
Abstract
China launched a major health-care reform in 2009 aimed to provide all citizens with equal access to basic health care with reasonable quality and financial risk protection. Since then, China has made substantial progress toward Universal Health Coverage (UHC). However, the access of UHC among internal migrants might be disadvantaged compared with local residents. This study aimed to provide an assessment of inequalities and trends in internal migrants’ access to Universal Health Coverage. Six rounds (2013–2018) of the China Migrants Dynamic Survey were used including 976,430 respondents. Financial protection was measured using the basic medical insurance enrollment proportion (BMIEP) and hospital reimbursement rate (HRB). Essential health services were measured using the standardized health record establishment proportion (SHREP) and standardized health education intervention coverage (SHEIC). The Erreyers Index (EI) and Wagstaff Index (WI) were used to measure socio-economic related UHC inequalities. The process of the Recentered Influence Function (RIF)-Ordinary Least Squares (OLS) method was used to decompose risk factors of the EI and WI. The average coverage rate of SHREP and SHEIC were 24.3% and 75.7%, respectively. The average coverage rate of BMIEP and the percentage of HRB were 87.4% and 58.3% respectively. Regarding inequalities, it was found that for SHREP and SHEIC, the general trends of inequalities raised while for BMIEP, the general trends decreased. Regarding HRB, it was less inequalities in 2018 compared with 2014. RIF-OLS regression showed that both individual factors and regional factors contributed to the inequalities in UHC among China’s internal migrants. Progress has been made in financial protection of migrants as the high coverage of BMIEP and its decrease in inequalities as well as lower inequalities in 2014 of HRB compared with 2018. While challenges remained in the lower coverage rate of SHEIC and increasing inequalities of SHREP and SHEIC. Policy efforts on narrowing down both individual and regional inequalities should be put forward.
Similar content being viewed by others
Introduction
The pursuit of Universal Health Coverage (UHC) – defined as equitable access to quality services without financial hardship1 – stands as a cornerstone of the United Nations’ 2030 Sustainable Development Agenda2. China’s 2009 health-care reform marked a pivotal step toward this goal, prioritizing nationwide social health insurance expansion and financial risk protection3. By 2023, this reform had significantly improved healthcare accessibility for the general population4. However, a critical unresolve challenge persists: systemic disparities in UHC access for internal migrants, a population exceeding 374 million (26% of China’s total population) as of 20205.
China’s UHC implementation remains constrained by the hukou system, an administrative framework tying social service entitlements to one’s registered birth place6. While reforms have expanded coverage to local residents, migrants face persistent institutional barriers including limited probability of insurance benefits across regions7, elevated out-of-pocket expenditures and underutilization of urban health facilities compared to local residents8.
The evidence regarding the impact of these reforms on trends and equity in the context of UHC is rather limited. Although a nationwide cross-sectional survey focusing on health insurance and financial protection among internal migrants in China has recently been published9, it lacks a historical perspective. Moreover, the existing literature on internal migrants in China and their access to health services has predominantly concentrated on specific health issues, such as maternal health or mental health10,11, with a notable absence of comprehensive studies on access to public health services. Previous research tracking China’s progress towards UHC has primarily targeted the general population and centered on hospital-based care and financial risk protection4,12. There is a significant gap in research assessing China’s recent trends towards UHC among vulnerable populations, particularly in terms of preventive services13. Therefore, measuring the trends of UHC among China’s internal migrants and incorporating preventive services coverage trends would greatly enhance the current body of knowledge. Additionally, analyzing the trends of UHC among migrants could offer valuable insights to the international community regarding the issue of migrants.
The present study aims to provide a more accurate assessment of trends and inequalities in access to health protection schemes and essential public health services (EPHSs) among China’s internal migrants over time. Additionally, risk factors of presenting inequalities would also be explored.
Methods
Study design and data sources
Six rounds (2013–2018) of the China Migrants Dynamic Survey (CMDS: https://www.chinaldrk.org.cn/wjw/#/home) were used in this study. The CMDS is an annual, national cross-sectional survey conducted by the National Health Commission of the People’s Republic of China, covering 31 provinces (districts and cities) and the Xinjiang Production and Construction Corps in China using a stratified, multi-stage, and proportionate-to-size (PPS) method for sampling. The study focuses on the status and access of migrants to health insurance and EPHSs in China. The respondents were internal migrants aged 15–59 years, who have lived outside their registered place of residence (county or city) for at least 1 months. Figure 1 presents data cleaning procedure of the sample. In total, 1,075,279 respondents completed the survey in six rounds of CMDS. As we focus on internal migration, cross-border migration was excluded from the analysis. And because the EPHSs cover population who reside in current place for at least 6 months, migrants with migration duration of less than 6 months were also excluded from the analysis. After excluding cross-border migration and within 6 months of migration duration, 978,152 respondents were included. Excluding 1722 respondents without reporting socio-economic status, there were 976,430 respondents included in descriptive analysis. After excluding 154 respondents who did not report marital status or migration scope, 976,276 respondents were included in equity analysis. All methods were carried out in accordance with relevant guidelines and regulations. We confirm that the informed consent was obtained from all subjects and/or their legal guardians.

Data cleaning procedure of the sample.
Measurements
Following the WHO and World Bank framework14 we measured UHC progress from two dimensions: coverage of essential health services and financial protection due to health-care costs. We chose two fundamental health services focused on prevention which targeted the whole population : the standardized health record establishment proportion (SHREP) and the standardized health education intervention coverage (SHEIC). The financial protection was measured using two indicators due to the essence of protecting population under health insurance coverage and reducing cost sharing: the basic medical insurance enrollment proportion (BMIEP) and the hospitalization reimbursement rate (HRB) (Table 1).
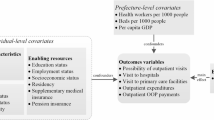
SES index generation
To analyze equity in UHC, we generate a socio-economic indicator (SES). The concept of SES refers to an individual’s relative material and social standing compared to others15. Using a single indicator to measure socioeconomic status may not adequately reflect an individual’s complex socioeconomic circumstances or situation. Integrating various socioeconomic factors into a single index provides valuable insights to a comprehensive socioeconomic gradient of inequities in UHC. In this study, SES was quantified by combining income condition, educational level, and occupation status. Income condition was measured using per capita monthly household income, calculated as follows:
Average Indexed Monthly Earnings (AIME) = individual’s per capita monthly income/national per capita monthly income.
The data for “national per capita monthly income” were obtained from the Statistical Yearbook16 published by the National Bureau of Statistics of China.
Actual per capita monthly household income = total monthly household income/number of household members.
Subsequently, the AIME was divided into six equal categories numerically, ranked from 1 to 6 representing the lowest to highest income groups.
Education was categorized into six levels: illiteracy = 1, primary school = 2, junior high school = 3, senior high school or technical secondary school = 4, junior college = 5, and undergraduate or above = 6.
According to the occupation classification from China’s State Statistics Bureau, the 8 general categories of occupation were consistently used throughout 1999 to 2022, which was classification used in the CMDS questionnaire. Our study used the occupational reputation developed by a previous study based on the 8 general categories17. Occupations were then rated on a 5-level scale: domestic helpers/agriculture/no fixed job/unemployed = 1, employees/self-employed = 2, middle class (employers) = 3, white-collar workers = 4, leaders = 5.
To create a composite SES index, Principal Components Analysis (PCA) was utilized. This method has been validated as a robust approach for describing SES differentiation within a population18. Factor scores were computed by weighting the raw responses with the factor loadings of the PCA. Bartlett’s Test of Sphericity showed: χ²3 = 225046.177, p < 0.001, rejecting the null hypothesis that the variables are uncorrelated. Meanwhile, the KMO measure of sampling adequacy was 0.619 (> 0.6), indicating that the data are suitable for factor analysis. The PCA extracts common factor variance percentage of 52.653%. Higher scores indicate higher levels of SES.
Statistical analysis
We did statistical analyses in STATA software 17.0. Descriptive analysis of basic demographic characteristics and UHC indicators were conducted.
Measuring socioeconomic-related UHC inequalities
Traditional measurement of inequalities, like the conventional concentration index (CI) has two drawbacks as below. Firstly, for bounded variables, the CI may depend on the mean of the health variable, making comparisons of populations with different mean health levels problematic19. Therefore, it is not suitable for tracking longitudinal inequalities with different mean health levels. Secondly, the CI does not satisfy the “mirror property”, that is, inequalities in health do not “mirror” those in ill-health20.
Wagstaff21 and Erreygers19 proposed different correction mechanisms to deal with these problems. In this study, we focused on Erreygers’ Index (EI) since it is the only one that measures quasi-absolute inequalities, i.e., it is insensitive to any feasible equal addition to the health variable. The Wagstaff Index (WI) measures relative differences and hence, it is possible that it gives larger inequalities than the Erreygers index when prevalence is low, as is the case for the prevalence in some unhealthy lifestyles. Thus, the EI and WI together could complement each other and provide better measures for longitudinal data to measure changes of inequalities over time.
The EI and WI can be written as.


where ai is the range of bounded variables, ai∈[amin, amax]. Ri is the relative rank of the ith individual in the socioeconomic status distribution. Bounded variable can be retransformed into an indicator of the proportional deviation from the minimum value: bi. This lies on the range [0, 1] and records only “real” changes in the underlying attribute, not “nominal” ones due to the choice of measurement scale. Under this transformation, the Erreygers and Wagstaff indices simplify, respectively, to.


The range of both the Wagstaff Index (WI) and Erreygers Index (EI) is −1 to + 1. When the value falls within the range of [−1,0) or (0,1], it indicates the presence of inequalities in UHC that favors either low or high socioeconomic status (SES) groups. If the value is negative (−1 < WI/EI < 0), it suggests the existence of UHC inequalities in favor of the lower SES group. Conversely, if the value is positive (0 < WI/EI < 1), it indicates UHC inequalities in favor of the higher SES group. The magnitude of the WI and EI values reflects the depth or extent of inequality. The larger the absolute value of WI or EI, the greater the level of inequality in health outcomes between different socioeconomic groups.
Decomposition of risk factors of inequalities in UHC
The process of the Recentered Influence Function (RIF)- Ordinary Least Squares (OLS) method is to use the recentered influence function (RIF) estimates of the UHC inequality index to find the relationship between the RIF and the explanatory variables and establish the regression function between the UHC inequality index and the explanatory variables to achieve causal recognition. The method is mainly divided into two steps. The first step is to estimate the RIF value of the WI and EI, and the second step is to use the RIF estimation value of the health inequality index as the explanatory variable and various factors X as explanatory variables to implement the OLS regression process22.
Results
Trends in access to health insurance and essential services
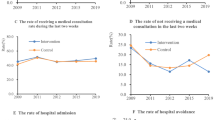
Individuals involved were comparable in most socio-demographic factors across survey years, but we observed an increasing trend education level and age, which was consistent to recent migration trends in China (Table 2). The average SHREP between 2013 and 2018 was 24.3%, indicating a less optimistic situation regarding documentation. During the period from 2013 to 2016, the SHREP showed an increasing trend, particularly between 2015 and 2016. However, from 2017 to 2018, the rate sharply declined. The average SHEIC between 2014 and 2018 was 78.4%, indicating a higher proportion of the population receiving health education. The years 2015 had the highest rates of SHEIC. For BMIEP, it remained consistently high (> 80%) with minimal fluctuations and peaked at 93.4% at 2018. Compared to 2014, the number of individuals receiving reimbursement for hospitalization significantly increased in 2018 (Table 3; Fig. 2). Probit regression showed that after controlling other factors, BMIEP experienced a general increase during the observation period while the SHEIC witnessed a general reduction. The SHREP increased at the beginning but decreased in later period. Compared with 2014, the HRB was higher in 2018 (Table 4; Fig. 3).

Trends of coverage of standardized health record establishment proportion, standardized health education intervention coverage, basic medical insurance enrollment proportion and hospitalization reimbursement rate.

Adjusted trends of coverage of standardized health record establishment proportion, standardized health education intervention coverage, basic medical insurance enrollment proportion and hospitalization reimbursement rate. Note: Age, gender, education, marital status, migration scope, migration duration, indexed average monthly wage, region, economic belt area, occupation were adjusted.

Trends of inequality index of coverage of standardized health record establishment proportion, standardized health education intervention coverage, basic medical insurance enrollment proportion and hospitalization reimbursement rate. Note: WI: Wagstaff Inde, EI: Erreygers Index.
Inequalities in access to health insurance and essential services
Regarding the trends of inequalities in coverage of SHREP, from 2013 to 2015, it was the lower SES group was in better situation than the higher SES group. Nevertheless, from 2016 onwards, the lower SES group was in worse situation than the higher counterpart and the inequalities continued to enlarge. For inequalities in SHEIC, the relative terms (WI) witnessed an increasing trend from 2014 to 2018 with number larger than 0, indicating enlarging inequalities favor higher SES group. While for absolute terms (EI), the year 2015 had largest decreasing rate of inequalities and afterwards, the inequalities increased until 2017. In terms of BMIEP, as it was a binary indicator, we mainly consider the results of EI. EI in BMIEP showed that the inequalities remained in favor of the higher SES group with fluctuation over time and had the lowest level in 2018. For HRB, due to limits to the data, we can only compare the 2018 situation with the 2014 one. It indicated that inequalities that favor higher SES groups decreased.
Decomposition of risk factors of inequalities
Results of RIF-OLS showed that age exaggerated inequalities in SHREP. Compared to males, females were more likely to experience inequalities. Compared to illiteracy, higher education groups had less inequalities in SHREP. Single migrants had lower risk of experiencing inequalities in SHREP. Larger migration scope increased inequalities in SHREP. Migrants with longer migration duration experienced lower levels of inequalities in SHREP. Higher income groups enjoyed higher level of equitable SHREP compared with lower ones. In terms of region, a negative coefficient indicating the Western region has a lower level of inequalities in SHREP while a positive coefficient representing that the Central and Eastern region has higher level of inequalities (both compared to the Northeastern region). For the economic zones, the Yangtze River Delta and Circum-bohai Sea economic zones enjoyed higher level of equitable HR coverage while the Pearl River Delta enjoyed less level. Compared with the initial year of 2013, the inequalities in SHREP decreased in 2014 and 2015 then increased in the following two years then dropped downed in 2018 again. Except for the 1 st level of occupation as babysitting and agricultural occupations and 5th level as leading groups, all the other occupation groups experienced lower level of inequalities in the SHREP (Table 5).
Results of RIF-OLS regression in SHEIC inequality index showed that younger, women, higher education level, marital status as not single, larger migration scope, shorter migration duration, lower income level suffered more from inequalities in SHEIC. Compared to Northeastern region, Western region had the largest inequalities in SHEIC. Compared to other regions, Pearl River Delta, Yangtze River Delta and Circum-bohai Sea experienced lower level of inequalities in HE coverage. For occupation, the 5th occupation levels showed higher inequalities in SHEIC whereas the 2nd to 4th levels presented lower inequalities compared with the 1 st level. Regarding year, the year 2014 experience the lowest inequalities compared with year 2015 to 2018 (Table 6).
RIF-OLS regression results in BMIEP inequality index found that higher age, female, primary school education or above, higer income level, economic zones than others, 2014 (compared with 2013) had less inequalities. Married, cross-provinces and cross cities (compared with cross counties), longer migration duration, living outside Northeastern regions, had higher inequalities in BMIEP. For occupation, compared with the 1 st level, the 2nd to the 3rd level had showed less inequalities while the 4th and the 5th presented higher inequalities in BMIEP (Table 7).
For risk factors of HRB inequalities index, higher age, female, higher income group, the Bohai Rim, they Year of 2018 had lower inequalities while higher education group, married, larger migration scope, regions outside the Western region faced higher inequalities. For occupation, compared with the 1 st category, the 2nd and the 3rd enjoyed lower inequalities whereas the 4th and the 5th had higher inequalities (Table 8).
Discussion
To the best of our knowledge, the current study is the first to measure inequalities and trends in UHC among China’s internal migrants with focus on preventive services. Our data for indicators were taken from the latest six rounds of nationally representative household surveys, including a large-scale sample of 976,430 individuals, in China. Notable progress has been made in the BMIEP with general steady increase and in the SHEIC with comparatively high coverage rate while the SHREP experienced fluctuations with relatively low rate. The HRB had significant improvements in 2018 compared with 2014 (Figs. 2 and 3). Inequalities in the SHREP, the SHEIC increased in general trends over time while the BMIEP generally decreased over time. Inequalities in the HRB dropped down in 2018 compared with 2014 (Fig. 5). Risk factors of the inequities included individual level factors: gender, education, income, marital status, occupation, migration duration, migration scope and contextual factors: region, economic zone.

Adjusted trends of inequality index of standardized health record establishment proportion, standardized health education intervention Coverage, basic medical insurance enrollment proportion and hospitalization reimbursement rate.
Our study highlights potential drivers for UHC promotion, mainly policy efforts. The steady increase of BMIEP and improvements in HRB together with decrease in inequities of BMEIP and HRB might be associated with efforts in financial protection put forward by the 2009 healthcare reform and the 2016 reform of health insurance to merge the Urban Residents Basic Medical Insurance and the New Rural Cooperative Medical Scheme, which both increased health insurance coverage among the whole population including migrants and prevented them from financial risks to some extents. For the increase in SHEIC, it coincided with the policy efforts in equalization of EPHSs (2014) among internal migrants with 1 year time-lag indicating the SHEIC increased one year after (2015) these policy efforts. These indicated to achieve UHC among the vulnerable groups such as migrants, sustained and targeting policy efforts are needed.
Though progresses have been made, this study also reveal that challenges remained in UHC among migrants, including the low rate of SHREP and HRB and the intensified inequities in SHREP and SHEIC. According to the goals set up by the National Commission of Health and Family Planning in 2017, the SHREP and the SHEIC among migrants should reach 80% and 95%, respectively by 202023. The current SHREP was 24.3% averagely from 2013 to 2018, indicating the process toward the target was far left behind. For SHEIC, the average coverage rate was 78.4% with the maximum coverage rate of 91.5% in 2015, which seems much closer to the target compared to the SHEIC. However, the inequities in SHEIC intensified (Fig. 5). The higher SES groups enjoyed increasingly higher probability of receiving health education services in the observation period. This was consistent with a study measuring health inequalities among China’s population which found that there was “pro-rich” health inequality in 2012–2016 and the extent of health inequality was the biggest in 201624. This might due to the higher SES group might have better health literacy and knowledge on EPHSs so they utilized more.
According to our findings, both individual factors and contextual factors were identified as risk factor of inequalities in UHC indicators. This was consistent with the Anderson Model25 which identified age, gender, education, occupation and income as individual factors and region related factors as contextual factors. In other words, the driver of inequalities of UHC consisted of both individual level socio-economic status and migration characteristics as well as regional socio-economic status. China’s decentralized and fragmented health system bring regional differences in resource preparation and service delivery. More developed regions are therefore having more service provision. However, internal migrants normally migrate from less developed region to more developed region which have heavy burdens providing services to enlarging population. In addition, the enjoyment of local public services is currently based on the hukou system indicating migrants cannot benefit in local areas.
The purpose of UHC is to ensure that all people have accessible, affordable and quality health provision, regardless of their wealth, gender or other circumstances26. It is therefore of great importance to measuring UHC progress from an equity perspective. Previous studies have discussed UHC progress among different education levels, income groups and regions12,27, the current study employed a SES approach which comprehensively reflect individual’s socio-economic status, providing adding value to the current knowledge. The current study focused on the vulnerable population- internal migrants in China, revealing that vulnerable groups need more attention in the way toward UHC and there might be further inequities in access to UHC within these groups. To compete these challenges, policy should incline to the “poor among the vulnerable”. Additionally, by employing WI and EI, the current study measuring inequalities in both absolute and relative terms, adding new approaches to current studies which mainly adopted the concentration index28,29, the slope index of inequalities and the relative index of inequalities30. The WI and EI satisfied the mirror conditions as they exhibit a property where the conclusions drawn from longitudinal analysis remain symmetry in analyzing changes in health inequality over time, therefore they are suitable for current longitudinal study.
The current study was the first attempt to analyze the inequalities and trends of migrants’ access to health insurance and EPHSs from a horizontal perspective using a national representative sample. Previously, migrants were under representative in national studies measuring progress toward UHC12. However, there were also two limitations. Firstly, due to the data availability, we did not include the catastrophic health expenditure to measuring financial protection and other EPHSs service coverage data to measuring essential health services. Secondly, data were based on self-reports and are therefore subject to bias, which could be especially problematic for questions about the utilization of essential health services.
In conclusion, remarkable and steady increases in BMIEP accompanied by the decreases in OOP and the decreases in inequalities in BMEIP and HRB proportion. Major advances were made in achieving financial protection against risk while greater attention is needed to improve the utilization of EPHSs among internal migrants. Firstly, there is a need of a shared digital health record integration across regions to address the current fragmented status. Secondly, more attractive and vivid policy propaganda on EPHSs should be provided to migrants to increase their awareness and further their utilization. Thirdly, targeted subsidies for health education programs in underserved areas should be provided to narrow down the inequalities in SHEIC at regional level. Lastly, the “poor of the vulnerable”-migrants with the lower SES status need to be the focus of policy targets to achieve the equalization of EPHSs among migrants as well as UHC.
Data availability
The data that support the findings of this study are available from National Commission of Health and Family Planning, People’s Republic of China. Restrictions apply to the availability of the data.
References
World Health, O. The World Health Report: Health Systems Financing: the Path To Universal Coverage (World Health Organization, 2010).
General Assembly of the United Nations. Transforming our world: the 2030 Agenda for Sustainable Development United Nations. 1–35. (2015) .
Yip, W. et al. 10 years of health-care reform in china: progress and gaps in universal health coverage. Lancet 394 (10204), 1192–1204 (2019).
Yip, W. et al. Universal health coverage in China part 1: progress and gaps. Lancet Public. Health. 8 (12), e1025–e34 (2023).
Finance; MoHRaSSMoHMo. Interim measures for the transfer and continuation of basic medical insurance for migrant workers. In: PRC tCPsGot, editor. Beijing (2009).
Cheng, T. & Selden (ed, M.) The origins and social consequences of china’s Hukou system. China Q. 139 644–668 (1994).
Peng, Y., Chang, W. & Zhou, H. al. e. Factors associated with health-seeking behavior among migrant workers in beijing, China. BMC Health Serv. Res. 10 (69), 1–10 (2010).
Mou, J. et al. Health care utilisation amongst Shenzhen migrant workers: does being insured make a difference? BMC Health Serv. Res. 9 (214), 1–9 (2009).
Chen, W. et al. Social health insurance coverage and financial protection among rural-to-urban internal migrants in china: evidence from a nationally representative cross-sectional study. BMJ Global Health. 2(4), 1–13 (2017).
Gu, H. et al. Internal migration and maternal health service utilization in jiangsu, China. Trop. Med. Int. Health. 22 (2), 124–132 (2017).
Zhan, S., Sun, Z. & Blas, E. Economic transition and maternal health care for internal migrants in shanghai, China. Health Policy Plann. 17 Suppl, 47–55 (2002).
Meng, Q. et al. Trends in access to health services and financial protection in China between 2003 and 2011: a cross-sectional study. Lancet 379 (9818), 805–814 (2012).
Feng, X. L., Zhang, Y., Hu, X. & Ronsmans, C. Tracking progress towards universal health coverage for essential health services in china, 2008–2018. BMJ Glob Health. 7 (11), 1–14 (2022).
World health organization, world bank. Monitoring progress towards universal health coverage at country and global levels: framework, measures and targets. World Health Organization. (2014).
Townsend, P., Phillimore, P. & Beattie, A. Health and Deprivation: Inequality and the North. 1st edition ed: Routledge; (1988).
China Statistical Yearbook [Internet]. China Statistics Press. . https://www.stats.gov.cn/sj/ndsj/2018/indexch.htm (2018).
Li, C. Prestige stratification in contemporary Chinese society: measurement of occupational prestige and socioeconomic status index. Sociol. Stud. 01(02), 74–102 (2005).
Vyas, S. & Kumaranayake, L. Constructing socio-economic status indices: how to use principal components analysis. Health Policy Plann. 21 (6), 459–468 (2006).
Erreygers, G. Correcting the concentration index. J. Health. Econ. 28 (2), 504–515 (2009).
Clarke, P. M., Gerdtham, U. G., Johannesson, M., Bingefors, K. & Smith, L. On the measurement of relative and absolute income-related health inequality. Soc. Sci. Med. 55 (11), 1923–1928 (2002).
Wagstaff, A. The bounds of the concentration index when the variable of interest is binary, with an application to immunization inequality. Health Econ. 14 (4), 429–432 (2005).
Heckley, G., Gerdtham, U-G. & Kjellsson, G. A general method for decomposing the causes of socioeconomic inequality in health. J. Health. Econ. 48, 89–106 (2016).
General office of the national health and family planning commission. Basic Public health and family planning services for the migrant population equalization assessment programme Beijing. http://www.nhc.gov.cn/ldrks/s7851/201707/2248023a33ad423198d29df8828960a8.shtml (2017).
Li, J. W. & Jin, F. An empirical study on the inequality in health and healthcare in china’s medical reform. J. Environ. Public. Health. 2022, 5789118 (2022).
Andersen, R. M., Davidson, P. L. & Baumeister, S. E. Improving access to care in America. Changing the US health care system: key issues in health services policy and management 3a edición San Francisco: Jossey-Bass. 3–31. (2007).
World health organization. The world health report – health systems financing: the path to universal coverage. Geneva: World Health Organization. (2010).
World health organization, the world bank. Tracking universal health coverage: 2021 global monitoring report. Geneva: world health organization and international bank for reconstruction and development / the world bank (2021).
Umuhoza, S. M. & Ataguba, J. E. Inequalities in health and health risk factors in the Southern African development community: evidence from world health surveys. Int. J. Equity Health. 17 (1), 52 (2018).
Al-Hanawi, M. K. Decomposition of inequalities in out-of-pocket health expenditure burden in Saudi Arabia. Soc. Sci. Med. 286, 114322 (2021).
Taniguchi, H. et al. Equity and determinants in universal health coverage indicators in iraq, 2000–2030: a National and subnational study. Int. J. Equity Health. 20 (1), 196 (2021).
Funding
No funding.
Author information
Authors and Affiliations
Contributions
YJ, YZ and CC contributed to the conception and the design of the work. KW, XQ, XK, TC, XW, YD contributed to the data analysis and interpretation of data. YZ drafted the work. All authors have approved the submitted version and have agreed both to be personally accountable for the author’s own constitutions and to ensure the questions related to the accuracy and integrity of any part of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
This was secondary analysis of publicly available data, and no participant consent forms were required to access this data set. This study was exempted from ethical review by Peking University Institutional Review Board (No. IRB00001052–16011).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zheng, Y., Wang, K., Qin, X. et al. Inequalities and trends in access to health insurance and essential public health services among internal migrants in china: 2013 to 2018. Sci Rep 15, 31830 (2025). https://doi.org/10.1038/s41598-025-17282-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-17282-w
