
Abstract
Taste and smell are critical for food intake and maintaining adequate energy balance, particularly in isolated, confined, and extreme (ICE) environments. Hypoxic conditions, low humidity, and limited chemosensory exposure at Concordia Station in Antarctica may impair taste and smell functions, though research remains scarce. Gustatory and olfactory functions were assessed in 19 participants (39.2 ± 10.9 years) during two overwintering missions at Antarctic Concordia Station. Testing occurred six weeks pre-departure, three times during isolation, and six months post-isolation. Gustatory function was evaluated using ODOFIN Taste Strips; olfactory function using ODOFIN Sniffin’ Sticks. Additionally, subjective sensory reports were collected. Hyposmia increased during isolation, accompanied by a trend toward declining smell identification (p = 0.054), with limited follow-up data offering no clear evidence of recovery. Hypogeusia was primarily reflected in an elevated prevalence of reduced salt sensitivity during mid- to late isolation (p = 0.036), returning to baseline levels post-expedition. Subjective evaluations only partially aligned with psychophysical test results. A one-year stay at Concordia Station revealed individual variability in chemosensory responses, highlighting the sensitivity of taste and smell to environmental extremes. While causality remains unclear, the findings emphasize the need to monitor chemosensory function in extreme settings and constrained environments in everyday life.
Similar content being viewed by others

Introduction
Ensuring sufficient energy and nutrient intake is a critical challenge in isolated, confined, and extreme (ICE) environments1,2,3, where environmental stressors can impact physiological and psychological well-being. Despite adequate food availability4, individuals in ICE settings often fail to meet their daily caloric requirements3,5,6, leading to weight loss and potential nutrient deficiencies6,7,8,9. These deficits are particularly concerning during long-duration stays10,11,12,13,14, where maintaining physical and cognitive function is essential3.
Among several potential contributors, alterations in taste and smell are suggested to affect dietary choices and food intake in ICE environments15, though their exact impact remains unclear. Taste perception plays a crucial role in nutrient detection, meal completion, and satiety16. It encompasses hedonics and at least five basic qualities sweet, sour, salty, bitter, and umami17, which regulate dietary intake16. The olfactory system contributes to food perception and thus plays a significant role in appetite regulation, food preferences, and avoidance behaviors16. Orthonasal odors stimulate appetite and shape dietary choices16, while also detecting dangers, and supporting social communication.
In ICE environments, such as space missions, polar stations, or isolated confined controlled environments like bed rest studies, anecdotal reports confirm altered taste and smell perceptions15,18,19,20. However, experimental findings from ICE environments remain inconsistent, highlighting the disparity between subjective perception and measured chemosensory performance. Findings range from overall18,21,22,23,24,25 or selective declines26,27,28,29 in sensory function to stable performances 26,28,30 or even improvements18,31, possibly reflecting the variability in environmental stressors, exposure durations, and methodological frameworks across studies.
The Concordia Research Station in Antarctica provides a unique opportunity to examine chemosensory function in a high-altitude ICE environment characterized by chronic hypobaric hypoxia, extreme cold, low humidity, circadian disruption, and prolonged isolation32. Crews frequently report nasal congestion, dryness, and sore throat33, symptoms often linked to reduced nasal airflow and impaired olfactory function. Similar symptoms and chemosensory impairments have also been found in other high-altitude research settings24,25,27,28,29, where hypoxia, cold, and isolation create environmental conditions partially comparable to those at Concordia. However, findings across studies remain inconsistent, and longitudinal data from environments that combine multiple ICE-related stressors are scarce, leaving key aspects of chemosensory adaptation poorly understood. Disparities between subjective reports and objective measurements further complicate interpretation.
This study addresses these gaps by examining how prolonged exposure to an ICE environment affects olfactory and gustatory function. Changes were assessed before (T0, Pre), during (T1, February; T2, June; T3, October), and after (T4, Post) a one-year stay at Concordia Station in Antarctica. In addition to mapping changes in sensory performance over time, the relationship between smell and taste were explored and discrepancies between subjective reports and psychophysical test outcomes were examined.
By focusing on these questions, the study advances our understanding of human sensory adaptation under extreme conditions. These insights are not only relevant for sustaining well-being and performance in remote expeditions and long-duration spaceflights but may also inform how sensory perception is affected by isolation, monotony, and altered environments in everyday life—such as in long-term care, during pandemic lockdowns, or other socially constrained settings.
Results
Study population
The final analysis included 19 Caucasian participants (84.2% male; mean age: 39.2 ± 10.9 years). The baseline characteristics are presented in Table 1.
At baseline, participants had an average body mass index (BMI) of 26.40 ± 3.04 kg/m2. By the end of the Antarctic stay, the mean BMI had decreased by 1.09 units to 25.31 ± 3.37 kg/m2 but had increased by 1.66 units at the 6-month follow-up to 26.97 ± 3.13 kg/m2, exceeding baseline levels. Most participants were non-smokers at baseline (84.2%). During isolation, daily smoking declined, with 15.8% reporting occasional use. At follow-up, daily smoking returned to 15.8%, and occasional smoking dropped to 10.5%. All assessments were conducted by one of two trained study physicians, each responsible for all repeated measurements within a given study campaign. The physicians were not part of the study sample.
Hyposmia was frequently associated with taste-related issues, particularly those involving salty taste
At baseline, 4 of 19 participants (21%) were classified as hyposmic, which is slightly above the expected 17% for comparable populations34. Hyposmia prevalence increased to 5/19 (26%) at T1 and peaked at 7/19 (37%) at T2 and T3 (Fig. 1A), though these increases were not statistically significant (Cochran’s Q = 2.2, p = 0.534), likely because individual trajectories were highly variable over time (Supplementary Figure S1a). T4 was excluded from analysis due to limited participation in olfactory testing (n = 5).

Prevalence of hyposmia, hypogeusia, partial hypogeusia and their combined occurrence. Prevalence of hyposmia (a), hypogeusia (b), partial hypogeusia (c), and their combined occurrence (d, e) before isolation (Pre, N = 19), during isolation (T1 = February, T2 = June, T3 = October, N = 19), and six months post-isolation (Post, n = 15). (a) Threshold, Discrimination and Identification (TDI) score range: 0–48; hyposmia: 16.25–30.5; normosmia: ≥ 30.75. (b) Taste score range: 0–16; hypogeusia: < 9; normogeusia: ≥ 9. (c) Subnormal: < 2 (sweet/sour/salty), < 1 (bitter); shown as counts and %. (d) Co-occurrence of hyposmia and subnormal scores for salty (%). (e) Co-occurrence of hyposmia and subnormal scores for bitter (%).
Hypogeusia was present in 3/19 participants (16%) at baseline, which is 10% higher than expected in healthy reference populations35. During the Antarctic stay, hypogeusia prevalence peaked at T1 with 6/19 (32%) and decreased and stabilized at T2 and T3 with 4/19 (21%, Cochran’s Q = 2.5, p = 0.479). Post-isolation, 3/15 (20%) showed hypogeusia (Fig. 1B; Cochran’s Q = 1.9, p = 0.760). In line with olfactory impairments, hypogeusia varied across individuals and did not follow a consistent pattern over time (Supplementary Figure S1b).
To further examine these gustatory impairments, subnormal scores for individual taste qualities were analyzed for partial hypogeusia (Fig. 1C). At baseline, 3/19 participants (16%) had subnormal scores for sweet, salty, and bitter tastes, whereas 4/19 (21%) were considered subthreshold for sour. Bitter and sweet scores improved over time, while sour and salty perception worsened, with subnormal salty scores doubling at T2 and T3 (6/19; 32%). Notably, post-isolation, salty scores improved (1/15; 7%), but subnormal sour scores persisted (5/15; 33%). Although no statistically significant differences were found in the prevalence of subnormal scores over time, a decreasing trend was observed for subnormal salty scores across T0–T4 (n = 15; Cochran’s Q = 8.2, p = 0.085; Fig. 1C).
Co-occurrence of hyposmia and hypogeusia was observed in one participant at T0, in two at T1, and in three at both T2 and T3 (Cochran’s Q = 1.4, p = 0.697), as reflected in a medium correlation between overall taste and smell scores at T2 (ρ = 0.479, p = 0.038). Hyposmia co-occurred with subnormal salty scores (Fig. 1D), particularly at T2 and T3 (four cases each). However, significant correlations between salty taste and olfactory function were only observed at T3: salty taste scores at this time point were strongly associated with the overall TDI score (sum score for smell threshold, discrimination and identification subscores; ρ = 0.542, p = 0.016) and moderately correlated with the smell identification subscore (ρ = 0.461, p = 0.047). Furthermore, both participants with bitter taste dysfunction at T2 also exhibited hyposmia (Fig. 1E). This co-occurrence was supported by a moderate correlation between TDI and bitter identification scores at T2 (ρ = 0.497, p = 0.030), and a positive correlation between odor discrimination and the bitter scores (ρ = 0.596, p = 0.007). Supplementary Table S1 contains the full set of correlation results across time points.
Although salty taste exhibited the highest prevalence of subnormal scores, the highest concentration of bitter and sour taste strips was not identified by up to 26.3% of participants. Nevertheless, no statistically significant differences emerged in identification performance at the highest concentration across taste qualities, with recognition rates remaining relatively stable (sweet: 94.7–100% (Cochran’s Q = 4.4, p = 0.223); sour: 73.7–84.2% (Cochran’s Q = 1.4, p = 0.709); bitter: 73.7–84.2% (Cochran’s Q = 1.6, p = 0.666); salty: 78.9–84.2% (Cochran’s Q = 1.1, p = 0.771)). Complete failures to identify a taste at any tested concentration, indicating no recognition across all levels, were documented for bitter (up to 15.8%), salty (up to 10.5%), and sour (up to 5.3%), while sweet was consistently identified at least at one concentration throughout all time points.
Taste confusion patterns aligned with previous reports36. Bitter was often undetected, while sour and salty were frequently confused, suggesting overlapping perception. Sweet was occasionally misidentified, but errors seemed random. Most identification errors occurred at low stimulus intensity, likely reflecting reduced sensory input to the central nervous system.
Smell function and salty taste progressively declined during isolation
In line with the data for hyposmia, the smell identification scores tended to decrease over time (χ2(3) = 7.65, p = 0.054, Fig. 2A), indicating a progressive impairment in the ability to identify familiar odors. However, the trend was not supported by the Bayes factor (BF10 = 0.472). Changes in TDI score (F(2.11,37.95) = 1.92, p = 0.158, BF10 = 0.522), threshold (F(3,54) = 1.95, p = 0.132, BF10 = 0.600) and discrimination subscores (χ2(3) = 3.45, p = 0.327, BF10 = 0.360) over time did not reach statistical significance (Fig. 2B–D). An exploratory subgroup analysis (n = 5) was conducted to evaluate changes in olfactory function six months post-isolation (Supplementary Figure S2). TDI scores declined significantly from T0 to T4 (F(4,16) = 5.94, p = 0.004, BF10 = 10.871), along with reductions in threshold (F(4,16) = 5.63, p = 0.005, BF10 = 11.904) and identification subscores (χ2(4) = 10.36, p = 0.035, BF10 = 2.736), indicating a progressive decline in olfactory sensitivity and identification ability over time. Comparable TDI scores at T3 and T4 suggest persisting olfactory impairment post-isolation.

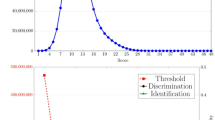
Olfactory performance over time. Test scores for overall smell score (combined Threshold, Discrimination and Identification (TDI) score) (a) with odor threshold (b), discrimination (c), identification subscores (d) were assessed before (Pre, N = 19) and during isolation (T1 = February, T2 = June, T3 = October, N = 19). Data shown as boxplots: median (─), mean (+), interquartile range (box), minimum (⟘), and maximum (⟙). Max scores: 16 per subtest, 48 total. Statistical trend: 0.05 ≤ p < 0.1.
Consistent with the overall pattern of hypogeusia—especially the increased occurrence of partial hypogeusia for salty taste—the salty identification score showed a significant change over time (n = 15, χ2(4) = 10.283, p = 0.036), though Bayesian analysis provided only weak evidence for this effect (BF10 = 1.047; Fig. 3A). Post hoc tests identified a significant reduction in salty taste identification scores at T2 compared to T4 (p = 0.033) and at T3 compared to T4 (p = 0.028), aligning with the upward trend observed in the prevalence rates of partial hypogeusia for salty taste (Fig. 1C). In contrast, no significant changes over time were observed in the identification scores for sweet (χ2(4) = 3.12, p = 0.538, BF10 = 0.095), sour (χ2(4) = 1.16, p = 0.884, BF10 = 0.074), or bitter tastes (χ2(4) = 3.19, p = 0.527, BF10 = 0.141), nor in overall taste identification (χ2(4) = 0.57, p = 0.966, BF10 = 0.071, Fig. 3B–E).

Gustatory performance over time. Taste identification scores are shown for salty (a), sweet (b), sour (c), bitter (d), and the total taste score (e) before isolation (Pre, N = 19), during isolation (T1 = February, T2 = June, T3 = October, N = 19), and six months post-isolation (Post, n = 15). Data shown as boxplots: median (─), mean (+), interquartile range (box), minimum (⟘), and maximum (⟙). Significant differences (p < 0.05) are marked (*). Max scores: 4 per subtest, 16 total.
A detailed summary of outcomes across all timepoints is presented in Supplementary Table S1.
Self-reported sensory changes were only partially reflected in psychophysical test results during isolation (T1–T3)
During isolation, changes in smell sensitivity were reported by 4/19 (21%), 7/19 (37%), and 5/19 (26%) of participants at T1, T2, and T3, respectively (Fig. 4A), with no significant differences between time points (Cochran’s Q = 1.4, p = 0.497). Initially, participants described reduced sensitivity and nasal congestion. By T3, however, three of the five participants mentioned an improvement. Assessing changes in olfactory sensitivity was described as challenging, likely due to the limited presence of odor stimuli during isolation. Self-reports only partially aligned with psychophysical test outcomes: while at T1, none of those reporting reduced smell met the criteria for hyposmia, alignment was observed in 3/7 at T2 and 2/5 at T3. This overall lack of alignment between self-reports and chemosensory tests was also reflected at the level of change scores, as perceived changes in smell sensitivity did not significantly correlate with measured changes in olfactory performance at any time point (Supplementary Table S1).

Psychophysical confirmed changes in subjective reports on olfactory and gustatory sensitivity. Frequency of subjects that reported changes in olfactory (a) and gustatory (b) sensitivity during the Antarctic stay (T1 = February, T2 = June, T3 = October, N = 19) and the proportion of psychophysical confirmed changes based on smell (a) and taste (b) tests. Results are presented as percentages (%).
Self-reported reductions in overall taste sensitivity were noted by 2/19 (11%) of participants at T1, 4/19 (21%) at T2, and 3/19 (16%) at T3 (Fig. 4B), with no significant differences across time points (Cochran’s Q = 1.2, p = 0.549). Perceived impairments in taste sensitivity were partially reflected in the psychophysical test results. At T1 and T2, 50% of participants who reported a decline in taste sensitivity were classified as hypogeusic, whereas none of the participants reporting a decline at T3 met the criteria for hypogeusia. However, perceived decline was significantly associated with the magnitude of change in measured salt taste perception, both from T0 to T1 (ρ = − 0.543, p = 0.016) and from T2 to T3 (ρ = − 0.499, p = 0.030).
Reported smell preferences commonly included nature-related odors (e.g., forest, flowers, rain) and food-related scents (e.g., vanilla, cinnamon) (Supplementary Figure S3a). Nearly half of participants (9/19, 47.4%) reported stable smell preferences across all time points, while the others showed variability or reported no preference at one or more time points. For taste, participants reported preferences for sweet (e.g., chocolate), sour (e.g., citrus fruits), and bitter flavors (e.g., vegetables or soft drinks) at T1, with sour tastes becoming more prominent at T2. Spicy foods were mentioned occasionally. By T3, participants mentioned a general appreciation of fresh fruits. Taste preferences remained stable across time points in most participants (11/19, 57.9%), with only minor variations or occasional missing responses (Supplementary Figure S3b).
Discussion
The primary objective of this study was to examine the effect of a prolonged stay in an ICE environment in Antarctica on olfactory and gustatory functions.
Hyposmia appeared to increase over time, accompanied by a downward trend in olfactory identification scores, reflecting substantial interindividual variability in sensory responses. While short-term hypoxia has been linked to olfactory changes24,28,29,37,38,39,40, the gradual impairment observed here suggests additional or delayed effects beyond constant hypobaric hypoxia. Reduced olfactory stimulation, as noted by a participant who reported difficulties in detecting changes due to limited odor exposure during isolation, may also be a contributing factor. This aligns with research indicating that olfactory stimulation is crucial for sustaining the function of the olfactory system 41,42. Additionally, consistent reports of nasal congestion and the prolonged exposure to low indoor humidity point to further environmental stressors that may have negatively impacted olfactory function32. While hypoxia, sensory deprivation, low humidity, and psychosocial stress are known to influence chemosensory function, the current study design does not allow for causal conclusions. However, the delayed onset of olfactory decline rather suggests that cumulative effects or additional factors may have contributed, though proposed mechanisms remain speculative.
Exploratory analysis six months post-isolation (T4) of five subjects revealed a significant decline in olfactory function compared to baseline, reflected in lower TDI, threshold, and identification scores. In the absence of documented upper respiratory tract infections, these are unlikely to explain the observed decline in olfactory function. Instead, factors such as prolonged sensory deprivation41,42 or cumulative in-mission effects32,33,41,42 may be more relevant. However, the significant interindividual variability observed at previous time points and the small sample size (n = 5) warrant cautious interpretation.
Partial hypogeusia appeared to increase, primarily reflecting a decline in salty taste sensitivity. The decline became most pronounced toward the end of the mission, suggesting possible long-term adaptation processes rather than acute effects27. Specifically, participants with partial hypogeusia showed reduced sensitivity to salty and sour tastes (both mediated by ion channels43), whereas their sensitivity to sweet and, to a lesser extent, bitter tastes (mediated by G protein-coupled receptors43) appeared to increase. The more pronounced increase in sweet taste perception may reflect an adaptive response to a higher daily caloric demand16. This response pattern has not been observed in other short- or long-term ICE studies44, and may provide new insight into how prolonged exposure to extreme environments affects taste perception. Concordia’s dry conditions, with low indoor humidity and variable outdoor humidity, may have contributed to these changes. Although there is limited direct evidence linking low humidity to taste changes, prolonged dryness could affect the oral mucosa45,46 due to fluid and electrolyte loss, which might influence how salty and sour tastes are perceived.
Additionally, the lack of olfactory stimuli at Concordia may have contributed to changes in taste sensitivity. Hyposmia is known to increase salt consumption47, which over time could reduce salt sensitivity48. Supporting this, participants with lower salt taste scores at T3 often showed hyposmia, and salty taste scores correlated with TDI scores, suggesting a compensatory increase in salt use47,48. After returning home, salt taste sensitivity seemed to normalize, likely due to better diet and environmental conditions. However, the prevalence of partial hypogeusia for sour remained high after isolation. This may be attributed to a combination of factors, including delayed mucosal recovery, limited exposure to acidic stimuli, and taste confusion. Given the many potential confounding factors, the causal relationships cannot be conclusively determined within the scope of this study. Although the sample size was sufficient to detect medium to large effects, further investigation is needed to clarify the underlying mechanisms, including potential sex-specific responses, interindividual variability in response to environmental stressors, and the impact of low test–retest reliability in taste measures49.
Olfactory and gustatory impairments did not consistently co-occur, but their correlation at T2 suggests partial interdependence. This aligns with previous findings: Stinton et al.50 found no clear effect of smell loss on taste, while Han et al.51 observed reduced taste sensitivity in individuals with smell disorders, although inconsistently. Similarly, Landis et al.52 reported a moderate decline in taste with long-term smell loss.
Notably, subjective reports of chemosensory impairments were less frequent than the impairments measured in the olfactory and gustatory tests. This limited agreement is well-documented in the literature, both in standard conditions53 and in other ICE environments, such as space missions19,20,30. Self-reported evaluations of olfaction in healthy, untrained individuals are often considered unreliable, influenced by nasal airflow rather than actual olfactory performance. This may be due to minimal attention typically given to smell in daily life53. In addition, subjective assessments of taste function have been shown to lack reliability35, with questionnaires54 often confirming the absence rather than the presence of impairments35. Taste dysfunction diagnosis is challenging due to several factors, including the low prevalence of impairments and misattribution of odor perception deficits to taste issues54. However, research during the COVID-19 pandemic showed that self-reports are reliable when impairments are severe or sudden55,56. Interestingly, three participants reported heightened smell sensitivity at the end of the Antarctic stay (T3), despite unchanged psychophysical measures, possibly due to odor deprivation enhancing occasional smells during isolation.
Participants frequently named natural odors, which were absent in the low-odor environment32, indicating sensory deprivation and a craving for natural stimuli. In several cases, these odors were associated with personal places of origin, suggesting an underlying sense of homesickness57. Food-related scents may be associated with comfort, indicating potential emotional coping58. Correspondingly, sweet taste preference was elevated early in isolation, possibly reflecting stress59,60 or higher energy demands during the active summer phase61.
Strengths and limitations
A key strength of this study is the unique year-long dataset from Concordia Station, collected under standardized ICE conditions. The repeated-measures design with five measurement points, including a baseline and a six-month follow-up, provides rare insights into the long-term progression of olfactory and gustatory functions. Validated tests were transported under controlled conditions and administered by trained crew members, ensuring high-quality results.
While the sample size (N = 19) is small, it exceeds typical ICE study cohorts (median N = 4–10)62,63. The predominantly male sample limiting sex-specific analyses, the lack of a control group, the relatively low test–retest reliability of the Taste Strips49 and incomplete follow-up data reduce generalizability. However, Bayesian inference and exploratory subgroup analyses helped mitigate some of these limitations. Above-normal baseline prevalence of chemosensory deficits in some participants may be a potential confounder. Causal attribution remains limited, as the study design does not allow for the distinct effects of hypoxia, low humidity, confinement, or sensory deprivation to be disentangled32.
Conclusion
This study suggests that prolonged exposure to an ICE environment, such as overwintering at Concordia Station, may lead to temporary and selective changes in smell and taste, with considerable individual variability. These findings highlight the potential benefit of increasing chemosensory stimulation during extended periods of isolation. While interpretability is limited by the sample size and study design, the findings nevertheless underscore the importance of monitoring chemosensory function in extreme settings—not only in polar and space missions, but also in other isolated or sensory-restricted environments such as submarines, remote work sites, or long-term care. Understanding these changes can help support appetite, mood, and well-being during prolonged confinement.
Methods
Study design
The study followed a repeated measures design with data collection at five time points (T0–T4): baseline (T0) six weeks before departure, during the Antarctic stay at the end of summer (February, T1), mid-winter (June, T2), and end of winter (October, T3), and at follow-up six months after return (T4). In line with the European Space Agency (ESA) protocol, this schedule captured long-term effects of the year-long mission at Concordia Station, which included continuous isolation from February to late October/early November. At each time point, standardized taste and smell tests were conducted to assess gustatory and olfactory function. Self-reported evaluations of taste and smell abilities were gathered via questionnaires during the isolation period (T1–T3).
Study setting
Concordia Station is located on the Antarctic Plateau at Dome C at 3233 m (10,607 ft) above sea level. Due to low barometric pressure, this corresponds to a physiological altitude of approximately 3800 m, resulting in chronic hypobaric hypoxia with inspired oxygen partial pressures at 21% O₂ ranging between 132 and 136 hPa (99.01–102.01 mmHg). The environment is characterized by extreme cold, low humidity, minimal microbial exposure, sensory deprivation, and the absence of natural light during the polar night32. Key environmental characteristics are summarized in Table 2. Concordia Station is jointly operated by the French Polar Institute (IPEV) and the Italian Antarctic Program (PNRA) and serves as a multidisciplinary research platform, enabling a wide range of scientific investigations in fields such as astronomy, glaciology, atmospheric sciences, and human physiology. During the Antarctic winter, the station hosts up to 13 crew members and remains completely isolated for nine months. Meals are prepared daily by professional chefs using mostly shelf-stable, frozen, or canned foods, with limited availability of fresh fruits and vegetables. As one of the most remote and environmentally extreme research stations on Earth, Concordia Station serves a validated analog for spaceflight, providing valuable insights into human adaptation in ICE environments and supporting the development of countermeasures to maintain health and performance.
Study population
This study included a convenience sample of 22 Caucasian volunteers (77.3% male; mean age: 38.1 ± 10.7 years, range: 24–56 years), comprising all crew members of the 2019/2020 and 2021/2022 overwintering teams at the Antarctic Concordia research station. No data were collected during the 2020/2021 season due to COVID-19-related operational restrictions. Crew members underwent a rigorous recruitment process coordinated by PNRA and IPEV in collaboration with ESA. The process included medical, physiological, and psychological evaluations, as well as interviews, to confirm participants’ physical fitness and psychological suitability for enduring prolonged isolation and extreme environments. Due to missing baseline data (n = 2) and one dropout after baseline assessment, the final sample consisted of 19 participants (84.2% male; mean age: 39.2 ± 10.9 years). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Ethics Committee of the University Hospital Tübingen, Germany (NCT03746145). Written informed consent was obtained from all participants prior to enrollment.
Data collection
The commercial taste and smell test kits were transported to Concordia station under controlled temperature conditions to prevent freezing, ensuring their integrity and reliability. All kits were used within their recommended shelf-life and stored appropriately. According to manufacturer guidelines, repeated use during the study period does not compromise test validity. At each time point, assessments were performed by one of two trained study physicians, each responsible for all repeated measures within a campaign.
Olfactory function was assessed using the validated ODOFIN Sniffin’ Sticks® test (blue kit; Burghart Messtechnik GmbH, Holm, Germany), which measures odor threshold (T, single-staircase procedure), discrimination (D, 16 odorant triplets, three-alternative forced choice), and identification (I, 16 common odorants, four-alternative forced choice). Each subtest has a maximum score of 16, resulting in a combined TDI score ranging from 1 to 48, with higher scores indicating better olfactory performance64. Tests were conducted under standardized, postprandial morning conditions. Five distinct randomization protocols were used for threshold and discrimination subtests (Supplementary Table S2) to determine the sequence and position of target pens and to reduce carry-over effects. No randomization was applied for the identification subtest, as participants received no feedback after testing, thereby minimizing potential learning effects across sessions. According to normative data, olfactory function was classified as anosmia (TDI ≤ 16), hyposmia (TDI 16.25–30.5), or normosmia (TDI 30.75–41.25)34,65. The assessment protocol and its clinical relevance are described in detail elsewhere34,66, highlighting its established use in both clinical and research settings.
Gustatory function was assessed using standardized ODOFIN Taste Strips® (Burghart Messtechnik GmbH, Holm, Germany), representing the four basic taste qualities that were impregnated with four graded concentrations of the respective stimuli (sweet: 0.4, 0.2, 0.1, 0.05 g/mL sucrose; sour: 0.3, 0.165, 0.09, 0.05 g/mL citric acid; salty: 0.25, 0.1, 0.04, 0.016 g/mL sodium chloride; bitter: 0.006, 0.0024, 0.0009, 0.0004 g/mL quinine hydrochloride)49,67,68. The test includes 16 impregnated filter paper strips and 2 blanks, presented in randomized order (Supplementary Table S2). Correct identifications were summed to a total taste score (range: 0–16), with subscores (0–4) for each quality. Blank strips were excluded from scoring. The full methodological protocol follows established guidelines67,68. According to normative criteria, hypogeusia was defined as a total score below the 10th percentile (< 9 points), and partial hypogeusia as reduced sensitivity to specific taste qualities (sweet, sour, salty < 2; bitter < 1)68, allowing more detailed interpretation compared to the olfactory tests. Assessments were performed under preprandial, controlled conditions in the morning, with instructions to abstain from food, beverages (except water), smoking, or oral hygiene one hour prior. Tests were conducted with open nares. This method is validated for adult use and widely applied in both clinical and research settings, as described in detail elsewhere68,69,70.
To complement the psychophysical assessments, participants completed a non-standardized self-report on chemosensory perception several days after psychophysical testing. The use of such self-report measures is a well-established procedure in chemosensory research, particularly for capturing individual sensory experiences that may not be fully reflected in standardized tests55,71. The self-reports were obtained several days after the psychophysical testing to minimize immediate test-related bias. In addition to reporting perceived changes in odor and taste preferences, participants were also asked whether they had noticed any alterations in their ability to perceive smells or tastes. Responses were provided in free-text format.
Statistical analysis
Data analysis was performed using SPSS 28.0.0.0 (SPSS Inc, Chicago, Illinois), JASP 0.18.1 (Intel) (JASP Team, 2023; https://jasp-stats.org/), and GraphPad Prism 10.1.1 for visualization. The main analyses (T0–T3) included 19 participants, with sufficient power (0.81) to detect medium-to-large effects (f = 0.28) via repeated measures F-test (α = 0.05; G*Power 3.1.9.7)72. Follow-up data (T4) were available for 5 participants (olfaction) and 15 participants (taste). No relevant baseline differences were found between these subgroups and the full sample.
Data are reported as mean ± SD, and frequencies are given in absolute values and percentages (%). Reference values for dysfunction prevalence were derived using weighted means.
Normally distributed data were analyzed using one-way repeated measures ANOVA, with Greenhouse–Geisser correction applied where appropriate. Non-normally distributed data were analyzed using Friedman tests. For binary variables, Cochran’s Q test was used to evaluate differences over time. Spearman’s ρ was used to calculate correlations between variables, given the ordinal nature of self-ratings and the non-normal distribution of test scores.
Significance was set at p < 0.05. Bayesian repeated measures ANOVA (prior width = 0.5) complemented frequentist results. Bayes factors (BF₁₀) quantified evidence strength: BF₁₀ > 1 supports H₁, < 1 supports H₀; values between 1–3 or 0.33–1 indicate weak, 3–10 or 0.1–0.33 moderate, and > 10 or < 0.1 strong evidence, respectively.
Data availability
The data that support the findings of this study are available from the corresponding author, IM, upon reasonable request.
References
Levi, J. An extraterrestrial sandwich: The perils of food in space. Endeavour 34, 6–11 (2010).
Smith, S. M., Rice, B. L., Dlouhy, H. & Zwart, S. R. Assessment of nutritional intake during space flight and space flight analogs. Procedia Food Sci. 2, 27–34 (2013).
Smith, S., Zwart, S., Douglas, G. & Heer, M. Human Adaptation to Spaceflight: The Role of Nutrition (National Aeronautics and Space Administration Lyndon B. Johnson Space Center, 2021).
Nutrition in Spaceflight and Weightlessness Models. (Lewis Publishers, 2000).
Heer, M., De Santo, N. G., Cirillo, M. & Drummer, C. Body mass changes, energy, and protein metabolism in space. Am. J. Kidney Dis. 38, 691–695 (2001).
Smith, S. M., Zwart, S. R., Block, G., Rice, B. L. & Davis-Street, J. E. The nutritional status of astronauts is altered after long-term space flight aboard the international space station. J. Nutr. 135, 437–443 (2005).
Bergouignan, A. et al. Towards human exploration of space: The THESEUS review series on nutrition and metabolism research priorities. NPJ Microgravity 2, 16029 (2016).
Heer, M., Baecker, N., Zwart, S. & Smith, S. Interactions Among artificial gravity, the affected physiological systems, and nutrition. In Artificial Gravity Vol. 20 (eds Clément, G. & Bukley, A.) 249–270 (Springer, 2007).
Smith, S. M. Nutritional Biochemistry of Space Flight (Space Science, Exploration and Policies Series). (Nova Science Publishers Incorporated, 2009).
Johnson, P. C., Rambaut, P. C. & Leach, C. S. Apollo 16 bio energetic considerations. Nutr. Metab. 16, 119–126 (1974).
Lane, H. W., Smith, S. M., Rice, B. L. & Bourland, C. T. Nutrition in space: Lessons from the past applied to the future. Am. J. Clin. Nutr. 60, 801S-805S (1994).
Lane, H. W. et al. Energy intake, body weight, and lean body mass are maintained in healthy, active women consuming a US space shuttle diet. J. Am. Diet. Assoc. 94, 87–88 (1994).
Rambaut, P. C., Leach, C. S. & Whedon, G. D. Metabolic energy requirements during manned orbital Skylab missions. Life Sci. Space Res. 15, 187–191 (1977).
Simpson, A. The effect of Antarctic residence on energy dynamics and aerobic fitness. Int. J. Circumpolar Health 69, 220–235 (2010).
Taylor, A. J. et al. Factors affecting flavor perception in space: Does the spacecraft environment influence food intake by astronauts?. Compr. Rev. Food Sci. Food Saf. 19, 3439–3475 (2020).
Boesveldt, S. & de Graaf, K. The differential role of smell and taste for eating behavior. Perception 46, 307–319 (2017).
Bachmanov, A. et al. Genetics of taste receptors. Curr. Pharm. Des. 20, 2669–2683 (2014).
Baranski, S. et al. Electrogustometric investigations during manned space flight. Aviat. Space Environ. Med. 54, 1–5 (1983).
Olabi, A., Lawless, H., Hunter, J., Levitsky, D. & Halpern, B. The effect of microgravity and space flight on the chemical senses. J. FOOD Sci. 67, 468–478 (2002).
Seddon, M. R., Fettman, M. J. & Phillips, R. W. Practical and clinical nutritional concerns during spaceflight. Am. J. Clin. Nutr. 60, 825S-830S (1994).
Enck, P. et al. Almost Nothing - Not Even Bariatric Surgery for Obesity - Changes Olfactory Sensitivity. J. Res. Obes. https://doi.org/10.5171/2014.491890 (2014).
Iakovleva, I. I. Electrometric study of the human taste analyzer normally and in the modelling of weightlessness. Vestn. Otorinolaringol. 15–17 (1982).
Bershad, E. M. et al. Marked olfactory impairment in idiopathic intracranial hypertension. J. Neurol. Neurosurg. Psychiatry 85, 959–964 (2014).
Rahne, T., Köppke, R., Nehring, M., Plontke, S. K. & Fischer, H.-G. Does ambient noise or hypobaric atmosphere influence olfactory and gustatory function?. PLoS ONE 13, e0190837 (2018).
Maga, J. A. & Lorenz, K. Effect of altitude on taste thresholds. Percept. Mot. Skills 34, 667–670 (1972).
Vickers, Z. M., Rice, B. L., Rose, M. S. & Lane, H. W. Simulated microgravity [bed rest] has little influence on taste, odor or trigeminal sensitivity. J. Sens. Stud. 16, 23–32 (2001).
Singh, S. B. et al. High altitude effects on human taste intensity and hedonics. Aviat. Space Environ. Med. 68, 1123–1128 (1997).
Huppertz, T. et al. Reduction of olfactory sensitivity during normobaric hypoxia. Auris Nasus Larynx 45, 747–752 (2018).
Altundağ, A. et al. The effect of high altitude on olfactory functions. Eur. Arch. Otorhinolaryngol. 271, 615–618 (2014).
Watt, D. G. et al. Canadian medical experiments on Shuttle flight 41-G. Can. Aeronaut. Space J. J. Aeronaut. Spat. Can. 31, 215–226 (1985).
Fleisch, A. Die Reizschwellen Des Druck-Und Geschmacksinnes Im Hochgebirge. (1944).
Van Ombergen, A., Rossiter, A. & Ngo-Anh, T. J. ‘White Mars’—nearly two decades of biomedical research at the Antarctic Concordia station. Exp. Physiol. 106, 6–17 (2021).
Mairesse, O. et al. Preparing for Mars: Human sleep and performance during a 13 month stay in Antarctica. Sleep 42, zsy206 (2019).
Oleszkiewicz, A., Schriever, V. A., Croy, I., Hähner, A. & Hummel, T. Updated sniffin’ sticks normative data based on an extended sample of 9139 subjects. Eur. Arch. Oto-Rhino-Laryngol. 276, 719–728 (2019).
Welge-Lüssen, A., Dörig, P., Wolfensberger, M., Krone, F. & Hummel, T. A study about the frequency of taste disorders. J. Neurol. 258, 386–392 (2011).
Doty, R. L., Chen, J. H. & Overend, J. Taste quality confusions: Influences of age, smoking, PTC taster status, and other subject characteristics. Perception 46, 257–267 (2017).
Bigdaj, E. V., Bezgacheva, E. A., Samojlov, V. O. & Korolyev, Y. N. The effects of hypoxic hypoxia on olfactory sensitivity in humans. Biophysics 63, 463–468 (2018).
Kuehn, M., Welsch, H., Zahnert, T. & Hummel, T. Changes of pressure and humidity affect olfactory function. Eur. Arch. Otorhinolaryngol. 265, 299–302 (2008).
Mazzatenta, A., Bondi, D., Di Giulio, C. & Verratti, V. Olfactory response to altitude hypoxia: A pilot study during a Himalayan trek. In Olfactory Response to Altitude Vol. 1375 (ed. Pokorski, M.) 55–61 (Springer, 2022).
Ruffini, R. et al. Adaptation of olfactory threshold at high altitude. In Neurotransmitter Interactions and Cognitive Function Vol. 837 (ed. Pokorski, M.) 19–22 (Springer, 2014).
Chen, B., Boesen, A., Olesch, F. T. & Hummel, T. A life without smell: Olfactory function in people working in odorless rooms. Laryngoscope 134, 382–387 (2024).
Wu, K. N., Tan, B. K., Howard, J. D., Conley, D. B. & Gottfried, J. A. Olfactory input is critical for sustaining odor quality codes in human orbitofrontal cortex. Nat. Neurosci. 15, 1313–1319 (2012).
Doyle, M. E., Premathilake, H. U., Yao, Q., Mazucanti, C. H. & Egan, J. M. Physiology of the tongue with emphasis on taste transduction. Physiol. Rev. 103, 1193–1246 (2023).
Gregson, R. A. M. An application of gustatory psychophysics in Antarctica. Chem. Senses 3, 141–147 (1978).
Guarnieri, G., Olivieri, B., Senna, G. & Vianello, A. Relative humidity and Its impact on the immune system and infections. Int. J. Mol. Sci. 24, 9456 (2023).
Nagda, N. L. & Hodgson, M. Low relative humidity and aircraft cabin air quality: Aircraft cabin air quality. Indoor Air 11, 200–214 (2001).
Henkin, R. I. Effects of smell loss (hyposmia) on salt usage. Nutrition 30, 690–695 (2014).
Sari, A. N., Farapti, F. & Md Nor, N. Salt taste threshold as a detection of salt intake in hypertensive individuals. J. Berk. Epidemiol. 10, 227–236 (2022).
Fjaeldstad, A., Niklassen, A. S. & Fernandes, H. M. Re-test reliability of gustatory testing and introduction of the sensitive taste-drop-test. Chem. Senses 43, 341–346 (2018).
Stinton, N., Atif, M. A., Barkat, N. & Doty, R. L. Influence of smell loss on taste function. Behav. Neurosci. 124, 256–264 (2010).
Han, P. et al. Decreased electrogustometric taste sensitivity in patients with acquired olfactory dysfunction. Rhinol. J. 56, 158–165 (2018).
Landis, B. N. et al. Chemosensory interaction: Acquired olfactory impairment is associated with decreased taste function. J. Neurol. 257, 1303–1308 (2010).
Landis, B. N. Ratings of overall olfactory function. Chem. Senses 28, 691–694 (2003).
Soter, A. et al. Accuracy of self-report in detecting taste dysfunction. Laryngoscope 118, 611–617 (2008).
Parma, V. et al. More than smell-COVID-19 is associated with severe impairment of smell, taste, and chemesthesis. Chem. Senses 45, 609–622 (2020).
Nguyen, H. et al. Covid-19 affects taste independent of taste-smell confusions: Results from a combined chemosensory home test and online survey from a large global cohort. Chem. Senses 48, bjad020 (2023).
Van Puyvelde, M. et al. Living on the edge: How to prepare for it?. Front. Neuroergonomics 3, 1007774 (2022).
Spence, C. Comfort food: A review. Int. J. Gastron. Food Sci. 9, 105–109 (2017).
Zhang, X. et al. Social isolation, brain food cue processing, eating behaviors, and mental health symptoms. JAMA Netw. Open 7, e244855 (2024).
Mastrogiovanni, N. A., Wheeler, A. K. & Clemens, K. J. Social isolation enhances cued-reinstatement of sucrose and nicotine seeking, but this is reversed by a return to social housing. Sci. Rep. 11, 2422 (2021).
Prinz, P. Sweetness preference and its impact on energy intake and body weight—A review of evidence. Front. Nutr. 10, 1289028 (2023).
Klos, B. et al. Effects of isolation and confinement on gastrointestinal microbiota—A systematic review. Front. Nutr. 10, 1214016 (2023).
Klos, B. et al. Effects of isolated, confined and extreme environments on parameters of the immune system—A systematic review. Front. Immunol. 16, 1532103 (2025).
Kobal, G. et al. Multicenter investigation of 1,036 subjects using a standardized method for the assessment of olfactory function combining tests of odor identification, odor discrimination, and olfactory thresholds. Eur. Arch. Otorhinolaryngol. 257, 205–211 (2000).
Hernandez, A. K. et al. Olfactory nomenclature: An orchestrated effort to clarify terms and definitions of dysosmia, anosmia, hyposmia, normosmia, hyperosmia, olfactory intolerance, parosmia, and phantosmia/olfactory hallucination. ORL 85, 312–320 (2023).
Hummel, T., Sekinger, B., Wolf, S. R., Pauli, E. & Kobal, G. ‘Sniffin’ sticks’: Olfactory performance assessed by the combined testing of odour identification, odor discrimination and olfactory threshold. Chem. Senses 22, 39–52 (1997).
Landis, B. N. et al. ‘Taste strips’—A rapid, lateralized, gustatory bedside identification test based on impregnated filter papers. J. Neurol. 256, 242–248 (2009).
Mueller, C. et al. Quantitative assessment of gustatory function in a clinical context using impregnated ‘taste strips’. Rhinology 41, 2–6 (2003).
Sauer, H. et al. Changes in gustatory function and taste preference following weight loss. J. Pediatr. 182, 120–126 (2017).
Wolf, A., Illini, O., Uy, D., Renner, B. & Mueller, C. A. A new extension to the taste strips test. Rhinol. J. 54, 45–50 (2016).
Gerkin, R. C. et al. Recent smell loss is the best predictor of COVID-19 among individuals with recent respiratory symptoms. Chem. Senses 46, bjaa081 (2021).
Faul, F., Erdfelder, E., Buchner, A. & Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 41, 1149–1160 (2009).
Acknowledgements
The authors gratefully acknowledge the participants for their valuable contribution to this study. I.M. acknowledges support by the German Aerospace Center (DLR), grant number 50WB1920. The authors acknowledge the European Space Agency (ESA), French Polar Institute (IPEV) and the Italian National Antarctic Research Programme (PNRA) for their support and collaboration in the framework of the ICELAND project. Special thanks to the ESA Human Exploration Science Support team for their valuable input. All authors thank the Open Access Publishing Fund of Tübingen University for support.
Funding
Open Access funding enabled and organized by Projekt DEAL. I.M. acknowledges support by the German Aerospace Center (DLR), grant number 50WB1920.
Author information
Authors and Affiliations
Contributions
Writing—original draft: BK; Writing—review & editing: BK, SW, KO, ST, HH, PE, IM; Conceptualization: BK, SW, IM; Investigation: BK, SW; Methodology: BK, SW, KO, ST, HH; Supervision: IM; Project administration: PE, IM; Validation: KO, IM; Funding acquisition: PE, IM; Visualization: BK.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Klos, B., Wolf, S., Ohla, K. et al. Effects of one year of extreme isolation in Antarctica on olfactory and gustatory functions. Sci Rep 15, 32369 (2025). https://doi.org/10.1038/s41598-025-16900-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-16900-x
