from 1.10 ± 0.12 at baseline to 1.42 ± 0.10 at week 2 (p = 0.023). No significant trends toward improvement were observed in sleep disturbances, which decreased from 1.31 ± 0.08 at baseline to 1.17 ± 0.07 at week 2 (p = 0.070). Sleep efficiency showed a no significant change from 0.52 ± 0.14 at baseline to 0.35 ± 0.09 at week 2 (p = 0.201), while use of sleeping medication remained unchanged (0.15 ± 0.07 at baseline versus 0.15 ± 0.08 at week 2, p = 1.000). Daytime dysfunction also shows no significant increase from 1.13 ± 0.10 at baseline to 1.15 ± 0.10 at week 2 (p = 0.881).
Discussion
Despite unchanged total energy, carbohydrate, and fat intake throughout the ordination period, meaningful shifts in macronutrient composition were observed (Table 2). Protein intake declined significantly in the first week and remained consistently lower in the second week, representing a reduction of over 20% from baseline. This decline is likely attributable to the traditional alms based dietary system, which tends to emphasize carbohydrate rich foods such as rice and sweets, while offering limited quantities of high-quality protein sources. Such dietary patterns align with previous studies on monastic food practices in Thailand21,24,25 and have been associated with nutritional imbalances contributing to high rates of obesity, diabetes, and other noncommunicable diseases (NCDs) among monks15. The structural reliance on food offerings, while culturally and religiously significant, may unintentionally promote a low protein, high carbohydrate dietary pattern, thereby increasing long term metabolic risk15.
Although reduced, average protein intake remained comparable to that of overweight Thai men and exceeded levels reported in Indian Buddhist monks17,26. Nevertheless, it fell short of the recommended intake (1.2 g/kg/day) required to preserve lean body mass during periods of restricted physical activity or intermittent fasting27, potentially contributing to the observed decline in muscle mass. In contrast, sugar intake nearly doubled by the second week, a trend consistent with prior findings of high sugar consumption among urban monks, often driven by sweetened beverages and desserts received through food offerings17,24. This observation parallels studies in Thai monks, where high glycemic diets and low physical activity were associated with insulin resistance and central adiposity18. While such intake may increase glycemic load and metabolic risk over time, this trend was accompanied by a significant increase in dietary fiber, possibly reflecting greater fruit and vegetable consumption. The nearly twofold increase in sugar intake during ordination is concerning, particularly given the associated risks of increased glycemic load and metabolic dysfunction over time. As monks are reliant on alms offerings and cannot selectively choose their foods, interventions at the community level such as encouraging healthier offerings including fruits, whole grains, and less processed sweets could represent a culturally sensitive strategy to mitigate this nutritional imbalance. Although fiber intake remained below recommended levels28, the observed upward trajectory parallels findings from time restricted eating interventions, where improvements in diet quality are often mediated by circadian alignment and reduced evening intake29.
Taken together, these findings highlight both the strengths and limitations of the alms based dietary model. The structured eating window imposed by Buddhist monastic practice aligns with core principles of time restricted eating and may naturally facilitate improvements in diet quality. However, imbalances such as insufficient protein and elevated sugar intake should be addressed if monastic dietary patterns are to serve as a practical model for promoting metabolic health. By the end of the two-week period, participants showed statistically significant reductions in body weight and BMI, with greater decreases in waist and hip circumferences. Although statistically significant, the short-term change in BMI may not yet be clinically impacted. Our results were consistent to previous study that body weight and BMI also slightly decrease (0.4 \(\:\pm\:\) 1.1 kg) after 2 weeks TRE among healthy young men30. In contrast, reductions in waist circumference, which are strongly associated with improvements in metabolic risk, may indicate early health benefits31. Waist circumference decreased by approximately 4.9% and hip circumference by 2.9%, contributing to an improved waist to hip ratio. These changes are particularly relevant to metabolic health, given the well-established association between central adiposity and cardiometabolic risk. A reduction in waist to hip ratio may be associated with a lower risk of myocardial infarction, as demonstrated in a recent meta-analysis32. Furthermore, previous evidence suggests that waist to hip ratio is a more reliable predictor of type 2 diabetes risk compared to body mass index (BMI), particularly in Asian populations where central adiposity is more strongly associated with metabolic complications33. Importantly, a reduction of approximately 5% in waist circumference is considered clinically meaningful, as increased waist circumference has been linked to greater cardiovascular disease specific mortality in dose response meta-analyses34. Thus, the observed improvements in central adiposity during ordination may not only represent early anthropometric changes but also signal potential longer-term benefits in reducing cardiometabolic and cardiovascular disease risks. Interestingly, no significant changes were observed in visceral fat levels or percent body fat. This may be due to the short duration of the study and the inherent limitations of bioelectrical impedance analysis in detecting small changes in adiposity over brief intervals35. Nevertheless, reductions in waist and hip circumference suggest early improvements in abdominal fat distribution.
A modest but statistically significant decline in muscle mass was also observed, likely resulting from the combination of reduced protein intake and decreased physical activity during the ordination period. Monastic routines involve periods of walking and chanting but are largely sedentary compared to preordination lifestyles14,17. The muscle loss observed, approximately 1.8%, raises concerns about nutritional adequacy and underscores the importance of ensuring sufficient protein intake, even during short-term fasting or lifestyle transitions. Although a modest decline in muscle mass was observed, it is important to note that short term muscle mass reductions may not have long term clinical implications if physical activity levels and nutritional intake are adequately restored following ordination. Future longitudinal studies are warranted to track the recovery of muscle mass and functional capacity after ordination, ensuring a comprehensive understanding of the health impacts of temporary lifestyle changes. These findings are consistent with previous time restricted eating trials reporting 1 to 3% reductions in body weight over periods ranging from 2 to 16 weeks36,37. Interpretation of muscle mass changes should be approached with caution, as bioelectrical impedance analysis (BIA) is sensitive to hydration status. Mild dehydration associated with fasting may lead to an underestimation of fat-free mass35. To minimize this potential bias, all measurements were conducted using the same device and at consistent times at both baseline and two weeks post-ordination. Our data suggest that the Buddhist ordination framework may offer a naturalistic and culturally grounded model of time restricted eating that produces measurable improvements in body composition, particularly in abdominal fat, even over a short period.
Contrary to expectations, a modest improvement in sleep quality was observed despite the adoption of a more demanding daily schedule; however, sleep quality remained below healthy thresholds. The global PSQI score decreased significantly, with the greatest improvements observed in sleep latency and subjective sleep quality. Participants reported falling asleep more quickly and feeling more rested, despite no significant changes in sleep efficiency. Several mechanisms may explain these improvements. The structured routine of monastic life promotes consistent sleep wake cycles, which has been shown to enhance circadian alignment and sleep quality38,39. Moreover, early morning light exposure during alms collection may strengthen circadian entrainment, thereby reducing sleep latency40. Although total sleep duration did not increase, the perceived improvement in restfulness suggests enhanced sleep quality, potentially reflecting more effective physiological recovery during sleep41.
These findings suggest a rapid physiological adaptation to the monastic lifestyle, in which regularity, reduced cognitive demands, and minimal exposure to digital and environmental disturbances may facilitate better sleep onset and subjective sleep quality39,42. The reduction in sleep latency may result from improved circadian regulation and decreased psychophysiological arousal, potentially influenced by mindfulness practices and a simplified daily routine43,44.
Emerging evidence also links time restricted eating to improved sleep regulation through metabolic pathways. Restricting food intake to early daytime hours may optimize circadian hormone secretion, which is critical for sleep initiation and maintenance6,45. The combined effect of time restricted eating patterns and structured daily routines may thus synergistically contribute to improvements in sleep health. Given the established association between sleep quality and weight regulation5,46,47, these results provide further support for the potential of Buddhist ordination to function as a culturally embedded lifestyle intervention with multidimensional health benefits. Beyond the structured routines of monastic life, the spiritual discipline inherent in Buddhist ordination, including practices such as mindfulness, reduced material attachment, and meditative focus, may have contributed to improved stress management and sleep quality. Spiritual motivations may foster greater emotional regulation, adherence to healthy behaviors, and resilience during the adaptation to new daily routines. These intrinsic factors could have synergistically enhanced the physiological benefits observed during the ordination period. However, this study did not assess caffeine consumption or perceived stress, both of which are established factors influencing sleep quality48,49. Incorporating these variables in future research would strengthen the validity and interpretability of sleep related findings.
Buddhist ordination may provide a culturally embedded model for metabolic health promotion through structured routines and time restricted eating. Short term ordination was associated with improvements in dietary composition, central adiposity, and sleep quality. These findings suggest that integrating spiritual practices into health interventions could enhance holistic outcomes. Monastic living, given its cultural acceptance and accessibility, offers valuable insights for developing structured interventions beyond monastic settings. By fostering physical, psychological, and spiritual well-being, Buddhist ordination presents a comprehensive framework for culturally grounded health promotion.
Methods
Study design
A prospective observational study was conducted between January and May 2024 at Wat Bowaniwet Wihan Ratchaworawihan, a Dhammayut Buddhist temple in Bangkok, Thailand. The study was designed to capture physiological changes during the early phase of ordination, a period characterized by substantial lifestyle transitions. Participants were assessed at three key time points: baseline (first day of ordination), after one week, and after two weeks (final week of ordination). At baseline, participants maintained their regular lifestyles, including their typical diet, sleep schedule, and physical activity patterns until ordination. During ordination, participants adopted monastic routines as dictated by Buddhist disciplinary codes, including pre-noon food consumption, increased sedentary activity (meditation and chanting), and structured sleep-wake schedules.
The duration of the study was set at two weeks, aligning with the minimum period of monastic ordination commonly practiced in Thai Buddhism. According to temple tradition, newly ordained monks must remain in the monastic order for at least two weeks before disrobing (“suek”). This provided a natural and culturally defined timeframe for data collection, ensuring that all participants were observed under consistent monastic conditions from ordination to the point of potential disrobing.
Importantly, participants were permitted to consume unrestricted quantities and types of food and beverages offered through alms during the eating window, reflecting real-world monastic practice. Researchers did not interfere with dietary choices to preserve ecological validity but provided telephone access for any study-related questions. The design aimed to evaluate how these organically structured routines affect dietary patterns, anthropometry, and sleep in a short timeframe.
In addition, the study protocol received approval from the Ethics Review Committee for Research Involving Human Research Subjects, Human Science Group, Chulalongkorn University (COA No. 013/67), adhering to the Declaration of Helsinki guidelines. Before enrollment, all participants provided written informed consent, and their information was maintained with strict confidentiality.
Sample size calculation
The sample size was determined based on the 0.05 level of significance (α), 80% power, effect size (0.44), using the BMI of obese men that enrolled in TRE protocol from the previous study50. Using this as the total population and considering an estimated drop-out rate of 30%, a target sample of at least 56 participants was set to ensure adequate statistical power to detect meaningful changes in dietary intake, body composition, and sleep parameters over time. A total of 52 participants completed the full study protocol.
Participants details
Fifty-two newly ordained Dhammayut Buddhist monks were recruited from Wat Bowaniwet Wihan Ratchaworawihan, Bangkok. Inclusion criteria were adults aged 20 years or older, with a BMI greater than 22.9 kg/m²51, willingness to undergo ordination for at least two weeks, fluency in Thai, and agreement to participate in the study. Exclusion criteria included early withdrawal from monkhood before the two-week period or incomplete data on questionnaires, dietary records, or body composition measurements.
Outcomes measurement
The primary outcome of the study was body weight, as a sensitive and direct marker of short-term physiological change. Secondary outcomes included other components of body composition, dietary intake, and sleep quality parameters such as sleep timing, duration, onset latency, efficiency, disturbances, use of sleep medications, and daytime functioning.
Dietary intake
At baseline, participants received standardized training from registered dietitians on how to accurately record food and beverage consumption. The training utilized visual aids, food models, and standard household measuring tools (e.g., cups, spoons, and bowls) to enhance portion size estimation and recording accuracy. Each participant was provided with a structured food recording handbook and was instructed to complete a 3-day dietary record each week, covering two weekdays and one weekend day.
In addition, a 24-hour dietary recall interview was conducted at baseline to capture dietary intake prior to ordination. This recall was administered by registered dietitian to ensure accuracy and minimize recall bias. All dietary records and recall data were reviewed for completeness and consistency before analysis. Moreover, any potential underreporting or overreporting of data was verified by contacting the participants directly to ensure accuracy. Nutrient intake—including total energy, macronutrients, dietary fiber, and sugar—was analyzed using the INMUCAL-Nutrients software (version 4.0), developed by the Institute of Nutrition, Mahidol University, Thailand, which is based on a validated Thai food composition database.
Body composition
Assessments were conducted in the early morning, prior to breakfast, at two time points: baseline (the day of ordination) and after two weeks of monastic life. Participants wore light clothing and removed any metallic items or accessories to minimize measurement variability. Body composition parameters, including body weight, body mass index (BMI), body fat percentage, visceral fat level, and muscle mass, were measured using a validated bioelectrical impedance analysis (BIA) device (TANITA BC-401, Tokyo, Japan).
Waist and hip circumferences were measured using a non-elastic measuring tape. Waist circumference was recorded at the midpoint between the lowest palpable rib and the superior border of the iliac crest, while hip circumference was measured at the widest point of the buttocks. To ensure consistency and cultural appropriateness, all anthropometric measurements were performed by trained male researchers, adhering to Buddhist monastic discipline52. The same equipment, measurement time, and standardized protocols were applied across both time points to minimize inter-rater and device variability.
Sleep quality
Sleep quality was assessed using the Thai version of the Pittsburgh Sleep Quality Index (PSQI)53, a validated and widely used instrument for evaluating subjective sleep characteristics. The PSQI was administered at two time points: baseline (pre-ordination) and at the end of the second week of ordination. The instrument includes 19 self-rated questions grouped into seven component scores: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications, and daytime dysfunction. Each component is scored from 0 to 3, with higher scores indicating greater impairment. These scores are summed to yield a global PSQI score ranging from 0 to 21. A global score greater than 5 is indicative of poor sleep quality. Sleep onset latency, one of the key subcomponents, was also specifically evaluated, with scores interpreted as follows: 0 = no difficulty falling asleep, 1 = mild difficulty, 2 = moderate difficulty, 3 = severe difficulty. Participants completed the questionnaire independently, with support provided by the research team when needed to ensure accuracy and completeness. All responses were reviewed for consistency immediately after collection.
Statistical analysis
Data were presented as mean ± standard error of the mean (SEM), while categorical variables such as education level and underlying disease were expressed as counts and percentages. Normality of distribution for key variables was tested using the Kolmogorov–Smirnov test. Paired samples t-tests were used to assess changes between time points. Repeated measures ANOVA was used to examine the effects of treatment, time, and interaction terms. A P-value < 0.05 was considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics (version 22.0; SPSS Inc., USA).
Strengths and limitations
This study is the first prospective investigation to assess short term physiological adaptations to Buddhist ordination, simultaneously evaluating changes in dietary intake, body composition, and sleep quality. The use of validated instruments, repeated measures, and a naturalistic monastic setting enhances both internal validity and real-world applicability. However, the limited observation period constrains the ability to generalize outcomes to longer term adaptations. Dietary intake was self-reported, which introduces the possibility of recall bias, although standardized protocols were used to mitigate this limitation. Waist circumference measurements were taken at non-standardized anatomical landmarks. In addition, physical activity was not assessed, and no biochemical or hormonal markers (e.g., glucose, cortisol) were collected, limiting the ability to interpret underlying metabolic changes.
The short duration of the study, coupled with the limited sensitivity of bioelectrical impedance analysis (BIA), may have restricted the detection of meaningful changes in visceral fat and muscle mass. Cultural context also imposes important constraints: monks rely on food offerings from laypeople during alms collection, thereby limiting their control over the nutritional quality and macronutrient composition of their diet. This structural dependence may contribute to the observed nutritional outcomes and should be taken into account when interpreting results and designing future interventions. Moreover, the study sample was limited to monks residing at Wat Bowonniwet Vihara, which may restrict the generalizability of the findings to other monastic communities. Future studies involving more diverse settings and longer follow-up periods are recommended to validate and expand upon these results.
Conclusion
This two-week study demonstrated that Buddhist ordination, as a natural model of time-restricted eating, led to significant improvements in dietary intake, body composition, and sleep quality. Reductions in protein intake and increases in sugar and fiber reflected shifts in alms based dietary patterns. Anthropometric measures improved, particularly in central adiposity, although muscle mass declined. Sleep quality also improved, especially in latency and subjective restfulness. These findings highlight the potential of short-term monastic practice as a culturally relevant framework for promoting holistic health.
Data availability
“The data presented in this study are available on reasonable request from the corresponding author.”
References
World Health Organization. WHO Acceleration Plan To Stop Obesity (World Health Organization, 2023).
Tremmel, M., Gerdtham, U. G., Nilsson, P. M. & Saha, S. Economic burden of obesity: A systematic literature review. Int. J. Environ. Res. Public. Health. 14, 435 (2017).
Blüher, M. & Obesity Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 15, 288–298 (2019).
Hill, J. O., Wyatt, H. R. & Peters, J. C. Energy balance and obesity. Circulation 126, 126–132 (2012).
Paoli, A., Tinsley, G., Bianco, A. & Moro, T. The influence of meal frequency and timing on health in humans: The role of fasting. Nutrients 11, 719 (2019).
Chaix, A., Manoogian, E. N. C., Melkani, G. C. & Panda, S. Time-restricted eating to prevent and manage chronic metabolic diseases. Annu. Rev. Nutr. 39, 291–315 (2019).
Li, Z., Heber, D., Li, Z. & Wan, J. Effects and possible mechanisms of intermittent fasting on health and disease: A narrative review. Nutr. Rev. 81, 1626–1635 (2023).
Sutton, E. F. et al. Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell. Metab. 27, 1212–1221e3 (2018).
Wilkinson, M. J. et al. Ten-hour time-restricted eating reduces weight, blood pressure, and atherogenic lipids in patients with metabolic syndrome. Cell. Metab. 31, 92–104e5 (2020).
Cienfuegos, S. et al. Effects of 4-and 6-h time-restricted feeding on weight and cardiometabolic health: A randomized controlled trial in adults with obesity. Cell. Metab. 32, 366–378e3 (2020).
Martens, C. R. et al. Short-term time-restricted feeding is safe and feasible in non-obese healthy midlife and older adults. Geroscience 42, 667–686 (2020).
Petersen, M. C. et al. Complex physiology and clinical implications of time-restricted eating. Physiol. Rev. 102, 1991–2034 (2022).
Tiyavanich, K. Forest Recollections: Wandering Monks in Twentieth-Century Thailand (University of Hawai’i Press Honolulu, 1997).
Sirivongs, P., Laisakul, K., Sriwilai, P., Kantachuvessiri, A. & Vathesatogkit, P. General health status of Thai monks living in Bangkok metropolitan temples. J Med. Assoc. Thai 102 (2019).
Jeamjitvibool, T., Arphorn, S., Chiawiriyabunya, I. & Taneepanichskul, S. Noncommunicable diseases and social determinants of health in Buddhist monks: An integrative review. Res. Nurs. Health. 45, 249–260 (2022).
Rothschild, J. et al. Time-restricted feeding and risk of metabolic disease: A review of human and animal studies. Nutr. Rev. 72, 308–318 (2014).
Chidambaram, M. R. & Asha, G. Assessment of lifestyle and health status of Buddhist monks. Int. J. Health Sci. Res. 10, 2249–9571 (2020).
Sirimongkon, P., Boonchieng, W. & Wungrath, J. A qualitative exploration of diet-related noncommunicable diseases from the perspectives of Thai Buddhist monks in Chiang Mai province, Thailand. J. Popul. Soc. Stud. 33, 844–858 (2025).
St-Onge, M. P. et al. Sleep and meal timing influence food intake and its hormonal regulation in healthy adults with overweight/obesity. Eur. J. Clin. Nutr. 72, 76–82 (2019).
Panyachit, S. Barefoot health: the healthy lifestyle path of monks in Thailand. J. Popul. Soc. Stud. 33, 343–361 (2025).
Srimantayamas, V., Promkhatkaew, C., Supavititpatana, B. & Jittanoon, P. Health behaviors and health-related quality of life among Buddhist monks with metabolic syndrome. Pac. Rim Int. J. Nurs. Res. 24, 159–171 (2020).
Garland, E. L. et al. Mindfulness training promotes upward spirals of positive affect and cognition: Multilevel and autoregressive latent trajectory modeling analyses. Front. Psychol. 6, 15 (2015).
Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R. & Kupfer, D. J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 28, 193–213 (1989).
Kamkokgruad, T., Chatthongpisut, R. & Intajarurnsan, S. Nutritional value of popular foods offered to monks by Thai Buddhists. Asian Health Sci. Technol. Rep. 27, 32–43 (2019).
Ko-amornsup, W. et al. Health survey of monks residing in urban areas: the Bangkok Noi model. Siriraj Med. J. 76, 746–757 (2024).
Ivanovitch, K., Klaewkla, J., Chongsuwat, R., Viwatwongkasem, C. & Kitvorapat, W. The intake of energy and selected nutrients by Thai urban sedentary workers: An evaluation of adherence to dietary recommendations. J. Nutr. Metab. 2014 145182 (2014).
Pasiakos, S. M., Margolis, L. M. & Orr, J. S. Optimized dietary strategies to protect skeletal muscle mass during periods of unavoidable energy deficit. FASEB J. 29, 1136–1142 (2015).
Stephen, A. M. et al. Dietary fibre in europe: current state of knowledge on definitions, sources, recommendations, intakes and relationships to health. Nutr. Res. Rev. 30, 149–190 (2017).
Mengi Çelik, Ö., Köksal, E. & Aktürk, M. Time-restricted eating (16/8) and energy-restricted diet: effects on diet quality, body composition and biochemical parameters in healthy overweight females. BMC Nutr. 9, 97 (2023).
LeCheminant, J. D., Christenson, E., Bailey, B. W. & Tucker, L. A. Restricting night-time eating reduces daily energy intake in healthy young men: A short-term cross-over study. Br. J. Nutr. 110, 2108–2113 (2013).
Rothberg, A. E. et al. Impact of weight loss on waist circumference and the components of the metabolic syndrome. BMJ Open. Diabetes Res. Care. 5, e000341 (2017).
Cao, Q., Yu, S., Wang, Y., Xu, D. & Zhang, M. Waist-hip ratio as a predictor of myocardial infarction risk: A systematic review and meta-analysis. Medicine 97, e11639 (2018).
Cheng, C. H. et al. Waist-to-hip ratio is a better anthropometric index than body mass index for predicting the risk of type 2 diabetes in Taiwanese population. Nutr. Res. 30, 585–593 (2010).
Wang, L. et al. Associations of obesity indices change with cardiovascular outcomes: A dose-response meta-analysis. Int. J. Obes. 48, 635–645 (2024).
Sergi, G., Lupoli, L., Bussolotto, M., Perini, P. & Coin, A. Measurement of lean body mass using bioelectrical impedance analysis: A consideration of the pros and cons. Aging Clin. Exp. Res. 29, 591–597 (2017).
Hutchison, A. T. et al. Time-restricted feeding improves glucose tolerance in men at risk for type 2 diabetes: A randomized crossover trial. Obesity 27, 724–732 (2019).
Nematy, M. et al. Effects of ramadan fasting on cardiovascular risk factors: A prospective observational study. Nutr. J. 11, 69 (2012).
Cappuccio, F., Miller, M. A. & Lockley, S. W. Sleep, Health, and Society: from Aetiology To Public Health (Oxford University Press, 2010).
Phillips, A. J. et al. Irregular sleep/wake patterns are associated with poorer academic performance and delayed circadian and sleep/wake timing. Sci. Rep. 7, 3216 (2017).
He, M., Cao, R., Liu, X., Xie, Z. & Chen, J. Shine light on sleep: Morning bright light improves nocturnal sleep and next morning alertness among college students. J. Sleep. Res. 32, e13724 (2023).
Baron, K. G., Reid, K. J., Kern, A. S. & Zee, P. C. Role of sleep timing in caloric intake and BMI. Obesity 19, 1374–1381 (2011).
Han, X., Zhou, E. & Liu, D. Electronic media use and sleep quality: Updated systematic review and meta-analysis. J. Med. Internet Res. 26, e48356 (2024).
Li, Y., Tang, J. & Chen, G. The effect of meditation-based mind-body interventions on older adults with poor sleep quality: A meta-analysis of randomized controlled trials. Behav. Sleep. Med. 23, 341–359 (2025).
Valck, E. D., Cluydts, R. & Pirrera, S. Effect of cognitive arousal on sleep latency, somatic and cortical arousal following partial sleep deprivation. J. Sleep. Res. 13, 295–304 (2004).
Charlot, A. et al. Beneficial effects of early time-restricted feeding on metabolic diseases: Importance of aligning food habits with the circadian clock. Nutrients 13, 1405 (2021).
Knowlden, A. P., Hackman, C. L., Sharma, M., Julka, D. & Watson, J. C. The relationship between sleep quantity, sleep quality and weight loss in adults: A scoping review. Clin. Obes. 14, e12634 (2024).
Leger, D., Bayon, V. & de Sanctis, A. The role of sleep in the regulation of body weight. Mol. Cell. Endocrinol. 418, 101–107 (2015).
Clark, I. & Landolt, H. P. Coffee, caffeine, and sleep: A systematic review of epidemiological studies and randomized controlled trials. Sleep. Med. Rev. 31, 70–78 (2017).
Kalmbach, D. A., Anderson, J. R. & Drake, C. L. The impact of stress on sleep: Pathogenic sleep reactivity as a vulnerability to insomnia and circadian disorders. J. Sleep. Res. 27, e12710 (2018).
Ünalacak, M. et al. Effects of ramadan fasting on biochemical and hematological parameters and cytokines in healthy and obese individuals. Metab. Syndr. Relat. Disord. 9, 157–161 (2011).
Weir, C. B. & Jan, A. BMI Classification Percentile and Cut off Points. (StatPearls Publishing, 2019).
Khantipālo, B. The Buddhist Monk’s Discipline. Some Points Explained for Laypeople (Buddhist Publication Society, 2008).
Sitasuwan, T., Chokchai, S., Ruangsuk, W., Phanasathit, W. & Sirijindarat, N. Reliability and validity of the Thai version of the Pittsburgh sleep quality index. J. Med. Assoc. Thai. 97, S57–S67 (2014).
Acknowledgements
The authors are grateful to all participants for their time. This project is funded by National Research Council of Thailand (NRCT): N42A680622 and the Faculty of Allied Health Sciences Endowment Fund Chulalongkorn University.
Author information
Authors and Affiliations
Contributions
P.S. contributed to conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, visualization, and writing—both original draft preparation and review/editing. P.R. contributed to conceptualization, project administration, investigation, and resources. C.C. contributed to methodology, investigation, resources, and reviewing/editing. T.K. and K.K. participated in investigation, resources, and reviewing/editing. S.A. contributed to conceptualization, methodology, project administration, funding acquisition, and reviewing/editing. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical declarations
The study protocol was approved by the office of Ethics Review Committee for Research Involving Human Research Subjects, Human Science Group, Chulalongkorn University (COA No. 013/67) in accordance with the Declaration of Helsinki.
Consent to participate
All participants provided written informed consent before enrolling in the study, and all participant information was kept confidential.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Moosan, P.C., Suklaew, P.O., Chusak, C. et al. Buddhist ordination as a culturally embedded model for improving diet, body composition, and sleep quality in overweight and obese adults. Sci Rep 15, 25353 (2025). https://doi.org/10.1038/s41598-025-11309-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-11309-y
Keywords
This article is cited by
-
Knowledge and determinants of plant-based diet adoption among healthcare providers in a Buddhist teaching hospital: a cross-sectional study
Journal of Health, Population and Nutrition (2026)
