
Abstract
This study aims to understand the mental health of South Koreans one year after the Seoul Halloween crowd disaster(hereafter referred to as the Seoul Halloween disaster), an anthropogenic disaster that occurred in 2022. In total, 651 participants completed three online surveys to measure anxiety, depression, and post-traumatic stress disorder (PTSD) over a year after the disaster. The collected data were then analyzed with descriptive statistics, repeated-measures analysis of variance (ANOVA), and independent samples t-tests using the SPSS 28 program. Six months after the Seoul Halloween disaster, the mean mental health scores, including those for anxiety, depression, and PTSD, were all above the cutoff point, and these results continued without significant change over the year. Mainly, for PTSD, the high-risk group consistently accounted for more than 30% of the subjects, with a mean score of 39, which is considerably above the cutoff of 25 for high risk. In addition, changes in alcohol consumption and intentionally avoiding the affected area had higher anxiety, depression, and PTSD. Therefore, there is a need to target a broader range of people for post-disaster psychological support and provide resources to prevent psychological trauma from becoming chronic with a medium- to long-term approach.
Similar content being viewed by others

Introduction
Disasters come in many forms, and those who experience them are exposed to psychological trauma1. Psychological trauma can result from direct exposure to a traumatic event, such as threatened death, serious injury, or sexual assault; indirect exposure, such as learning that it has happened to a family member, relative, or friend; or repeated exposure to aversive aspects of the traumatic event. Symptoms include anxiety and depression, fear, sleep problems, difficulty concentrating, and social isolation2. Psychological trauma may improve over time, but in the long term, it can increase the risk of mental illnesses such as post-traumatic stress disorder (PTSD), depression, and anxiety disorders3. This psychological trauma varies depending on the type of disaster, with anthropogenic disaster (e.g., war, terrorism, industrial accidents, collapse, etc.) causing more significant psychological trauma than disasters caused by natural hazards (e.g., floods, earthquakes, volcanic eruptions, etc.)4. This is because in some cases there is no clearly defined point at which the tragedy ends, as it may affect an indeterminate number of people at the same time. Such ambiguity can make the perceived threat seem prolonged or unpredictable, leading to increased confusion and distress5. They are also associated with political conflicts and economic crises and are indirectly affected by the media6 ; therefore, mental health issues need to be addressed in depth.
The Seoul Halloween disaster, which occurred on October 29, 2022, was a large-scale anthropogenic disaster that caused 159 deaths and 320 injuries when Halloween celebrators converged on a narrow alleyway after social boundaries due to the pandemic were relaxed7. The accident scene was broadcast unfiltered on SNS, and the arrival of a cardiac arrest patient at the hospital was also broadcast live. This indiscriminate exposure led to a statement that the event could cause unprecedented national trauma8. According to the National Trauma Center, 7,141 psychological counseling sessions were conducted over a year, and 2,049 (28.7%) of those who received counseling were from the general public, followed by bereaved families, witnesses, and the injured. In addition, a previous study of people in their 20s and 30s six months after the disaster confirmed that 37% of the general public suffered from partial or complete PTSD after the Seoul Halloween disaster despite having experienced it indirectly9. Furthermore, 1,316 firefighters were identified as still receiving treatment or care for psychological difficulties due to the Seoul Halloween disaster more than a year later.
As such, changes in mental health in response to disaster exposure need to be studied more comprehensively, as disaster exposure can result in a broad spectrum of symptoms which may improve over time10 or, in some people, may manifest as chronic depression, anxiety, or PTSD11. Furthermore, because disaster-related emotions and experiences can lead to recall bias due to efforts to overcome them, asking the same subjects about their mental health at different points after a disaster can best prevent recall bias12. Accordingly, this study, conducted every three months starting six months after the Seoul Halloween disaster, is a significant contribution to the literature. Specifically, in this study, the mental health of participants, such as depression, anxiety, and PTSD, was checked at different points in time and analyzed according to whether they had changed their drinking frequency or avoidance after the disaster. Therefore, this study aims to explore the mental health problems that the public who is exposed to disasters may experience and how these problems change. In addition, we aim to provide evidence on post-disaster mental health and a framework for establishing an appropriate system for future disaster mental health issues and support periods.
Methods
Participants and data collection
This study recruited participants from a panel of adults aged 19 to 69 residing in South Korea through a professional survey company (Korea Research Co.). The company maintains a large-scale, pre-registered online panel and used quota sampling, a type of non-probability sampling, to reflect the national population distribution by age, gender, and region of residence. Education level, income, and occupation were not controlled. Recruitment was conducted via email and mobile phone notifications sent to panel members who met the basic eligibility criteria. Participants were informed that this was a longitudinal study consisting of three surveys, and that they would receive a small financial incentive from the company for completing each survey. From May 16, 2023, to November 10, 2023, we conducted the survey at three time points: 1,007 participants responded to the first survey. At 9 months, 195 participants did not respond, meaning 812 participants completed the second survey at that time. At 12 months, 161 of the 812, or 19.8%, did not respond. In the end, 651 participants (64.6%) who participated at all three time points were included in the analysis. The participant flow diagram for this study is shown in Fig. 1.

Participant flow diagram.
Measures
Sociodemographic variables included age, gender, occupation, residence region, and family type, as well as type of disaster exposure, change in drinking frequency after the disaster, and intentional avoidance of the disaster area. We also used self-report questionnaires to measure anxiety, depression, and PTSD.
Anxiety (GAD-7)
Anxiety was screened using the Generalized Anxiety Disorder-7 (GAD-7)13a 7-item self-report questionnaire and diagnostic assessment tool for generalized anxiety disorder. Items are rated on a 4-point Likert scale (0 = never, 3 = almost every day) with a total score ranging from 0 to 21, with 0 to 4 categorized as normal, 5 to 9 as mild, 10 to 14 as moderate, and 15 or more as severe. A representative question is, “I feel nervous, anxious, or impatient.” The Korean version of the GAD-7 (Cronbach’s α = 0.89) was used in this study, and the coefficient of this study was 0.92.
Depression (PHQ-9)
Depression was measured using the Patient Health Questionnaire-9 (PHQ-9)14 tool, a 9-item self-report questionnaire for the screening, diagnosis, and severity of depression. Items are rated on a 4-point Likert scale (0 = never, 3 = almost every day), with higher scores indicating more depressive symptoms. A total score of 0–4 is considered normal, 5–9 is considered mild, 10–19 is considered moderate, and 20–27 is considered severe. A representative question is, “I feel down, depressed, or hopeless.” The Korean version of the PHQ-9 has a Cronbach’s α of 0.89, which coefficient was found to be 0.92 in this study.
Post-traumatic stress disorder (IES-R-K)
PTSD was measured using the Impact of Event Scale-Revised Korean Version (IES-R-K) by Eun (2005)15. The scale consists of 22 items rated on a 5-point Likert scale, with total scores ranging from 0 to 88. The higher the total score, the more severe the post-traumatic stress, where 0–17 is considered normal, 18–24 is considered at risk, and 25 and above is considered high risk. A representative question is, “When I think about the event, I feel the emotions I felt at the time come back.” The Cronbach’s α of the IES-R-K was 0.83, and the coefficient of this study was 0.95.
Analysis
This study’s data were analyzed using SPSS 28.0 for Windows. Demographic characteristics were analyzed with frequency analysis and descriptive statistics, and multiple selection of survey items was analyzed with frequency analysis according to multiple selection. Multiple-choice results are presented as percentages of the total number of duplicate responses. Differences in anxiety, depression, and PTSD levels across time points were analyzed using repeated-measures ANOVA. The effects on mental health of gender, exposure to the Seoul Halloween disaster, changes in drinking frequency after the disaster, and intentional avoidance were analyzed using logistic regression. Statistical significance was defined as p < .05.
Ethical considerations
This study was approved by the Institutional Review Board of Chung-Ang University (IRB number 1041078-20221129-HR-019). The researcher explained the purpose and procedures of the study to the survey company and signed a confidentiality agreement. All participants provided informed consent prior to participation. The informed consent form outlined the purpose of the study, the procedures involved, the researcher’s name and contact information, and a statement that participants could withdraw from the study at any time without penalty. The researcher developed the entire research questionnaire. The company distributed the research questionnaire in the form of a URL after final approval by the researcher. The collected data were initially checked by the survey company and then processed by the researcher through a review and coding process. All research procedures were conducted in accordance with relevant institutional and national guidelines and regulations, and in compliance with the Declaration of Helsinki and its later amendments.
Results
The general characteristics of the final 651 participants are presented in Table 1. There were 320 (49.2%) men and 331 (50.8%) women, with 165 participants (25.3%) in their 50s, 151 (23.2%) in their 60s, and 144 (22.1%) in their 40s. Regarding occupation, 455 (69.9%) were employed, while 31 (4.8%) were students. Of the participants, 295 (45.3%) lived in Seoul and the Seoul metropolitan area, and 356 (54.7%) lived in other regions. By family type, 292 (44.9%) lived with parents and children, followed by 113 (17.4%) living with a partner. Regarding exposure to the Seoul Halloween disaster, 46 respondents (7.0%) reported direct or indirect exposure, while 605 respondents (93.0%) reported no such exposure. Among the 46 exposed respondents, 27 (58.7%) reported that a family member, relative, or friend had been physically injured, 9 (19.6%) reported the death of a family member or friend, 6 (13.0%) had witnessed death or injury at the scene, and 4 (8.7%) reported physical injury to themselves. These types of exposure were evaluated to reflect Criterion A of the PTSD diagnostic criteria (e.g., experiencing or witnessing life-threatening events) and were categorized in the analysis as types of disaster exposure. When asked about changes in drinking frequency after the incident, 150 (23.0%) responded that their drinking frequency had changed. In addition, when asked if they had intentionally avoided the area (Itaewon, Seoul) after the incident, 261 (40.1%) responded that they had. Among the multiple responses given regarding the reason why they had avoided the area, the most frequent response (44%) was that thinking about the area gave rise to negative feelings (sadness, anxiety, fear, and panic) followed by the area triggering memories of the incident (40.1%) and physical symptoms such as headaches (11.5%).
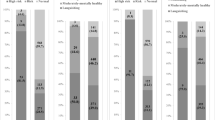
Participants’ mental health and changes over time are displayed in Table 2; Fig. 2. For anxiety, mean scores at 6, 9, and 12 mths were 4.74 ± 4.57, 4.58 ± 4.59, and 4.33 ± 4.68, respectively, with no statistically significant change over time (p = .263). For depression, mean scores were 5.19 ± 5.10, 5.25 ± 5.48, and 5.40 ± 5.39 at 6, 9, and 12 mths, respectively. These differences were not statistically significant (p = .765). The mean scores remained above the cutoff of 5 at all three time points. For PTSD, the mean scores were 19.09 ± 17.07, 17.95 ± 17.01, and 19.27 ± 18.54 at 6, 9, and 12 mths, respectively, with no statistically significant difference over time (p = .341). The 18-point cutoff for PTSD separates the normal and at-risk groups, and the scores at all three time points were interpreted as borderline. Among participants at high risk for PTSD, the mean score was 39.93 ± 11.50 at 9 mths and 41.48 ± 14.25 at 12 mths. These changes were also not statistically significant.

Percentage of mental health severity by time after Seoul Halloween disaster.
Table 3 presents the effects of gender, exposure to the Seoul Halloween disaster, changes in drinking frequency after the disaster, and intentional avoidance on anxiety, depression, and PTSD. As shown in Table 2, the mean differences in mental health across time points were not significant and were not persistent, so logistic regression analyses were conducted using cutoff points for anxiety, depression, and PTSD. The results indicated that gender did not have a statistically significant effect on anxiety and PTSD but did have a significant effect on depression (p = .035). The effects of exposure to the Seoul Halloween disaster, changes in drinking frequency after the disaster, and intentional avoidance were all found to significantly affect anxiety, depression, and PTSD at the 0.05 significance level. Specifically, individuals who were exposed to the Seoul Halloween disaster (answered “Yes”) had 4.038 times more anxiety, 2.907 times more depression, and 20.762 times more PTSD compared to those who were not exposed (answered “No”). Those who reported changes in drinking frequency after the disaster showed 1.863 times more anxiety, 1.750 times more depression, and 2.076 times more PTSD compared to those who reported no change. Lastly, individuals who intentionally avoided the area after the disaster exposure 2.765 times more anxiety, 2.395 times more depression, and 5.012 times more PTSD compared to those who did not avoid the area.
Discussion
This study was conducted to understand the mental health of the public in Korea one year after the Seoul Halloween disaster to provide baseline data on the current state of disaster mental health and the duration of support needed. Ultimately, this study finds that anxiety, depression, and PTSD continued to remain above the cutoff scores one year after the disaster and did not change at statistically significant levels. This finding differs from those of previous studies16,17 showing that most people recover after about two months following an anthropogenic disaster. In this study, the prevalence of PTSD remained above 30% without any significant change at any time point, which may be due to the persistence of PTSD in high-risk individuals18. Furthermore, 10–30% of victims exposed to disasters may progress to chronic PTSD11which suggests that additional psychological support may be needed.
Furthermore, our finding that there were no statistically significant changes in mental health by the first memorial day of the Seoul Halloween disaster diverges from previous studies that have reported increases in anxiety, depression, and PTSD on disaster anniversaries19,20. Psychological trauma, such as PTSD, may be more evident when there is a cognitive relationship with the traumatic event21. In the case of the Seoul Halloween disaster, the psychological trauma may have been different depending on how the event was interpreted, as some viewed it as “you went to enjoy Halloween, knowing there would be a large crowd, and then you had an accident“22while others viewed it as social turmoil and political conflict. It is also conceivable that those at high risk for PTSD at previous points in time may have already had a high-stress response, which may have prevented further changes.
In addition, although only 7% of the participants in this study reported being victimized by the Seoul Halloween disaster, more than 30% were consistently at high risk for PTSD, and anxiety and depression remained high. This suggests a high prevalence of indirect trauma. In the case of the Seoul Halloween disaster, many people were exposed to indirect trauma as photos of the scene were shared indiscriminately on SNS, and such exposure through various media can lead to severe psychological trauma23,24,25. In fact, studies have found no difference in PTSD levels between people who have directly experienced tragic disasters such as 9/11 and those who have been indirectly exposed to disasters through television26and indirect traumatic experiences of anthropogenic disasters have been found to significantly impact on suicidal behavior27. Indeed, exposure to disasters increases existential anxiety about the meaning of life28so it is necessary to approach media dissemination cautiously and objectively immediately after a disaster and restrict media contact with vulnerable populations.
Notably, we found that females were more affected by depression, which is consistent with previous research demonstrating that women have higher levels of depressive symptoms after disasters29. However, for PTSD, there was no difference by gender, which is contrary to previous studies that found higher levels of PTSD in women30,31,32. However, given that previous research has shown that men recover from PTSD more slowly than women33 and that PTSD may be differentially affected by trauma load rather than gender when individuals are exposed to disasters34it is necessary to focus on the individual’s trauma load in the case of the Seoul Halloween disaster and support psychological trauma regardless of gender.
Furthermore, anxiety, depression, and PTSD were higher among those who changed their drinking habits after the Seoul Halloween disaster. This is consistent with previous research showing that post-disaster drinking changes are associated with sleep problems and PTSD35. In addition, previous research on post-disaster drinking trends has confirmed that drinking changes are more dangerous for those at risk of PTSD and lead to mental health decline and chronic alcoholism over time36. Therefore, it is necessary to provide programs that can shift harmful coping mechanisms such as drinking and monitor them separately.
Finally, when looking at mental health differences regarding the experience of intentionally avoiding the area where the disaster occurred in Seoul (Itaewon), we found statistically higher levels of anxiety, depression, and PTSD among those who intentionally avoided the area. Avoidance is a coping strategy to protect oneself from trauma, and it is one emotion that appears in subjects exposed to disasters37. However, avoidance can impair adaptation to stress and serve as a negative coping mechanism for treatment38. Our findings are consistent with previous research showing that avoidance coping strategies are associated with higher levels of depression after real-life disasters39 and that avoidance symptoms negatively impact PTSD by activating the brain’s fear circuitry40. Indeed, the participants in this study reported that the main reason for avoiding the accident area was negative emotions such as sadness, anxiety, and fear. Avoidance of locations where anthropogenic disasters have occurred may lead to long-term negative impacts on the local community, including economic decline and social stigma. While this study did not directly investigate these consequences, the observed patterns of avoidance behavior suggest a need for broader discussions on how to support affected communities in recovery, including promoting public engagement through culturally meaningful and safe activities.
In addition, the lack of significant differences in anxiety, depression, and PTSD across the three times suggests that psychological distress remained persistently high over time. This stability may be due to the chronic nature of trauma responses, insufficient early intervention, or already elevated stress levels among high-risk individuals.
Overall, the significance of this study is that it identifies and compares mental health one year after a disaster. As the Seoul Halloween disaster occurred in the center of downtown Seoul and resulted in many casualties, the psychological trauma experienced by the public in this case differs from that studied in previous longitudinal studies and is ongoing. Therefore, governments and communities must provide integrated and systematic psychological trauma treatment and support programs after disasters. In particular, high-risk groups should be screened early to prevent chronicity and the deterioration of mental health.
Conclusion
This longitudinal study of psychological trauma in the public in Korea after the Seoul Halloween disaster provides information on differences in mental health according to the participants’ circumstances. In particular, the participants experienced high levels of psychological trauma after the disaster that remained unchanged up to one year after the disaster, which indicates that the psychological trauma of the disaster is likely to be chronic. In addition, the level of psychological trauma varied depending on whether the participants changed their drinking frequency after the disaster or intentionally avoided the area after the disaster, which suggests that it is necessary to identify individual coping strategies after the disaster and provide appropriate early interventions to address the psychological trauma that may emerge later. Furthermore, this study included subjects who did not experience the disaster firsthand, confirming that psychological trauma can occur through indirect exposure to a disaster, even if it is not experienced directly. Thus, this study suggests that mental health problems following disasters are not unique to particular groups but rather may occur in the mid-to-long term for the population, providing a basis for the scope and timing of post-disaster psychological support.
Limitations
There are several limitations to this study. First, there are no data on the sub-acute period (up to one to three months after the disaster), which is when adverse reactions to psychological trauma are most pronounced and can be an important time point for longitudinal studies. The lack of measurement at this point in time limits our ability to identify trajectories of mental health change after the disaster. Second, there are no data on the internal or external support systems that may have influenced participants’ mental health. Psychological responses after a disaster can vary depending on the availability of personal coping resources, social support, and access to mental health services. Because this study collected data from independent cross-sectional samples at different time points, it was not possible to control for these potentially confounding factors. Third, this study did not include a non-exposed comparison group. Although all survey items were explicitly framed in relation to the Seoul Halloween disaster - ensuring that participants responded in the context of the event - it remains difficult to fully attribute the observed levels of anxiety, depression and PTSD solely to disaster exposure, especially in the absence of baseline data. To partially address this limitation, we included several indirect indicators of exposure and trauma-related outcomes, such as self-reported exposure status, changes in post-disaster alcohol consumption, and avoidance behaviours related to the disaster site. Although these indicators do not substitute for a control group, they provide contextual evidence to help interpret the findings in the light of disaster-related psychological responses.
Therefore, it is recommended that follow-up studies examine mental health immediately after the event to provide a longitudinal trajectory and further investigate general mental health to examine changes in mental health that reflect the individual characteristics of the participants.
Finally, this study used quota sampling based on demographic characteristics; however, as a non-probability sampling method, it has limitations in terms of the representativeness of the sample. Therefore, caution is warranted when generalizing the findings to the broader population affected by the disaster. In particular, the sample may not fully capture the mental health status of all individuals impacted by the event, and this limitation should be taken into consideration when interpreting the results.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Gerber, M. et al. Influence of multiple traumatic event types on mental health outcomes: Does count matter? J. Psychopathol. Behav. Assess. 40 (4), 645–654. https://doi.org/10.1007/S10862-018-9682-6 (2018).
Engelbrecht, A., Jones, E., Burdett, H., Silva, M. & Bhui, K. The symptomatology of psychological trauma in the aftermath of war (1945–1980): UK army veterans, civilians and emergency responders. Psychol. Med. 49 (5), 811–818. https://doi.org/10.1017/S0033291718001460 (2019).
Anthony, P. Springer,. Somatic health issues in trauma-related disorders: Effects on psychobiological axes affecting mental and physical health in Person Centered Approach to Recovery in Medicine 177–216 (2019). https://doi.org/10.1007/978-3-319-74736-1_10
Makwana, N. Disaster and its impact on mental health: A narrative review. J. Fam Med. Prim. Care. 8 (10), 3090–3095. https://doi.org/10.4103/jfmpc.jfmpc_893_19 (2019).
Krakowczyk, J. et al. Development and psychometric evaluation of the Man-Made disaster-related distress scale (MMDS). Psychiatry Res. 324, 115193. https://doi.org/10.1016/j.psychres.2023.115193 (2023).
Kalcza Janosi, K., Kotta, I., Marschalko, E. & Szabo, K. The fear of war scale (FOWARS): Development and initial validation. Soc. Sci. 23 (5), 283. https://doi.org/10.3390/socsci12050283 (2023).
Ministry of the Interior and Safety. Press releases on the deaths and injuries in the Itaewon tragedy. (2022)., Dec 03 https://www.mois.go.kr/frt/bbs/type010/commonSelectBoardArticle.do?bbsId=BBSMSTR_000000000008&nttId=97414
Korean Association of Neuropsychiatry. Korean Society of Neuropsychiatry Statement on the Itaewon tragedy. (2022). https://www.knpa.or.kr/content/community/search.php?q=%EC%9D%B4%ED%83%9C%EC%9B%90 Oct 30).
Seo, D. Y. A Study of Indirect Trauma and Related Variables by Media: Focusing on the Itaewon Disaster (Ajou University Graduate School Master’s Degree in Psychology, 2023).
Kunii, Y. et al. Review of mental health consequences of the great East Japan earthquake through long-term epidemiological studies: The Shichigahama health promotion project. Tohoku J. Exp. Med. 257 (2), 85–95. https://doi.org/10.1620/tjem.2022.J039 (2022).
Lenferink, L., Keijser, J., Boelen, P., Nickerson, A. & Smid, G. Trajectories of grief, depression, and posttraumatic stress in disaster-bereaved people. Depress. Anxiety. 37 (1), 35–44. https://doi.org/10.1002/da.22850 (2020).
Moreno-Serra, R., Anaya-Montes, M., León-Giraldo, S. & Bernal, O. Addressing recall bias in (post-)conflict data collection and analysis: lessons from a large-scale health survey in Colombia. Confl. Health. 16 (1). https://doi.org/10.1186/s13031-022-00446-0 (2022).
Seo, J. G. & Park, S. P. Validation of the generalized anxiety disorder-7 (GAD-7) and GAD-2 in patients with migraine. J. Headache Pain. 16 (1), 97 (2015).
Park, S. J., Choi, H. R., Choi, J. H., Kim, K. W. & Hong, J. P. Reliability and validity of the Korean version of the patient health questionnaire-9 (PHQ-9). Anxiety Mood. 6 (2), 119–124 (2010). https://www.kci.go.kr/kciportal/ci/sereArticleSearch/ciSereArtiView.kci?sereArticleSearchBean.artiId=ART001493301
Eun, H. J. et al. A study on reliability and validity of the Korean version of impact of event scale-revised. J. Korean Neuropsychiatr Assoc 44(3), 303–310; (2005). http://uci.or.kr/G704-001050.44.3.009 (2005).
Rimé, B., Páez, D., Basabe, N. & Martínez, M. Social sharing of emotion, posttraumatic growth, and emotional climate: Follow-up of Spanish citizen’s response to the collective trauma of March 11th terrorist attacks in Madrid. Eur. J. Soc. Psychol. 40 (6), 1029–1104. https://doi.org/10.1002/ejsp.700 (2010).
Lee, H. P., Choi, Y. K., Lee, J. H. & Lee, H. S. The psychological consequences of indirect trauma exposure through the news on the Sewol ferry disaster. Korean J. Cult. Soc. Issues. 22 (3), 411–430. https://doi.org/10.20406/KJCS.2016.22.3.411 (2016).
Richard, F. et al. Factors associated with persistent posttraumatic stress disorder among U.S. military service members and veterans. BMC Psychiatry. 18 (1), 1–11. https://doi.org/10.1186/S12888-018-1590-5 (2018).
Rabinowitz, E. et al. The 50th anniversary of May 4, 1970 is associated with elevations of distress but no increase in mental health symptoms. Stress Health. 38 (3), 556–567. https://doi.org/10.1002/smi.3117 (2022).
Nemeth, D. et al. Addressing anniversary reactions of trauma through group process: The hurricane katrina anniversary wellness workshops. Int. J. Group. Psychother. 62 (1), 129–142. https://doi.org/10.1521/ijgp.2012.62.1.129 (2012).
Kube, T., Elssner, A. & Herzog, P. The relationship between multiple traumatic events and the severity of posttraumatic stress disorder symptoms—Evidence for a cognitive link. Eur. J. Psychotraumatol. 14 (1), 2165025. https://doi.org/10.1080/20008066.2023.2165025 (2023).
Peik, S. H. & Cho, M. H. 10.29 Itaewon halloween tragedy and grievabilty for the living: The stories of the survivors. Korean J. Cult. Sociol. 31 (3), 165–224. https://doi.org/10.17328/kjcs.2023.31.3.004 (2023).
Lee, J. H. et al. Exploring the factors associated with indirect trauma caused by a human-made disaster on the general population: A community study five years after the Sewol ferry incident. Int. J. Disaster Risk Reduct. 60 (1), 102262. https://doi.org/10.1016/j.ijdrr.2021.102262 (2021).
Uvais, N. Disaster-related media exposure and its impact on mental health. J. Fam Med. Prim. Care. 9 (1), 448–449. https://doi.org/10.4103/jfmpc.jfmpc_981_19 (2020).
Hopwood, T. & Schutte, N. Psychological outcomes in reaction to media exposure to disasters and large-scale violence: A meta-analysis. Psychol. Violence. 7 (2), 316–327. https://doi.org/10.1037/vio0000056 (2017).
Jarolmen, J. & Sisco, H. Media effects on post-traumatic stress disorder and the world trade center tragedy. Best Pract. Mental Health. 1 (2), 133–139 (2005).
Lee, M. Y. & Na, J. H. The effects of social disaster indirect trauma experience on suicidal behavior in university students - The dual mediating effects of smartphone addiction and alcohol addiction. Korea Inst. Youth Facil Environ. 21 (2), 15–24. https://doi.org/10.55063/kiyfe.2023.21.2.2 (2023).
Scott, B. G. & Weems, C. F. Natural disasters and existential concerns: A test of tillich’s theory of existential anxiety. J. Humanist Psychol. 53, 114–128. https://doi.org/10.1177/0022167812449190 (2013).
Taha, P. & Sijbrandij, M. Gender differences in traumatic experiences, PTSD, and relevant symptoms among the Iraqi internally displaced persons. Int. J. Environ. Res. Public. Health. 18 (18), 9779. https://doi.org/10.3390/ijerph18189779 (2021).
Hiscox, L., Sharp, T., Olff, M., Seedat, S. & Halligan, S. Sex-based contributors to and consequences of post-traumatic stress disorder. Curr. Psychiatry Rep. 25, 233–245. https://doi.org/10.1007/s11920-023-01421-z (2023).
Christiansen, D. & Berke, E. Gender- and sex-based contributors to sex differences in PTSD. Curr. Psychiatry Rep. 22 (19). https://doi.org/10.1007/s11920-020-1140-y (2020).
Onose, T. et al. Sex differences in post-traumatic stress disorder in cardiovascular patients after the great East Japan earthquake: A report from the CHART-2 study. Eur. Heart J. Qual. Care Clin. Outcomes. 3 (3), 224–233. https://doi.org/10.1093/ehjqcco/qcx009 (2017).
Yang, Y. et al. A follow-up study on the post-traumatic stress disorders among middle school students in Wenchuan earthquake region. Chin. J. Prev. Med. 45 (4), 354–358 (2011).
Wilker, S. et al. Sex differences in PTSD risk: evidence from post-conflict populations challenges the general assumption of increased vulnerability in females. Eur. J. Psychotraumatol. 12, 1930702. https://doi.org/10.1080/20008198.2021.1930702 (2021).
Yagi, A. et al. Changes in drinking behavior among evacuees after the Fukushima Daiichi nuclear power plant accident: The Fukushima health management survey. Fukushima J. Med. Sci. 66 (3), 133–142. https://doi.org/10.5387/fms.2019-24 (2020).
Kanehara, A. et al. Trends in psychological distress and alcoholism after the great East Japan earthquake of 2011. SSM Popul. Health. 2, 807–812. https://doi.org/10.1016/j.ssmph.2016.10.010 (2016).
Van Vliet, K. Springer New York, Shame and avoidance in trauma in Trauma Rehabilitation After War and Conflict: Community and Individual Perspectives 247–263 (2010). https://doi.org/10.1007/978-1-4419-5722-1_11
Lobban, J. & Murphy, D. Using Art therapy to overcome avoidance in veterans with chronic post-traumatic stress disorder. Int. J. Art Ther. : Inscape. 23 (3), 99–114. https://doi.org/10.1080/17454832.2017.1397036 (2018).
Silverstein, M. et al. Avoidance as an obstacle to preventing depression among urban women at high risk for violent trauma. Arch. Women’s Mental Health. 19 (1), 63–70. https://doi.org/10.1007/s00737-015-0521-4 (2016).
Sripada, R., Liberzon, I. & Garfinkel, S. Avoidant symptoms in PTSD predict fear circuit activation during multimodal fear extinction. Front. Hum. Neurosci. 7 https://doi.org/10.3389/fnhum.2013.00672 (2013).
Funding
This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (Ministry of Science and ICT; MSIT) (NRF-2023R1A2C2003043).
Author information
Authors and Affiliations
Contributions
C.Y: Conceptualization, Methodology, Writing(review & editing), Supervision, Project administration. S.H: Conceptualization, Methodology, Formal analysis, Investigation, Writing(original draf & review & editing).
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Choi, YJ., Song, H. Changes in citizens’ anxiety, depression, and PTSD after the Seoul Halloween crowd crush in 2022. Sci Rep 15, 30299 (2025). https://doi.org/10.1038/s41598-025-15634-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-15634-0
