
Abstract
Perioperative hyperglycemia is associated with increased morbidity and mortality. We report the findings of our quality improvement project on the use of an electronic insulin dosing calculator (EIC) to reduce intraoperative hyperglycemia in a cohort of cardiac surgical patients. A pilot and a modified EIC were sequentially implemented in adult patients undergoing cardiopulmonary bypass (CPB) procedures. Outcome measures (average blood glucose (BG) before, during and after CPB), process measures (percent EIC implementation) and balancing measures (incidence of hypoglycemia and average insulin doses utilized) were compared between baseline (no-protocol), pilot and modified EIC periods. 248, 142, and 239 patients were enrolled during the baseline, pilot and modified EIC phases, respectively. The EIC was implemented in 97% (138 out of 142 patients) during the pilot phase and in 86% of patients (206 out of 240 patients) during the modified EIC phase. Average BG levels on CPB were highest at baseline compared with pilot and modified EIC phases (mean, SD, 209 mg/dl,+/-45), vs. 189.8,+/-38 mg/dl vs. 188 mg/dl, +/-40) mg/dl, respectively, p = 0.002). Mean BG values were highest at baseline compared to pilot and modified EIC phases at end of procedure (182.4, +/-49 mg/dl, vs. 122, +/-30 mg/dl, vs.123.3, mg/dl, +/-38.3, vs., respectively, p = < 0.001) and at the ICU (164 ,+/-44.4, mg/dl, vs. 140, +/-37.9 mg/dl, vs. 143.4, +/-36 mg/dl, respectively p = < 0.001). Hypoglycemia was significantly lower during EIC phase compared with baseline (1% vs. 7%, p = 0.008). Less insulin was used during the pilot and modified EIC phases compared to baseline (15.2, +/-10.3, U vs. 15.8, +/-10.2 U, vs. 31.6 +/-20.27 U, respectively, p = 0.006). These preliminary findings suggest EIC effectiveness in reducing intraoperative hyperglycemia in patients undergoing CPB.
Similar content being viewed by others

Introduction
Intraoperative hyperglycemia, defined as blood glucose levels > 180 mg/dl, occurs in about 60%-80% of patients undergoing cardiopulmonary bypass (CPB)- requiring cardiac surgery. Uncontrolled intraoperative hyperglycemia is associated with increased morbidity, mortality, lengths of stay and hospital costs in the cardiac surgical population1,2. Hyperglycemia may occur in patients with an established diagnosis of diabetes or in isolation of diabetes (stress hyperglycemia). Stress hyperglycemia occurs due to a shift in the balance between the anabolic hormone insulin and the catabolic counter regulatory hormones towards the latter, leading to an accelerated glycogenolysis and gluconeogenesis coupled with a reduction in glucose uptake by tissues3. Recent literature suggests potential insulin degradation through hemolysis of red blood cells rather than adhesion on artificial surfaces of CPB systems. Stress hyperglycemia per se is associated with worse outcomes compared to hyperglycemia that occur in conjunction with diabetes4. Furthermore, 40% of patients encountering stress hyperglycemia progress to diabetes within the first year of hospital discharge. As a result, a reduction in intraoperative blood sugar to levels below 180 mg/dl became a quality benchmark recommended by the Society of Thoracic Surgeons (STS)5,6. Additionally, the Joint Commission and the Centers for Medicare and Medicaid (CMS) have incorporated postoperative blood glucose control in the Surgical Care Improvement Project (SCIP) to be used in the pay for performance programs as a quality benchmark7,8.
To adjust for the dynamic insulin requirements in the operating room setting, intravenous short acting insulin preparations is the preferred preparation for glucose control in this setting.
Despite the adaptability of intravenous (IV) insulin preparations to the dynamics swings of intraoperative blood glucose levels, human-based protocols are associated with substantial variability in insulin dosing, frequency of glucose checks and errors in calculations, all may paradoxically lead to suboptimal glucose control and adverse outcomes9.
Compared to human-based protocols, electronic insulin calculators (EIC) overcome many of the shortcomings of human based protocols10. Additionally, as composite protocols, insulin calculators can more accurately predict and account for insulin resistance in a large population of patients11. Herein, we report our initial experience with the EIC in reducing intraoperative hyperglycemia in a cohort of CPB-requiring cardiac surgical patients.
Materials and methods
Patient information in the form of demographic characteristics, comorbidities, blood glucose (BG) levels on admission, intraoperatively and post operatively in the ICU and floor, and admission HbA1c were abstracted from the electronic medical records. Venous blood samples were used for glucose measurements. Our institutional protocol entails measurements of BG every 20 min intraoperatively. We calculated the average BG values pre, during and post CPB. The pre bypass period extended from the first blood sample after conduction of general anesthesia till the initiation of CPB. CPB period extended from the initiation till the end of CPB. The post CPB period extended from end of CPB until the end of the procedure.
Context
This quality improvement project was conducted at our institutional Main Hospital at the cardiovascular surgical operating rooms (CVOR). Adult patients undergoing CPB-requiring cardiac surgeries were eligible for the study. Patients undergoing non-CPB requiring, and minimally invasive cardiac surgeries were excluded from the study. The University of Alabama Institutional Review Board (IRB) approved the study (IRB-300006438).
Stakeholders
A multidisciplinary effort by multiple stakeholders contributed to the design, development and implementation of the IV electronic insulin calculator (EIC) at the Cardiothoracic Anesthesiology Division at UAB including departments and specialties of Cardiac Anesthesia, Critical Care, Endocrinology, Nursing Anesthesia, Pharmacy, Clinical Informatics, Nursing Informatics, and Information Technology. A project charter was created by the interdisciplinary team for the project.
QI methodology
A (Plan-Do-Study-Analyze, PDSA) cycle was initiated on this project after collection of baseline data. Baseline data were collected to address the state of the hyperglycemia problem in our population. The second PDSA cycle was initiated to collect data on the pilot EIC protocol to assess the efficiency of the pilot protocol in controlling intraoperative hyperglycemia and to identify potential areas for improvement that led to the initiation of the modified EIC protocol.
Baseline period
A representative sample of baseline data (10/01/2019 until 10/31/2019) was used. Pareto charts were depicted to describe the frequency of cases for that period. Control charts were depicted to demonstrate the mean blood glucose levels over three intraoperative time intervals: pre-, on-, and post-CPB and at anesthesia end to describe the current process and identify areas for improvement.
A pre-intervention flow map was created to address the following areas of improvement during the baseline period (Fig. 1):
-
1.
Absence of a standardized insulin concentration bags;
-
2.
Absence of a standardized process for bolus dosing for insulin;
-
3.
Absence of standardized process for insulin infusion during the procedure;
-
4.
Interruption of insulin infusion between the operating room and ICU upon transfer of patients from the operating room to the intensive care unit (ICU).

Pre-intervention flow map representing the baseline period. The process starts when patient is in the operating room and ends in the intensive care unit. oval-shaped areas are beginning and end sections of the process. Trapezoid areas are decision-making points. Rectangular areas are phases of the process. (?) represent varaibility of the baseline process. CVOR: cardiovascular operating room; ICU: intensive care unit.
Measures
The following measures were sought at baseline, pilot and after initiation of the modified EIC.
-
a.
Outcome measures: average blood glucose levels at: pre-CPB, on- CPB, post- CPB, at anesthesia end, and on arrival to the intensive care unit (ICU).
-
b.
Process measures: proportion of patients on whom the EIC was successfully implemented.
-
c.
Control measures:
-
i.
incidence of hypoglycemia defined as blood glucose levels < 70 mg/dl at end of procedure.
-
ii.
total amount of insulin utilized intraoperatively.
Intervention
The team addressed potential areas for improvement and was able to create standardized premixed insulin bags that were delivered from the central pharmacy to the CVOR before the start of each case (Fig. 2). We learned from previous EIC experience in our hospital that EIC was successfully implemented in the trauma and burn intensive care unit (TBICU) at UAB in 2018 to control hyperglycemia in patients suffering from stroke and those who are recovering from different neurosurgical procedures. These patients suffer from stress responses that may lead to hyperglycemia which may worsen the stroke. We theorized that the stroke stress response may mimic the CPB- induced stress response and hence the EIC, with some modifications, may be extrapolated for use in the CVOR. After consulting with the TBICU team and our endocrinologists and taking into consideration the dynamics of CPB-requiring surgeries, the clinical characteristics of our cardiac surgical population, and workflow of the CV Division, our development team designed a revised algorithm to target an intraoperative blood glucose level of 140–180 mg/dl for overall insulin titration logic. The EIC was completely integrated in the electronic medical record. A provider places an order for the insulin infusion with the linked rate after the patient is electronically admitted to the cardiac operating room. Ordering providers were educated on the new orders via an online educational module as well as super user training. An excel sheet was placed on a shared CV Division common drive to encourage providers to share their feedback and to report any episodes of hyper/hypoglycemia with the pilot EIC protocol. An order template was created with an initial default insulin sensitivity coefficient (ISC) or multiplier of 0.02. The ‘multiplier’ is an index of a patient’s insulin sensitivity or resistance with higher values reflecting greater resistance and lower sensitivity. It helps calculate how much insulin to give based on how high the blood sugar is: a higher multiplier means more insulin is needed to lower any given blood glucose. The original multiplier was 0.02, and that is why we recommended that as the starting point. It was derived from a regression analysis of the White et al. algorithm12 which studied a small group of lean subjects with type 1 diabetes who has mostly what we would consider normal insulin sensitivity. However, recognizing that a fixed multiplier (like 0.02) is not suitable for all patients, especially those with insulin resistance (type 2 diabetes/obese), illness, or stress, Davidson at al. suggested using a dynamic multiplier13. Our insulin calculator uses a dynamic multiplier, which adjusts automatically based on how effectively the blood glucose is lowering, it increases if the glucose is not falling fast enough, and it decreases if the glucose is falling too fast, to reduce the risk of hypoglycemia.
This template was based on simulation experimentation by our development team to accommodate to the expected and known increase in insulin resistance on CPB. If an override to the standard settings is needed, the provider was presented with an electronic option that would deactivate the EIC and a recovery form to recover the protocol after inactivation. The calculator was initiated when the BG increases above 180 mg/dl. To limit glucose excursions, parenteral nutrition, and vasoactive medications were accounted for in the template for EIC. The insulin infusion was continued from the CV operating room to the ICU upon transport of patients (supplementary material 1, the insulin calculator protocol). The same ISC was maintained through the modified iteration of the EIC.
A flow chart was created to address process measures for the pilot phase in the form of (Fig. 2):
-
1.
Variability among providers in activating the EIC;
-
2.
Variability among procedures in selecting the insulin multiplier using in EIC in response to hyperglycemia on CPB;
-
3.
Frequent events of hypoglycemia at the end of procedure particularly during bed delays.

Flow chart after initiation of pilot phase electronic insulin calculator addressing areas for improvement at the baseline phase. Oval-shaped areas are beginning and end sections of the process. Trapezoid areas are decision-making points. CVOR: cardiovascular operating room; ICU: intensive care unit; EIC: electronic insulin calculator.
PDSA cycle 1
A modified version of the EIC was developed and implemented by the team with the following changes:
-
1.
Electronic adjustment of the EIC for type of cardioplegia solution delivered during CPB;
-
2.
Standardizing the trigger to activate the EIC at 180 mg/dl;
-
3.
Standardizing the discontinuation of the EIC at 90 mg/dl;
-
4.
Creating an electronic insulin protocol for treating hypoglycemia activated at a blood glucose level of 70 mg/dl.
-
5.
When our insulin infusion calculator was used for patients receiving the dextrose-containing Buckberg Blood for cardioplegia, it was significantly more challenging to maintain the patient’s blood glucose within the target range. We reviewed the higher insulin requirements of this patient population with the Director of the Division of Endocrinology, who recommended increasing the value of the recommended multiplier - and the resulting insulin infusion rate - by 50% only while the patient is receiving Buckberg Blood cardioplegia. We added a Cardioplegia Adjustment checkbox to the insulin calculator for anesthesia providers to indicate when the patient is receiving Buckberg Blood, which modifies the formula to effect this 50% increase. To minimize the potential for error, the code behind the insulin calculator only displays this Cardioplegia adjustment box while the patient is located in the CVOR.
-
6.
The modified EIC was initiated on 11/16/2021. Data were collected by the team from 11/16/2021 through 2/28/2022.
Statistical analysis
Pareto charts were used to describe the frequency of procedures at baseline. Control charts were used to measure the variation in blood glucose levels pre/on and post CB and at anesthesia end at baseline pilot and modified protocol phases. Flow charts were used to describe process measures at the 3 phases. Descriptive statistics were performed. Continuous variables were reported as means and standard deviations (SD) or median and interquartile ranges (IQR), as appropriate. Discrete variables were reported as percentages and proportions, as appropriate. One way analysis of variance (ANOVA) or Kruskal-Wallis test was used to compares the means of continuous variables, as appropriate. Chi squared test was used to analyze binary outcomes. A statistical level of significance was chosen at an alpha value of 0.05. Analyses were conducted using QI Macrosinc SPC Software for EXCEL 2022 and STATA SE 18.
Results
Baseline phase
The baseline phase included 248 patients. CABGs were the most frequent procedure performed during the baseline phase CABG, followed by ‘multiple procedures’, ‘valves’, ‘aortic surgeries’ and ‘miscellaneous’. Mean blood glucose levels at pre-, on- and post-CPB, at anesthesia end and first ICU BG were 142 (+/-35.6) mg/dl, 209 (+/-45) mg/dl, 186.7 (+/-45.6) md/dl, 182.4 (+/49) mg/dl, and 164 (+/-44.4) mg/dl, respectively. The average amount of intraoperative insulin used was 31.6 (+/-20.27) U (Table 1).
Pilot phase
A total of 142 patient charts were analyzed. The most frequent procedure performed during this period was CABG followed by ‘aortic aneurysms’, ‘multiple procedures’, ‘valves’ and ‘miscellaneous’. Mean blood glucose values at pre-, on- and post-CPB, at anesthesia end and first ICU were: 132 (+/-30) mg/dl, 189.8 (+/-37.7) mg/dl, 185.4 (+/-37.6) mg/dl, 122 (+/-30) mg/dl, and 140(+/-37.9) mg/dl, respectively. The average amount of intraoperative insulin used was 15.8 (+/-10.2) U (Table 1).
Modified EIC phase
A total of 239 patient charts were analyzed. The most frequent procedures performed were ‘multiple procedures’ followed by CABG, ‘valves’, ‘aortic surgeries’ and ‘miscellaneous’ (Fig. 3). Mean blood glucose levels at pre-, on- and post-CPB and at anesthesia end were 136.5 (+/-32.4) mg/dl, 188.2 (+/-40.2) mg/dl, 190 (+/-34.8) mg/dl, 123 mg/dl, and 123.3 (+/-38.3) mg/dl, 143.4(+/-36) respectively. The average amount of intraoperative insulin used was 15.2 (+/-10.3) U (Table 1).
Pre/post EIC implementation analysis
The EIC was implemented in 97% of patients (138 out of 142 patients) during the pilot phase and in 86% of patients (206 out of 239 patients) during the modified EIC phase. No significant differences existed in pre-CPB and post-CPB mean blood glucose levels between the three protocol implementation periods. Average BG levels on CPB were highest at baseline compared with pilot and modified EIC periods (mean, SD, 209 mg/dl,+/-45), vs. 189.8,+/-38 mg/dl vs. 188 mg/dl, +/-40) mg/dl, respectively, p = 0.002). Mean BG values were highest at baseline compared to pilot and modified EIC phases at end of procedure (182.4, +/-49 mg/dl, vs. 122, +/-30 mg/dl, vs.123.3, mg/dl, +/-38.3, vs., respectively, p = < 0.001) and at the ICU (164 ,+/-44.4, mg/dl, vs. 140, +/-37.9 mg/dl, vs. 143.4, +/-36 mg/dl, respectively p = < 0.001) (Fig. 4). Hypoglycemia was significantly lower during EIC phases compared with baseline (1% vs. 7%, p = 0.008, chi sq.). Less insulin units were used during the pilot and modified EIC phases compared to baseline (15.2, +/-10.3, U vs. 15.8, +/-10.2 U, vs. 31.6 +/-20.27 U, respectively, p = 0.006), (Table 1) (Supplementary material 2- example of patient’s blood glucose sampling course).

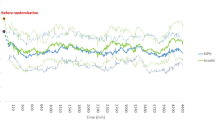
A-D Control charts of baseline, pilot and modified EIC protocol phases. A On CPB average blood glucose. B Anesthesia end average blood glcuose. C First intensive care unit average blood glcuose. D Mean insulin levels at baseline, pilot and modified protocol phases. UCL: upper control limit, CL: control limit; LCL: lower control limit; BG: blood glucose; ICU: intensive care unit; CPB: cardiopulmonary bypass. BL: baseline; EIC: electronic insulin calculator. UCL and LCL represent 2 standard deviations above and below the mean.

A-D Box plots representing the median and interquartile ranges of blood glucose values at the three study phases; baseline, pilot and modified. A cardiopulmonary bypass, B Anesthesia end; C First intensive care unit average blood glcuose; and D insulin levels at baseline, pilot and modified protocol phases. BL: baseline.
Discussion
In this study, we demonstrate that EIC resulted in a significant reduction in mean BG at during CPB, at procedure end, and in the first BG reading at the ICU. Additionally, EIC was associated with less hypoglycemic episodes, and less amount of insulin utilized intraoperatively. The EIC, in its pilot phase, resulted in lower SHR compared with baseline and the modified EIC Phases.
Our study is an extension of previous studies that have used automated insulin protocols during CPB14,15. In a randomized controlled study, Kaddoum el al. demonstrated the superiority of an automated insulin dosing system compared to standard of care in patients undergoing CPB. The authors demonstrated less incidence of hyperglycemia and a tighter glycemic control compared to human-based systems. Compared to the Kaddoum’s study that was exclusively performed on diabetic patients, our study included a larger sample size, reported on hypoglycemia, and included diabetic and non-diabetic patients. The latter is an important consideration as it reports on stress hyperglycemia in non diabetic patients that is associated with adverse outcomes. Additionally, the EIC, contrary to Kaddoum’ system was advantageously embedded in the electronic health record. While a study by Herzig’s et al.15. demonstrated the superiority of a subcutaneous insulin closed loop system in attaining sustained glycemic control with less incidence of hyper or hypoglycemia in diabetic patients undergoing non-cardiac surgery, the utility of subcutaneous insulin during in a rapidly changing blood glucose values context such as CPB remains to be studied.
While implemented mainly in the operating room, our results agree with previous studies that used electronic insulin dosing postoperatively in CPB-requiring cardiac surgeries. Chancellor et al.8demonstrated a significant reduction in hyperglycemic events with the use of an electronic insulin protocol coupled with an endocrinology consult service. In comparison, our study used a different cut-off for hyperglycemia (180 mg/dl vs. 200 mg/dl). Additionally, the definition the authors’ protocol, was associated with higher episodes of hypoglycemia that they defined differently from us as BG < 60 mg/dl. Chancellor et al.8, also measured clinical outcomes associated with their protocol in comparison with our study that focused on the effectiveness of EIC implementation. In addition, our study is in line with.
Shelden et al.11. used an electronic insulin protocol at the cardiovascular ICU at the University of Michigan where they demonstrated that aggressive nurse training led to an increase in conformation to target BG levels of 70–180. Yet, the protocol itself did not significantly change the incidence of hyper or hypoglycemia compared to pre-implementation. Compared to our study, Shelden et al.11 enrolled a larger number of patients, had a different target BG and different definition of hypoglycemia. In summary, EIC has been safely and successfully implemented in the perioperative setting.
It is important to highlight that we have chosen only a sample of the baseline state during the months of October 2019. This may not be representative of the entire population at baseline. In fact, analysis of the baseline state over a longer period demonstrated a higher maximum average compared to our analysis. In addition, we have analyzed average values at 3-time intervals intraoperatively rather than the highest values. The rationale behind this is the numerous blood draws taken during these time intervals and, more importantly, hyperglycemic value above the trigger point of EIC activation at 180 mg/dl may be too high undermining the effects of EIC by starting the protocol from too high of a blood glucose level.
We have analyzed all comers of CPB-requiring cardiac surgical patients rather than individual surgeries. These procedures vary widely in terms of duration of CPB, drugs administered on CPB and surgical practices, all factors that would have altered the blood glucose levels. Our rationale for using all comers is to test the performance of the EIC over a spectrum of blood glucose levels and to include previously overlooked, yet equally affected by worse outcomes, procedures such transplant and aortic surgeries.
Currently, the EIC is used hospital-wide. In response to the overshooting of BG that occur during CPB, we have added an additional iteration of the EIC to start the EIC at a lower threshold (140 mg/dl). A parallel hypoglycemia protocol has been added to treat any hypoglycemic events. We are currently exploring options of using machine learning to individualize the EIC delivery.
Our study has some limitations. First, we did not measure time to and time within target BG levels with our protocol, as has been the case in similar electronic protocols16. Second, we did not measure outcomes of hyperglycemia such as sternal wound infections and atrial fibrillation. This is attributed to the nature of this quality improvement study that focuses on the processes of achieving glycemic control. It is to be known, though, that previous studies found that commencement of intraoperative glycemic control is associated with a reduction in the incidence of surgical site infection in cardiac surgical patients17,18. Further study is warranted to determine the influence of the tighter intra-operative glucose management from our system on clinical outcomes.
Third, we have only analyzed intraoperative and a subset of postoperative glycemic control values prior to initiation of diet and resumption of glycemic control medications, all are important factors that influence glycemic control. Fourth, we have not accounted for the glucose infused via cardioplegia on CPB which could have explained the peak of BG during this period. However, the Del Nido cardioplegia used at our institution is a non-glucose containing and its contribution to the surge on pump BG is likely to be slim.
In summary, The EIC has created a stable process for the intraoperative control of BG in CPB-requiring cardiac surgical patients and has been successfully associated with a reduction in intraoperative BG values. Importantly, the electronic nature of this protocol reduces the rate of human errors and their consequential adverse events. Being an iterative process, more data are being collected to study clinical outcomes associated with glycemic control achieved through EIC.
In its ideal iteration, EIC is a potentially generalizable process that can be implemented intraoperatively to create a new standard of intraoperative glycemic control.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Jones, K. W. et al. Hyperglycemia predicts mortality after CABG: postoperative hyperglycemia predicts dramatic increases in mortality after coronary artery bypass graft surgery. J. Diabetes Complications. 22, 365–370 (2008).
Axelsson, T. A. et al. Long-term outcomes after coronary artery bypass surgery in patients with diabetes. Interact. Cardiovasc. Thorac. Surg. 30, 685–690 (2020).
Mifsud, S., Schembri, E. L. & Gruppetta, M. Stress-induced hyperglycaemia. Br. J. Hosp. Med. (Lond). 79, 634–639 (2018).
Boden, G. Gluconeogenesis and glycogenolysis in health and diabetes. J. Investig Med. 52, 375–378 (2004).
Saager, L. et al. A randomized study in diabetic patients undergoing cardiac surgery comparing computer-guided glucose management with a standard sliding scale protocol. J. Cardiothorac. Vasc Anesth. 22, 377–382 (2008).
Duncan, A. E. et al. Role of intraoperative and postoperative blood glucose concentrations in predicting outcomes after cardiac surgery. Anesthesiology 112, 860–871 (2010).
Russo, N. Perioperative glycemic control. Anesthesiol Clin. 30, 445–466 (2012).
Chancellor, W. Z. et al. Electronic glycemic management system and endocrinology service improve value in cardiac surgery. Am. Surg. 87, 568–575 (2021).
Lee, A. et al. Computerisation of a paper-based intravenous insulin protocol reduces errors in a prospective crossover simulated tight glycaemic control study. Intensive Crit. Care Nurs. 26, 161–168 (2010).
Alamri, N. & Seley, J. J. Evaluation of several electronic glycemic management systems. J. Diabetes Sci. Technol. 12, 60–62 (2018).
Shelden, D. et al. Improving hospital glucometrics, workflow, and outcomes with a computerized intravenous insulin dose calculator built into the electronic health record. J. Diabetes Sci. Technol. 15, 271–278 (2021).
White, N. H., Skor, D. & Santiago, J. V. Practical closed-loop insulin delivery. A system for the maintenance of overnight euglycemia and the calculation of basal insulin requirements in insulin-dependent diabetics. Ann. Intern. Med. 97, 210–213 (1982).
Davidson, P. C., Steed, R. D. & Bode, B. W. Glucommander: a computer-directed intravenous insulin system shown to be safe, simple, and effective in 120,618 h of operation. Diabetes Care. 28, 2418–2423 (2005).
Kaddoum, R. et al. Automated versus conventional perioperative glycemic control in adult diabetic patients undergoing open heart surgery. BMC Anesthesiol. 22, 184 (2022).
Herzig, D. et al. Perioperative fully Closed-Loop insulin delivery in patients undergoing elective surgery: an Open-Label, randomized controlled trial. Diabetes Care. 45, 2076–2083 (2022).
Blaha, J. et al. Comparison of three protocols for tight glycemic control in cardiac surgery patients. Diabetes Care. 32, 757–761 (2009).
Hweidi, I. M., Zytoon, A. M., Hayajneh, A. A., Al Obeisat, S. M. & Hweidi, A. I. The effect of intraoperative glycemic control on surgical site infections among diabetic patients undergoing coronary artery bypass graft (CABG) surgery. Heliyon 7, e08529 (2021).
Sato, H. et al. The association of preoperative glycemic control, intraoperative insulin sensitivity, and outcomes after cardiac surgery. J. Clin. Endocrinol. Metabolism. 95, 4338–4344 (2010).
Acknowledgements
Anesthesiology and Perioperative Medicine data resource supported by the UAB Department of Anesthesiology and Perioperative Medicine, provided Informatics services for this project.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by AZ, ZN, DB, GB, HS and JB. Editing of the manuscript was performed by TR, BH, JA, and CL. Conception of the insulin calculator protocol and editing of the manuscript was undertaken by JA. The first draft of the manuscript was written by [AZ] and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the University of Alabama Institutional Review Board (IRB) (IRB-300006438, 2022). Patients’ consent was waived by University of Alabama Institutional Review Board on the basis of: the research poses no more than minimal risks to subjects, the waiver would not alter or effect the rights or the welfare of the subjects involved in the research, the research could not be practically carried out without the waiver of consent, and It would not be appropriate to provide these subjects with information about the results of the research as the results would have no affect on the subjects. The procedure has been completed for these subjects. There is no anticipated benefit to subjects that would change what has already occurred. The EIC protocol has been implemented at our institution has become the standard of care.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zaky, A., Novak, Z., Roberson, T. et al. Controlling intraoperative hyperglycemia in the cardiac surgical patient using the computerized electronic insulin dose calculator. Sci Rep 15, 31930 (2025). https://doi.org/10.1038/s41598-025-17806-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-17806-4
