
Abstract
This study aims to explore interrelationships among leisure activities and depression and the mediating roles of activities of daily living (ADL) and self-reported health (SRH) among older adults in China. Data were extracted from 9,893 participants aged 50 and older from the Chinese Longitudinal Healthy Longevity Survey (CLHLS) conducted in 2018. Pearson correlation analysis and multiple stepwise regression analysis were conducted by using SPSS, and the mediating effect was tested using the Process plugin. Leisure activities were negatively correlated with depression (r = − 0.169, P < 0.001), and positively correlated with ADL and SRH (r = 0.223, r = 0.123, P < 0.001). ADL and SRH were negatively correlated with depression (r = − 0.120, − 0.376, P < 0.001). Leisure activities can not only directly and negatively affect depression, but also can indirectly affect depression through positive effects on ADL and SRH. The mediating effect accounts for 30.79% of the total effect. ADL and SRH play mediating roles in the relationship among leisure activities and depression. The participation of elderly people in leisure activities reduces the risk of depression by increasing their level of daily activity ability and perceived health.
Similar content being viewed by others


Introduction
In Globally, mental disorders were the seventh leading cause of disability attributing to 970 million prevalent cases in 2019; depressive and anxiety disorders being the leading contributors to this burden1. Depression is ranked by WHO as the single largest contributor to global disability and is also the major contributor to suicide deaths2. Depressive disorders, peaking in older adulthood, affect approximately 63 million people or 7% of the population aged 60 years and older worldwide3. As China has entered an aging society, the proportion of people aged 60 and over in China reached 18.70%, and the proportion of people aged 65 and over reached 13.50%, with a trend of increasing year by year4, and thus improving mental health and particularly preventing depression among older adults are gradually becoming serious public health issues in China, especially after experiencing the COVID-19 epidemic.
A growing body of research has emphasized the protective role of leisure activities in promoting successful aging and psychological well-being5,6,7. Leisure activities-including physical, cognitive, intellectual, and social forms-are consistently linked to better health outcomes and reduced depression among older adults8,9,10,11,12. According to the Activity Theory, active engagement in meaningful leisure roles supports life satisfaction and psychological adaptation in older age. The theory posits that maintaining social roles and active lifestyles helps preserve older adults’ mental well-being13.
Furthermore, the Health Belief Model suggests that an individual’s willingness to engage in health-promoting behaviors-such as leisure activity-is influenced by perceived susceptibility to illness, perceived benefits of the behavior, and self-efficacy14. In this context, older adults who perceive health benefits from physical and social engagement are more likely to adopt and maintain leisure behaviors that protect against depression.
Leisure activities has also been found to be significantly related to depression and quality of life8, able to prevent depression as well as anxiety in the elderly10,15 and was a positive method to improve mental health16,17,18,19,20,21,22,23,24,25. Specifically, physical activity is inversely related to incident depression and anxiety, with higher levels of PA leading to a lower risk of depression and anxiety, and depression and anxiety are probably causally related to physical inactivity20,21; physical activity could reduce symptoms of depression and anxiety16,17,18,19; successful leisure participation in old age helps in relieving psychological stress, improving life satisfaction and life quality26 and associates with lowered all-cause mortality among older adults27,28. Physical activity has thus been proposed as an adjunct treatment therapy for depression and anxiety22,23,25.
ADL is an important indicator of the health of the elderly, and it is also their most basic self-care ability29. As age increases, the body functions of the elderly gradually decline, and their ability to engage in daily activities is impaired, resulting in not only the loss of independent living skills, but also a decrease in their range of activities and social participation, which limits their interpersonal communication and leads to negative emotions such as depression30. Studies have clearly shown that there is a close relationship between the ADL ability, social support, and depression status of elderly people31 and the worse the ADL ability, the higher the probability of depression in elderly people32.
SRH is a subjective indicator of health status containing biological, mental, social, and functional aspects of a person, including individual and cultural beliefs and health behaviors33. Studies show that SRH is a significant predictor of various aspects of current health status34, an important indicator of depression35 and is also associated with quality of life and depression36. Furthermore, depression has been shown to be associated with poor SRH as well as increased mortality in the general population37, and fair or poor SRH at baseline to be predictive of a twofold increased risk for major depression at follow-up, even after adjusting for socio-demographic characteristics, lifestyle-related behaviors, disability and diabetes characteristics (OR = 2.05, 95% CI 1.20–3.48)38.
Although many studies have been carried out to examine factors affecting depression among older adults, few studies have examined the relationships among those relevant factors simultaneously (e.g., leisure activities, ADL, SRH and depression) and there have been no studies to investigate the relationships between leisure activities and depression through mediating factors such as ADL or SRH. Therefore, t his study aims to explore interrelationships among leisure activities and depression and the mediating roles of ADL and SRH among older adults in China, using data from the CLHLS.
Materials and methods
Data source and samples
This study utilizes data from CLHLS conducted in 2018. The research was led by Professor Zeng Yi, Director of the Center for Healthy Aging and Family Studies at Peking University and covers 23 out of 31 provinces in China. The 2018 follow-up survey contains 15,874 respondents over 50 years of age and contains more than 750 questions including extensive data on demographics, socioeconomic conditions, psychological traits, social participation, and health conditions, and all data are collected via face-to-face interviews during inhome visits39. The Ethics.
Committee of Peking University approved the CLHLS study (IRB00001052–13074)40.More detailed information about the CLHLS and the detailsof the sampling design, response rates, attrition, and systematic assessments of data quality were available elsewhere41.
In the study, adults who met the following inclusion criteria were included: (a) complete information on variables of leisure activities, SRH and depression, (b) complete data related to variables such as age, sex, residence, education level, marital status, and economical status. A total of 15,874 participants were surveyed in the 2018 wave of the CLHLS. After excluding adults who did not meet the inclusion criteria, there were 9,893 older adults in the final analysis.
Assessment of leisure activities
A six-question index of activity was used to assess the participation in leisure activities of the participants. The participants were asked “ do you participate in the following activities? ”. The activities were provided as follows: (a) doing garden work, (b) reading newspapers or books, (c) playing cards or mahjong, (d) watching TV or listening to radio, (e) taking part in some social activities and (f) other outdoor activities (Tai Ji, square dance, visit and interact with friends, other outdoor activity). Responses for each activity in this study were recorded into a 5- frequency: “1. almost everyday ”, “ 2. not daily but at least once in a week ”, “ 3. not weekly but at least once in a month”, “4. not monthly but sometimes”, and “5. never”. Then we reverse 1–5 so that the higher the scores were, the higher level of participation in leisure activities. Total scores range from 6 to 30.
Assessment of activities of daily living
ADL was assessed by the ADL scale, including bathing, dressing, toileting, indoor transfers, continence, and feeding. Responses for each activity in this study were recorded into a 3 options: a score of 1 = without assistance, 2 = one part assistance or 3 = more than one part assistance. Then we reverse 1–3 so that the higher the scores were, the higher level of ADL. Total ADL score ranged from 6 to 18. Adequate properties of the scale have been reported in other studies among older adults in China42 and elsewhere43.
Assessment of self-reported health
SRH was assessed by the question as follows: How do you rate your health at present? with answers “1. very good ” “ 2. good ” “ 3. so - so” “ 4. bad ” “ 5. very bad ”. Then we reverse 1–5 so that the higher the scores were, the healthier participants were.
Assessment of depression
Depression was measured using the 10-item Center for Epidemiological Studies Depression Scale (CESD-10), which has shown adequate reliability44. For each item, participants were asked to rate “ how often you felt this way during the past week”. Responses were recorded on a five-point scale: 1 = always; 2 = often; 3 = sometimes; 4 = seldom; 5 = never. We reverse 1–5 so that the higher the scores were, the more severe in depression. Total scores range from 10 to 50. The Cronbach’s alpha for the CESD-10 in the study was 0.933.
Assessment of other variables
A number of factors related to demographics, socio-life status, and health were included in this study, as these may be risk factors for depression in older adults. They are age, sex, residence, education level, marital status, and economic status. Residence was divided into “urban” and “rural”. Education level was captured by asking participants their years of schooling.Marital status was categorized as “married and living with spouse”, “widowed”, and “others”. Economic status was divided into three groups, namely “Rich”, “so-so” and “poor”.
Statistical analysis
All analyses were conducted using SPSS 26.0 (SPSS Inc., Chicago, IL, USA) and the PROCESS macro (Version 3.5) developed by Andrew F. Hayes. Descriptive statistics and Pearson correlations were first calculated to explore relationships between variables. To examine the mediating roles of ADL and SRH in the relationship between leisure activities and depression, we employed Hayes’ PROCESS macro Model 4, which is specifically designed for testing parallel mediation models. This model allows for estimating multiple indirect effects from a single predictor through multiple mediators operating in parallel. We used 5,000 bootstrap samples to calculate bias-corrected 95% confidence intervals for the indirect effects. Mediation was considered statistically significant if the confidence intervals did not include zero.
Control variables including age, sex, residence, education level, marital status, and economic status were included in all regression models to account for potential confounding effects. Results are presented in terms of total, direct, and indirect effects with standardized coefficients.This analytic approach allows us to clarify the unique contribution of each mediator and assess whether ADL and SRH function as distinct, simultaneous pathways linking leisure activities to depression.
Results
Characteristics of the study population
Among the participants,45.7% were men (n = 4525) whereas 54.3% were women(n = 5368). Their average age is 83.2 years old, with an average education level of 3.7 years. 58.1% of the participants live in urban areas, 20.2% are rich, and 45.2% are married and living with spouse(Table 1).
Correlation analysis between depression, leisure activities, activities of daily living and self-reported health
Correlation analysis result indicated that depression and leisure activities are negatively correlated (r = −0.169, P < 0.001); depression had a negative correlation with ADL and SRH (r = − 0.120, − 0.376, P < 0.001); leisure activities had a positive correlation with ADL and SRH (r = 0.223, 0.123, P < 0.001). In the above analysis, sex, age, residence, education, marital status, and economic status are used as control variables.
An analysis of the mediating effect of activities of daily living and self-reported health
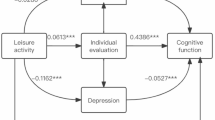
Leisure activities can not only directly and negatively affect depressive symptoms, but also can indirectly affect depressive symptoms through positive effects on ADL and SRH. The total mediating effect accounts for 30.79% of the total effect. Among them, the mediating effect of ADL accounts for 5.04% of the total effect, and the mediating effect of SRH accounts for 25.76% of the total effect. See Tables 2, 3 and 4, and Fig. 1.
*** p < 0.001.

Mediating Diagram of ADL and SRH in Leisure Activities and Depressive Symptoms.
Discussion
This study aims to explore interrelationships among leisure activities and depression and the mediating roles of ADL and SRH among older adults in China. The results showed that participation of leisure activities can not only reduce depressive symptoms directly but also can reduce depressive symptoms through the mediating effect of ADL and SRH.
The result demonstrated a negative relationship between leisure activities and depression among China older adults, consistent with the finding of previous studies16,17,18,19,20,21,45. This finding can be explained by the fact that increased frequency of participation in leisure activities, such as frequent game of cards/mahjong and TV/radio entertainment, is particularly important to reduce risk factors such as social isolation for older adults and associated with a lower risk of cognitive impairment46 and lesser feelings of loneliness47. Engaging in leisure activity helps the elderly find hobbies and release psychological pressure, thereby reducing depression46.
The study also demonstrated the indirect effect between leisure activity and depression in Chinese older adults can be mediated by ADL and SRH. In other words, leisure activity could improve ADL and SRH, and furthermore relieves their depression among elderly adults. The findings of this study enrich our understanding of the relationship between leisure activities and depression and provide a basis for policy interventions. Research shows that impaired ADL is a risk factor for the occurrence of depression48, and ADL impairment has a negative impact on personal life, and elderly people become dependent on others due to their inability to fully take care of themselves, feeling worthless and hopeless, leading to negative emotions49, while participating in leisure activities will improve the ADL ability of elderly people, thereby reducing the occurrence of depression. This also suggests that elderly people should actively participate in leisure activities, prevent ADL damage, and prevent depression.
SRH status has a mediating effect of 25.76% on the impact of leisure activities on depressive symptoms. In line with previous analyses conducted in Western countries, which indicated that SRH was negatively associated with depression among older adults38,50, we further confirmed that SRH was negatively associated with depressive symptoms among older adults in China, and SRH can negatively predict depressive symptoms, consistent with previous studies36. Given that, it is crucial to intervene to prevent depression when SRH worsens. Meanwhile, in order to reduce the occurrence of depressive symptoms, it is necessary to strengthen health education for the elderly, advocate for them to practice a healthy lifestyle, enhance their awareness of self health management, provide long-term care services that combine medical and elderly care, and improve their SRH level.
Strengths & Limitations
This study has several notable strengths. Firstly, it utilizes a large and representative sample from China, enhancing the generalizability of the findings and providing valuable references for similar research in other countries. Secondly, the study not only explores the direct relationship between leisure activities and depression among older adults but also analyzes the mediating roles of ADL and SRH. This multi-faceted approach enriches our understanding of the complex interactions among these variables.
However, this study has several limitations. First, the cross-sectional design limits causal inference; longitudinal data are needed to establish temporal relationships. Second, all variables were self-reported, which may introduce recall or social desirability biases. Third, the lack of clinical diagnoses of depression means that results reflect symptom severity rather than clinical cases. Future research should employ longitudinal designs and consider objective health measures to strengthen evidence for causal mechanisms.
Conclusion
This study’s results validate that elucidates the interconnections among leisure activities, ADL, SRH and depression among older adults in China. The findings underscore the significant positive influence of leisure activities on ADL and SRH and their role in reducing depression. Additionally, ADL and SRH was found to be a crucial factor in alleviating depression. These relationships highlight the partial and serial mediating effects of ADL and SRH on the link between leisure activities and depression.
The insights gained from this study can be instrumental in developing targeted health and physical education programs aimed at enhancing the mental well-being of older adults in China. Such programs should emphasize the promotion of leisure activities as a means to improve ADL and SRH and reduce depression. By addressing these factors, it is possible to create more effective interventions to support mental health among the elderly population, ultimately contributing to better overall quality of life.
Data availability
The datasets generated and/or analyzed during the current study are available in the Beijing University Open Research Data Platform repository, Center for Healthy Aging and Development, Beijing University, 2020, “Chinese Longitudinal Healthy Longevity Survey (CLHLS) in China”. https://doi.org/10.18170/DVN/WBO7LK. The datasets used are available from the first author on reasonable request.
References
IHME. Global Burden of Disease Study 2019 (GBD 2019) Results: Seattle, United States of America: Institute for Health Metrics and Evaluation (IHME). (2020). https://ghdx.healthdata.org/gbd-2019
World Health Organization. Depression and other common mental disorders: global health estimates. World Health Organization (2017). https://iris.who.int/handle/10665/254610
World Health Organization. Mental health of older adults. (2017). https://www.who.int/en/news-room/fact-sheets/detail/mental-health-of-older-adults
National Bureau of Statistics. The seventh National census. National Bureau Statistics (2021). https://www.gov.cn/guoqing/2021-05/13/content_5606149.htm
Yen, H. Y. & Lin, L. J. Quality of life in older adults: benefits from the productive engagement in physical activity. J. Exerc. Sci. Fit. 16 (2), 49–54. https://doi.org/10.1016/j.jesf.2018.06.001 (2018).
Sala, G. et al. The impact of leisure activities on older adults’ cognitive function, physical function, and mental health. PLOS ONE. 14 (11), e0225006. https://doi.org/10.1371/journal.pone.0225006 (2019).
Zhao, X., Yu, J. & Liu, N. Relationship between specific leisure activities and successful aging among older adults. J. Exerc. Sci. Fit. 21 (1), 111–118. https://doi.org/10.1016/j.jesf.2022.11.006 (2023).
Jeong, E. H. & Park, J. H. The relationship among leisure activities, depression and quality of life in Community-Dwelling elderly Koreans. Gerontol. Geriatric Med. 6, 233372142092344. https://doi.org/10.1177/2333721420923449 (2020).
Kim, E. C., Jeong, A., Lee, D. H., Park, D. H. & Jeon, J. Y. Impact of leisure physical activity and resistance exercise on the prevalence of depressive symptoms in Korean adults: analysis of the Korean National health and nutrition examination survey. J. Affect. Disord. 356, 329–337. https://doi.org/10.1016/j.jad.2024.04.028 (2024).
Bone, J. K. et al. Engagement in leisure activities and depression in older adults in the united states: longitudinal evidence from the health and retirement study. Soc. Sci. Med. 294, 114703. https://doi.org/10.1016/j.socscimed.2022.114703 (2022).
Dupuis, S. L. & Smale, B. J. A. An examination of relationship between psychological Well-Being and depression and leisure activity participation among older adults. Loisir Et Société / Soc. Leisure. 18 (1), 67–92. https://doi.org/10.1080/07053436.1995.10715491 (1995).
Guerrero Barragán, A., Lucumí, D. & Lawlor, B. Association of leisure activities with cognitive impairment and dementia in older adults in colombia: A SABE-Based study. Front. Neurol. 12, 629251. https://doi.org/10.3389/fneur.2021.629251 (2021).
Havighurst, R. J. Successful aging. Gerontologist 1 (1), 8–13 (1961).
Becker, M. H. The health belief model and personal health behavior. Health Educ. Monogr. 2 (4), 324–473 (1974).
Fancourt, D. & Tymoszuk, U. Cultural engagement and incident depression in older adults: evidence from the english longitudinal study of ageing. Br. J. Psychiatry. 214 (4), 225–229. https://doi.org/10.1192/bjp.2018.267 (2019).
Dale, L. P., Vanderloo, L., Moore, S. & Faulkner, G. Physical activity and depression, anxiety, and self-esteem in children and youth: an umbrella systematic review. Ment. Health. Phys. Act. 16, 66–79. https://doi.org/10.1016/j.mhpa.2018.12.001 (2019).
Rebar, A. L. et al. A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol. Rev. 9 (3), 366–378. https://doi.org/10.1080/17437199.2015.1022901 (2015).
McDowell, C. P. et al. Physical activity and generalized anxiety disorder: results from the Irish longitudinal study on ageing (TILDA). Int. J. Epidemiol. 47 (5), 1443–1453. https://doi.org/10.1093/ije/dyy141 (2018).
Ku, P. W., Fox, K. R. & Chen, L. J. Physical activity and depressive symptoms in Taiwanese older adults: A seven-year follow-up study. Prev. Med. 48 (3), 250–255. https://doi.org/10.1016/j.ypmed.2009.01.006 (2009).
Wanjau, M. N. et al. Physical activity and depression and anxiety disorders: A systematic review of reviews and assessment of causality. AJPM Focus. 2 (2), 100074. https://doi.org/10.1016/j.focus.2023.100074 (2023).
Mammen, G. & Faulkner, G. Physical activity and the prevention of depression. Am. J. Prev. Med. 45 (5), 649–657. https://doi.org/10.1016/j.amepre.2013.08.001 (2013).
Rosenbaum, S., Tiedemann, A., Sherrington, C., Curtis, J. & Ward, P. B. Physical activity interventions for people with mental illness: asystematic review and meta-analysis. J. Clin. Psychiatry. 75 (9), 14465 (2014). https://www.psychiatrist.com/jcp/physical-activity-interventions-ment al-illness-systematic/
Anderson, E. & Shivakumar, G. Effects of Exercise and Physical Activity on Anxiety. Frontiers in Psychiatry, 4. (2013). https://doi.org/10.3389/fpsyt.2013.00027
Craft, L. L. & Perna, F. M. The benefits of exercise for the clinically depressed. Prim. Care Companion J. Clin. Psychiatry. 6 (3), 104–111. https://doi.org/10.4088/pcc.v06n0301 (2004).
Belvederi Murri, M. et al. Physical exercise in major depression: reducing the mortality gap while improving clinical outcomes. Front. Psychiatry. 9 https://doi.org/10.3389/fpsyt.2018.00762 (2019).
Rowe, J. W. & Kahn, R. L. Successful aging. Gerontologist 37 (4), 433–440. https://doi.org/10.1093/geront/37.4.433 (1997).
Kobayashi, T. et al. Prospective study of engagement in leisure activities and All-Cause mortality among older Japanese adults. J. Epidemiol. 32 (6), 245–253. https://doi.org/10.2188/jea.JE20200427 (2022).
Li, Z. H. et al. Leisure activities and All-Cause mortality among the Chinese Oldest-Old population: A prospective Community-Based cohort study. J. Am. Med. Dir. Assoc. 21 (6), 713–719. https://doi.org/10.1016/j.jamda.2019.08.003 (2020).
Xiong, B. Y., Liu, T. Y. & Chen, T. Prevalence and associated factors of decline inactivities of daily living among middle-aged and older adults [J]. Chin. Gen. Pract. 25 (16), 1950–1955. https://doi.org/10.12114/j.issn.1007-9572.2022.0131 (2022).
Wang, X. et al. Associations of psychological distress with positive psychological variables and activities of daily living among stroke patients: A cross-sectional study. BMC Psychiatry. 19 (1), 381. https://doi.org/10.1186/s12888-019-2368-0 (2019).
Huang, H. R. et al. Analysis of loneliness and its risk f actors in 597 retired elderly people in Shenzhen. China J. Conval. Med.,, 26:1003–1006. https://doi.org/10.13517/j.cnki.ccm.2017.09.049 (2017).
Zhuang Xiaowei, C. et al. A cross-sectional study on the psychological health, daily living activity ability, and social support of elderly people [J]. Chin. J. Rehabilitation Med. 32 (10), 1162–1166. https://doi.org/10.3969/j.issn.1001-1242.2017.10.016 (2017).
Stanojević Jerković, O., Sauliūnė, S., Šumskas, L., Birt, C. & Kersnik, J. Determinants of self-rated health in elderly populations in urban areas in slovenia, Lithuania and UK: findings of the EURO-URHIS 2 survey. Eur. J. Public. Health. ckv097. https://doi.org/10.1093/eurpub/ckv097 (2015).
Choi, Y. Is subjective health reliable as a proxy variable for true health? A comparison of Self-rated health and Self-assessed change in health among Middle-aged and older South Koreans. Health Social Welf. Rev. 36 (4), 431–459. https://doi.org/10.15709/HSWR.2016.36.4.431 (2016).
Kim, Y. & Jang, E. Low Self-Rated health as A risk factor for depression in South korea: A survey of young males and females. Healthcare 9 (4), 452. https://doi.org/10.3390/healthcare9040452 (2021).
Vaez, M., Kristenson, M. & Laflamme, L. Perceived quality of life and Self-Rated health among First-Year university students. Soc. Indic. Res. 68 (2), 221–234. https://doi.org/10.1023/B:SOCI.0000025594.76886.56 (2004).
Lavretsky, H. et al. Predictors of Two-Year mortality in a prospective UPBEAT study of elderly veterans with comorbid medical and psychiatric symptoms. Am. J. Geriatric Psychiatry. 10 (4), 458–468. https://doi.org/10.1097/00019442-200207000-00012 (2002).
Badawi, G. et al. Self-rated health: A predictor for the three year incidence of major depression in individuals with type II diabetes. J. Affect. Disord. 145 (1), 100–105. https://doi.org/10.1016/j.jad.2012.07.018 (2013).
Yi, Z. Reliability of Age Reporting Among the Chinese Oldest-Old in the CLHLS Datasets. In Z. Yi, D. L. Poston, D. A. Vlosky, & D. Gu (Eds.), Healthy Longevity in China (Vol. 20, pp. 61–78). Springer Netherlands. (2008). https://doi.org/10.1007/978-1-4020-6752-5_4
Yue, Z. et al. The association between falls and anxiety among elderly Chinese individuals: the mediating roles of functional ability and social participation. J. Affect. Disord. 301, 300–306. https://doi.org/10.1016/j.jad.2022.01.070 (2022).
Zeng, Y., Feng, Q., Hesketh, T., Christensen, K. & Vaupel, J. W. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in china: A cohort study. Lancet 389 (10079), 1619–1629. https://doi.org/10.1016/S0140-6736(17)30548-2 (2017).
Byun, M., Kim, J. & Kim, J. E. Physical and psychological factors contributing to incidental falls in older adults who perceive themselves as unhealthy: A Cross-Sectional study. Int. J. Environ. Res. Public Health. 18 (7), 3738. https://doi.org/10.3390/ijerph18073738 (2021).
Teixeira, L., Araújo, L., Duarte, N. & Ribeiro, O. Falls and fear of falling in a sample of centenarians: the role of multimorbidity, pain and anxiety. Psychogeriatrics 19 (5), 457–464. https://doi.org/10.1111/psyg.12423 (2019).
Chen, H. & Mui, A. C. Factorial validity of the center for epidemiologic studies depression scale short form in older population in China. Int. Psychogeriatr. 26 (1), 49–57. https://doi.org/10.1017/S1041610213001701 (2014).
Li, W. et al. Leisure activity and cognitive function among Chinese old adults: the multiple mediation effect of anxiety and loneliness. J. Affect. Disord. 294, 137–142. https://doi.org/10.1016/j.jad.2021.07.051 (2021).
Xu, M. et al. Engagement in leisure activities and cognitive function by socioeconomic groups in china: A prospective cohort study. J. Affect. Disord. 327, 362–367. https://doi.org/10.1016/j.jad.2023.02.026 (2023).
Teh, J. K. L. & Tey, N. P. Effects of selected leisure activities on preventing loneliness among older Chinese. SSM-Population Health. 9, 100479. https://doi.org/10.1016/j.ssmph.2019.100479 (2019).
CHEN J F,FANG M W,XIAO C et al. Activities of daily living and depressive symptoms in the Chinese elderly.Chinese General Practice,2020,23(22):2852–2855,2862.https://link.cnki.net/urlid/13.1222.R.2019112 8.1017.064.
Hossain, B., Yadav, P. K., Nagargoje, V. P. & Vinod Joseph, K. J. Association between physical limitations and depressive symptoms among Indian elderly: marital status as a moderator. BMC Psychiatry. 21 (1), 573. https://doi.org/10.1186/s12888-021-03587-3 (2021).
Molarius, A. & Janson, S. Self-rated health, chronic diseases, and symptoms among middle-aged and elderly men and women. J. Clin. Epidemiol. 55 (4), 364–370. https://doi.org/10.1016/S0895-4356(01)00491-7 (2002).
Author information
Authors and Affiliations
Contributions
YZ contributed to all aspects of the study, including designing this research. SS collected, processed and analyzed. ZJ material availability and funding. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of interest
There was no conflict of interest between Yongduo Zhang, Shuo Sun and Zongqiang Jin and agreed to publish.
Consent for publication
Informed consent is obtained from all participants in the manuscript.
Ethics statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the the Ethics Committee of Peking University (IRB00001052-13074) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, Y., Sun, S. & Jin, Z. Leisure activities indirectly affect depression in older chinese adults through activities of daily living and self-rated health. Sci Rep 15, 28481 (2025). https://doi.org/10.1038/s41598-025-14596-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-14596-7
