
Abstract
Falls constitute a significant public health issue affecting middle-aged and older adults.The consequences of falls extend beyond physical injuries and compromised quality of life to encompass psychological and socioeconomic dimensions. Investigate the mediating role of Activities of Daily Living (ADL) in the relationship between balance ability and falls. This study utilized data from the 2015 China Health and Retirement Longitudinal Study (CHARLS). Balance ability was assessed using the Short Physical Performance Battery (SPPB), while ADL were evaluated through the CHARLS ADL questionnaire. Demographic factors and health-related indicators were incorporated as covariates.Data analysis was conducted in StataMP 17, employing chi-square tests, independent samples t-tests, correlation analysis, and parallel mediation analysis. Results revealed significant between-group differences in gender, marital status, and education level (all p < 0.001) between fallers and non-fallers.Females accounted for 67.6% of fall incidents, surpassing the male proportion (32.3%). Mediation analysis identified a significant direct effect of balance ability on falls (c’ = 0.002, p < 0.05), with ADL demonstrating partial mediation (a*b = 0.019, 95% CI: 0.014–0.026). Our findings demonstrates significant associations between falls, balance ability, and ADL disability. Activities of daily living (ADL) disability partially mediates the association between balance ability and falls. However, the observed associations were modest in strength, and the study’s cross-sectional design, reliance on self-reported data, and high baseline balance scores in the sample limit causal inference and generalizability. These results highlight the multifactorial nature of falls and underscore the importance of integrated prevention strategies that address both physical function and other potential mediators.
Similar content being viewed by others

Introduction
Population aging represents a significant demographic trend in the twenty-first century, exerting profound socioeconomic impacts across all societal domains. Globally, approximately 58 million individuals reach the age of 60 annually, with projections indicating this age cohort will constitute 22% of the global population by 20501. China, hosting one-fifth of the world’s elderly population, faces particular challenges in ensuring the health and well-being of its aging citizens.
Falls constitute a critical public health challenge impacting middle-aged and older adults. National surveillance data indicate falls as the leading cause of injury-related mortality among Chinese adults aged 65 years and above.The consequences of falls primarily manifest through physical functional decline and deterioration in quality of life. Post-fall fracture incidence demonstrates significant age-related disparities, with substantially higher rates observed in older populations. Fractures frequently precipitate chronic pain, mobility limitations, and prolonged immobilization, elevating risks of thrombosis, pneumonia, and other complications. Cranial trauma from falls—including concussions and intracranial hemorrhage—imposes disproportionate health burdens on older adults2,3. The impact of falls extends beyond physical health to psychological well-being and socioeconomic dimensions. Psychologically, falls may trigger cascading mental health consequences. Post-fall syndrome frequently manifests as kinesiophobia, restricting physical activity and compromising life quality4. Epidemiologic studies demonstrate elevated depression rates among older adults with fall histories5. Socioeconomically, fall injuries escalate healthcare expenditures while perpetuating cycles of disability, functional decline, and productivity losses, substantially burdening social welfare systems3. Fall prevention requires multifactorial interventions addressing physiological, psychological, and socioenvironmental determinants. Fall prevention requires multifactorial interventions addressing physiological, psychological, and socioenvironmental determinants. Multidisciplinary strategies integrating exercise regimens, pharmacological optimization, and environmental modifications demonstrate proven efficacy in risk mitigation6,7,8.
Balance ability constitutes a critical determinant for maintaining functional independence in older adults.Age-related deterioration in balance capacity demonstrates a strong association with escalating fall risk9. Multidimensional determinants of balance ability encompass physiological decline, sensory degradation, cognitive impairment, psychosocial factors, environmental interactions, and polypharmacy effects10,11,12. Research has shown that multi-factor interventions can effectively improve or maintain the balance ability of the elderly13. Balance assessment methodologies span static evaluations (Berg Balance Scale, BBS), dynamic analyses (gait kinematics), and proactive/reactive stability testing paradigms8. Methodological diversity characterizes both balance evaluation and rehabilitation strategies. These tools enable precise fall risk stratification and inform personalized intervention protocols. Current research priorities include developing context-sensitive interventions for seamless integration into daily living activities.
Activities of daily living (ADL) encompass essential self-care capacities fundamental to autonomous functioning.With the increase of age, the decline of ADL has become a key factor affecting the quality of life of middle-aged and elderly people.Current research investigates ADL disability through three conceptual frameworks:Physiological studies have found that age-related declines in physiological functions, including reduced muscle strength, limited joint mobility, and diminished sensory perception, significantly affect ADL14.Chronic conditions such as cardiovascular diseases, diabetes mellitus, and arthritis further exacerbate ADL disability in middle-aged and older adults.Psychological research demonstrates that mental health issues like depression and anxiety reduce life motivation and self-confidence, thereby impairing ADL performance. For example, depressed older adults often exhibit diminished initiative and interest in daily tasks, accompanied by fatigue and weakness, ultimately resulting in ADL disability15. Sociological research has found that the completeness of social support systems, the adaptability of home environments, and the utilization of community resources significantly impact older adults’ ADL.Additionally, ADL disability can increase older adults’ hospitalization risk and long-term care needs, while prolonged treatment negatively affects mental health, reducing life satisfaction and well-being16. Therefore, a strong correlation exists between ADL capacity and quality of life in older adults.
Prior research has extensively established the independent associations between balance impairment, ADL disability, and fall risk in older adults. Studies confirm that diminished balance capacity directly increases fall incidence17, while ADL limitations exacerbate fall susceptibility due to functional dependence18. However, the mediating role of ADL disability in the pathway linking balance ability to falls remains underexplored. Leaving a gap in understanding the mechanistic interplay in aging populations like China, where sociocultural and healthcare contexts differ. This study addresses this by quantifying ADL’s mediation effect using nationally representative data, thus bridging a critical knowledge gap in fall prevention frameworks.
Methods
Study setting and participants
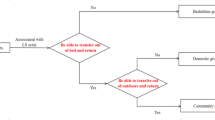
The China Health and Retirement Longitudinal Study (CHARLS), a nationally representative survey, provides comprehensive data on physical health, mental well-being, and intergenerational interactions among middle-aged and older adults, serving as a robust foundation for aging-related research. To address research objectives, longitudinal data from 2011, 2013, and 2015 underwent preliminary screening, with cross-sectional analysis conducted using the 2015 dataset. The Harmonized CHARLS dataset from the Gateway to Global Aging Data platform rectified baseline information discrepancies in repeated participants across 2011–2015 survey waves. For methodological transparency, key variables (ADL disability, balance ability, fall history) were extracted, and two models were constructed for analysis: Model 1 (demographic-adjusted) and Model 2 (health-covariate-adjusted). Initial screening excluded deceased individuals and new enrollees from the 2015 CHARLS data, yielding 25,586 eligible participants. Following standardized protocols for functional assessments, 14,303 participants completing all three balance ability tests were retained.Exclusion criteria removed 7,261 participants with incomplete physical activity records, 15 with missing fall/health data, and 2,481 with invalid BMI/ADL measurements. The final analytical sample comprised 4,378 participants meeting stringent inclusion criteria. Mathematical modeling examined the balance ability-fall risk association and ADL-mediated effects using standardized metrics (see Fig. 1).

Sample selection flowchart.
Balance ability test and ADLs assessment method
Balance assessment: We exclusively utilized the balance subtest of the Short Physical Performance Battery (SPPB) to evaluate static balance ability. The strength (chair stand test) and gait speed components of the full SPPB were not included in this analysis, as our focus was on isolating the relationship between postural stability and fall risk. The balance assessment comprises three progressive difficulty levels: SIDE-BY-SIDE stance, SEMI-TANDEM stance, and FULL-TANDEM stance. CHARLS protocol initiates testing with SEMI-TANDEM stance, reverting to SIDE-BY-SIDE if unsuccessful, then progressing to FULL-TANDEM when performance criteria are met. This study employed standardized SPPB balance scoring criteria as follows:0: Unable to complete any stance tests1: SIDE-BY-SIDE stance only 2: SIDE-BY-SIDE + SEMI-TANDEM stances 3: SIDE-BY-SIDE + SEMI-TANDEM stances with FULL-TANDEM < 30/60 s 4: Full completion of all three stance tests.
The CHARLS ADL assessment employs Lawton and Brody’s (1969) Physical Self-Maintenance Scale, comprising both basic and instrumental ADL components. This study focused on six basic ADL items: dressing, bathing, eating, toileting, continence control, and bed transfer. Each item uses a 4-point scale: 1 (no difficulty), 2 (difficulty but independent completion), 3 (requires assistance), and 4 (unable to perform).Higher participant scores indicate a greater level of ADL disability.
Other covariates
Covariates were derived from the 2015 CHARLS questionnaire, physical examinations, and functional assessments. To investigate the effects of additional covariates on fall risk, covariates were stratified into Model 1 and Model 2. Model 1 ( Demographic-adjusted ) : age, sex, educational attainment, and marital status. Educational attainment was categorized as: 1) Less than lower secondary 2) Upper secondary and vocational training 3) Tertiary education. Marital status was classified into: 1) Never married 2) Married 3) Divorced 4) Widowed or living alone. Model 2 ( Demographic + Health-adjusted ) : height, weight, BMI, waist circumference, physical activity patterns, and alcohol consumption.Physical activity intensity levels were defined as: 1) Vigorous: Heavy lifting, digging, farming, aerobic exercises, fast cycling 2) Moderate: Carrying light loads, bicycling at regular pace, mopping, tai chi, brisk walking 3) Light: Walking for transportation or leisure. Height measurements were standardized to meters for BMI calculation using the formula: BMI = weight (kg) / height (m)2.
Statistical analysis
Data processing was performed using StataMP 17.Categorical variables are presented as counts (percentages), while continuous variables are expressed as mean ± standard deviation (SD) or median (interquartile range, IQR).Between-group differences (fallers vs. non-fallers) were assessed using chi-square tests for categorical variables and independent samples t-tests for continuous measures.Bivariate correlation analysis confirmed associations between fall incidence, ADL disability, and balance ability. Covariates were selected a priori based on established fall risk frameworks19 (WHO Global Report on Falls Prevention, 2007).
We employed a parallel single-mediator model to examine the mediating role of ADL disability in the relationship between balance ability (independent variable, IV) and falls (dependent variable, DV). Additionally, correlation analyses between ADL disability and physical activity parameters (intensity/frequency) evaluated exercise-induced effects on functional independence.
Ethics statement
All CHARLS survey waves received ethical approval from the Peking University Biomedical Ethics Committee.The fieldwork protocol for this household survey was approved under Approval Code: IRB00001052-11,015.Written informed consent was obtained from all participants20.
Results
Comparison of baseline characteristics between fallers and non-fallers
This cross-sectional analysis utilized multi-source data from the 2015 China Health and Retirement Longitudinal Study (CHARLS) to examine the association between balance ability and falls in middle-aged and older adults.Table 1 presents baseline characteristics of the 4,378 participants (mean age 61.2 years; female predominance 61.1%).Among them, 933 individuals (67.6% female, 32.4% male) reported ≥ 1 fall incident during the preceding two years.Fallers exhibited marginally higher mean age than non-fallers, though the difference was not statistically significance (p > 0.05).The faller group demonstrated higher proportions of individuals with lower educational attainment, divorced, widowed, or living alone status.In terms of ADL, fallers displayed significantly higher composite scores (7.093 ± 1.833) compared to non-fallers (6.498 ± 1.279).Statistically significant differences were found across all ADL subdomains between groups (p < 0.001).Balance ability scores were significantly lower in fallers (3.638 ± 0.691) versus non-fallers (3.730 ± 0.575) (p < 0.001).
Interrelationships among falls, balance capacity, and activities of daily living (ADLs)
Table 2 delineates the interrelationships between falls, balance ability, and ADL disability in middle-aged and older adults.Significant negative correlations emerged between fall incidence and balance metrics: Balance 1 (r = -0.037, p = 0.015), Balance 2 (r = -0.04, p = 0.008), Balance 3 (r = -0.057, p < 0.001), and composite balance score (r = -0.057, p < 0.001).A positive association was observed between falls and ADL impairment (r = 0.196, p < 0.001).Balance ability was inversely correlated with ADL disability (r = -0.146, p < 0.001).
Mediating role of activities of daily living (ADLs)
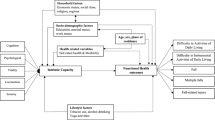
To examine the mediating role of ADL disability, we constructed two parallel mediation models (Fig. 2) : Model 1 adjusted for demographic covariates (age, sex, education, marital status). Model 2 further incorporated health-related covariates (BMI, physical activity, alcohol consumption). Path coefficients (β) and 95% confidence intervals (CI) are reported for all direct/indirect effects.

The conceptional framework of the mediation models.
As depicted in Fig. 2, both models confirmed significant negative paths from balance ability to ADL disability (Model 1: β = -0.404; Model 2: β = -0.414, p < 0.001) and from ADL disability to falls (Model 1: β = -0.046; Model 2: β = -0.047, p < 0.001). The direct effect of balance ability on falls remained significant only in Model 2 (β = 0.023, p = 0.038). Crucially, the indirect effect via ADL was consistent across models (a × b = 0.019), accounting for 48.7% of the total effect. The exclusion of zero from these intervals indicates significant mediation effects21.
Associations between activities of daily living (ADLs) and exercise modalities/frequency
Table 3 delineates associations between ADL disability and physical activity modalities/frequencies.Non-significant correlations were found between ADL disability and vigorous-intensity exercise (r = -0.003, p = 0.837) or its weekly frequency (r = -0.005, p = 0.743).Significant negative correlations emerged for moderate-intensity exercise (r = -0.07, p < 0.001), walking duration (r = -0.041, p = 0.007), weekly moderate-intensity activity frequency (r = -0.067, p < 0.001), and weekly walking frequency (r = -0.06, p < 0.001).These findings suggest ADL disability is modulated through physical activity parameters, predominantly mediated via moderate-intensity exercise and walking engagement.
Discussion
Leveraging data from the China Health and Retirement Longitudinal Study (CHARLS), this study investigated the association between balance ability and falls among middle-aged and older Chinese adults, while examining the role of ADL disability in this relationship. The results revealed a significant association between balance ability and fall incidence in this population,with ADL disability demonstrated partial mediation effects in the balance ability-fall risk pathway. Physical activity modalities and their frequencies showed significant associations with ADL disability.
Our multidimensional analysis of fall determinants revealed significantly elevated fall incidence among individuals with compromised balance ability. Gillian Quinn et al. identified significant disparities in balance ability between fallers and non-fallers through clinical balance assessments17. Fall risk exhibits significant demographic variation, particularly across age strata and sex categories.Physiological studies attribute higher female fall rates to sex-specific vulnerabilities including accelerated bone mineral density loss and sarcopenia progression22. Age-related deterioration in sensory integration, neuromuscular coordination, and musculoskeletal function progressively impairs postural control mechanisms23. The age-associated sarcopenia trajectory exacerbates fall risk through compromised kinetic stability24,25. Therefore, the mechanism by which balance ability influences falls should be comprehensively examined from multiple perspectives.
Mediation analyses revealed partial mediation of balance ability’s effect on falls through ADL disability pathways. Individuals with compromised balance ability exhibited ADL limitations that amplified fall susceptibility. As a direct fall determinant, balance ability enhancement represents a critical intervention target for fall prevention. Clinical evidence substantiates exercise interventions as effective modalities for improving balance ability across patient populations. Mind–body exercises (e.g., Tai Chi, yoga) demonstrate efficacy in balance enhancement and fall risk reduction26. Pratik Lamichhane et al. documented augmented reality-based training’s benefits for balance optimization and fall prevention27. Alex Martino Cinnera et al. reported dual-task training’s selective efficacy in improving dynamic balance (despite limited static balance effects) in multiple sclerosis patients28.Similar therapeutic benefits have been replicated in stroke rehabilitation contexts29. ADL disability partially explains the link between balance impairment and falls. This suggests that interventions targeting ADL (e.g., task-specific training) may amplify the benefits of balance-focused exercises in fall prevention. ADL disability directly reflects integrated neuromuscular functions including muscle strength, balance control, and mobility.Non-fallers exhibited superior isokinetic strength in key muscle groups (e.g., hip abductors) compared to fallers30, suggesting that muscle weakness may constrain ADL performance (ambulation, sit-to-stand transitions) and escalate fall susceptibility.Gait instability and postural deficits, being primary fall determinants, also critically modulate ADL disability31.
While our study demonstrates statistically significant associations between balance ability, ADL disability, and falls, it is crucial to interpret these findings within the context of the specific characteristics of our data and the inherent limitations of the study design. The correlation coefficients observed, although statistically significant (p < 0.001), were relatively modest in magnitude (e.g., r = -0.057 for balance ability and falls, r = 0.196 for ADL disability and falls). This indicates that while balance ability and ADL disability are associated with fall risk in this population, they explain a limited proportion of the variance in fall occurrence individually. The partial mediation effect of ADL disability (a*b = 0.019), while statistically significant, also represents a quantitatively small indirect effect. This underscores the complexity of fall etiology and suggests that a multitude of other factors, beyond balance and basic ADLs, contribute substantially to fall risk in middle-aged and older adults. Our findings support the inclusion of balance and ADL assessment in multifactorial fall risk evaluations, but highlight that they are unlikely to be strong sole predictors.
Our baseline analysis found no statistically significant associations between the three physical activity modalities and fall incidence. Conversely, Yoshiro Okubo et al. demonstrated that reactive/volitional stepping interventions reduced fall rates by approximately 50% in older adults32. Integrated with our findings, the ADL-physical activity associations suggest a multifactorial interplay between exercise patterns and fall mechanisms. The observed inverse relationships between ADL disability and moderate-intensity exercise/walking engagement indicate their protective effect on functional independence in aging populations. A community-based study of older women revealed that cadence intensity (e.g., peak 30/60 steps/min) more effectively reduces peripheral artery disease (PAD) risk than total daily steps, suggesting moderate-intensity walking (e.g., brisk walking) may reduce ADL disability via vascular function optimization33. Miyuki Nemoto et al. demonstrated that a 12-week multimodal intervention (5 sessions/week combining aerobic exercise, resistance training, and cognitive tasks) enhanced prefrontal activation and improved executive function/attentional control in frontotemporal lobar degeneration (FTLD) patients, facilitating complex ADL execution (dressing, feeding)34. High-frequency and diversified activity regimens enhance behavioral regulation capacities through neuroplasticity mechanisms. This further indicates that physical activity patterns play a significant role in improving ADL disability. Regarding exercise frequency, weekly moderate-intensity exercise frequency and weekly walking frequency demonstrate better performance in improving ADL disability. Among populations with cognitive impairment or dementia, function-oriented care approaches and long-term multimodal exercise may help maintain activities of daily living capacity, such as combined cognitive and physical function training. This suggests that activity methods need to be diversified and may require higher frequency to sustain the effects35,34,36,37. Exercise modalities exhibit intrinsic consistency with frequency parameters, as temporal accumulation of varied activities synergistically enhances functional outcomes.Joseph Michael Northey et al. established that ≥ 150 min/week of moderate-intensity exercise improves cognitive performance in adults over 50, irrespective of baseline cognitive status36. While direct evidence for ADL enhancement remains limited, appropriate exercise prescription demonstrates multifactorial benefits including reduced type 2 diabetes risk (HR 0.72) and dementia prevention (RR 0.58)37,38.
As an important mediating factor in fall risk among older adults, ADL disability is influenced by multifactorial determinants, necessitating comprehensive intervention strategies for its enhancement.Current evidence establishes strong associations between ADL disability and geriatric comorbidities including stroke and osteoporosis39,18. The high prevalence of chronic conditions may constrain mobility patterns and amplify fall risk during routine activities.Therefore, in the intervention measures to prevent falls, in addition to considering reasonable activity patterns, we should also pay attention to rational medication management, provision of assistive devices, and home environment modifications (e.g., installing handrails, replacing flooring with anti-slip materials)40,41. Complementary evidence from M.J. Chandler et al. substantiates cognitive remediation and behavioral strategies as viable modalities for ADL disability improvement39.
The cross-sectional design precludes establishing causal relationships between balance, ADL, and falls. Reliance on self-reported falls and functional status (ADL) introduces potential for recall and reporting bias. Furthermore, The average balance ability score in our final analytical sample (mean = 3.71, SD = 0.60 on a 0–4 scale) was relatively high. This suggests that a significant portion of participants had good baseline balance function, potentially limiting the variability available to detect stronger associations between balance deficits and falls. The SPPB balance subscale, while a valid clinical tool, may have reduced sensitivity to detect subtle balance impairments in a population performing well overall, creating a potential ceiling effect. Future research should employ longitudinal designs to better elucidate causal pathways and investigate the effectiveness of interventions targeting both balance improvement and ADL enhancement in diverse populations, including those with greater functional limitations. Incorporating objective measures of falls and physical function could further strengthen the evidence.
In conclusion, this study provides evidence supporting statistically significant, albeit modest, associations between lower balance ability, higher ADL disability, and increased fall risk among middle-aged and older Chinese adults, with ADL disability acting as a partial mediator. The relatively high baseline balance in our sample and the limitations inherent in the cross-sectional design and self-reported measures necessitate cautious interpretation of the effect sizes and causal pathways. These findings reinforce the multifactorial nature of falls. Balance enhancement remains a crucial intervention target. Improving ADLs is vital for functional independence, but its specific role as a mediator of fall risk driven by balance deficits appears quantitatively limited in this relatively high-functioning population. Future longitudinal research, incorporating objective measures of balance, function, and falls, and focusing on diverse populations including those with greater functional impairment, is needed to confirm these pathways and quantify the clinical impact of interventions targeting them.
Conclusion
This study, utilizing cross-sectional data from the CHARLS cohort, demonstrates statistically significant associations between falls, balance ability, and ADL disability among middle-aged and older Chinese adults. Balance ability suggests a direct association with fall risk, while ADL disability exhibits a partial mediating effect in this pathway. Physical exercise remains an important, potentially modifiable intervention target for improving balance capacity. Therefore, improving ADL disability may represent one strategy to mitigate fall risk. However, the modest strength of the observed associations and the high baseline balance scores indicate that these factors likely have limited predictive power on their own and underscore the necessity for multifactorial fall prevention approaches. Furthermore, the cross-sectional design and reliance on self-reported data limit causal inferences regarding these relationships.
Data availability
The data supporting this study are from the China Health and Retirement Longitudinal Study (CHARLS), a publicly available dataset managed by the National School of Development at Peking University. Researchers can access the data by registering and submitting a request through the CHARLS official website (http://charls.pku.edu.cn).
References
WHO. World report on ageing and health. 2015. https://apps.who. int/iris/handle/10665/186463 (accessed June 10, 2022).
Yu, W. Y., Hwang, H. F., Chen, C. Y. & Lin, M. R. Situational risk factors for fall-related vertebral fractures in older men and women. Osteoporos. Int. 32(6), 1061–1070. https://doi.org/10.1007/s00198-020-05799-x (2021).
Vaishya, R. & Vaish, A. Falls in older adults are serious. Ind. J. Orthop. 54(1), 69–74. https://doi.org/10.1007/s43465-019-00037-x (2020).
Barr, J. et al. Topography of cholinergic nerve terminal vulnerability and balance self-efficacy in Parkinson’s Disease. J. Integr. Neurosci. 23(9), 178. https://doi.org/10.31083/j.jin2309178 (2024).
Hull, S. L., Kneebone, I. I. & Farquharson, L. Anxiety, depression, and fall-related psychological concerns in community-dwelling older people. Am. J. Geriatr. Psychiatr. 21(12), 1287–1291. https://doi.org/10.1016/j.jagp.2013.01.038 (2013).
Zhao, R., Feng, F. & Wang, X. Exercise interventions and prevention of fall-related fractures in older people: A meta-analysis of randomized controlled trials. Int. J. Epidemiol. 46(1), 149–161. https://doi.org/10.1093/ije/dyw142 (2017).
Lee, J., Negm, A., Peters, R., Wong, E. K. C. & Holbrook, A. Deprescribing fall-risk increasing drugs (FRIDs) for the prevention of falls and fall-related complications: A systematic review and meta-analysis. BMJ Open 11(2), e035978. https://doi.org/10.1136/bmjopen-2019-035978 (2021).
Kahraman, T., Çekok, F. K., Üğüt, B. O., Keskinoğlu, P. & Genç, A. One-Year Change in the physical functioning of older people according to the international classification of functioning domains. J. Geriatr. Phys. Ther. 44(1), E9–E17. https://doi.org/10.1519/JPT.0000000000000234 (2021).
Blodgett, J. M., Ventre, J. P., Mills, R., Hardy, R. & Cooper, R. A systematic review of one-legged balance performance and falls risk in community-dwelling adults. Ageing Res. Rev. 73, 101501. https://doi.org/10.1016/j.arr.2021.101501 (2022).
Noamani, A., Lemay, J. F., Musselman, K. E. & Rouhani, H. Characterization of standing balance after incomplete spinal cord injury: Alteration in integration of sensory information in ambulatory individuals. Gait. Posture. 83, 152–159. https://doi.org/10.1016/j.gaitpost.2020.10.027 (2021).
Pazzaglia, C. et al. Comparison of virtual reality rehabilitation and conventional rehabilitation in Parkinson’s disease: A randomised controlled trial. Physiotherapy 106, 36–42. https://doi.org/10.1016/j.physio.2019.12.007 (2020).
Harwood, R. H. et al. Promoting activity, independence, and stability in early dementia and mild cognitive impairment (PrAISED): Randomised controlled trial. BMJ 29(382), e074787. https://doi.org/10.1136/bmj-2023-074787 (2023).
Kaneda, K., Sato, D., Wakabayashi, H., Hanai, A. & Nomura, T. A comparison of the effects of different water exercise programs on balance ability in elderly people. J. Aging Phys. Act. 16(4), 381–392. https://doi.org/10.1123/japa.16.4.381 (2008).
Campbell, E. et al. The effect of exercise on quality of life and activities of daily life in frail older adults: A systematic review of randomised control trials. Exp. Gerontol. 147, 111287. https://doi.org/10.1016/j.exger.2021.111287 (2021).
Cano, F., Alves, E., de GuedesPinho, L. & Fonseca, C. Functional capacity of institutionalized older people and their quality of life, depressive symptoms and feelings of loneliness: A cross-sectional study. Nurs. Rep. 14(4), 3150–3164. https://doi.org/10.3390/nursrep14040229 (2024).
Payette, M. C., Bélanger, C., Léveillé, V. & Grenier, S. Fall-related psychological concerns and anxiety among community-dwelling older adults: Systematic review and meta-analysis. PLoS ONE 11(4), e0152848. https://doi.org/10.1371/journal.pone.0152848 (2016).
Quinn, G., Comber, L., Galvin, R. & Coote, S. The ability of clinical balance measures to identify falls risk in multiple sclerosis: A systematic review and meta-analysis. Clin. Rehabilit. 32(5), 571–582. https://doi.org/10.1177/0269215517748714 (2018).
Al-Sari, U. A., Tobias, J. H. & Clark, E. M. Self-reported everyday physical activities in older people with osteoporotic vertebral fractures: A systematic review and meta-analysis. Osteoporo. Int.: A J.Establ. Result. Coop. Between Eur. Found. Osteoporo. Natl. Osteoporo. Found. USA 29(1), 19–29. https://doi.org/10.1007/s00198-017-4287-6 (2018).
World Health Organization. Ageing And Life Course Unit. WHO global report on falls prevention in older age. Geneva, Switzerland: World Health Organization. [Pdf] Retrieved from the Library of Congress, https://www.loc.gov/item/2021763108/ (2008).
Cohort profile: The China health and retirement longitudinal study (CHARLS) Int. J. Epidemiol. 43, 61–68 (2014).
Zhonglin, W. & Baojuan, Y. E. Analyses of mediating effects: The development of methods and models. Adv. Psychol. Sci. 22(5), 731–745 (2014).
Gandham, A. et al. Falls, fractures, and areal bone mineral density in older adults with sarcopenic obesity: A systematic review and meta-analysis. Obes. Rev. 22(5), e13187. https://doi.org/10.1111/obr.13187 (2021).
Jehu, D. A. et al. Risk factors for recurrent falls in older adults: A systematic review with meta-analysis. Maturitas 144, 23–28. https://doi.org/10.1016/j.maturitas.2020.10.021 (2021).
Beaudart, C. et al. Sarcopenia in daily practice: Assessment and management. BMC Geriatr. https://doi.org/10.1186/s12877-016-0349-4 (2016).
Beaudart, C., Zaaria, M., Pasleau, F., Reginster, J. Y. & Bruyère, O. Health outcomes of Sarcopenia: A systematic review and meta-analysis. PLoS ONE 12(1), e0169548. https://doi.org/10.1371/journal.pone.0169548 (2017).
Wang, L. C. et al. Optimal exercise parameters of tai chi for balance performance in older adults: A meta-analysis. J. Am. Geriatr. Soc. 69(7), 2000–2010. https://doi.org/10.1111/jgs.17094 (2021).
Lamichhane, P. et al. Augmented reality-based training versus standard training in improvement of balance, mobility and fall risk: A systematic review and meta-analysis. Ann. Med. Surg. (Lond). 85(8), 4026–4032. https://doi.org/10.1097/MS9.0000000000000986 (2023).
Martino Cinnera, A., Bisirri, A., Leone, E., Morone, G. & Gaeta, A. Effect of dual-task training on balance in patients with multiple sclerosis: A systematic review and meta-analysis. Clin. Rehabil. 35(10), 1399–1412. https://doi.org/10.1177/02692155211010372 (2021).
Ge, L. et al. Effects of traditional Chinese exercises on the rehabilitation of limb function among stroke patients: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 29, 35–47. https://doi.org/10.1016/j.ctcp.2017.08.005 (2017).
de Almeida Nagata, C., Hamu, TCDDS., Pelicioni, PHS., Pelicioni, PHS., & Durigan, JLQ. Influence of lower limb isokinetic muscle strength and power on the occurrence of falls in community-dwelling older adults: A longitudinal study. PloS one. (2024).
Colón-Emeric, CS., McDermott, CL., Lee, DS. & Berry, SD. Risk assessment and prevention of falls in older community-dwelling adults: A review. JAMA (2024).
Okubo, Y., Schoene, D. & Lord, S. R. Step training improves reaction time, gait and balance and reduces falls in older people: A systematic review and meta-analysis. Br. J. Sport. Med. 51(7), 586–593. https://doi.org/10.1136/bjsports-2015-095452 (2017).
Chenfei. Li., Litao, Du., Xue, X., Zhao, Na. & Qiang, He. Associations of daily steps and step intensity with peripheral arterial disease in Chinese community-dwelling older women. Exp. Gerontol. (2025).
Nemoto, M., Nemoto, K., Sasai, H., Higashi, S. & Ota, M. Long-term multimodal exercise intervention for patients with frontotemporal lobar degeneration: Feasibility and preliminary outcomes. dementia and geriatric cognitive disorders extra (2024).
Resnick, B., Boltz, M., Galik, E., McPherson, R. & Kuzmik, A. Nursing use of function-focused care with hospitalized patients living with dementia. Clin. Nurs. Res. (2024).
Northey, J. M., Cherbuin, N., Pumpa, K. L., Smee, D. J. & Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sport. Med. 52(3), 154–160. https://doi.org/10.1136/bjsports-2016-096587 (2018).
Mayor, S. Moderate exercise cuts type 2 diabetes risk but more is better, review finds. BMJ 17(355), i5605. https://doi.org/10.1136/bmj.i5605 (2016).
Lam, F. M. et al. Physical exercise improves strength, balance, mobility, and endurance in people with cognitive impairment and dementia: A systematic review. J. Physiother. 64(1), 4–15. https://doi.org/10.1016/j.jphys.2017.12.001 (2018).
Stolwyk, R. J., Mihaljcic, T., Wong, D. K., Chapman, J. E. & Rogers, J. M. Poststroke cognitive impairment negatively impacts activity and participation outcomes: A systematic review and meta-analysis. Stroke 52(2), 748–760. https://doi.org/10.1161/STROKEAHA.120.032215 (2021).
Montesinos, L., Castaldo, R. & Pecchia, L. Wearable inertial sensors for fall risk assessment and prediction in older adults: A systematic review and meta-analysis. IEEE Trans. Neural. Syst. Rehabil. Eng. 26(3), 573–582. https://doi.org/10.1109/TNSRE.2017.2771383 (2018).
Lachance, C. C. et al. Compliant flooring to prevent fall-related injuries in older adults: A scoping review of biomechanical efficacy, clinical effectiveness, cost-effectiveness, and workplace safety. PLoS ONE 12(2), e0171652. https://doi.org/10.1371/journal.pone.0171652 (2017).
Author information
Authors and Affiliations
Contributions
J.J.wrote the main manuscript text , data analysis and visualization. J.J. and Z.Q. enabled conceptualization and provided methodology. Z.C. and C.K. participated in paper review and editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jiang, J., Zhou, Q., Zhang, C. et al. Activities of daily living mediate the association between balance and falls in middle aged and older adults. Sci Rep 15, 28694 (2025). https://doi.org/10.1038/s41598-025-14608-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-14608-6
