
Abstract
Despite increased screening efforts and accessibility of healthcare services, the prevalence of chronic disease is on the rise in Singapore. Digital technology has become a valuable tool to aid management of chronic diseases. However, its utilisation remains challenging among older Singaporeans. Our study aims to explore the barriers and facilitators to the use of digital technology for chronic disease management among middle-aged and older adults in Singapore using the Unified Theory of Acceptance and Use of Technology (UTAUT) model. A population-based cross-sectional survey was conducted among Singaporeans and Permanent Residents aged 45–99 years, who provided informed consent. Interviewers conducted surveys in 14 blocks in District 22 (Jurong West). The questionnaire utilised the UTAUT model and included sociodemographic data. A total of 306 valid responses were analysed. For a good perception of digital technology, increasing age (OR = 0.961; 95%CI: 0.930–0.998, p = 0.038) is a significant barrier while having a tertiary-level education is a significant facilitator (OR = 2.52; 95%CI 1.18–5.38, p = 0.02). Regarding usage of digital technology, higher income (OR = 2.49; 95%CI: 1.15–5.40, p = 0.021), good performance expectancy (OR = 1.21; 95%CI:1.08–1.36, p = 0.001) and social influence (OR = 1.20; 95%CI:1.10–1.31, p = < 0.001) were the significant facilitators. Education, age, income, access to technology, marital status and perception of technology significantly influence digital technology usage for chronic disease management. Such demographic implications should be considered by policy makers to enhance the usage profile of digital health technologies. Future research could investigate the specific causes for the current trends observed, and explore potential interventions to increase adoption of technology among older adults.
Similar content being viewed by others

Introduction
Chronic diseases are defined as conditions lasting 1 year or longer which require continuous medical care and/or limit activities of daily living1. The World Health Organisation estimates that chronic diseases cause 74% of all deaths globally2, revealing their threat to individual health and global public health infrastructure.
In Singapore, 82.2% of older adults suffer from chronic diseases and the number with three or more chronic diseases has nearly doubled from 2009 (20%) to 2017 (38%)3. Furthermore, the estimated annual healthcare cost for patients in Singapore with multimorbidity was almost twice that of patients without (SGD683 vs. SGD344) in 20174.
Older adults face significant barriers to healthcare access5,6,7, and unmet health needs leading to faster disease progression8,9,10,11,12,13, increased hospitalisation rates, and higher healthcare costs6,7,8. Socioeconomic status, education level, and digital literacy play a crucial role in healthcare engagement and technology adoption, particularly among elderly populations. Research has shown that lower-income and less-educated older adults experience reduced access to digital health solutions, further exacerbating disparities in chronic disease management14. Although previous studies have indicated that older adults exhibit lower rates of healthcare technology adoption, these barriers are modifiable through targeted interventions, such as tailored digital literacy programmes, financial assistance for technology access, and blended care models that combine traditional in-person visits with telehealth options9,10,12,13,14. Given the rising prevalence of multimorbidity in ageing populations, a comprehensive strategy that integrates social, technological, and economic considerations is essential to mitigating the physical, psychological, and financial burden on patients, caregivers, and the healthcare system.
Digital health technologies encompass a broad range of tools designed to improve healthcare access, delivery, and management. These include mobile health applications, wearable devices, electronic health records, remote monitoring tools, artificial intelligence-driven decision support systems, and telehealth platforms. Such innovations facilitate personalised healthcare interventions, remote patient monitoring, and real-time health data tracking, thereby enhancing convenience, accessibility, and chronic disease management15. In Singapore, digital health platforms like HealthHub, OneNUHS, and Doctor Anywhere play a critical role in healthcare transformation. HealthHub serves as a national health portal that consolidates medical records and appointment scheduling, while OneNUHS enhances patient engagement within the National University Health System. Meanwhile, Doctor Anywhere provides a teleconsultation service, enabling patients to access medical advice, prescriptions, and follow-ups remotely. These platforms exemplify how digital health solutions are integrated into Singapore’s healthcare ecosystem, supporting both preventive care and chronic disease management. Yet, concerns over privacy, confidentiality and security remain16. Older Singaporeans may also prefer face-to-face interaction, perceiving technology as unnecessary11. Thus, knowledge regarding perception may be crucial to improve the usage of digital health technologies in Singapore.
The Unified Theory of Acceptance and Use of Technology (UTAUT) integrates eight established models, including the Technology Acceptance Model (TAM) and Diffusion of Innovations (DOI), making it a comprehensive framework for studying technology adoption17. While models like TAM and DOI primarily focus on individual perceptions (e.g., ease of use, usefulness), UTAUT extends this by incorporating social and organisational influences, such as clinician recommendations and system-level support. Moreover, the original UTAUT model incorporates four key determinants—performance expectancy, effort expectancy, social influence, and facilitating conditions—which are particularly relevant in understanding digital technology adoption among older adults with chronic diseases. Given that our study focuses on the interplay between sociodemographic factors and digital technology acceptance, rather than behavioural extensions like hedonic motivation or habit (which are emphasised in UTAUT2)18, the original UTAUT framework was deemed the most appropriate. The UTAUT has been validated by multiple studies to evaluate perception towards digital health technology18,19,20,21,22,23. It identifies four key moderating variables and four direct determinants that affect perception and digital technology use (Fig. 1).

A summary of the link between sociodemographic factors and actual usage of digital technology with reference to the Unified Theory of Acceptance and Use of Technology (UTAUT) model (8).
Given Singapore’s ageing population and the growing burden of chronic disease management, UTAUT is well-suited to assessing how older adults adopt digital health technologies by accounting for infrastructure, technical support, and policy frameworks—key factors in Singapore’s structured healthcare ecosystem. Its broader scope allows for a more holistic analysis of facilitators and barriers, making it a stronger choice than alternative models for this study. The UTAUT provides a comprehensive framework to assess how older adults interact with digital health technologies. The model allows us to capture not only individual beliefs but also broader system-level facilitators and barriers, making it a more robust choice than alternative models for this study.
While technology offers promising solutions to improve medical outcomes and reduce healthcare costs, the usage of technologies among older adults could prove challenging. Within Singapore, studies about perception and usage of digital health technologies have rarely been specific to chronic disease management. Since the use of technology is often intertwined with social determinants, there is a need for focused research within Singapore’s middle-aged and elderly population.
Our study thus aims to explore the barriers and facilitators to the use of digital technology for chronic disease management in middle-aged and older adults using the UTAUT model in Singapore. We hypothesise that factors including higher education level, younger age, higher socio-economic status, and frequent access to technology are associated with better perception of and increased usage of digital health technologies for chronic disease management.
Methods
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Study design and setting
A population-based cross-sectional survey was designed by Yong Loo Lin School of Medicine students, and conducted at Jurong West Streets 71, 81, 91, 92, and 93 under faculty supervision, between December 2023 - January 2024.
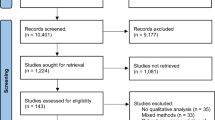
Random sampling without replacement was employed to generate the blocks to be visited. Housing and Development Board (HDB) blocks were enumerated, where 54% were randomly selected. Of 26 blocks (2,352 units), initial randomised generation selected 14 blocks (1410 units). Within these blocks, one eligible resident per unit was selected to participate. Out of 1410 units, 570 units had no response after 2 attempts and 457 units rejected being interviewed. The resulting 383 units attempted the questionnaire. 17 participants did not meet the age inclusion criteria, 20 participants had no comorbidities, and 40 participants gave incomplete responses. Consequently, 306 valid responses were collected (Fig. 2).

Flowchart of Sampling Procedure.
Our inclusion criteria included: (1) Singaporeans and Permanent Residents aged 45–99 (2) Able to provide informed consent (3) Able to complete the questionnaire (4) At least 1 chronic disease. Exclusion criteria included: (1) Cognitively impaired, scoring < 4 in the Abbreviated Mental Test (AMT-4) administered at interviewers’ discretion.
This cross-sectional study employed voluntary sampling through an electronic face-to-face one-time self-administration anonymised questionnaire, precluding interviewer assistance unless required. Notification letters were distributed to residents informing them about the study. The questionnaires were administered 2 weeks later on both weekday nights and weekends to maximise accessibility of participants. Households with residents unavailable at time of visit were tracked and revisited within a week.
This study was conducted in accordance with relevant ethical guidelines and was approved by the Saw Swee Hock School of Public Health Departmental Ethics Review Committee (Reference number: SSHSPH-202). Responses were collected through an anonymised, self-administered, electronic questionnaire, ensuring that no personally identifiable information was recorded at any stage. Informed consent was obtained before participation, and participants were explicitly informed that their responses would remain anonymous. Participants had the right to withdraw at any time, and any incomplete responses were automatically removed from analysis to maintain data integrity. All questionnaires were administered in English, and real-time clarifications in other languages were provided by the multilingual study team when needed. Collected data was securely stored on an encrypted server and was only accessible to authorised researchers involved in the study. No raw data containing potential identifiers was shared outside the research team.
Questionnaire
The questionnaire designed to be completed within 15 min, consists of 31 questions split into five sections.
Section 1 collected socio-demographic data: Sex, Marital Status, Age, Ethnicity, Highest Education Qualification, Employment Status, Average Monthly Household Income, Type of Housing, Access to Technology.
Section 2 assessed comorbidity status and digital technology platforms used to manage comorbidities. Comorbidity status was assessed using a self-reported measure, where participants indicated whether they had been diagnosed with one or more chronic conditions (e.g., diabetes, hypertension, cardiovascular disease) without specifying individual conditions. This section further measured participant confidence in managing comorbidity through a 10-point Likert Scale. Questions were adapted from the validated Self-Efficacy to Manage Chronic Disease (SEMCD) questionnaire24,25.
Sections 3, 4 and 5 were questions modified from the 3 domains of the UTAUT model: Performance Expectancy (PE), Effort Expectancy (EE) and Social Influence (SI), assessing the applicability and perceptions of digital health technologies17. Questions were constructed with a 5-point Likert scale ranging from “Strongly Agree” to “Strongly Disagree”.
Minor adaptations were made to the UTAUT and SEMCD instruments to enhance feasibility and contextual relevance. These included simplifying Likert scale responses from 7 to 5 points and condensing the 6-item SEMCD questionnaire into a 5-item by omitting the item on physical pain. The rationale for this exclusion was that the domain of physical discomfort was less relevant to the chronic diseases and digital health interventions explored in this population. These author-led modifications were not formally validated or endorsed by the original developers. All modifications are reported here for transparency and reproducibility.
The study relied on voluntary participation. The AMT-4 was administered at interviewers’ discretion excluding potential participants with cognitive limitations.
Selected demographics were grouped into categories to ensure even distribution. Marital status was grouped into “Married” and “Unmarried” (“Widowed”, “Divorced” and “Single”). Ethnicity was categorized as “Chinese” and “Non-Chinese” (“Malay”, “Indian”, and “Others”). Education was split into “Primary School or less” (“No education” and “Primary School”), “Secondary school” and “Tertiary” (“Junior College”, “NITEC”, “Diploma”, “Degree”). Employment was grouped into “Employed” (“Employed (Full Time)” and “Employed (Part Time)”), “Unemployed” (“Unemployed and seeking employment”, “Unemployed and not seeking employment”, “Student”) and “Retired”. Income was categorized as “<$3000” and “≥$3000” (“$3000–7000” and “≥$7000”). Number of comorbidities was split into “1–2 conditions” and “≥3 conditions” (“3–4 conditions” and “≥6 conditions”). The remaining variables were ungrouped and kept as raw responses.
Statistical analysis
From our data, we calculated a Management Score (maximum 50) based on five questions from the SEMCD scale to evaluate respondents’ confidence in managing their comorbidities. We also calculated an Impression score based on the 14 UTAUT model questions of 5 points each (maximum 70), which has 3 domains - PE (4 questions), EE (5 questions) and SI (5 questions). The Impression score (binary variable) was used to evaluate respondents’ perception of digital health technology overall, with a “Good Impression” defined as scoring ≥ 56 out of 70 for the UTAUT model. For each domain, Domain Impression Scores were also calculated with “Good Impression” defined as ≥ 16 out of 20 for PE, and ≥ 20 out of 25 each for EE and SI.
Usage of digital health technology was defined as a respondent’s ability to name at least one digital platform they used for chronic disease management.
Our demographic data consisted of categorical and continuous variables. Categorical variables (Sex, Employment) were assigned numbers and percentages. While distribution of continuous variables (Age, Management score), were evaluated by constructing histograms. Since both variables had skewed distributions, we calculated median and interquartile ranges and used descriptive statistics to illustrate the distribution of respondents across the UTAUT model questions.
Univariate logistic regression was performed to determine the association between sociodemographic factors and two outcomes: perception (based on UTAUT model) and usage of digital health technology Multivariate regression models were then constructed with statistically significant variables in a forward stepwise method based on ascending p values.
The same statistically significant factors were also selected for subgroup analyses to determine the association between sociodemographic factors and each domain of the UTAUT model, based on the above-defined Domain Impression Scores. Both univariate and forward step-wise multivariate models were generated.
Data analysis was conducted using R (Version, 4.3.1). Statistical significance set at p < 0.05.
Results
Table 1 depicts the demographics of participants. The median age was 63 and the majority were female (55.88%), married (76.14%) and Chinese (69.61%). Distribution across 3 education levels was relatively equal. Participants were mainly retired (45.10%) or employed (40.85%), with majority having an average household income of <$3000/month (55.23%) and living in 4–5 room HDBs (60.13%). 77.45% of participants used their digital devices daily, with majority having used ‘HealthHub’ before to manage their chronic conditions (58.50%). Lastly, most participants had 1–2 chronic health conditions (71.24%) and took 1–2 medications for their conditions (54.90%).
Univariate analysis
Supplementary Table 1 summarises the association between perception towards digital health technology and sociodemographic factors. Older, unmarried, retired, and participants who occasionally accessed technology were associated with poorer perception. Conversely, participants with secondary school education and above, and household income ≥$3000/month were associated with better perception.
Supplementary Table 2 summarises the associations between PE, EE and SI with sociodemographic factors. Older and unmarried participants were associated with good scores for all subgroups. Participants with occasional access to technology were associated with good PE and SI. Retirees and participants with ≥ 3 comorbidities were associated with good PE. Conversely, participants with tertiary education were associated with good scores for all subgroups, and those with secondary school education were associated with good PE. Participants with household income ≥$3000/month were associated with good PE and SI.
Supplementary Table 3 summarises the association between participants’ usage of digital health technologies and sociodemographic factors. Older, unmarried, retired, and participants who occasionally accessed technology were less likely to use digital health technologies. Conversely, participants with secondary school education and above, household income ≥$3000/month, who lived in 4–5 room HDBs and better scores for SEMCD, overall impression and individual subgroups were more likely to use digital health technologies.
Multivariate analysis
Table 2 summarises the multivariate analysis of the association between perception of digital health technologies and statistically significant sociodemographic factors from univariate analysis. We found that older participants were associated with poorer perception, whereas those with tertiary education were associated with good perception. We also found that participants who occasionally accessed technology were associated with good PE and SI, while unmarried participants were associated with good EE and SI. Conversely, those with secondary school education and above and household income ≥$3000/month were associated with good PE.
Table 3 summarises the multivariate analysis of the association between usage of digital health technologies and statistically significant sociodemographic factors from univariate analysis. We found that participants with household income ≥$3000/month, good PE and good SI were more likely to use digital health technologies.
Discussion
Our study showed that increasing age, being unmarried and occasional access to technology are key barriers to using digital technology in chronic disease management. Conversely, having higher education and higher income are key facilitators. Higher income, good PE and SI were consistently associated with digital technology usage.
Our study found older age was associated with a poorer perception of digital technology in chronic disease management. Likewise, a previous study showed older individuals had lower self-efficacy and higher anxiety rates regarding digital technology use26. Decline in cognitive abilities, steep learning curves and physical, functional, visual limitations also hamper their adoption of new technologies26,27. As such, they demonstrate lower digital literacy and proficiency, resulting in poorer perceptions of technology, translating to poor usage as per the UTAUT model17. A study in Singapore further corroborated that health-seeking behaviour among older adults was not technology-centric, but leaned towards seeking direct medical care11.
In our study, occasional access to technology was associated with poorer PE and SI. Studies have shown that low perceived usefulness leads to decreased usage of digital health technologies which begets social isolation, potentially causing lower awareness of digital health technology and missed health announcements28,29. Hence, occasional access to technology is a barrier for use of digital technology in chronic disease management. This is consistent with a previous study that shows habitually using technology increases technology usage for other purposes, including digital health30.
Our study found that being married was associated with higher EE and SI. A previous study found that married individuals experience greater social support from their partners compared to other relationships31. This explains our findings where married participants experienced higher SI than unmarried individuals. Moreover, their children may provide digital assistance to their parents, facilitating ease of use, thereby increasing their EE32,33.
In our study, higher education was associated with better PE and perception. Previous studies reported that higher education is linked to higher cognitive function, contributing to greater skills acquisition capabilities34,35. These individuals have greater propensity to appreciate digital health technologies in managing their chronic disease, translating to a higher PE and better perception, predisposing to greater usage.
Higher income was another key facilitator for higher PE and usage of digital technology in our study. This is consistent with previous studies which reported positive attitudes and greater receptiveness towards digital technologies in higher income groups; due to greater access and exposure36,37,38,39. This predisposes to greater PE, facilitating greater usage.
These findings have critical policy implications for improving digital health adoption among older adults, particularly in addressing barriers related to age, education, and income. Policymakers can implement targeted initiatives such as subsidising digital devices and providing affordable or free access to digital health platforms to alleviate financial constraints for lower-income individuals. Additionally, bridging the digital literacy gap through community-based, multilingual education programmes and workshops tailored to older adults can enhance confidence and familiarity with digital health tools27. Integrating blended care models, where digital health technologies complement traditional face-to-face interactions, may facilitate gradual adoption among those less familiar with technology40. Public health campaigns should emphasise the benefits, ease of use, and security of digital health technologies to build trust and increase acceptance, leveraging healthcare professionals and community organisations for effective outreach41. Emphasising the necessity of user-centred design, ensures that digital health platforms are intuitive, accessible, and seamlessly integrated with existing healthcare infrastructure. Special attention should be given to usability among older adults, including simplified interfaces, voice-assisted navigation, and multilingual support. Additionally, platforms must be designed to enhance interoperability with existing hospital systems, minimising disruptions in clinical workflows and maximising adoption among healthcare professionals42. By implementing these policy-driven strategies, digital health adoption can be scaled equitably, ensuring that older adults and underserved populations are not left behind43.
By incorporating these insights into policy, healthcare operations, and technology development, digital health adoption can be optimised, ultimately leading to better patient outcomes and improved healthcare efficiency. Future research should continue to build on this foundation by exploring longitudinal impacts and refining implementation strategies to provide evidence-based recommendations for sustained and inclusive digital health integration. Policymakers could promote subsidising of digital devices and community-based digital literacy programs in lower-income areas. In addition, targeted digital literacy and training programs for older adults or those with lower educational attainment may aid bridging the digital divide. Likewise, addressing concerns about data privacy and trust, as identified in our survey, may involve transparent communication about data protection practices and the development of trusted digital platforms. These measures could help enhance the usage profile of digital health technologies across diverse population groups.
Strengths and limitations
The main strength of our study was the usage of the UTAUT model and validated SEMCD scale to measure perception towards digital technology. Both models provided established and reliable measures of our outcomes and variables, increasing the objectivity, accuracy and potential translatability of our paper.
Although UTAUT provides a robust framework for understanding technology adoption, its application in the healthcare sector is subject to debate due to the multifaceted, interdisciplinary nature of healthcare systems. Unlike consumer-oriented technologies, healthcare innovations must accommodate organizational constraints, regulatory environments, and interprofessional collaboration, factors that UTAUT does not fully address.
While our study adapted UTAUT to offer valuable insights, future research should consider alternative or extended models that incorporate sociotechnical perspectives, recognizing the dynamic interactions between technical systems, healthcare professionals, and institutional factors. A previous systematic review has highlighted that patient adoption of digital health tools is influenced by a range of sociotechnical factors beyond those captured by UTAUT44. These include usability challenges, data privacy concerns, clinician-patient trust, integration with existing healthcare workflows, and the level of institutional support for technology implementation. Expanding the theoretical framework in future studies could provide a more holistic understanding of facilitators and barriers to adoption in healthcare contexts.
Another strength lay in our systematic and rigorous approach in conducting interviews. Interviewers meticulously documented the blocks visited and maintained a live, shared manual response tracking sheet of units which responded, denied response or did not answer, requiring repeat visiting. Thorough examination of all units within each block further eschewed duplicate responses. Moreover, the use of electronic devices to conduct surveys minimised interviewer bias.
Limitations of our study include: First, comorbidity status was assessed at an aggregate level, meaning that we did not differentiate between specific chronic conditions. While this approach allowed us to analyse general trends in digital health adoption, it may not capture condition-specific barriers and facilitators that could influence engagement with digital health technologies. For example, individuals with mobility-related conditions might face different adoption challenges compared to those managing chronic metabolic diseases. Second, the digital health needs and usability concerns may vary depending on the severity and progression of a condition, which was not accounted for in our assessment. Future studies should consider examining adoption patterns across specific chronic conditions to provide more targeted insights into disease-specific digital health interventions. Third, the use of voluntary sampling may introduce non-response bias, as responders might differ in sociodemographic characteristics from non-responders. The exclusion of residents from private housing, comprising 20% of the population (63), may also impact the overall sample representation of the population, threatening internal validity. Fourth, confinement to the Singapore population with a small sample size (n = 306) limits generalisability and external validity. Fifth, although the questionnaire was electronically self-administered in a face-to-face setting, administrators were available to provide minimal assistance when required, such as helping participants navigate technical issues. This design choice allowed us to simulate typical interactions with digital platforms. However, it may have introduced selection bias by favouring individuals with a baseline level of digital literacy. Future studies could consider alternative administration modes to ensure inclusion of participants with minimal or no digital experience. Sixth, while the UTAUT framework enabled us to systematically assess perception and engagement patterns, future research employing qualitative or sociotechnical approaches could better elucidate nuanced challenges—such as data literacy, personalization needs, and trust—in digitally mature healthcare environments. While this study identified key associations between sociodemographic characteristics and digital health perceptions, it does not capture the experiential or structural dimensions influencing use. Future qualitative studies are needed to deepen understanding of usability challenges, trust, personalization, and health system integration. Seventh, the use of the UTAUT framework and SEMCD scale inherently focuses on specific constructs of technology acceptance and self-efficacy, which do not fully capture the complex and multifaceted nature of digital health adoption in chronic disease management. This limitation suggests that the claims presented, while supported by the quantitative analysis, should be interpreted with caution. Future longitudinal and mixed-methods research are warranted to establish causal relationships and to explore broader contextual and experiential factors influencing digital health engagement. Eighth, modifications were made to the original UTAUT and SEMCD instruments, including the reduction of SEMCD from six to five items. As these changes were not accompanied by formal re-validation, our total scores cannot be benchmarked against normative data. This limits the generalisability and comparability of our findings. However, the retained items reflect the core dimensions of chronic disease self-management and remain relevant to the local digital health context. The score of 35 out of 50—equivalent to an average item score of 7—was interpreted as indicative of moderate to high self-efficacy within this population. Future studies should consider using formally validated adaptations to enhance the robustness and external validity of findings.
Conclusions
Higher education and higher income were found to be facilitators in using digital technologies for chronic disease management, while being older, unmarried and having reduced frequency of access to technology were found to be barriers. Future research could further investigate the specific causes for the current trends observed, and explore potential interventions to increase adoption of technology among older adults. Demographic implications could also be considered by policymakers to enhance the usage profile of digital health technologies.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
National Center for Chronic Disease Prevention and Health Promotion. About Chronic Diseases 2021 [Available from: https://www.cdc.gov/chronicdisease/about/index.htm
World Health Organisation. Noncommunicable diseases 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (2023).
Chan, A. et al. Transitions in health, employment, social engagement And intergenerational transfers In Singapore study (THE SIGNS study)–I: descriptive statistics and analysis of Key aspects of successful ageing (2018).
Tan, S. Y. et al. Healthcare cost of patients with multiple chronic diseases in Singapore public primary care setting. Ann. Acad. Med. Singap. 50, 809–817 (2021).
Fitzpatrick, A. L., Powe, N. R., Cooper, L. S., Ives, D. G. & Robbins, J. A. Barriers to health care access among the elderly and who perceives them. Am. J. Public Health. 94, 1788–1794 (2004).
Maresova, P. et al. Consequences of chronic diseases and other limitations associated with old age – a scoping review. BMC Public. Health. 19, 1431 (2019).
Doetsch, J., Pilot, E., Santana, P. & Krafft, T. Potential barriers in healthcare access of the elderly population influenced by the economic crisis and the troika agreement: a qualitative case study in lisbon, Portugal. Int. J. Equity Health. 16, 184 (2017).
Bähler, C., Huber, C. A., Brüngger, B. & Reich, O. Multimorbidity, health care utilization and costs in an elderly community-dwelling population: a claims data based observational study. BMC Health Serv. Res. 15, 23 (2015).
Ginting, M. L. et al. A Patient-Centred medical home care model for Community-Dwelling older adults in singapore: A Mixed-Method study on patient’s care experience. Int. J. Environ. Res. Public. Health. 19, 4778 (2022).
Toh, H. J. et al. Virtual geriatric care: user perception of telegeriatrics in nursing homes of Singapore. Commun. Comput. Inform. Sci. 91–105 (2015).
Low, S. T. H., Sakhardande, P. G., Lai, Y. F., Long, A. D. S. & Kaur-Gill, S. Attitudes and perceptions toward healthcare technology adoption among older adults in singapore: A qualitative study. Front. Public. Health. 9, 588590 (2021).
Bertera, E. M., Tran, B. Q., Wuertz, E. M. & Bonner, A. A study of the receptivity to Telecare technology in a community-based elderly minority population. J. Telemed Telecare. 13, 327–332 (2007).
Frishammar, J., Essén, A., Bergström, F. & Ekman, T. Digital health platforms for the elderly? Key adoption and usage barriers and ways to address them. Technol. Forecast. Soc. Chang. 189, 122319–122319 (2023).
Chong, J. H. S. et al. Perceptions and experiences of a multi-domain preventive health programme: a qualitative study informing future community-based health interventions in Singapore. BMC Public. Health. 24, 2954 (2024).
Taylor, M. L. et al. Digital health experiences reported in chronic disease management: an umbrella review of qualitative studies. J. Telemed Telecare. 28, 705–717 (2022).
Moulaei, K., Moulaei, R. & Bahaadinbeigy, K. Barriers and facilitators of using health information technologies by women: a scoping review. BMC Med. Inf. Decis. Mak. 23, 176 (2023).
Venkatesh, V., Morris, M. G., Davis, G. B. & Davis, F. D. User acceptance of information technology: toward a unified view. MIS Q. 27, 425–478 (2003).
Uncovska, M., Freitag, B., Meister, S. & Fehring, L. Patient acceptance of prescribed and fully reimbursed mHealth apps in germany: an UTAUT2-based online survey study. J. Med. Syst. 47, 14 (2023).
Nunes, A., Limpo, T. & Castro, S. L. Acceptance of mobile health applications: examining key determinants and moderators. Front. Psychol. 10, 2791 (2019).
Wu, P., Zhang, R., Zhu, X. & Liu, M. Factors influencing continued usage behavior on mobile health applications. Healthc. (Basel). 10, 208 (2022).
de Veer, A. J. et al. Determinants of the intention to use e-Health by community dwelling older people. BMC Health Serv. Res. 15, 103 (2015).
Breil, B., Kremer, L., Hennemann, S. & Apolinário-Hagen, J. Acceptance of mHealth apps for Self-Management among people with hypertension. Stud. Health Technol. Inf. 267, 282–288 (2019).
Haldane, V. et al. Perspectives on acceptance and use of a mobile health intervention for the prevention of atherosclerotic cardiovascular disease in singapore: Mixed-Methods study. JMIR Mhealth Uhealth. 7, e11108 (2019).
Ritter, P. L. & Lorig, K. The english and Spanish Self-Efficacy to manage chronic disease scale measures were validated using multiple studies. J. Clin. Epidemiol. 67, 1265–1273 (2014).
Lorig, K. R., Sobel, D. S., Ritter, P. L., Laurent, D. & Hobbs, M. Effect of a self-management program on patients with chronic disease. Eff. Clin. Pract. 4, 256–262 (2001).
Czaja, S. J. et al. Factors predicting the use of technology: findings from the center for research and education on aging and technology enhancement (CREATE). Psychol. Aging. 21, 333–352 (2006).
Choi, N. G. & Dinitto, D. M. The digital divide among low-income homebound older adults: internet use patterns, eHealth literacy, and attitudes toward computer/internet use. J. Med. Internet Res. 15, e93 (2013).
Huang, T. World Internet Project Survey: results for Auckland. Auckland Council technical report 2019:TR2019/2001 (2017).
Umoh, M. E., Prichett, L., Boyd, C. M. & Cudjoe, T. K. M. Impact of technology on social isolation: longitudinal analysis from the National health aging trends study. J. Am. Geriatr. Soc. 71, 1117–1123 (2023).
Oulasvirta, A., Rattenbury, T., Ma, L. & Raita, E. Habits make smartphone use more pervasive. Personal. Uniquit. Comput. 16, 105–114 (2012).
Soulsby, L. & Bennett, K. Marriage and psychological wellbeing: the role of social support. Psychology 6, 1349 (2015).
Haddock, A., Ward, N., Yu, R. & O’Dea, N. Positive effects of digital technology use by adolescents: A scoping review of the literature. Int. J. Environ. Res. Public. Health. 19, 14009 (2022).
Olson, K. E., O’Brien, M. A., Rogers, W. A. & Charness, N. Diffusion of technology: frequency of use for younger and older adults. Ageing Int. 36, 123–145 (2011).
Lövdén, M., Fratiglioni, L., Glymour, M. M., Lindenberger, U. & Tucker-Drob, E. M. Education and cognitive functioning across the life span. Psychol. Sci. Public. Interest. 21, 6–41 (2020).
Levine, M. D. Differences in learning and neurodevelopmental function in school-age children. In: Carey, W. B. C., Coleman A. C, Elias, W. L., Feldman, E. R., Heidi, M. (eds.) Developmental-Behavioral Pediatrics, Fourth Edition. 535–46 (W.B. Saunders,Philadelphia, 2009).
Abu-Shanab, E. & Income Divide A determinant of technology acceptance. Int. Arab. J. e-Technology (IAJeT). 3, 121–127 (2013).
Gaylin, D. S., Moiduddin, A., Mohamoud, S., Lundeen, K. & Kelly, J. A. Public attitudes about health information technology, and its relationship to health care quality, costs, and privacy. Health Serv. Res. 46, 920–938 (2011).
He, Y., Chen, Q. & Kitkuakul, S. Regulatory focus and technology acceptance: perceived ease of use and usefulness as efficacy. Cogent Bus. Manage. 5, 1459006 (2018).
Paccoud, I. et al. Socioeconomic and behavioural factors associated with access to and use of personal health records. BMC Med. Inf. Decis. Mak. 21, 18 (2021).
Shaw, J., Brewer, L. C. & Veinot, T. Recommendations for health equity and virtual care arising from the COVID-19 pandemic: narrative review. JMIR Form. Res. 5, e23233 (2021).
Latulippe, K., Hamel, C. & Giroux, D. Social health inequalities and eHealth: A literature review with qualitative synthesis of theoretical and empirical studies. J. Med. Internet Res. 19, e136 (2017).
Keesara, S., Jonas, A. & Schulman, K. Covid-19 and health care’s digital revolution. N Engl. J. Med. 382, e82 (2020).
Kruse, C. S. et al. Telehealth and patient satisfaction: a systematic review and narrative analysis. BMJ Open. 7, e016242 (2017).
Jacob, C., Sezgin, E., Sanchez-Vazquez, A. & Ivory, C. Sociotechnical factors affecting patients’ adoption of mobile health tools: systematic literature review and narrative synthesis. JMIR Mhealth Uhealth. 10, e36284 (2022).
Funding
S. Hilal was supported by National Medical Research Council Singapore, Transition Award [A-0006310-00-00], Ministry of Education, Academic Research Fund Tier 1 [A-0006106-00-00] and Absence Leave Grant [A-8000336-00-00].
Author information
Authors and Affiliations
Contributions
M.M.T.T., R.S.H.H., W.J.W.H.G. wrote the manusccript and performed the analysis. S.H. reviewed the manuscript, provided supervision and obtained funding.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tan, M.M.T., Wong, R.S.H., Goh, W.J.W.H. et al. Facilitators and barriers for use of digital technology in chronic disease management. Sci Rep 15, 29267 (2025). https://doi.org/10.1038/s41598-025-15549-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-15549-w
