
Abstract
In Sub-Saharan Africa (SSA), the burden of low birthweight (LBW) remains high, leading to considerable short- and long-term consequences for both newborns and mothers. However, limited evidence exists on the disparities and geographical distribution of LBW among adolescent (15–19 years) and non-adolescent women (20–49 years). This study aimed to assess the age-related disparity, geospatial distribution and determinants of LBW in SSA. The study used Demographic and Health Survey (DHS) data from 33 SSA countries released between 2010 and 2023. Concentration curves and indices, absolute and relative difference measures, spatial autocorrelation and hotspot analysis, and multilevel modelling were employed to explore differences in LBW by maternal age group. A total of 27,889 (15.5%) of adolescent women and 152,521 (84.5%) non-adolescent women were included in the analysis. LBW was significantly concentrated among adolescents (CI = − 0.096, p < 0.001), with a 13.2% prevalence compared to 8.3% in non-adolescents, highlighting a 4.9% absolute difference (relative difference = 1.60, p < 0.001). Lower educational level, unemployment, fewer number of antenatal care (ANC) visits, lacking permission to get medical care and being single marital status were the common variables significantly associated with LBW in both adolescent and non-adolescent women. However, unintended pregnancy and early sexual initiation were significantly associated with LBW in only adolescent women while distance to healthcare facilities and lower parity were found to be significantly associated with LBW only in non-adolescent women. At community level, region was a significant factor for LBW in both groups. Spatial autocorrelation and hotspot analysis showed that LBW was randomly distributed among adolescents (Moran’s test of − 0.0106 and p value = 0.904) but clustered in Mauritania, Mali, Niger, and Chad for non-adolescent women. This study found significant age-related disparities in LBW across SSA, with adolescent mothers facing a disproportionate burden. This underscores the need to focus on preventing adolescent pregnancy and providing support for pregnant adolescents by improving access to ANC, education, and economic empowerment to prevent adverse birth outcomes. Random distribution of LBW in adolescent women indicates the need for adolescent-specific regional interventions across SSA countries.
Similar content being viewed by others


Introduction
Low birthweight (LBW) is a significant public health issue in developing countries, causing serious health problems for newborns. Globally in 2025, 15–20% of newborns were born with a birthweight of less than 2.5 kg1. More than 90% of LBW is reported in low and middle income countries (LMICs), with considerable disparities in Sub-Saharan Africa (SSA) (13%), East Asia (6%) and South Asia (28%)2. Maternal malnutrition3 and medical conditions like high blood pressure4, diabetes5 and infections6, maternal characteristics like advanced age, multiple pregnancies and short birth intervals7, as well as behavioural factors like smoking and alcohol use can lead to LBW8. LBW can result in numerous short and long term consequences, including increased fetal and neonatal mortality, impaired growth and cognitive development and a higher risk of noncommunicable diseases (NCDs) later in life9,10. Compared to neonates born weighing ≥ 2.5 kg, those born with LBW face a greater risk of mortality, stunting, low IQ levels, adult obesity and NCDs such as heart failure and diabetes8. Additionally, LBW is an indicator of major public health problems, including chronic maternal malnutrition, poor health and insufficient healthcare during pregnancy2,11.
The World Health Organization (WHO) has set an ambitious goal of decreasing LBW by 30% by the year 2025 (later extended to 2030)12. To attain this target, a yearly reduction of 1.9% in LBW globally is required8,13. However, achievements from 2000 to 2020 have fallen far short of this goal. LBW decreased yearly by 1.3% between 2000 and 2004, by 1.4% between 2005 and 2009, by 1% between 2010 and 20158 and by just 0.3% between 2012 and 202013. More focused, consistent and accelerated efforts are required to improve the progress in reducing LBW within the specified timeframe14.
Previous studies indicated that the occurrence of LBW differs by geographic location and socioeconomic background in SSA countries. For example, a recent study analysed from DHS data found that LBW is highly prevalent in Mauritania (25%) and the lowest rate of LBW was reported in Seirra Lione (5%)15. Another study also reported presence of regional difference in LBW in SSA ranging from 4.8 to 25%16. LBW also varied across socioeconomic positions, with higher prevalence observed among women with lower levels of education, those who were unemployed, and those from households with lower wealth status17. However, age related difference in LBW is not conclusive showing a U-shaped relationship between the mother’s age and LBW, signifying an increased risk for LBW in both advanced-age and younger adolescent women18,19. Studies showed that older age is significantly associated with LBW due to preexisting medical conditions, obstetric history and underlaying maternal characteristics20,21. In contrast, teenagers are more likely to have a LBW baby due to unplanned pregnancy, social stigma, lack of prenatal care and not being physically mature enough to become pregnant at a young age22,23,24.
Although several studies have assessed the prevalence and determinants of LBW25,26,27, there is limited evidence assessing the geospatial distribution of LBW and disparities between adolescents and non-adolescents in SSA. Most existing evidence has not analysed LBW using age stratification, which limits the understanding of disparities between adolescent and non-adolescent mothers. Without stratification, important differences in the risk and burden of LBW remain hidden, hindering the development of targeted public health interventions, such as effective resource allocation. To address this gap, the present study used DHS data from SSA countries and applied a range of analytical approaches including concentration curves and indices, absolute and relative difference measures, multilevel modelling, and spatial analysis to comprehensively understand differences in LBW between adolescent and non-adolescent women. These analyses will support policymakers in making informed decisions on resource allocation to enhance maternal and newborn healthcare in the region, contributing significantly to achieving the WHO’s target of a 30% reduction in LBW by 2030. In addition, this kind of advanced statistics is important for formulating interventions and policies that are context- and age-specific, developing interventions for health inequalities and forecasting the problem in other regions to improve birth outcomes.
Materials and methods
Data source
This study used data from the DHS of SSA countries. DHS project is managed by ICF International in Rockville, Maryland, USA and funded by U.S. Agency for International Development (USAID)28. DHS data are nationally representative household surveys conducted every five years. These surveys are conducted for monitoring and evaluating policy impact in various areas, including marriage, fertility, mortality, family planning, reproductive health, maternal and child health, nutrition and HIV/AIDS. The DHS data collected from different countries are comparable, as they use the same tools and methodology across the countries29. There are different records in DHS surveys such as a household record, individual women record, men record, pregnancy record, children record, household member record, biomarker record, HIV record and geographic dataset. For this specific study, the children record (referred to as KR file) and geographic file were utilized as the main data sources. A total of 41 countries (of the 44 countries in the SSA region) have participated in DHS at some point. This study included 33 SSA countries for which DHS data were available for any year between 2010 and 2023. Inclusion of the countries was mainly based on data availability, as some datasets were restricted, and others had no DHS data at all. Additionally, only data released since 2010 were considered for inclusion.
Since some variable names and formats differ between DHS-7 and DHS-8, we used the same dataset type (the KR file) for all countries to ensure comparability across populations. Each country’s data was cleaned independently prior to appending together. These include renaming variables to align them across surveys, removing variables not relevant to the study objectives, and recoding variables with differing categories. Then the datasets were appended to create a pooled dataset. Further data cleaning was conducted, and sampling weights were applied to account for the complex survey design.
Population and sampling techniques
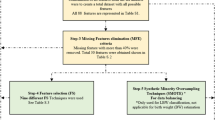
The study participants in DHS were selected using a two-stage stratified cluster sampling. In the first stage, a list of enumeration areas was drawn from the census population of each country using probability sampling proportional to the size of the population in each cluster. The second stage was a sample of the population selected from the total enumeration area. Women who did not have a singleton live birth in the last five years, such as still birth and multiple pregnancy, were excluded from analysis. A weighted sample size of 180,410 women (152,521 non-adolescents and 27,889 adolescents) was included in the analysis. For multilevel analysis, the unit of analysis was individual number of adolescent and non-adolescent women who had history of childbirth in the five years prior to the survey. For the spatial analysis, the unit of analysis was the number of clusters pooled from all countries and the clusters with longitude of zero were excluded as their coordinates do not represent their exact locations. Accordingly, 19,024 clusters were pooled from 33 SSA countries (Fig. 1).

Flowchart of data extraction for age-related disparities and geospatial distribution of LBW in SSA.
Study variables and measurements
Outcome variable
The outcome variable of the study was LBW for the most recent birth, defined by weight < 2500 g at birth (normal birthweight otherwise). The variable LBW was extracted from records measured during delivery generating continuous data25,26.
Stratifier variable
As recommended by the International Center for Equity in Health, age of the women was used as a disparity stratifier variable and categorized as adolescent (15–19 years) and non-adolescent women (20–49 years) for comparing LBW30. In DHS data, a woman’s age was recorded in two ways: age at the time of the survey and age at the time of childbirth. The latter is not directly reported but is calculated by subtracting the mother’s date of birth from the child’s date of birth and dividing by 12 to convert months to years. This derived age reflects the mother’s exact age when the birth happened and was used in our analysis, as it aligns with the timing of the outcome.
Explanatory variables
Several variables were selected as explanatory variables (individual and community level variables) based on the literature23,24 and data availability. Individual level variables include demographic variables such as marital status, education, sex of household head, sex of newborn, wealth index and income categories of the countries. The DHS survey calculated the wealth index using principal component analysis from different indicators and reported five indexes: richest, richer, middle, poorer and poorest. To make the analysis and interpretation simple and clear, the richest and richer were categorized to “rich”, middle to “middle” and poorer and poorest to “poor”. The income categories of countries were classified according to the World Bank economic categories as follows: LIC with a gross national income per capita below $1135, LMIC with incomes ranging from $1136 to $4465, and UMIC with incomes ranging from $4466 to $13,84531. Reproductive-related variables such as pregnancy intention, parity, timing of antenatal care, ANC utilisation, and ANC packages were included as individual level explanatory variables. Moreover, barriers to health care accessibility variables such as distance, money, and permission to seek health facility were used as individual level variables. Community level variables include residence, region where they live (Central, Eastern, Southern, Western Africa) and community media exposure. The classification of “exposed” or “not exposed” to media was based on access to any of newspapers, radio or television. Community media exposure was percentage of women exposed to at least one media32. SSA countries were classified into Central, Eastern, Southern, and Western Africa based on UN geographic classifications33.
Statistical analysis
Data was analysed using STATA software version 18.034 and ArcMap 10.8.235. For all data analysis (concentration index, multilevel analyses and spatial analysis), weighting was performed to ensure the representativeness of the sample. The Pearson’s chi-square test was used to assess differences in the age distribution of women (adolescent and non-adolescent) and outcome variable.
Concentration curve and concentration index
The presence of age-related disparity of LBW was visualized using the concentration curve. The curve was used to illustrate the cumulative percentage of LBW on the y-axis against the cumulative percentage of women on the x-axis, ranked from the youngest to the oldest. The direction of the association between LBW and age disparity is indicated by the line of equality (at 45°), which is positive when the curve falls below the line of equality (LBW is concentrated among non-adolescents) and negative when it falls above the line of equality (LBW is concentrated among adolescents)36. When there is no age-related disparity (perfect equality), the concentration index is zero and the concentration curve lies directly on the line of equality at 45°. Concentration index (CI) was computed to quantify the degree of age-related disparity of LBW among pregnant women37:
where CI is concentration index, yi is LBW, \(\mu - i\) is mean of LBW, Ri is cumulative percentage that each participant represents over the total population after categorizing LBW by the age distribution. Since the outcome variable LBW in this analysis is binary, the limits of CI range between μ − 1 (lower limit) and 1 − μ (upper limit) rather than from − 1 to 1. To address this issue, the study utilized the Erreygers normalized concentration index (ECI), which is a modified version of the generalized concentration index38.
Mathematically
In addition, absolute difference (AD) and relative difference (RD) was computed to compare difference in LBW among adolescent and non-adolescent women in all countries. AD represents the difference in LBW between adolescent and non-adolescent women. When a value of AD is greater than 0, LBW is higher in adolescent and when it is less than 0, LBW is higher in non-adolescent women. RD is the ratio of LBW in adolescent women to non-adolescent women. When the value is greater than 1, LBW is high in adolescent and when it is less than 1, LBW is high in non-adolescent women39.
Multilevel analysis
Both bivariable and multivariable analyses was fitted to assess the effect of individual and community-level factors on LBW. Two level mixed effects model was employed due to hierarchical nature of the DHS sampling procedure and to avoid clustering effects of individual and community level factors on outcome variable. To check the suitability of the multilevel mixed effects model to the DHS dataset, the intra-class correlation (ICC) coefficient which measures the total heterogeneity attributable to community-level factors was done whether the variances of the random part are different from zero over the community-level factors. ICC is the ratio between cluster variance to the total variance. Four models were constructed to run multilevel logistic regression. Null model without any covariates. At this stage, ICC was used to check for the suitability of multilevel analysis40. Model I was fitted to understand the effect of individual-level variables on the LBW and Model II to see the effect of community-level factors on LBW. Finally, Model III was fitted to understand the simultaneous effect of individual and community-level factors on LBW. Proportional change in variance (PCV) was computed to capture the estimated variance between models. The results of fixed effects were interpreted with an adjusted odds ratio (AOR) with a 95% confidence interval (95%CI). The random effect was interpreted using ICC and PCV and compared across the progressive models. Log-likelihood ratio (LLR) was used to compare models with different sets of parameters. The selection of variables for the multivariable analysis depends on the level of significance (p value < 0.25) in bivariable analysis. Variance inflation factor (VIF) was used to assess the presence of multicollinearity among explanatory variables.
Spatial analysis
Spatial analysis was conducted using ArcGIS V.10.6, integrating data from three sources. First, the DHS dataset from 33 countries was obtained from the Measure DHS website, with the main outcome variable being LBW. Second, the geographic coordinates for the same countries were also obtained from the Measure DHS website, converted to Excel format, and then merged with the DHS dataset using v001 as common variable. Third, the DHS spatial boundaries (shapefiles of the African continent) were downloaded and merged with the calculated proportions using ArcMap software. The merged data was projected from World Geodetic System (WGS) 1984 to a sinusoidal projection to comply with spatial statistical requirements. The sinusoidal projection was specifically chosen for its suitability in mapping continents near the equator, such as Africa and South America41,42.
Autocorrelation analysis was employed to assess the pattern of distribution of LBW across the selected countries using Global Moran’s I statistic test. The distribution can be random distribution, clustering effect or dispersion between the clusters43,44. The value of Moran’s I test ranges from − 1 (negative Z-score) which indicates the condition is dispersed to + 1 (positive Z-score) which indicate the LBW is clustered to specific areas. If the value of Moran’s I test is close to 0, the condition is distributed randomly35. After the cluster pattern of LBW was identified by Moran’s I test, a hotspot analysis (Getis-Ord G) was used to identify the areas with the highest and lowest risk of LBW45. The G statistic measures the extent of clustering of either high or low values. A high positive G value signifies the presence of hotspots or areas where high values are concentrated, whereas a significant negative G value highlights cold spots, where low values are densely concentrated. The significance of the G statistic is assessed by z-scores and p values.
Spatial interpolation was mapped to predict LBW in unsampled areas based on data from sampled enumeration areas. The Kriging method was utilized for prevalence of LBW extrapolation, based upon specific assumptions46. The first assumption is that the outcome variable is normally distributed (simple kriging), which is assessed by histograms in ArcGIS47. Second, the variance is assumed to be constant or equally distributed in different areas of the map, which was checked by using Voronoi diagram in ArcGIS48. The third criterion is the absence of trends, evaluated through trend analysis. Ordinary and simple kriging are commonly used interpolation methods. Ordinary kriging does not require the data to be normally distributed, whereas simple kriging assumes a known mean and may require data transformation if the distribution is not normal. We used ordinary Kriging interpolation which does not require the normal distribution of the data47.
Ethics approval
Deakin University granted exemption from ethics review for utilizing the publicly accessible DHS dataset. The data are publicly available in various formats on the Measure DHS website (http://idhsdata.org). We applied for access to the DHS data (both for survey dataset and geographic dataset) by providing the study objectives of our study and received a formal permission letter for access to the SSA countries datasets, which is managed by ICF International in Rockville, Maryland, USA.
Result
Characteristics of participants
A total of 180,410 weighted participants were included in the study. Of these participants, 27,889 (15.5%) were adolescent women, while 152,521 (84.5%) were non-adolescent women at the time of childbirth. Among the adolescent women, 37.4% lived in urban areas, more than 70% of household heads were male, 40.2% were from a poor household, more than half (55.0%) were employed and 69.9% were married. Among the non-adolescent women, 43.1% lived in urban areas, 77.1% of household heads were male, 25.9% had no formal education, 29.9% were unemployed and 25.9% were from Western Africa. The timing of ANC initiation within three months of gestation was low for adolescents 26.7% vs 33.5% in non-adolescent. Lastly, nearly half of adolescent and non-adolescent women were exposed to media, with 47.8% and 50.8% exposed, respectively (Table 1).
LBW disparities among adolescent and non-adolescent women
This study showed that 13.2% of adolescent women have LBW baby, significantly higher than that of non-adolescent women (% of LBW = 8.3% AD = 4.9%, p < 0.001). The concentration curve showed that the line of LBW was lying slightly above the line of equality (CI = − 0.096, p value < 0.001), indicating LBW was modestly concentrated among the disadvantaged group (adolescent women). The results found that there was a statistically significant disparity in LBW between adolescent and non-adolescent women, with the absolute disparities of 4.9%, or LBW is 1.6 times higher in adolescent than non-adolescent women (Fig. 2).

Age-related disparity of LBW in 33 SSA countries Data sources: Demographic and Health Surveys DHS 2010–2023.
The Equiplot was constructed to compare LBW among adolescent non-adolescent women for all countries (Fig. 3). The graph showed that, except two countries (Chad and South Africa), the prevalence of LBW was higher in adolescent women compared to non-adolescent women. The highest rate of LBW in adolescent was observed in Mauritania (25.3%) followed by Gabon (19.0%) and Cote d’Ivoire (17.6%). Seirra Leonne (4.6%), Chad (5.1%) and Cameroon (8.7%) reported the lowest LBW among adolescent women. However, the highest rate of LBW for non-adolescent women was observed in Mauritania (22.4%) followed by South Africa (13.7%) and Mali (13.4%). The lowest rate of LBW among non-adolescent women was reported in Seirra Leone (4.3%), Cameroon (5.2%) and Democratic republic of Congo (5.4%).

Equiplot comparing LBW among babies of adolescent and non-adolescent women. Data sources: Demographic and Health Surveys DHS 2010–2023. Note: The vertical reference line on X -axis shows the pooled LBW at regional level in SSA (9.0%).
When compared to the regional pooled level (9.0%), LBW among adolescent women was generally higher for the majority of the countries (30 countries)while three countries reported LBW below the pooled regional level (Chad, Cameroon, and Seirra Leone). LBW among non-adolescent women was lower than the pooled regional level in most countries (20 countries) and only three countries scored LBW in non-adolescent women below the average regional level (Chad, Cameroon, and Seirra Leone) (Fig. 3).
Thirty-one countries showed a significantly greater absolute difference in LBW among adolescent women compared to non-adolescent women. In contrast, South Africa (− 0.3) and Chad (− 2.0) had lower absolute differences, indicating that LBW was higher among non-adolescent women than adolescent women (Fig. 4A). Regarding relative differences, Liberia, Benin and Togo had the highest RD, with LBW being 2.5, 2.1, and 2 times higher among adolescent women compared to non-adolescent women, respectively. In Chad, the RD was less than 1, with values of 0.7 indicating that LBW among adolescent women was 30% lower compared to non-adolescent women (Fig. 4B).

Absolute disparity of LBW between adolescent and non-adolescent women (4A). Relative disparity of LBW between adolescent and non-adolescent women (4B). Data sources: Demographic and Health Surveys DHS 2010–2023.
Spatial distribution of low birthweight in SSA
The spatial autocorrelation analysi, with Moran’s I test result of − 0.0106 (p value = 0.904) suggests that LBW among adolescent women appears to be randomly distributed across the geographic regions studied in SSA. However, the occurrence of LBW was clustered among non-adolescent women in SSA, with Moran’s I test of 0.99649 (p value < 0.001) (Fig. 5A–D). Further spatial analysis (investigation of clusters) therefore focused only on LBW among non-adolescent women.

Geospatial distribution of LBW among adolescent (A and C) and non-adolescent women (B and D). Data sources: Demographic and Health Surveys DHS 2010–2023 (regions shaded grey were not included in the analysis) (Map was generated using ArcMap 10.8. 235).
The Getis-Ord G hotspot analysis revealed that countries in Western Africa such as Mauritania, Mali, Niger, and Chad were hotspot areas of LBW among non-adolescent women at a 99% CI, while Angola was reported as a hotspot at a 95% CI. Countries like South Africa, Lesotho, Tanzania, Rwanda, Burundi, Uganda, Togo, Ivory Coast, Liberia and Sierra Leone were identified as cold spots at a 99% confidence level (Fig. 6A).

Hotspot analsysis (A) and Kringing interpolation (B) of LBW among non-adolescnt women. (Note-both analysis were not conducted for adolescent women as the distribution of LBW was random). Data sources: Demographic and Health Surveys DHS 2010–2023 (regions shaded grey were not included in the analysis) (Map was generated using ArcMap 10.8.235).
Ordinary Kriging interpolation was used to map the predicted LBW in an unsampled areas of SSA region. LBW was predicted to be high among non-adolescent women in some parts of Western (Niger, Mali and Mautiania), Central (Chad), and Eastern Africa (Ethiopia) (Fig. 6B).
Determinants of LBW among adolescent and non-adolescent women in SSA
Results of random effects model
The ICC was 5.5% among adolescents and 1.9% among non-adolescents, indicating that 5.5% and 1.9% of the total variation in LBW was attributable to differences between clusters, with the remaining variation explained by individual-level factors. Additionally, the PCV decreased across the models, suggesting that the final model was more effective in explaining between-cluster variation. The final model was selected based on its lower LLR and AIC values, indicating a better model fit (Table S1).
Results of fixed effects model
In multivariable multilevel analysis, eleven variables were selected for adolescents and fourteen for non-adolescents (Table 2). Common individual level factors significantly associated with LBW in both groups were women’s education, employment, ANC visits, marital status, and permission to get medical care. Pregnancy intention and age at first sex were significant factors only in adolescent women while parity and distance to health facilities were only significant in non-adolescent women. At community level, region was a significant factor for LBW in both groups.
Among adolescent women, those with no formal education had 16% higher odds of experiencing LBW (AOR = 1.16, 95% CI 1.00, 1.31), while those with only primary education had 27% higher odds (AOR = 1.27, 95% CI 1.17, 1.39), compared to those with secondary or higher education. Among non-adolescent women, lack of formal education and attending primary-level education were associated with 34% (AOR = 1.34, 95% CI 1.26, 1.42) and 18% (AOR = 1.18, 95% CI 1.12, 1.24) increase odds of LBW, respectively. Being single was also associated with increased odds of LBW by 13% among adolescents (AOR = 1.13, 95% CI 1.03, 1.24) and by 11% among non-adolescents (AOR = 1.11, 95% CI 1.02, 1.20).
Unemployed adolescent and non-adolescent women had 1.10 and 1.20 times higher odds of giving birth to LBW baby compared to their employed counterparts (AOR = 1.10, 95% CI: 1.02, 1.19; AOR = 1.20, 95% CI: 1.15, 1.25). Among adolescent women, lack of ANC and incomplete ANC follow-up was associated with 35% and 25% increase in the odds of LBW (AOR = 1.35, 95% CI: 1.23, 1.48) and (AOR = 1.25, 95% CI:1.14, 1.37), respectively. In non-adolescent women, the absence of ANC and incomplete ANC follow-up increased the odds of LBW by 24% (AOR = 1.24, 95% CI: 1.18, 1.30) and 17% (AOR = 1.17, 95% CI: 1.11, 1.24), respectively. Furthermore, adolescent women who reported that obtaining permission to seek medical care as a big problem had 16% higher odds of LBW (AOR = 1.16, 95% CI: 1.05, 1.27), while in non-adolescents, this problem increased the odds of LBW by 15% (AOR = 1.15, 95% CI: 1.09, 1.21). Adolescent women with unintended pregnancies had higher odds of delivering LBW baby compared to those with intended pregnancies (AOR = 1.20; 95% CI: 1.08, 1.48). Similarly, adolescents who initiated sexual activity during late adolescence had reduced odds of LBW compared to those who initiated sexual activity before the age of 18 (AOR = 0.92; 95% CI: 0.88, 0.99).
Among non-adolescent women, the odds of LBW were 1.61 times higher in those with only one live birth compared to those with more than four births (AOR = 1.61, 95% CI: 1.49, 1.72). Women who reported distance of health facility as big problem had 1.08 times higher odds of giving birth to LBW baby (AOR = 1.08, 95%CI: 1.03, 1.13). At the community level, adolescent women from Western Africa had 1.16 times higher odds of having LBW baby compared to those from Southern Africa (AOR = 1.16; 95% CI: 1.03, 1.31). Among non-adolescent women, those from Western and Eastern Africa had 1.20 (AOR = 1.20; 95% CI: 1.12, 1.28) and 1.16 (AOR = 1.16; 95% CI: 1.08, 1.24) times higher odds of LBW, respectively, compared to their counterparts in Southern Africa (Table 2).
Discussion
This study assessed the age-related disparity, determinants and geographical distribution of LBW in SSA using concentration index, multilevel analysis and geospatial analysis. These analyses are crucial to inform decision-makers to develop context- and age-related interventions to reduce LBW across SSA countries. The study revealed a statistically significant disparity in LBW between adolescent and non-adolescent women. LBW was 13.2% among adolescents compared to 8.3% in non-adolescents, with an absolute disparity of 4.9% and a relative disparity of 1.60.
A study in Canada also found similar disparity in LBW, where LBW was 1.56 times higher among adolescents when compared to adults49. Adolescent women face obstacles in accessing adequate prenatal care due to socioeconomic factors, such as poverty50, limited education51 and inadequate healthcare availability52,53, which can result in an increased risk of LBW. Moreover, physiological immaturity and social factors, such as stigma and psychological stress of adolescent pregnancy54, can contribute to LBW among adolescents. It is important to develop and implement targeted interventions that improve healthcare access, education, socioeconomic support and societal attitudes toward adolescent pregnancy to mitigate these disparities.
In this study, high maternal education level is a protective factor for LBW both in adolescent and non-adolescent women. The finding is in line with studies conducted in different settings such as LMIC55, India56,57, USA58, Italy59, and multicounty study60. This shows the importance of maternal education in preventing maternal and neonatal birth outcomes regardless of age of the women. This possibly due to educated mother knows the importance of attending ANC, had higher autonomy in decision making, seeking healthcare, and establishing healthy social and family support. To reduce the burden of LBW, efforts should prioritize improving female education, particularly among adolescents as higher educational attainment is associated with increased health literacy, better ANC utilization, and delayed childbearing. In addition, integrating reproductive health education into primary or secondary school curricula can empower young women with the knowledge and skills necessary for healthy pregnancies.
Giving single live birth and early initiation of sexual intercourse are a risk factor for LBW which is supported by studies done in different settings61,62. The importance of parity and early sexual initiation in influencing LBW could be due to complications associated with a first-time pregnancy that increase the likelihood of LBW, particularly among adolescent mothers63. Early sexual activity and early childbirth mainly happen during adolescent period often under circumstances where individuals may not be adequately informed or prepared64. This suggests the importance of targeted programs in promoting delayed sexual initiation and contraceptive utilisation during the early age to reduce the risk of early pregnancies and associated complications leading to LBW. This underscores that interventions targeting early age of the women could have lasting effects on their subsequent births when they become adults.
In both adolescents and non-adolescents, lack or incomplete ANC follow up increase the likelihood of LBW regardless of the age of the women. This is supported by studies conducted in LMIC55, SSA26, Indonesia65, and Bangladesh66. This is attributed to the absence of early screening and treatment for adverse birth outcomes, lack of continuous follow-up for pregnancy-related disorder, lack of counselling and education, and inadequate preparation for delivery among women who receive incomplete or no ANC follow-up. Therefore, raising awareness and promoting the importance of ANC follow-up should be continuously given for all pregnant women, regardless of their age in the region.
The finding that unmarried associated with the odds of LBW among adolescent and non-adolescent highlights that unmarried women may lack support and resources from husband and family67, hindering healthcare access and prenatal support68. Addressing these barriers is crucial to support unmarried adolescent mothers and improve birth outcomes. Employment showed 90% and 80% protective factors against LBW among adolescent and non-adolescent women, respectively. The significance of socio-economics status such as unemployment increasing the odds of LBW underlines the importance of addressing economic challenges in improving birth outcomes. Unemployed women may have limited access to healthcare, including prenatal care and regular medical follow-up69. Therefore, addressing economic challenges such as employment is essential for reducing LBW rates among adolescent and non-adolescent women.
Women who reported presence of big problem in obtaining permission to visit a healthcare facility had higher odds of giving birth to LBW baby in both groups. This associated with lack of autonomy and lack of involvement in decision-making during pregnancy and childbirth which negatively affect birth outcomes70. Therefore, enhancing women’s education, providing financial support, and focusing on rural women could help alleviate the challenges associated with autonomy and decision-making.
Untended pregnancy increases the likelihood of LBW by 20% in adolescent women. The finding is aligns with previous studies conducted in Ethiopia71, low income settings72 and Iran73. This attributed to lack of early and regular ANC follow up in adolescents, which is critical for monitoring fetal growth and addressing pregnancy complications. Additionally, women with unplanned pregnancies may have lower levels of birth preparedness and complication readiness, increasing the risk of adverse birth outcomes74. Therefore, this finding highlights the importance of preventing unintended pregnancies as a strategy to reduce LBW among adolescent women.
Although LBW disproportionately affects adolescent women in SSA, our findings reveal a random spatial distribution of LBW among adolescents, in contrast to the clustered patterns observed among non-adolescent women in certain countries. This suggests that adolescent women across SSA may face similar risk factors, and that region-wide interventions specifically targeting this group remain limited. Shared socio-economic challenges like poverty, early marriage, limited access to education and healthcare, and weak parental support are common among adolescent girls in SSA, contributing to this uniform distribution75. Additionally, issues like gender-based violence, substance abuse, low access to reproductive health services, and inadequate sexual health education are prevalent in the region and exacerbate the risk of LBW76.
Among non-adolescent women, those residing in Western and Eastern Africa had significantly higher odds of delivering LBW baby compared to women in Southern Africa. This regional disparity is further supported by the spatial analysis, which identified Western Africa as a significant hotspot for LBW. Countries in Western Africa including Mauritania, Mali, Niger, and Chad were identified as hotspot areas for LBW among non-adolescent women. This finding is consistent with previous research from SSA, which also reported high LBW prevalence in these countries16,26,77. For example, Mauritania has been highlighted as one of the regions with the highest LBW burden78. The consistency between the multilevel and spatial analyses suggests that contextual and structural factors at the regional level may play a critical role in shaping LBW. Studies conducted in SSA found that the number of ANC visit and adequacy of maternal service utilisation is relatively low in this region compared to countries listed as cold spot areas for LBW such as South Africa and Lesotho79,80. In addition, study done by Nyarko S.H. identified Western Africa as a hotspot areas for anaemia during pregnancy42, which may contribute to high LBW in this region. A study reported a steady rise in LBW rates in Western Africa between 2000 and 2020, largely attributed to persistent maternal undernutrition77. These findings highlight the importance of geographically targeted interventions and policies to address regional inequalities of LBW across SSA. Addressing the high burden of LBW in Western Africa requires both short and long-term strategies. In the short term, expanding access to prenatal care and increasing awareness about maternal health are essential. In the long term, efforts should focus on improving strengthening women’s empowerment and enhancing nutritional and economic opportunities for women to sustainably reduce LBW in the region.
Strength and limitations of the study
The strength of this study was employing multiple analyses to understand disparity, distribution and determinants of LBW, along with utilizing a large dataset from 33 countries, easing the generalization of findings for the SSA region. However, some of the limitations of this study are firstly, incomplete data and unmeasured birthweights, which may lead to underestimation or overestimation of LBW prevalence in the region. Secondly, LBW distribution is assessed at the country level, indicating cautious interpretation as specific districts with high LBW concentrations within each country remain unidentified. Future researchers should assess the distribution of LBW at district level and the contextual factors influencing LBW in countries where it is prevalent, especially among non-adolescent women. While we assessed LBW differences by country, the contributing factors may differ by context. Future research should explore country-specific drivers of LBW among adolescent and non-adolescent women. Although we carefully followed all recommended steps to merge data from different rounds of DHS (DHS 7 and DHS 8), and the merging process is unlikely to have significantly affected the analysis, caution is still needed when interpreting and generalizing the findings.
Conclusion and recommendation
Our findings reveal that adolescent mothers bear a disproportionate burden of LBW across SSA. Furthermore, spatial analysis identified random distribution of LBW among adolescent women, but clustered in Mauritania, Mali, Niger, and Chad for non-adolescent women highlighting the presence geographic disparities. This underscores the need to focus on improving maternal education, employment opportunities and access to ANC for women as a key intervention to reduce age-related disparities, with equitable allocation of resources between adolescents and non-adolescents to mitigate the burden of LBW and improve wellbeing of women and neonates. Additionally, we recommend that policymakers prioritize strategies to prevent unintended pregnancies and postpone adolescent pregnancies, as these measures could significantly improve wellbeing of adolescent women. Random distribution of LBW in adolescent women underscores the need for adolescent-specific regional interventions that address the unique need of adolescent mothers across SSA.
Data availability
The data are publicly available in various formats on the Measure DHS website (http://idhsdata.org).
Abbreviations
- ANC:
-
Antenatal care
- CI:
-
Confidence interval
- DHS:
-
Demographic health survey
- LBW:
-
Low birthweight
- LIC:
-
Lower income countries
- LMIC:
-
Lower middle-income countries
- NCDs:
-
Non-communicable DISEASES
- SSA:
-
Sab-Saharan Africa
- UMIC:
-
Upper middle income countries
- WHO:
-
World Health Organization
- VIF:
-
Variance inflation factor
References
World Health Organisation (WHO). Low Birth Weight (2025).
World Health Organization (WHO). Global Nutrition Targets 2025: Low Birth Weight Policy Brief (World Health Organization, 2014).
da Silva Lopes K, Ota, E., Shakya, P. et al. Effects of nutrition interventions during pregnancy on low birth weight: An overview of systematic reviews. BMJ Glob. Health 2(3), e000389 (2017).
Lim, W.Y., Lee, Y.S., Tan, C.S. et al. The association between maternal blood pressures and offspring size at birth in Southeast Asian women. BMC Pregnancy Childbirth 14(1), 403 (2014).
Kong, L., Nilsson, I.A., Gissler, M. et al. Associations of maternal diabetes and body mass index with offspring birth weight and prematurity. JAMA Pediatr. 173(4), 371–378 (2019).
Xiao, P.L., Zhou, Y.B., Chen, Y. et al. Association between maternal HIV infection and low birth weight and prematurity: A meta-analysis of cohort studies. BMC Pregnancy Childbirth 15(1), 246 (2015).
Pusdekar, Y.V, Patel, A.B., Kurhe, K.G. et al. Rates and risk factors for preterm birth and low birthweight in the global network sites in six low-and low middle-income countries. Reprod. Health 17, 1–16 (2020).
World Health Organization (WHO). UNICEF-WHO Low Birthweight Estimates: Levels and Trends 2000–2015 (World Health Organization, 2019).
Reyes, L. & Manalich, R. Long-term consequences of low birth weight. Kidney Int. 68, S107–S111 (2005).
Gupta, N. D., Deding, M. & Lausten, M. The effect of low birth weight on height, weight and behavioral outcomes in the medium-run. Econ. Hum. Biol. 11(1), 42–55 (2013).
Muthayya, S. Maternal nutrition & low birth weight-what is really important. Indian J. Med. Res. 130(5), 600–608 (2009).
UNICEF and World Health Organization (WHO). Country consultation on low birthweight and preterm birth estimates. In Tecnical Note (2022).
UNICEF. Low Birth Weight. In Unicef for Every Child (2023).
World Health Organization (WHO). UNICEF/WHO Low Birthweight Estimates: levels and trends 2000–2020 (World Health Organization, 2023).
Geberu, D.M., Baffa, L.D., Hagos, A. et al. Pooled prevalence and factors of low birth weight among newborns in the top 20 countries with the highest infant mortality: Analysis of recent demographic and health surveys. BMJ Open 15(4), e098090 (2025).
Mare, K.U., Andarge, G.G., Sabo, K.G. et al. Regional and sub-regional estimates of low birth weight and its determinants in 44 low-and middle-income countries: Evidence from demographic and health survey data. BMC Pediatr. 25(1), 342 (2025).
Ngandu, C.B., Momberg, D., Magan, A. et al. The association between household socio-economic status, maternal socio-demographic characteristics and adverse birth and infant growth outcomes in sub-Saharan Africa: A systematic review. J. Dev. Orig. Health Dis. 11(4), 317–334 (2020).
Aras, R. Y. Is maternal age risk factor for low birth weight?. Arch. Med. Health Sci. 1(1), 33–37 (2013).
Restrepo‐Méndez, M.C., Lawlor, D.A., Horta, B.L. et al. The association of maternal age with birthweight and gestational age: A cross-cohort comparison. Paediatr. Perinat. Epidemiol. 29(1), 31–40 (2015).
Kusrini, I., Supadmi, S., Mulyantoro, D.K. et al. Demographic characteristics of mother as predictor of low birth weight in Eastern Indonesia. Syst. Rev. Pharm 12(1), 1514–1518 (2021).
Goisis, A,, Remes, H., Barclay, K. et al. Advanced maternal age and the risk of low birth weight and preterm delivery: A within-family analysis using Finnish population registers. Am. J. Epidemiol. 186(11), 1219–1226 (2017).
Guimarães, A.M., Bettiol, H., Souza, L.D. et al. Is adolescent pregnancy a risk factor for low birth weight?. Rev. Saude Publica 47, 11–19 (2013).
Mousumi, G. Association of maternal age and low socio-economic status of women on birth outcome. Int. Res. J. Soc. Sci. 3(10), 21–27 (2014).
Vieira, C.L., Coeli, C.M., Pinheiro, R.S. et al. Modifying effect of prenatal care on the association between young maternal age and adverse birth outcomes. J. Pediatr. Adolesc. Gynecol. 25(3), 185–189 (2012).
Tessema, Z.T., Tamirat, K.S., Teshale, A.B. et al. Prevalence of low birth weight and its associated factor at birth in Sub-Saharan Africa: A generalized linear mixed model. PLoS ONE 16(3), e0248417 (2021).
Weyori, A.E., Seidu, A.A., Aboagye, R.G. et al. Antenatal care attendance and low birth weight of institutional births in sub-Saharan Africa. BMC Pregnancy Childbirth 22(1), 283 (2022).
Feresu, S.A., Harlow, S.D., Woelk, G.B. Risk factors for low birthweight in Zimbabwean women: A secondary data analysis. PLoS ONE 10(6), e0129705 (2015).
ICF. Demographic and Health Survey (DHS) Manuals (2017).
Alam, N., Hajizadeh, M., Dumont, A. et al. Inequalities in maternal health care utilization in sub-Saharan African countries: A multiyear and multi-country analysis. PLoS ONE 10(4), e0120922 (2015).
Pelotas, F.U.o. International center for equity in health. BMC Pregnancy and Childbirth. https://equidade.org/home (2020).
World Bank. World Bank Country and Lending Groups. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (2022).
Chintsanya, J., DHS Working Papers (2013).
(UN), U.N. United Nations Statistics Division (UNSD). Standard country or area codes for statistical use (M49). https://unstats.un.org/unsd/methodology/m49/. https://unstats.un.org/unsd/methodology/m49/.
Kohler, U. & Kreuter, F. Data Analysis Using Stata (Stata Press, 2005).
Scott, L. M. & Janikas, M.V. Spatial statistics in ArcGIS. In Handbook of applied spatial analysis: Software tools, methods and applications 27–41 (Springer, 2009).
O'Donnell, O., O'Neill, S., Van Ourti T. et al. Conindex: Estimation of concentration indices. Stata J. 16(1), 112–138 (2016).
Koolman, X. & Van Doorslaer, E. On the interpretation of a concentration index of inequality. Health Econ. 13(7), 649–656 (2004).
Erreygers, G. Correcting the concentration index. J. Health Econ. 28(2), 504–515 (2009).
van Zon, S.K., Bültmann, U., Mendes de Leon CF. et al. Absolute and relative socioeconomic health inequalities across age groups. PLoS ONE 10(12), e0145947 (2015).
Peugh, J. L. A practical guide to multilevel modeling. J. Sch. Psychol. 48(1), 85–112 (2010).
ArcMap. Coordinate systems, map projections, and transformations. https://pro.arcgis.com/en/pro-app/3.1/help/mapping/properties/sinusoidal.htm#:~:text=The%20sinusoidal%20projection%20is%20appropriate,on%20their%20own%20central%20meridians.
Nyarko, S.H., Boateng, E.N., Dickson, K.S. et al. Geospatial disparities and predictors of anaemia among pregnant women in Sub-Saharan Africa. BMC Pregnancy Childbirth 23(1), 743 (2023).
Tsai, P.J., Lin, M.L., Chu, C.M. et al. Spatial autocorrelation analysis of health care hotspots in Taiwan in 2006. BMC Public Health 9, 1–13 (2009).
Fortin, M.-J. & Dale, M. R. Spatial autocorrelation. In The SAGE handbook of spatial analysis 89–103 (2009).
Sánchez-Martín, J.-M., Rengifo-Gallego, J.-I. & Blas-Morato, R. Hot spot analysis versus cluster and outlier analysis: An enquiry into the grouping of rural accommodation in Extremadura (Spain). ISPRS Int. J. Geo Inf. 8(4), 176 (2019).
Geography, G., Kriging Interpolation–The Prediction Is Strong in this One. Dostopno na: https://gisgeography.com/kriging-interpolation-prediction/ ogled, 2019. 5.
Kaymaz, I. Application of kriging method to structural reliability problems. Struct. Saf. 27(2), 133–151 (2005).
Feng, X. & Murray, A. T. Allocation using a heterogeneous space Voronoi diagram. J. Geogr. Syst. 20, 207–226 (2018).
DeMarco, N., Twynstra, J., Ospina, M.B. et al. Prevalence of low birth weight, premature birth, and stillbirth among pregnant adolescents in Canada: a systematic review and meta-analysis. J. Pediatr. Adolesc. Gynecol. 34(4), 530–537 (2021).
Chaibva, C. N., Ehlers, V. J. & Roos, J. H. Midwives’ perceptions about adolescents’ utilisation of public prenatal services in Bulawayo, Zimbabwe. Midwifery 26(6), e16–e20 (2010).
Michael, T. O., Nwokocha, E. E. & Agbana, R. D. Issues in antenatal care services utilization among unmarried adolescents in Akwa Ibom State, Nigeria. J. Popul. Soc. Stud. 31, 359–380 (2023).
Miteniece, E., Pavlova, M., Rechel, B. et al. Barriers to accessing adequate maternal care in Latvia: A mixed-method study among women, providers and decision-makers. Health Policy 123(1), 87–95 (2019).
Herwansyah, H., Czabanowska, K., Kalaitzi, S. et al. The utilization of maternal health services at primary healthcare setting in Southeast Asian Countries: A systematic review of the literature. Sex. Reprod. Healthc. 32, 100726 (2022).
Sebők-Welker, T., Posta, E., Ágrez, K. et al. The Association Between Prenatal Maternal Stress and Adolescent Affective Outcomes is Mediated by Childhood Maltreatment and Adolescent Behavioral Inhibition System Sensitivity (Child Psychiatry & Human Development, 2023).
Mahumud, R. A., Sultana, M. & Sarker, A. R. Distribution and determinants of low birth weight in developing countries. J. Prev. Med. Public Health 50(1), 18–28 (2017).
Khan, N., Mozumdar, A. & Kaur, S. Determinants of low birth weight in India: An investigation from the National Family Health Survey. Am. J. Hum. Biol. 32(3), e23355 (2020).
Mumbare, S.S., Maindarkar, G., Darade, R. et al. Maternal risk factors associated with term low birth weight neonates: A matched-pair case control study. Indian Pediatr. 49(1), 25–28 (2012).
Martinson, M. L. & Choi, K. H. Low birth weight and childhood health: The role of maternal education. Ann. Epidemiol. 39, 39–45 (2019).
Cantarutti, A., Franchi, M., Monzio Compagnoni M. et al. Mother’s education and the risk of several neonatal outcomes: An evidence from an Italian population-based study. BMC Pregnancy Childbirth 17(1), 221 (2017).
Silvestrin, S., da Silva, C.H., Hirakata, V.N. et al. Maternal education level and low birth weight: a meta-analysis. Jornal de Pediatria (Versão em Português) 89(4), 339–345 (2013).
Taywade, M. & Pisudde, P. Study of sociodemographic determinants of low birth weight in Wardha district, India. Clin. Epidemiol. Global Health 5(1), 14–20 (2017).
Sharma, S.R., Giri, S., Timalsina, U., Bhandari, S.S. et al. Low birth weight at term and its determinants in a tertiary hospital of Nepal: A case-control study. PLoS ONE 10(4), e0123962 (2015).
Ursache, A., Lozneanu, L., Bujor, I. et al. Epidemiology of adverse outcomes in teenage pregnancy—A northeastern Romanian tertiary referral center. Int. J. Environ. Res. Public Health 20(2), 1226 (2023).
World Health Organization (WHO). Contraceptive Use at First Sex Agency, Consent, and Coercion: Young People’s Experiences of First Sex in Ashanti and Northern Regions, Ghana (QRS24). In An Analysis Brief from The DHS Program (2022).
Siramaneerat, I., Agushybana, F. & Meebunmak, Y. Maternal risk factors associated with low birth weight in Indonesia. The Open Public Health J. 11(1) (2018).
Khan, J.R., Islam, M.M., Awan, N. et al. Analysis of low birth weight and its co-variants in Bangladesh based on a sub-sample from nationally representative survey. BMC Pediatr. 18(1), 100 (2018).
Merklinger-Gruchala, A. & Kapiszewska, M. Marital status, father acknowledgement, and birth outcomes: Does the maternal education matter?. Int. J. Environ. Res. Public Health 20(6), 4868 (2023).
Shah, M. K., Gee, R. E. & Theall, K. P. Partner support and impact on birth outcomes among teen pregnancies in the United States. J. Pediatr. Adolesc. Gynecol. 27(1), 14–19 (2014).
Banke-Thomas, O. E., Banke-Thomas, A. O. & Ameh, C. A. Factors influencing utilisation of maternal health services by adolescent mothers in Low-and middle-income countries: A systematic review. BMC Pregnancy Childbirth 17(1), 65 (2017).
Shome, S., Pal, M. & Bharati, P. Influence of maternal autonomy and socioeconomic factors on birth weight of infants in India. Malays. J. Nutr. 24(1), 35–46 (2018).
Wado, Y. D., Afework, M. F. & Hindin, M. J. Effects of maternal pregnancy intention, depressive symptoms and social support on risk of low birth weight: a prospective study from southwestern Ethiopia. PLoS ONE 9(5), e96304 (2014).
Hall, J.A., Barrett, G., Copas, A. et al. Reassessing pregnancy intention and its relation to maternal, perinatal and neonatal outcomes in a low-income setting: A cohort study. PLoS ONE 13(10), e0205487 (2018).
Omani-Samani, R., Ranjbaran, M., Mohammadi, M. et al. Impact of unintended pregnancy on maternal and neonatal outcomes. J. Obstet. Gynecol. India 69(2), 136–141 (2019).
Exavery, A., Kanté, A.M., Hingora, A. et al. How mistimed and unwanted pregnancies affect timing of antenatal care initiation in three districts in Tanzania. BMC Pregnancy Childbirth 13(1), 35 (2013).
Ajayi, A.I., Athero, S., Muga, W. et al. Lived experiences of pregnant and parenting adolescents in Africa: A scoping review. Reprod. Health 20(1), 113 (2023).
Maharaj, N. R. Adolescent pregnancy in sub-Saharan Africa—A cause for concern. Front. Reprod. Health 4, 984303 (2022).
Dwomoh, D., Sewor, C., Mohammed, S.A. et al. Secular trends in low birth weight and child undernutrition in West Africa: evidence from complex nationwide surveys, 1985–2019. Public Health Nutr. 25(9), 2358–2370 (2022).
Ahinkorah, B.O., Amadu, I., Seidu, A.A. et al. Prevalence and factors associated with the triple burden of malnutrition among mother-child pairs in Sub-Saharan Africa. Nutrients 13(6), 2050 (2021).
Habte, A., Hailegebreal, S. & Simegn, A. E. Predictors of maternal health services uptake in West African region: A multilevel multinomial regression analysis of demographic health survey reports. Reprod. Health 21(1), 45 (2024).
Fenta, S.M., Fenta, H.M., Yilema, S.A. et al. Individual and community-level factors associated with adequate antenatal care service utilization in sub-Saharan Africa. Trop. Med. Health 52(1), 70 (2024).
Acknowledgements
We would like to extend our sincere gratitude to the Deakin University Postgraduate Research Scholarship (DUPRS) for sponsoring this PhD project. The authors would like to thank the DHS program for letting us use the DHS dataset for this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
TT, JAO, and LG involved in the inception and design of the study. TT, JAO, and EHL participated in the analysis and interpretation of the result. TT, JAO, LG and EHL involved in developing the initial drafts of the manuscript and revising subsequent drafts. TT, JAO, LG, and MD prepared the final draft of the manuscript. All authors read and approved the final draft of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tolossa, T., Gold, L., Lau, E. et al. Age-related disparities and spatial distribution of low birthweight in sub-Saharan Africa: using data from demographic and health survey. Sci Rep 15, 34068 (2025). https://doi.org/10.1038/s41598-025-14614-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-14614-8
