
Abstract
There are few tools support postmastectomy radiotherapy (PMRT) decisions for triple-negative breast cancer (TNBC) patients. This study aimed to develop a whole slide image (WSI)-based risk score to identify PMRT beneficiaries. We analyzed 608 TNBC patients treated at West China Hospital, Sichuan University (WCH) and 182 patients from The Cancer Genome Atlas (TCGA), diagnosed between 2011 and 2019. Utilizing features extracted from hematoxylin and eosin-stained WSI and clinicopathological characteristics, an image score and a clinicopathological score for each patient were computed via eXtreme Gradient Boosting, combined into a comprehensive risk score. Multivariate Cox proportional hazards regression analyses revealed a higher image score strongly associated with worse 5-year invasive disease-free survival (iDFS) (HR = 8.80, P < 0.001), overall survival (OS) (HR = 9.02, P < 0.001), and locoregional recurrence-free survival (LRFS) (HR = 8.39, P = 0.003). The integrated risk score outperformed clinicopathological score in prognostic accuracy, as evidenced by the area under the curve (WCH validation cohort, iDFS: 0.805 vs. 0.756; OS: 0.874 vs. 0.807; LRFS: 0.957 vs. 0.870; TCGA cohort, iDFS: 0.683 vs. 0.598; OS: 0.685 vs. 0.617). Importantly, PMRT significantly improved OS in “high-risk” patients identified by the risk score, but not in “low-risk” patients in both WCH and TCGA cohorts. These findings suggest that the WSI-based risk score shows promise as a tool for prognostic assessment and guiding PMRT decision-making in TNBC patients.
Similar content being viewed by others


Introduction
Triple-negative breast cancer (TNBC) is a heterogeneous disease characterized by the absence of estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2, accounting for 15–20% of all breast cancer cases1,2. Compared to other subtypes, TNBC is associated with an earlier age of onset, larger tumor size, higher recurrence rate, and more aggressive biology, resulting in a poorer prognosis2,3. The lack of endocrine and targeted therapies makes reducing recurrence and metastasis risk an urgent challenge for oncologists. Postmastectomy radiotherapy (PMRT) is a key treatment strategy for TNBC patients, as it improves locoregional recurrence-free survival (LRFS) and overall survival (OS)4,5.
In general, PMRT is recommended for breast cancer patients with ≥ 4 involved axillary lymph nodes (N2–3) or tumor size > 5 cm (T3–4)6. However, the role of PMRT in TNBC patients specifically has not been thoroughly evaluated7,8. Furthermore, PMRT is linked with adverse effects, including financial burden and long-term toxicities9, highlighting the need for more precise methods to identify TNBC patients who would benefit from PMRT.
Previous studies have demonstrated associations between eligibility for PMRT and advanced T/N stage, younger age, estrogen receptor-negative, and lymphovascular invasion (LVI)10,11. Our team has also reported that these clinicopathological risk factors can aid in personalizing PMRT decisions for breast cancer patients12,13. Meanwhile, hematoxylin and eosin (H&E)-stained whole slide images (WSIs) are widely used for predicting patient prognosis14,15, and there is growing interest in using deep learning models based on WSIs to predict radiotherapy response16,17. This suggests that histopathological characteristics derived from WSIs could provide valuable insights into PMRT outcomes and prognosis.
In this study, we aimed to employ machine learning to extract prognostic features from H&E-stained WSIs and combine them with key clinicopathological parameters to calculate a risk score. This risk score is designed to support PMRT decision-making for TNBC patients.
Materials and methods
Study population
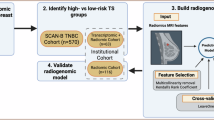
Patients diagnosed with TNBC between March 2011 and May 2019 were recruited from the Breast Cancer Information Management System18,19,20 at West China Hospital, Sichuan University (WCH), and The Cancer Genome Atlas (TCGA) database. Inclusion criteria for the WCH cohort were as follows: (a) TNBC diagnosis with unilateral cancer; (b) no distant metastasis confirmed by imaging and pathological examination before treatment; (c) availability of at least one H&E-stained formalin-fixed paraffin embedded tissue section WSI. For patients undergoing neoadjuvant therapy, biopsy WSIs were used. The patient selection flowchart for each experiment is presented in Fig. 1a. Non-neoadjuvant TNBC patients from TCGA with WSIs and information on age, T/N stage (AJCC 8th ), surgical procedure, and PMRT were included for external validation of prognostic and PMRT decision-making models.

The patient selection process and schematic diagram of experimental design. (a) The flow chart of the patient selection process. (b) The schematic diagram of experimental design (created by BioRender.com). WSIs were divided into small tiles for energy analysis firstly. High-energy tiles were retained for further tumor cell segmentation and cell features quantification. Thus, the image score was calculated by a XGBoost model using important features selected by Cox regression analysis. Similar methods were applied to the clinicopathological score (containing age, T stage, N stage) and the risk score (containing the image score and age, T stage, N stage). Finally, patients were divided into “high-risk” and “low-risk” groups according to the risk score, and these patients could or could not benefit from PMRT. (c) The top 80 high energy value tiles (top) and the low energy value tiles (bottom) calculated using Sobel filter. Scale bar: 100 μm. Mask-RCNN, the mask region convolutional neural network; PMRT postmastectomy radiotherapy.
Ethics approval and consent to participate
This study was conducted following the Declaration of Helsinki and was approved by the Ethics Committee of West China Hospital, Sichuan University (No. 1308 in 2022), and a waiver of informed consent was granted.
Follow-up and outcomes
The follow-up duration ranged from 3 to 218 months. The endpoints included 5-year invasive disease-free survival (iDFS), OS and LRFS. Event definitions follow previously published article21. Notably, LRFS data were unavailable for TCGA cohort. All time-to-event endpoints were defined as the time in months from the date of pathology diagnosis.
Data partition
Three sets of eXtreme Gradient Boosting (XGBoost) experiments were conducted: (1) extracting WSI features to calculate the image score, (2) calculating the clinicopathological score using clinicopathological prognostic factors, and (3) combining the image score and prognostic factors to compute the risk score for prognostic prediction and PMRT benefit-risk stratification. The WCH dataset was randomly divided into training and validation cohorts at a ratio of 6:4, ensuring tiles from the same patient remained in the same cohort. TCGA dataset was used as the test cohort. Data partition was shown in Supplementary Fig. S1a&b.
WSI feature extraction, the image score and clinicopathological score calculation
The study framework is depicted in Fig. 1b. Initially, WSIs were segmented into 2000 × 2000-pixel tiles using Python’s Openslide package. Energy values for each tile were calculated using an efficient implementation of Sobel filter22, with high-energy tiles (enriched in tumor cells; Fig. 1c) confirmed by pathologists used for tumor cell segmentation via a mask region convolutional neural network23. From 126 tumor cell features, statistical metrics (mean, median, variance, maximum, minimum, quartile, and standard deviation) were calculated through the skimage (scikit-image) image processing library24, generating 882 variables. Following univariate Cox regression, 255 variables (P < 0.01) were retained for subsequent steps to enhance robustness and minimize overfitting. In this step, we introduced the False Discovery Rate (FDR) to assess the reliability of univariate Cox regression analysis. These variables, along with tumor cell count and energy value, were used as input data, and information on events and timing of invasive recurrence within 5 years were used as the outcome label to establish the XGBoost model and output the image score (XGBoost model 1; see the following function). The XGBoost model was selected since it has been shown to be effective in predicting disease risk25. Image score at the patient level was determined by the median score of each tile of the patient.
Where xi represent the independent variables, and ft(xi) is each tree output function. A similar methodology was employed for generating each patient’s clinicopathological score (XGBoost model 2). During the implementation of the XGBoost model, important parameters (Supplementary Methods; Supplementary Table S1) were adjusted using Grid Search26 to optimize its performance. Further details regarding this algorithm can be found in our previously published article27.
The risk score calculation and PMRT benefit-risk stratification
The risk score (XGBoost model 3; Fig. 1b) was computed by integrating the image score with clinicopathological prognostic factors, using 5-year iDFS as the outcome. Patients with unknown T/N stage or those undergoing breast-conserving surgery (BCS) were not included in this experiment (Fig. 1a). The optimal risk score cutoff was determined using the Youden index from survival receiver operating characteristic (ROC) curves in R. The cutoff aimed to satisfy two criteria simultaneously: (1) PMRT significantly improved outcomes in the “high-risk” group, with a smaller P value indicating stronger significance; and (2) no significant outcome differences between PMRT and non-PMRT groups in the “low-risk” cohort, with the P value being as large as possible. Specifically, time-dependent ROC curves were constructed to guide the design of a composite scoring function that simultaneously satisfied dual statistical significance thresholds (p-values). Candidate cut-offs were iteratively evaluated by stratifying patients into high- and low-risk groups, followed by survival analysis comparing PMRT-treated versus untreated subgroups. The final cut-off was selected through a comprehensive search across all candidate thresholds to optimize stratification robustness and clinical interpretability.
Statistical analysis
Clinicopathological variables analyzed included age, menopausal status, tumor grade, T/N stage, Ki-67 index, LVI, and treatment details. Cox proportional hazards regression and Kaplan–Meier analyses were performed to evaluate survival outcomes. XGBoost-based Shapley’s additive explanation (SHAP; XGBoost model 4) was used to assess variable importance28. We performed Cox regression analysis in R 4.1.2, Chi-square test or Fisher’s test for characteristics and Kaplan‒Meier analysis in GraphPad Prism 8.0.2, and SHAP plotting in Python 3.7.12, with P < 0.05 considered statistically significant.
Results
Baseline characteristics
Table 1 summarizes the detailed characteristics of the study participants. The preliminary analysis included 608 TNBC patients from the WCH cohort, with a median age of 48 years (range: 23–81). Among these, 212 patients (34.87%) received PMRT, 103 patients (16.94%) received neoadjuvant chemotherapy (NACT), 601 patients (98.85%) received adjuvant chemotherapy (ACT), and 54 patients (8.88%) underwent BCS. The chemotherapy regimens of patients receiving PMRT and those not receiving PMRT (no-PMRT) are shown in Supplementary Table S2. Before 2020, most patients received two-dimensional technique radiotherapy, while a significant number of patients received intensity-modulated radiotherapy after 2020. PMRT administration was negotiated by the physician and the patient, adhering to the guidelines of the Chinese Society of Clinical Oncology (CSCO) and the European SocieTy for Radiation Oncology (ESTRO). The prescribed dose was 46–50 Gy in 25 fractions, targeting the ipsilateral chest wall as well as the supraclavicular and infraclavicular regions. In the independent test cohort, 182 TNBC patients from TCGA were included, with a median age of 55 years (range: 27–90). In this cohort, 92 patients (50.55%) received PMRT, 74 patients (40.66%) received ACT, and 49 patients (26.92%) underwent BCS. Each patient contributed 1–7 H&E-stained WSIs, resulting in 1,417 WSIs and 25,187 tiles used in the analysis. Supplementary Tables S3 and S4 present the detailed characteristics of PMRT and no-PMRT patients in the WCH cohort and TCGA cohort, respectively.
The image score emerges as a negative prognostic predictor for TNBC patients
During a mean follow-up period of 84.2 (range: 3–218) months, 95 patients (15.63%) experienced invasive recurrence, 21 patients (3.45%) experienced locoregional recurrence, and 67 patients (11.02%) died within 5 years. Univariate Cox analysis identified advanced T stage, N stage, and NACT as significant predictors of invasive recurrence [T2–4 vs. T1: hazard ratio (HR) = 1.88, 95% confidence interval (CI) 1.27–2.78, P = 0.002; N1–3 vs. N0: HR = 2.36, 95% CI 1.72–3.24, P < 0.001; NACT: HR = 2.39, 95% CI 1.54–3.72, P < 0.001] and mortality (T2–4 vs. T1: HR = 2.07, 95% CI 1.25–3.42, P = 0.004; N1–3 vs. N0: HR = 3.00, 95% CI 1.99–4.52, P < 0.001; NACT: HR = 3.50, 95% CI 2.13–5.76, P < 0.001) within 5 years (Table 2). Meanwhile, the image score demonstrated a strong correlation with poor outcomes in both the WCH validation cohort (iDFS: HR = 8.39, 95% CI 3.70–19.04, P < 0.001; OS: HR = 9.60, 95% CI 3.73–24.66, P < 0.001; LRFS: HR = 5.78, 95% CI 1.31–25.54, P = 0.021) and TCGA test cohort (iDFS: HR = 3.32, 95% CI 1.59–6.92, P = 0.001; OS: HR = 2.86, 95% CI 1.16–7.05, P = 0.022) (Fig. 2a).

The image score for prognosis analysis. (a) The results of the relationship between the image score and survival analyzed by univariate Cox regression. Relative importance of variables according to SHAP for 5-year OS (b, c), LRFS (d, e), and iDFS (f, g). PMRT postmastectomy radiotherapy, LVI lymphovascular invasion, SHAP Shapley’s Additive Explanation.
Although age showed no significant correlation with survival, it was included in the multivariable Cox analysis alongside T stage, N stage, NACT, and the image score because it is often of concern to clinicians (Table 3). Multivariable analysis confirmed the image score as an independent predictor of poorer iDFS (HR = 8.80, 95% CI 4.85–15.96, P < 0.001), OS (HR = 9.02, 95% CI 4.24–19.17, P < 0.001), and LRFS (HR = 8.39, 95% CI 1.96–35.97, P = 0.004). In addition, the SHAP diagrams in Fig. 2b–g indicated that the image score held the highest predictive importance, followed by N stage and other clinicopathological variables.
Further employing SHAP analysis to visualize the contributions of clinicopathological features to the image score revealed that age, T-stage, and N-stage were the most influential features (Supplementary Fig. S2). Patients with advanced N-stage exhibited significantly higher image scores (Supplementary Fig. S3). Visual comparison of WSI tiles corresponding to the highest- and lowest-scoring cases showed that tiles with high image score exhibited a greater degree of nuclear atypia, increased mitotic figures, and larger, more prominent perinuclear halos. In contrast, tiles with low image score displayed more uniform nuclear morphology (Supplementary Fig. S4).
The risk score outperforms the clinicopathological score in prognostic prediction
To evaluate whether WSI features improve prognostic prediction ability, the predictive performance of the clinicopathological score (comprising age, T stage, and N stage) and the risk score was compared using area under the ROC curve (AUC), as shown in Fig. 3. The risk score consistently outperformed the clinicopathological score in both the WCH validation cohort (OS: 0.874 vs. 0.807; LRFS: 0.957 vs. 0.870; iDFS: 0.805 vs. 0.756) and TCGA test cohort (OS: 0.685 vs. 0.617; iDFS: 0.683 vs. 0.589). Additionally, the image score also showed slightly higher predictive accuracy than the clinicopathological score (Fig. 3a–e).

Comparison of the performance of the image score, clinicopathological score, and risk score in predicting survival. The ROC curves for predicting 5-year OS (a), LRFS (b), iDFS (c) of the WCH validation cohort (n = 209) and 5-year OS (d), iDFS (e) of TCGA test cohort (n = 182). AUC area under the curve.
Identifying PMRT candidates according to the risk score
In view of the toxicity of PMRT and its variable efficacy among patients, we sought to utilize the risk score to identify those most likely to benefit from this treatment. Due to the limited number of T1–2N0 patients receiving PMRT (7/281), we performed a 1:1 exact matching based on T stage, N stage, and age, ultimately including 14 T1–2N0 patients (Fig. 1a). This resulted 254 patients from the WCH cohort being enrolled in the PMRT benefit-risk stratification experiment (Supplementary Fig. S1c). As a result, patients were stratified into “high-risk”(n = 169) and “low-risk” (n = 85) groups based on an optimal risk score cutoff of 0.611 (range: 0.222–2.328). Kaplan‒Meier analysis revealed that PMRT significantly improved OS (P = 0.011) and LRFS (P = 0.015) in the “high-risk” group but provided no significant benefits in the “low-risk” group (OS: P = 0.343; LRFS: P = 0.779) (Fig. 4a–d). Similar findings were observed in the TCGA cohort for OS, comprising 133 patients after excluding those treated with BCS (Fig. 4e&f). Although “high-risk” patients in the WCH cohort demonstrated improved iDFS with PMRT (P = 0.002), the TCGA cohort only showed a trend towards improvement (P = 0.088; Supplementary Fig. S5).This aligns with prior findings that PMRT predominantly improves local control and OS29,30.

Kaplan‒Meier survival curves of 5-year OS and LRFS in the PMRT and no-PMRT groups. 5-year OS of the “high-risk” (a) and “low-risk” (b) patients in the WCH cohort. 5-year LRFS of the “high-risk” (c) and “low-risk” (d) patients in the WCH cohort. 5-year OS of the “high-risk” (e) and “low-risk” (f) patients in TCGA cohort. PMRT, postmastectomy radiotherapy; no-PMRT, did not receive postmastectomy radiotherapy. The P-value determined by log-rank test.
Discussion
As we known, histopathology has always been the gold standard of disease diagnosis, with tumor cellular characteristics closely linked to tumor biology. In this study, we extracted features and computed image scores from H&E-stained WSIs of 608 TNBC patients from WCH cohort and 182 TNBC patients from TCGA. This image score emerged as an independent predictor of 5-year OS, LRFS, and iDFS. More importantly, the risk score, which integrates the image score with clinicopathological factors, demonstrated superior performance in predicting prognosis compared to traditional characteristics. It also successfully identified “high-risk” individuals s likely to benefit from PMRT, underscoring its potential utility in guiding treatment decisions.
Compared with traditional pathological characteristics, WSIs of cancerous tissues have surfaced as a new crucial resource for clinical diagnosis, treatment response assessment, and prognosis prediction31. By leveraging the pattern discernment capabilities of machine learning algorithms and voluminous, multiscale information inherent in WSIs, our team has previously demonstrated the utility of these features for prognosis prediction and validated their performance on publicly available datasets, including the National Lung Screening Trial32, breast cancer, and low-grade glioma datasets from TCGA33,34. Moreover, WSI features have also shown robust prognostic prediction potential across a variety of diseases, including hepatocellular carcinoma35, bladder cancer36, cervical cancer37, and diabetic kidney disease38.
In the present study, the image score outperformed N/T stage and NACT as a prognostic predictor. This superiority may be attributed to the comprehensive information encapsulated in WSIs, such as details on cell mitosis39, tumor-stromal ratio40, tumor grade41, and even gene expression42. In addition, our proposed risk score surpassed a recently reported model combining clinicopathological features and WSI data to predict recurrence (local, regional, and distant) and death in TNBC patients, achieving an optimal AUC of 0.7743. Thus, the risk score we developed serves as a reliable tool for identifying TNBC patients who may benefit from PMRT, offering personalized treatment options.
It is worth mentioning that the role of the 21-gene OncotypeDX recurrence score in decision-making on PMRT has attracted much attention44,45. However, it is specifically designed for estrogen receptor-positive breast cancer patients. For TNBC and other subtypes, our previous studies emphasized the importance of clinicopathological risk factors in PMRT benefit stratification12,13. Consistent with these findings, this study reaffirmed the predictive value of tumor size and lymph node involvement in TNBC patients. Notably, our results align with previous studies of similar design46,47,48. Wang et al.46. analyzed 1,474 postmastectomy T1–2N1 patients, and identified age ≤ 40 years, histological grade 3, 2–3 positive lymph nodes, and T2 stage (> 3 cm) as independent predictors of poor locoregional control. Xu et al.48. also proposed that age ≤ 40 years, 3 positive lymph nodes, T2 stage and Ki-67 index > 20% were independent risk factors for predicting breast cancer specific survival in T1–2N0–1 postmastectomy patients. These studies further suggested that patients with ≥ 2 risk factors might benefit from PMRT46,48. Our investigation found that 90.17% (211/234) of “high-risk” TNBC patients, as classified by the risk score, had ≥ 2 risk factors in age ≤ 40 years, T2–4 stage and > 1 positive lymph node. In contrast, 68.63% (105/153) of “low-risk” patients had ≤ 1 risk factor. These findings highlight the potential of WSI-based risk score to enable precise and personalized PMRT decision-making.
This study inevitably has some limitations. The independent TCGA cohort lacked LRFS data, and the models were trained using data from a single center, which may limit generalizability. To address this issue, we will continue collecting samples prospectively for validation. Data heterogeneity modestly impacts model performance. First, features extracted from biopsy WSIs exhibit lower representational capacity than the global patterns observable in surgical resection specimens. Second, while patient data across diagnostic/treatment years were randomly distributed in training/validation sets, evolving radiotherapy regimens may introduce subtle confounding effects. Future validation should employ standardized samples and contemporary radiotherapy guidelines to enhance scenario-specific utility.
Despite these constraints, our work provides innovative prognostic tools and valuable insights for PMRT application in TNBC patients. Additionally, this model leverages existing patient-specific digital H&E-stained postoperative pathology slides and electronic medical record (EMR)-derived age and T/N stage data through a fully automated pipeline. Upon finalization of the pathology report, artificial intelligence analysis is triggered, generating real-time risk scores that are either embedded within the pathology report or directly transmitted to the multidisciplinary team platform. The model enables analysis within routine clinical timeframes at near-zero marginal cost and integrates seamlessly with existing workflows.
Conclusions
Compared to traditional clinicopathological parameters, the WSI-based risk score demonstrated improved prognostic prediction performance. Following further validation, it holds promise as a tool for precisely identifying TNBC patients suitable for PMRT, thereby facilitating the development of more targeted and effective treatment strategies.
Data availability
Research data are stored in an institutional repository and will be shared upon reasonable request from the corresponding author.
Abbreviations
- TNBC:
-
Triple-negative breast cancer
- PMRT:
-
Postmastectomy radiotherapy
- LRFS:
-
Locoregional recurrence-free survival
- OS:
-
Overall survival
- LVI:
-
Lymphovascular invasion
- NACT:
-
Neoadjuvant chemotherapy
- ACT:
-
Adjuvant chemotherapy
- H&E:
-
Hematoxylin and eosin
- WSI:
-
Whole slide image
- WCH:
-
West China Hospital, Sichuan University
- TCGA:
-
The Cancer Genome Atlas
- iDFS:
-
Invasive disease-free survival
- XGBoost:
-
EXtreme Gradient Boosting
- BCS:
-
Breast-conserving surgery
- ROC:
-
Receiver operating characteristic
- SHAP:
-
Shapley’s additive explanation
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- AUC:
-
The area under the ROC curve
References
Leon-Ferre, R. A. & Goetz, M. P. Advances in systemic therapies for triple negative breast cancer. BMJ (Clinical Res. ed.). 381, e071674 (2023).
Kumar, H. et al. A review of biological targets and therapeutic approaches in the management of triple-negative breast cancer. J. Adv. Res. 54, 271–292 (2023).
Di Leone, A. et al. Local treatment of Triple-Negative breast cancer: Is mastectomy superior to breast-Conserving surgery?? J. Pers. Med. 13 (2023).
O’Rorke, M. A., Murray, L. J. & Brand, J. S. Bhoo-Pathy, N. The value of adjuvant radiotherapy on survival and recurrence in triple-negative breast cancer: A systematic review and meta-analysis of 5507 patients. Cancer Treat. Rev. 47, 12–21 (2016).
Kim, D., Kim, J. H., Kim, I. A., Chang, J. H. & Shin, K. H. Impact of postmastectomy radiation therapy on breast cancer patients according to pathologic nodal status after modern neoadjuvant chemotherapy. Cancer Res. Treat. 55, 592–602 (2023).
Machado, L. B., Brody, M. B., Rotenberg, S. E., Stachelek, G. C. & Fernandez, J. G. Breast cancer tumor board: A radiologist’s guide to postmastectomy radiation therapy. Radiographics: Rev. Publication Radiological Soc. North. Am. Inc. 43, e220086 (2023).
Xia, L. Y., Xu, W. Y. & Zhao, Y. Effect of postmastectomy radiotherapy on T1-2N1M0 triple-negative breast cancer. PloS One. 17, e0270528 (2022).
Wang, X. et al. T1-2N1M0 triple-negative breast cancer patients from the SEER database showed potential benefit from post-mastectomy radiotherapy. Oncol. Lett. 19, 735–744 (2020).
Kim, K. et al. The role of Post-Mastectomy radiotherapy in T1-2N1 breast cancer patients: propensity score matched analysis. Cancers 15 (2023).
Kantor, O. et al. Optimizing axillary management in clinical T1-2N0 mastectomy patients with positive Sentinel lymph nodes. Ann. Surg. Oncol. 29, 972–980 (2022).
Sittenfeld, S. M. C. et al. A multi-institutional prediction model to estimate the risk of recurrence and mortality after mastectomy for T1-2N1 breast cancer. Cancer 128, 3057–3066 (2022).
Luo, C. et al. Nomogram predicting locoregional recurrence to assist Decision-Making of postmastectomy radiation therapy in patients with T1-2N1 breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 103, 905–912 (2019).
Luo, C. et al. The effect of postmastectomy radiation therapy on high-risk patients with T1-2N0 breast cancer. Breast (Edinburgh Scotland). 60, 1–5 (2021).
Lee, M. Recent advancements in deep learning using whole slide imaging for cancer prognosis. Bioengineering 10 (2023).
Duggento, A., Conti, A., Mauriello, A. & Guerrisi, M. Toschi, N. Deep computational pathology in breast cancer. Sem. Cancer Biol. 72, 226–237 (2021).
Pan, Y. et al. Whole slide imaging-based deep learning to predict the treatment response of patients with non-small cell lung cancer. Quant. Imaging Med. Surg. 13, 3547–3555 (2023).
Huang, D. S. et al. Intelligent Computing Theories and Application (Springer, 2022).
Zhang, Q. et al. Real-world efficacy and safety of Pyrotinib in patients with HER2-positive metastatic breast cancer: A prospective real-world study. Front. Pharmacol. 14, 1100556 (2023).
Wang, J. et al. Comparison of dyslipidemia incidence in Chinese early-stage breast cancer patients following different endocrine therapies: A population-based cohort study. Front. Endocrinol. 13, 815960 (2022).
Liu, X. et al. Treatment patterns and outcomes in older women with early breast cancer: a population-based cohort study in China. BMC Cancer. 21, 226 (2021).
Tolaney, S. M. et al. Updated standardized definitions for efficacy end points (STEEP) in adjuvant breast cancer clinical trials: STEEP version 2.0. J. Clin. Oncology: Official J. Am. Soc. Clin. Oncol. 39, 2720–2731 (2021).
Avidan, S. & Shamir, A. Seam carving for content-aware image resizing. ACM Trans. Graph. 26, 10 (2007).
Zhang, Y. et al. Deep Learning-based automatic diagnosis of breast cancer on MRI using mask R-CNN for detection followed by ResNet50 for classification. Acad. Radiol. 30 (Suppl 2), S161–S171 (2023).
van der Walt, S. et al. scikit-image: image processing in python. PeerJ 2, e453 (2014).
Li, Y. et al. Prediction of lung cancer risk in Chinese population with genetic-environment factor using extreme gradient boosting. Cancer Med. 11, 4469–4478 (2022).
salsa. Performance comparison of grid search and random search methods for hyperparameter tuning in extreme gradient boosting algorithm to predict chronic kidney failure. IJIES 14, 198–207 (2021).
Liu, P. et al. Optimizing survival analysis of XGBoost for ties to predict disease progression of breast cancer. IEEE Trans. Bio Med. Eng. 68, 148–160 (2021).
Gramegna, A. & Giudici, P. S. H. A. P. An evaluation of discriminative power in credit risk. Front. Artif. Intell. 4, 752558 (2021).
Kayali, M. et al. Post-mastectomy radiation therapy in Triple-Negative breast cancer patients: analysis of the BEATRICE trial. Ann. Surg. Oncol. 29, 460–466 (2022).
McGale, P. et al. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet (London England). 383, 2127–2135 (2014).
Song, A. H. et al. Artificial intelligence for digital and computational pathology. Nat. Rev. Bioeng. 1, 930–949 (2023).
Aberle, D. R. et al. The National lung screening trial: overview and study design. Radiology 258, 243–253 (2011).
Liu, P., Ji, L., Ye, F., Fu, B. & AdvMIL Adversarial multiple instance learning for the survival analysis on whole-slide images. Med. Image. Anal. 91, 103020 (2024).
Liu, P., Ji, L., Ye, F., Fu, B. & GraphLSurv A scalable survival prediction network with adaptive and sparse structure learning for histopathological whole-slide images. Comput. Methods Programs Biomed. 231, 107433 (2023).
Shi, J. Y. et al. Exploring prognostic indicators in the pathological images of hepatocellular carcinoma based on deep learning. Gut 70, 951–961 (2021).
Zheng, Q. et al. Accurate diagnosis and survival prediction of bladder cancer using deep learning on histological slides. Cancers 14 (2022).
Chen, C. et al. The pathological risk score: A new deep learning-based signature for predicting survival in cervical cancer. Cancer Med. 12, 1051–1063 (2023).
Liu, X. et al. Diagnosis of diabetic kidney disease in whole slide images via AI-driven quantification of pathological indicators. Comput. Biol. Med. 166, 107470 (2023).
van Bergeijk, S. A. et al. Deep learning supported mitoses counting on whole slide images: A pilot study for validating breast cancer grading in the clinical workflow. J. Pathol. Inf. 14, 100316 (2023).
Atallah, N. M. et al. Deciphering the morphology of Tumor-Stromal features in invasive breast cancer using artificial intelligence. Mod. Pathology: Official J. United States Can. Acad. Pathol. Inc. 36, 100254 (2023).
Shafi, S. & Parwani, A. V. Artificial intelligence in diagnostic pathology. Diagn. Pathol. 18, 109 (2023).
Bourgade, R. et al. Deep learning for detecting BRCA mutations in High-Grade ovarian cancer based on an innovative tumor segmentation method from whole slide images. Mod. Pathology: Official J. United States Can. Acad. Pathol. Inc. 36, 100304 (2023).
Hacking, S. M. et al. Whole slide image features predict pathologic complete response and poor clinical outcomes in triple-negative breast cancer. Pathol. Res. Pract. 246, 154476 (2023).
Mamounas, E. P. et al. Association between the 21-gene recurrence score assay and risk of locoregional recurrence in node-negative, Estrogen receptor-positive breast cancer: results from NSABP B-14 and NSABP B-20. J. Clin. Oncology: Official J. Am. Soc. Clin. Oncol. 28, 1677–1683 (2010).
Goodman, C. R. et al. 21-Gene recurrence score assay predicts benefit of Post-Mastectomy radiotherapy in T1-2 N1 breast cancer. Clin. Cancer Research: Official J. Am. Association Cancer Res. 24, 3878–3887 (2018).
Wang, X. et al. Impact of clinical-pathological factors on locoregional recurrence in mastectomy patients with T1-2N1 breast cancer: who can omit adjuvant radiotherapy? Breast Cancer Res. Treat. 190, 277–286 (2021).
Park, H. J. et al. Incorporating risk factors to identify the indication of Post-mastectomy radiotherapy in N1 breast cancer treated with optimal systemic therapy: A multicenter analysis in Korea (KROG 14–23). Cancer Res. Treat. 49, 739–747 (2017).
Xu, F. F. et al. Practical model to optimize the strategy of adjuvant postmastectomy radiotherapy in T1-2N1 breast cancer with modern systemic therapy. Front. Oncol. 12, 789198 (2022).
Acknowledgements
This study would like to thank the whole slice scanning support from the histopathology platform of the Institute of Clinical Pathology West China Hospital, Sichuan University.
Funding
This work was supported by Research Supporting Project from Science and Technology of Sichuan Province (2023YFH0095/23NSFSC1623), the 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYJC21035/ZYGX2022YGRH015), the Postdoctor Research Fund of West China Hospital, Sichuan University (2024HXBH034), the Technology Innovation Research Project of Chengdu Science and Technology Bureau (2024-YF05-00723-SN), and Shanghai Roche Pharmaceuticals Ltd. (SL45024).
Author information
Authors and Affiliations
Contributions
H.C. and L.Z.Z. have equally contributed to this work. H.C., X.R.Z., and F.Y. designed this study. L.Z.Z., X.R.Z., and H.C. processed, analyzed and interpreted data. L.Z.Z., L.P. J., P.L., C.X.L., and H.C. contributed to the experiments. L.Z.Z. and H.C. wrote the draft. X.R.Z., T.L., B.P., and F.Y. review and edited the draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, H., Zhang, L., Liu, P. et al. A whole slide image-based risk score predicts prognosis and postmastectomy radiotherapy benefit in triple negative breast cancer patients. Sci Rep 15, 31255 (2025). https://doi.org/10.1038/s41598-025-12957-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-12957-w
